Different Risk for Hypertension, Diabetes, Dyslipidemia, and Hyperuricemia According to Level of Body Mass Index in Japanese and American Subjects

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
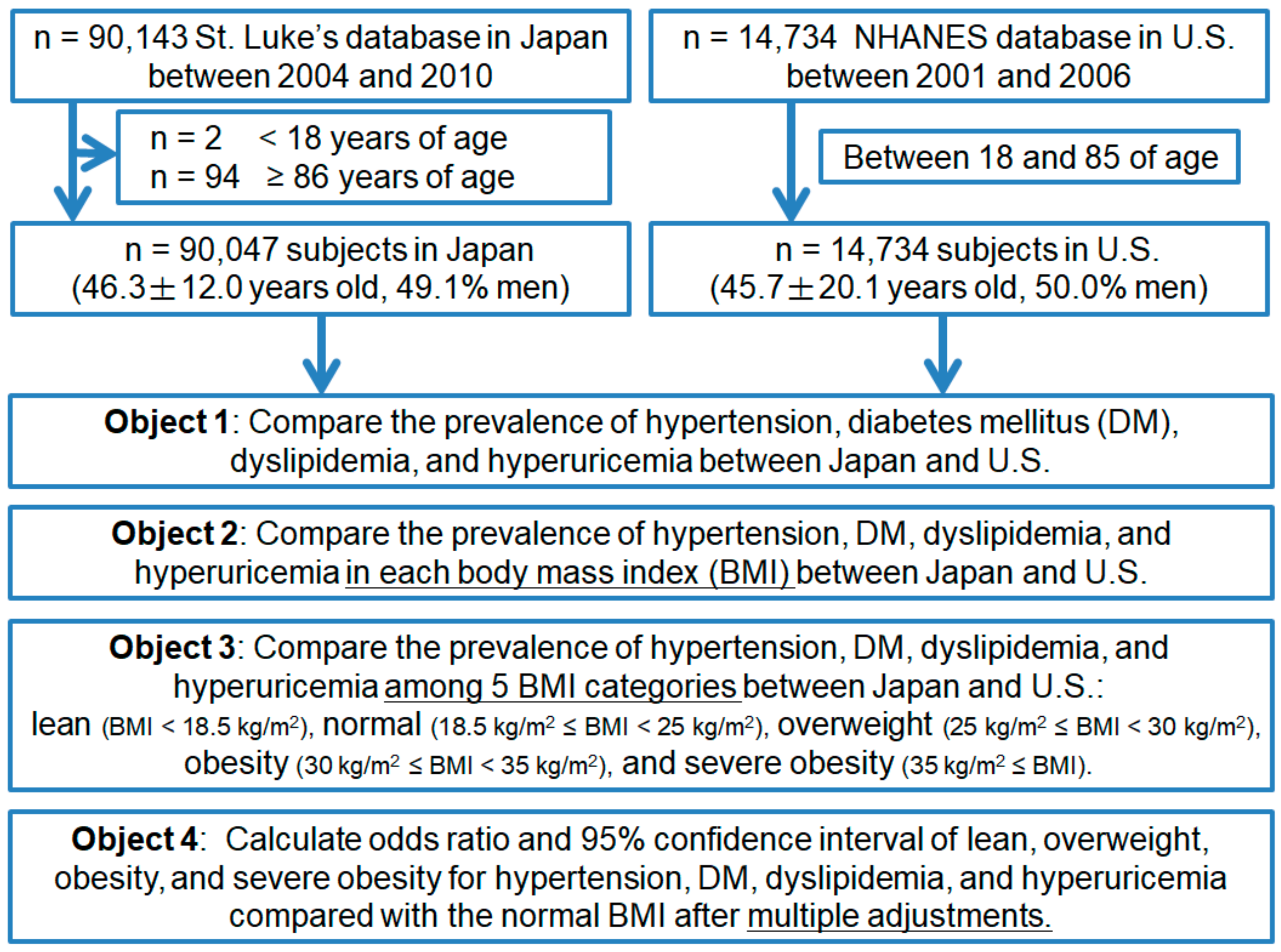
2.1. Study Population
2.2. Definition of the Cardio-Metabolic Risk Factors
2.3. Definition of Other Covariates
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Study Subjects Characteristics
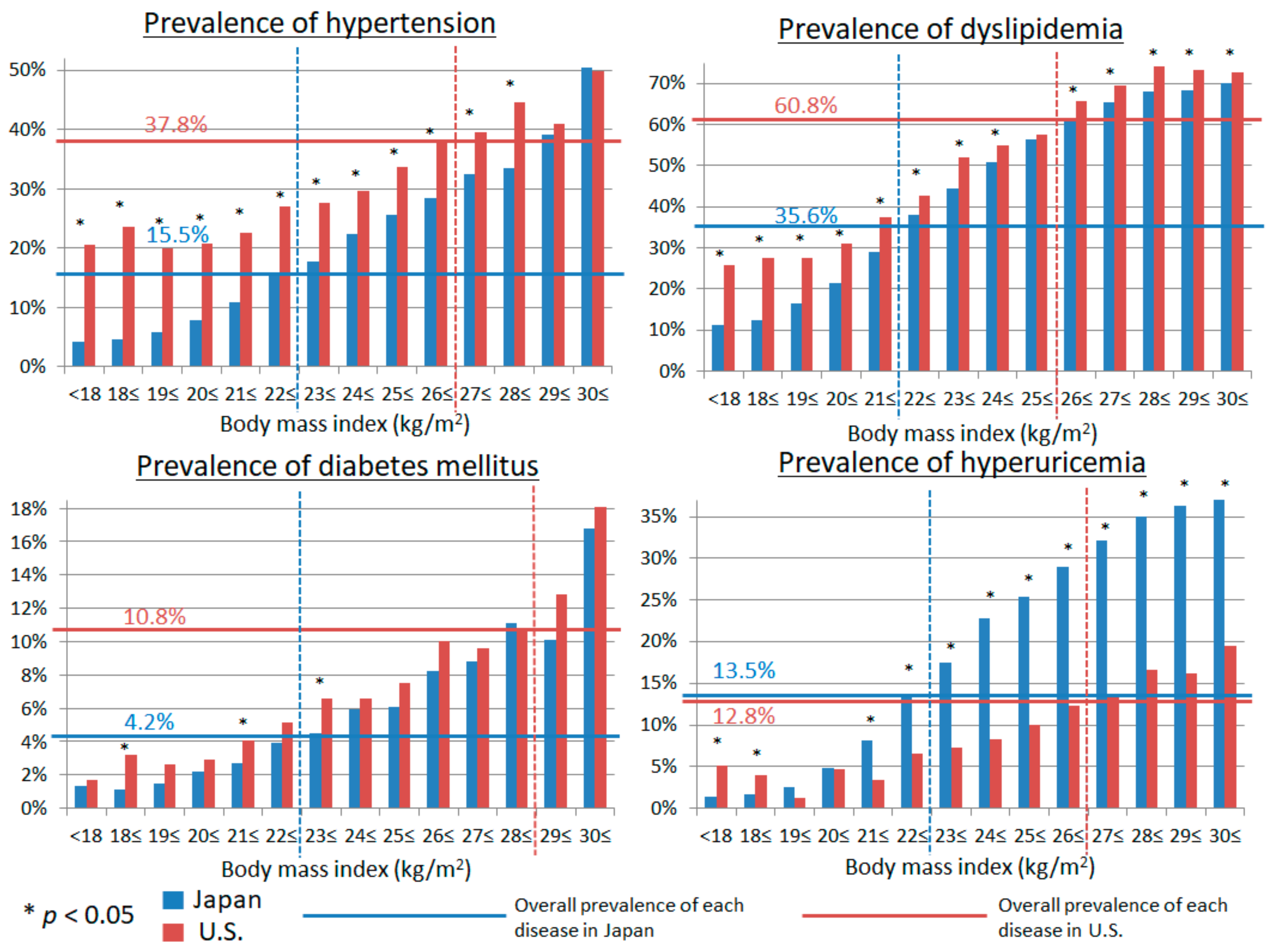
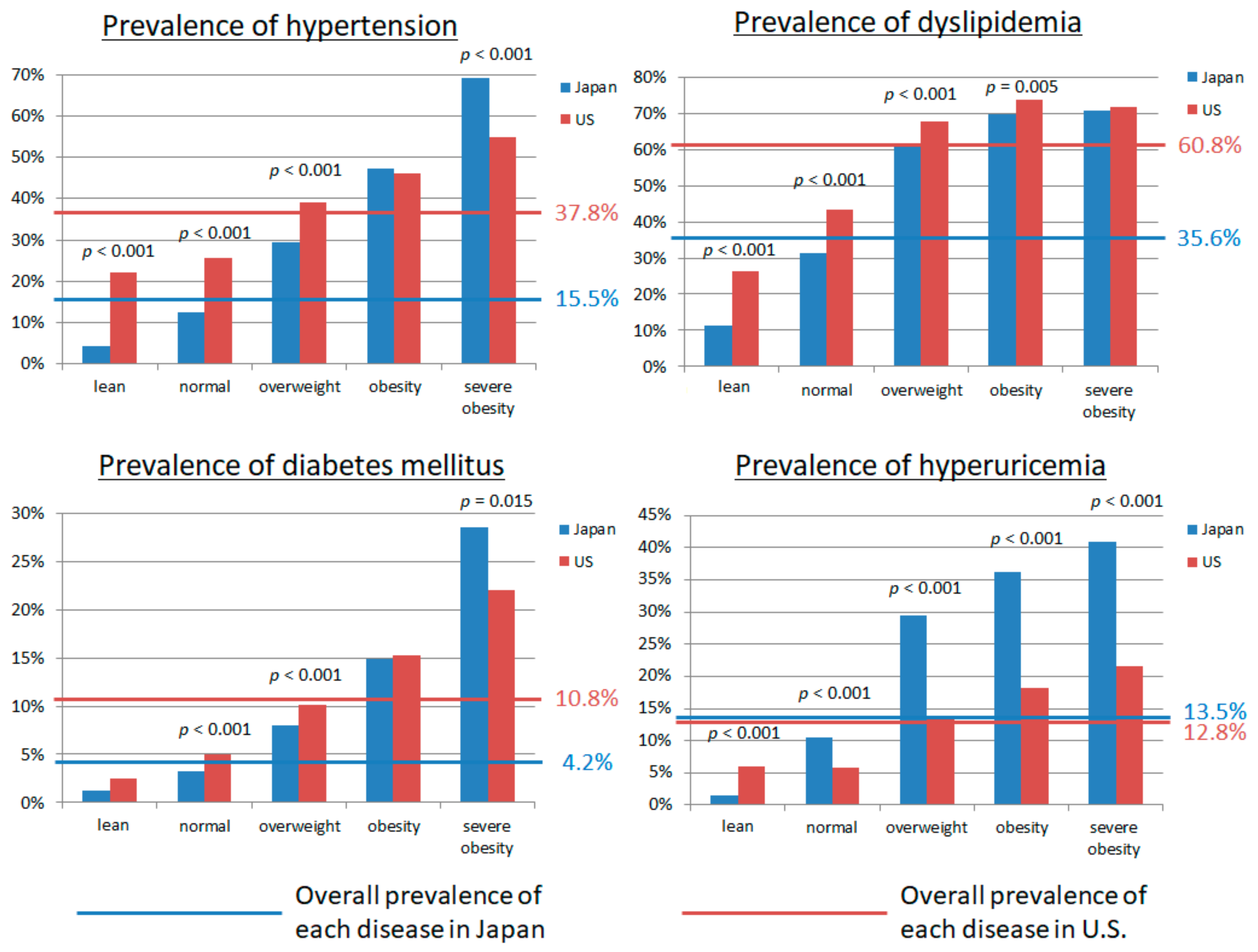
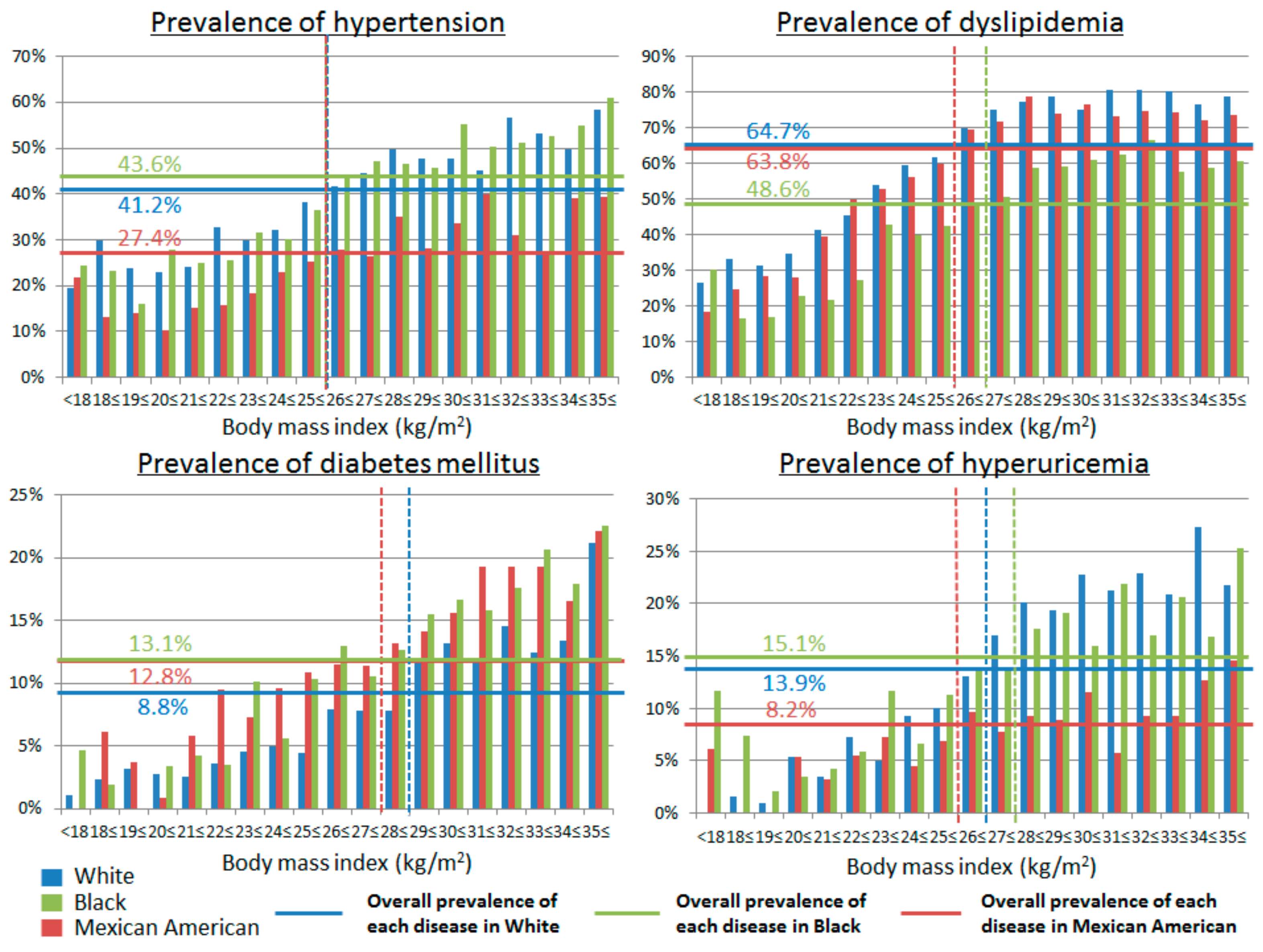
3.2. The Prevalence of Cardio-Metabolic Risk Factors in Relation to BMI in Japan and U.S.
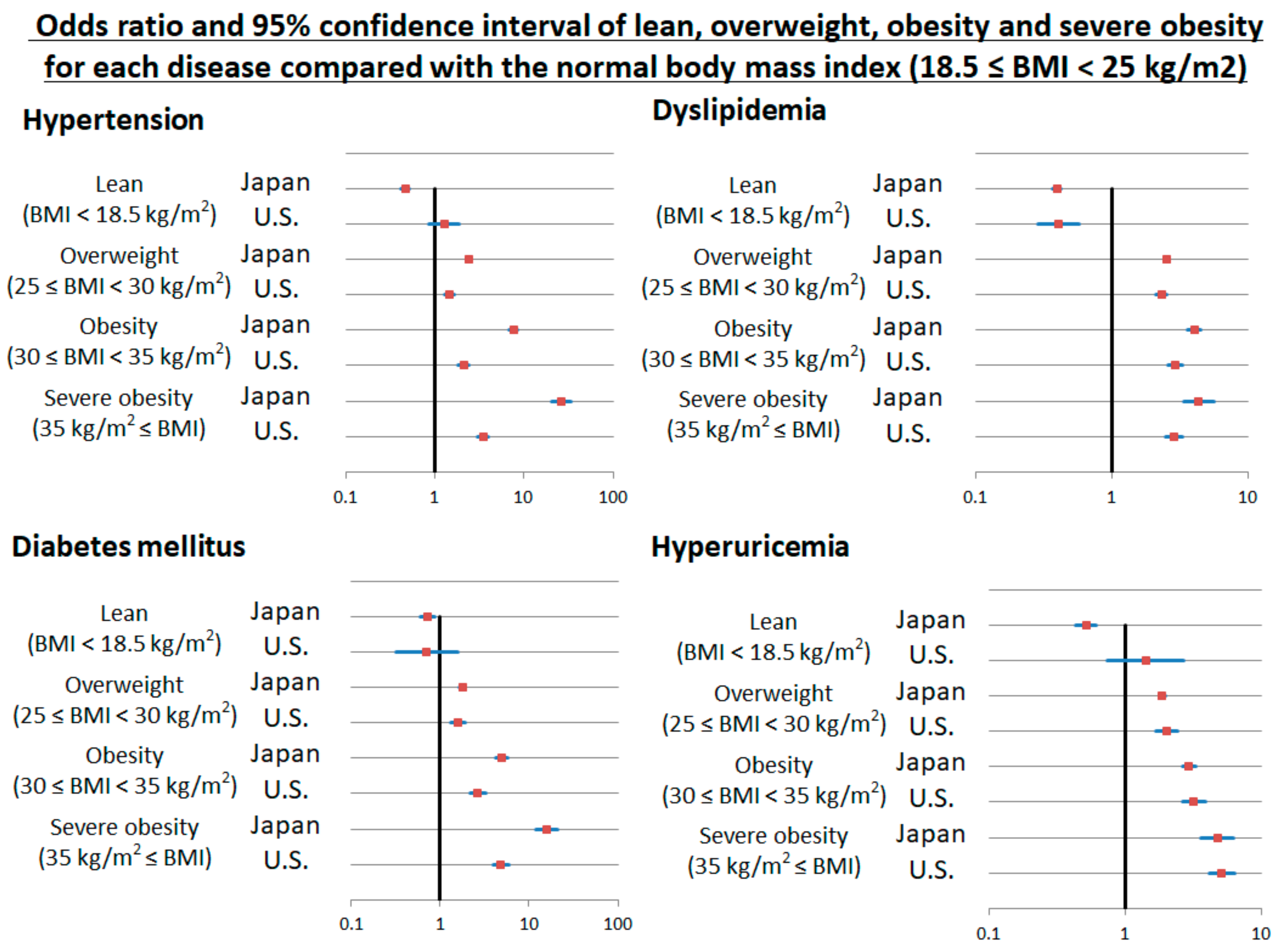
3.3. Multivariable Regression Analysis
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef]
- Droyvold, W.B.; Nilsen, T.I.; Kruger, O.; Holmen, T.L.; Krokstad, S.; Midthjell, K.; Holmen, J. Change in height, weight and body mass index: Longitudinal data from the hunt study in Norway. Int. J. Obes. 2006, 30, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Copeland, W.K.; Vedanthan, R.; Grant, E.; Lee, J.E.; Gu, D.; Gupta, P.C.; Ramadas, K.; Inoue, M.; Tsugane, S.; et al. Association between body mass index and cardiovascular disease mortality in east asians and south asians: Pooled analysis of prospective data from the asia cohort consortium. BMJ 2013, 347, f5446. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Health Observatory (GHO) Data; Overweight and Obesity. Available online: http://www.who.int/gho/ncd/risk_factors/overweight/en/ (accessed on 2 August 2018).
- Senauer, B.; Gemma, M. Why is the Obesity Rate So Low in Japan and High in the U.S.? Some Possible Economic Explanations. Food Ind. Center Univ. Minn. 2006. Available online: http://ageconsearch.umn.edu/record/14321/files/tr06-02s.pdf?version=1 (accessed on 2 August 2018).
- NCD Risk Factor Collaboration. Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef]
- WHO, Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Kuwabara, M.; Niwa, K.; Nishi, Y.; Mizuno, A.; Asano, T.; Masuda, K.; Komatsu, I.; Yamazoe, M.; Takahashi, O.; Hisatome, I. Relationship between serum uric acid levels and hypertension among Japanese individuals not treated for hyperuricemia and hypertension. Hypertens. Res. 2014, 37, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Niwa, K.; Nishihara, S.; Nishi, Y.; Takahashi, O.; Kario, K.; Yamamoto, K.; Yamashita, T.; Hisatome, I. Hyperuricemia is an independent competing risk factor for atrial fibrillation. Int. J. Cardiol. 2017, 231, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Hisatome, I.; Roncal-Jimenez, C.A.; Niwa, K.; Andres-Hernando, A.; Jensen, T.; Bjornstad, P.; Milagres, T.; Cicerchi, C.; Song, Z.; et al. Increased serum sodium and serum osmolarity are independent risk factors for developing chronic kidney disease; 5 year cohort study. PLoS ONE 2017, 12, e0169137. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Bjornstad, P.; Hisatome, I.; Niwa, K.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Jensen, T.; Milagres, T.; Sato, Y.; Garcia, G.; et al. Elevated serum uric acid level predicts rapid decline in kidney function. Am. J. Nephrol. 2017, 45, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Motoki, Y.; Ichiura, K.; Fujii, M.; Inomata, C.; Sato, H.; Morisawa, T.; Morita, Y.; Kuwabara, K.; Nakamura, Y. Association between toothbrushing and risk factors for cardiovascular disease: A large-scale, cross-sectional Japanese study. BMJ Open 2016, 6, e009870. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Motoki, Y.; Sato, H.; Fujii, M.; Ichiura, K.; Kuwabara, K.; Nakamura, Y. Low frequency of toothbrushing practices is an independent risk factor for diabetes mellitus in male and dyslipidemia in female: A large-scale, 5-year cohort study in Japan. J. Cardiol. 2017, 70, 107–112. [Google Scholar] [CrossRef] [PubMed]
- National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/ (accessed on 2 August 2018).[Green Version]
- Shimamoto, K.; Ando, K.; Fujita, T.; Hasebe, N.; Higaki, J.; Horiuchi, M.; Imai, Y.; Imaizumi, T.; Ishimitsu, T.; Ito, M.; et al. The Japanese society of hypertension guidelines for the management of hypertension (JSH 2014). Hypertens. Res. 2014, 37, 253–390. [Google Scholar] [PubMed]
- International Expert Committee. International expert committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, T.; Sasaki, J.; Ishibashi, S.; Birou, S.; Daida, H.; Dohi, S.; Egusa, G.; Hiro, T.; Hirobe, K.; Iida, M.; et al. Executive summary of the Japan atherosclerosis society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan—2012 version. J. Atheroscler. Thromb. 2013, 20, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, H. Japanese guideline for the management of hyperuricemia and gout: Second edition. Nucleosides Nucleotides Nucleic Acids 2011, 30, 1018–1029. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of diet in renal disease study group. Ann. Int. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- WHO. Physical Status: The Use and Interpretation of Anthropometry; Report of a WHO Expert Committee; WHO Technical Report Series 854; World Health Organization: Geneva, Switzerland, 1995. Available online: http://www.who.int/childgrowth/publications/physical_status/en/ (accessed on 2 August 2018).
- WHO. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. Available online: http://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/ (accessed on 2 August 2018).
- Popkin, B.M.; Siega-Riz, A.M.; Haines, P.S.; Jahns, L. Where’s the fat? Trends in U.S. Diets 1965–1996. Prev. Med. 2001, 32, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Serdula, M.K.; Dietz, W.H.; Bowman, B.A.; Marks, J.S.; Koplan, J.P. The continuing epidemic of obesity in the United States. JAMA 2000, 284, 1650–1651. [Google Scholar] [CrossRef] [PubMed]
- Sugano, M.; Hirahara, F. Polyunsaturated fatty acids in the food chain in Japan. Am. J. Clin. Nutr. 2000, 71, 189S–196S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Y.L.; Dixon, Z.; Himburg, S.; Huffman, F. Asian students change their eating patterns after living in the United States. J. Am. Diet. Assoc. 1999, 99, 54–57. [Google Scholar] [CrossRef]
- Tseng, M.; Wright, D.J.; Fang, C.Y. Acculturation and dietary change among Chinese immigrant women in the United States. J. Immigr. Minor. Health 2015, 17, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, T.; Kajio, H.; Sugiyama, T. Obesity, diabetes, and length of time in the United States: Analysis of national health and nutrition examination survey 1999 to 2012. Medicine 2016, 95, e4578. [Google Scholar] [CrossRef] [PubMed]
- Kitakaze, M. Trends in characteristics of CVD in Asia and Japan: The importance of epidemiological studies and beyond. J. Am. Coll. Cardiol. 2015, 66, 196–198. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. National Health and Nutrition Survey in 2010 (Kokumin Kenkou Eiyou Chousa) 2012. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450171 (accessed on 2 August 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Japan | U.S. | p | |
|---|---|---|---|
| Number of subjects | 90,047 | 14,734 | |
| Age (years old) | 46.3 ± 12.0 | 45.7 ± 20.1 | <0.001 |
| Sex (male) | 49.1% | 50.0% | 0.090 |
| Height (cm) | 164.3 ± 8.7 | 167.7 ± 10.2 | <0.001 |
| Weight (kg) | 60.8 ± 12.4 | 79.5 ± 20.2 | <0.001 |
| Body mass index (kg/m2) | 22.4 ± 3.3 | 28.2 ± 6.4 | <0.001 |
| Smoking | 40.6% | 49.1% | <0.001 |
| Drinking habits | 62.1% | 67.8% | <0.001 |
| Hypertension | 15.5% | 37.8% | <0.001 |
| Diabetes mellitus | 4.2% | 10.8% | <0.001 |
| Fasting blood glucose (mg/dL) | 99.4 ± 15.6 | 97.1 ± 33.2 | <0.001 |
| HbA1c (%) | 5.10 ± 0.59 | 5.54 ± 0.97 | <0.001 |
| Dyslipidemia | 35.6% | 60.8% | <0.001 |
| Total cholesterol (mg/dL) | 201.4 ± 34.4 | 199.2 ± 44.1 | <0.003 |
| Low-density lipoprotein cholesterol (mg/dL) | 116.8 ± 30.7 | 132.8 ± 44.9 | <0.002 |
| High-density lipoprotein cholesterol (mg/dL) | 62.4 ± 15.6 | 53.9 ± 16.1 | <0.001 |
| Triglyceride (mg/dL) | 100.3 ± 81.9 | 143.8 ± 135.7 | <0.000 |
| Hyperuricemia | 13.5% | 12.8% | 0.020 |
| Serum uric acid (mg/dL) | 5.29 ± 1.42 | 5.34 ± 1.44 | <0.001 |
| Chronic kidney disease | 5.7% | 7.5% | <0.001 |
| Japan | U.S. | ||||||
|---|---|---|---|---|---|---|---|
| Hypertension | OR | 95% CI | p | OR | 95% CI | p | |
| Body mass index | per 1 kg/m2 increased | 1.230 | 1.222–1.239 | <0.001 | 1.068 | 1.060–1.077 | <0.001 |
| Diabetes mellitus | |||||||
| Body mass index | per 1 kg/m2 increased | 1.170 | 1.157–1.182 | <0.001 | 1.086 | 1.076–1.096 | <0.001 |
| Dyslipidemia | |||||||
| Body mass index | per 1 kg/m2 increased | 1.223 | 1.217–1.230 | <0.001 | 1.073 | 1.065–1.081 | <0.001 |
| Hyperuricemia | |||||||
| Body mass index | per 1 kg/m2 increased | 1.157 | 1.148–1.166 | <0.001 | 1.089 | 1.078–1.100 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuwabara, M.; Kuwabara, R.; Niwa, K.; Hisatome, I.; Smits, G.; Roncal-Jimenez, C.A.; MacLean, P.S.; Yracheta, J.M.; Ohno, M.; Lanaspa, M.A.; et al. Different Risk for Hypertension, Diabetes, Dyslipidemia, and Hyperuricemia According to Level of Body Mass Index in Japanese and American Subjects. Nutrients 2018, 10, 1011. https://doi.org/10.3390/nu10081011
Kuwabara M, Kuwabara R, Niwa K, Hisatome I, Smits G, Roncal-Jimenez CA, MacLean PS, Yracheta JM, Ohno M, Lanaspa MA, et al. Different Risk for Hypertension, Diabetes, Dyslipidemia, and Hyperuricemia According to Level of Body Mass Index in Japanese and American Subjects. Nutrients. 2018; 10(8):1011. https://doi.org/10.3390/nu10081011
Chicago/Turabian StyleKuwabara, Masanari, Remi Kuwabara, Koichiro Niwa, Ichiro Hisatome, Gerard Smits, Carlos A. Roncal-Jimenez, Paul S. MacLean, Joseph M. Yracheta, Minoru Ohno, Miguel A. Lanaspa, and et al. 2018. "Different Risk for Hypertension, Diabetes, Dyslipidemia, and Hyperuricemia According to Level of Body Mass Index in Japanese and American Subjects" Nutrients 10, no. 8: 1011. https://doi.org/10.3390/nu10081011