A Synergistic Formulation of Plant Extracts Decreases Postprandial Glucose and Insulin Peaks: Results from Two Randomized, Controlled, Cross-Over Studies Using Real-World Meals

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
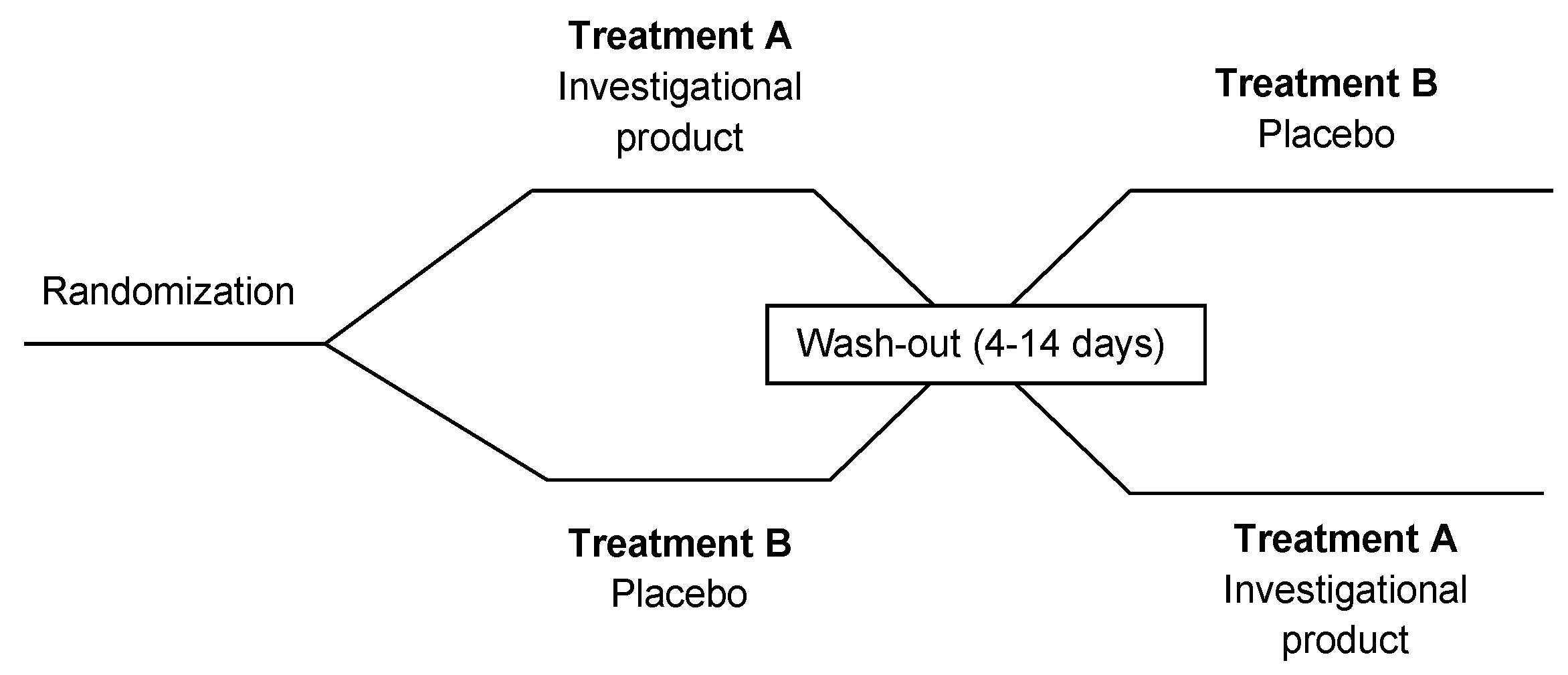
2.1. Study Design
2.2. Investigational Products
2.3. Inclusion and Exclusion Criteria
2.4. Meals
2.5. Study Procedures
2.6. Anthropometric Measurements
2.7. Biochemical Measurements
2.8. Statistical Analysis
- Independent samples Student’s t-test will be conducted.
- Hypothesis H0: means in both populations are equal, therefore m1 = m2.
- Hypothesis H1: means in both populations are different, therefore m1 ≠ m2.
- Significance level (probability of type I error): a = 0.05.
- Standard deviation in the population: s = 60 and s = 75.
- Target power: 80% and 90%.
2.9. Ethical Approval and Consent to Participate
3. Results
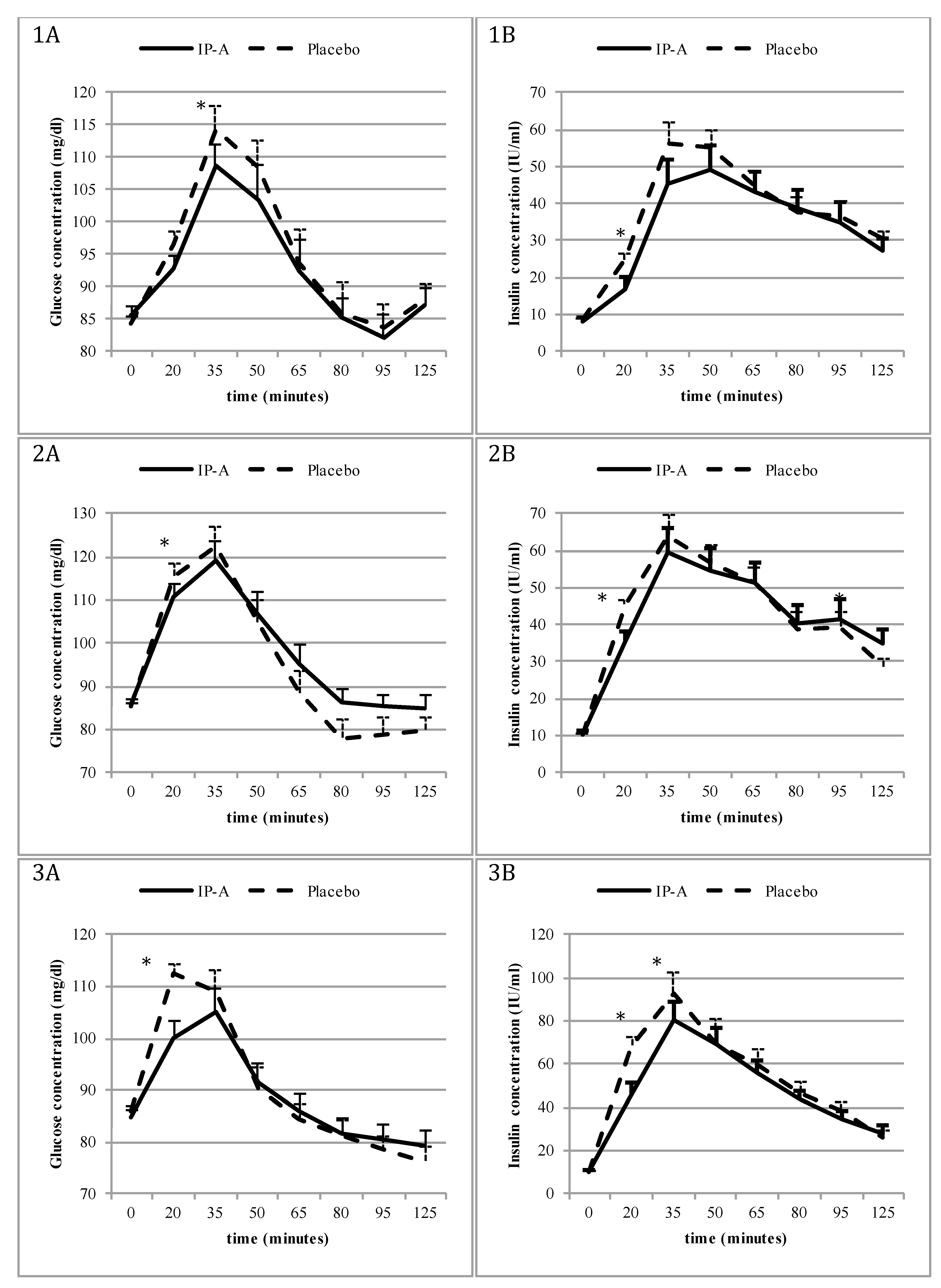
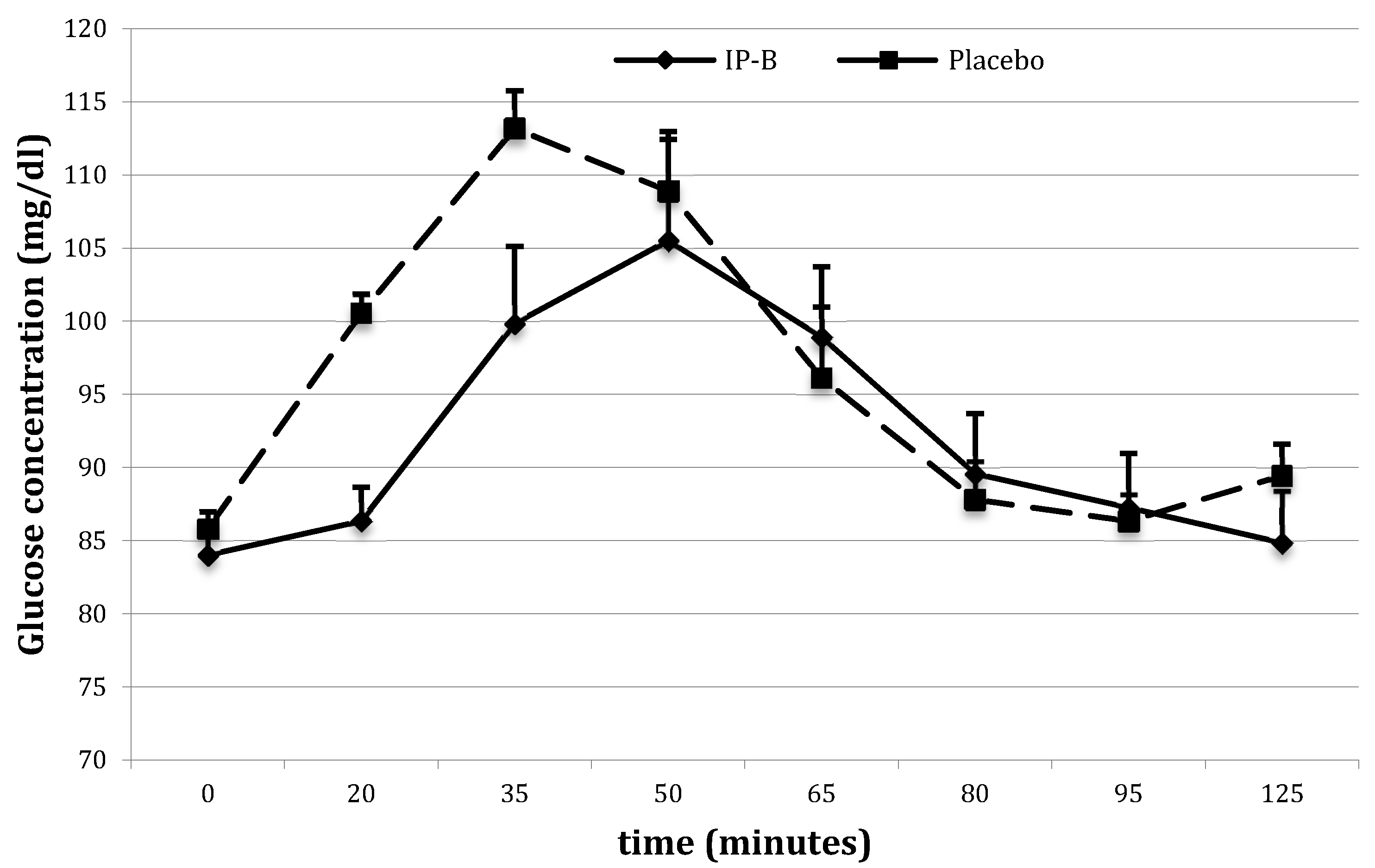
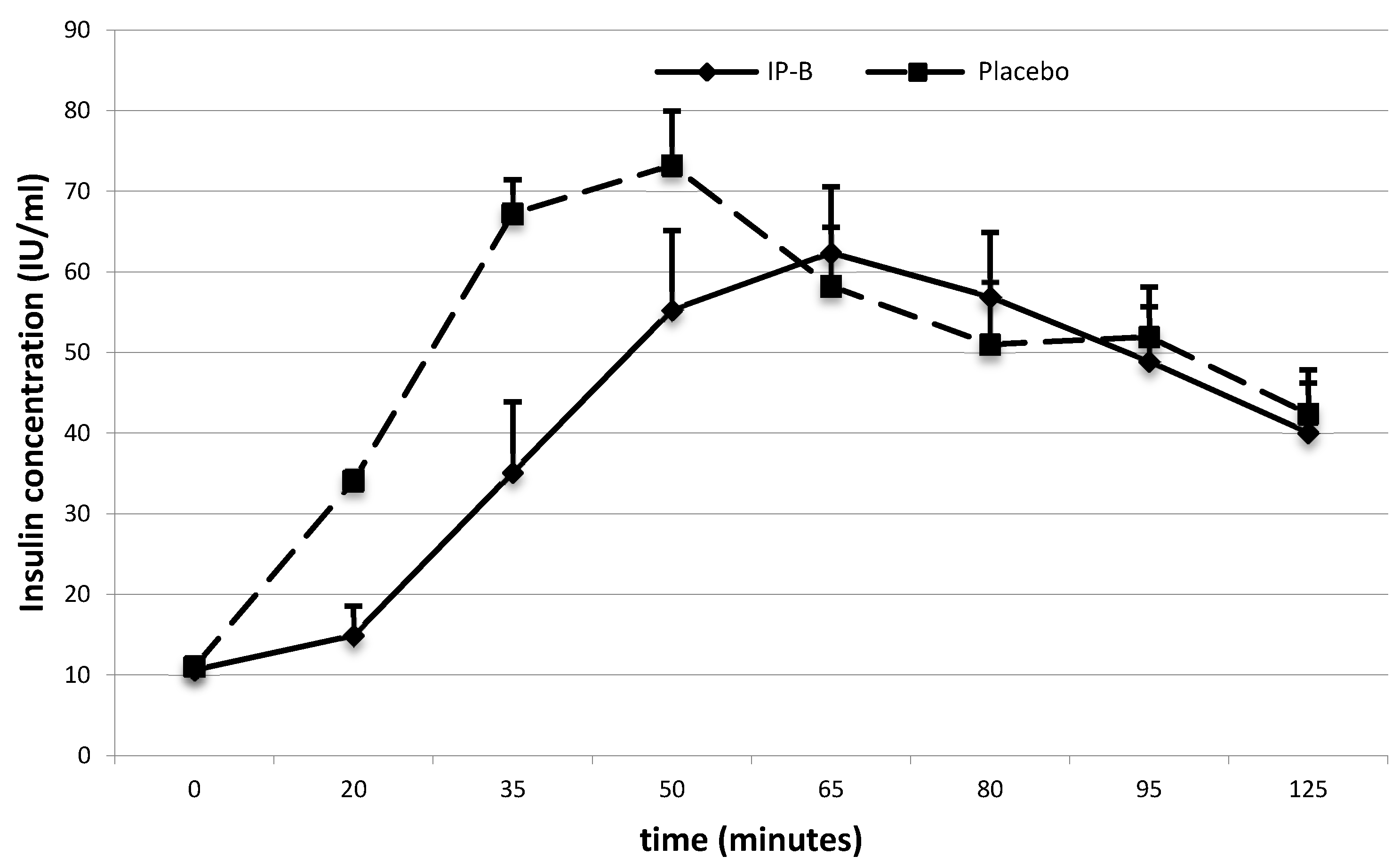
3.1. The Effect of IP-A/IP-B on Glucose and Insulin Concentrations after a High-GI/GL Meal (Study 1)
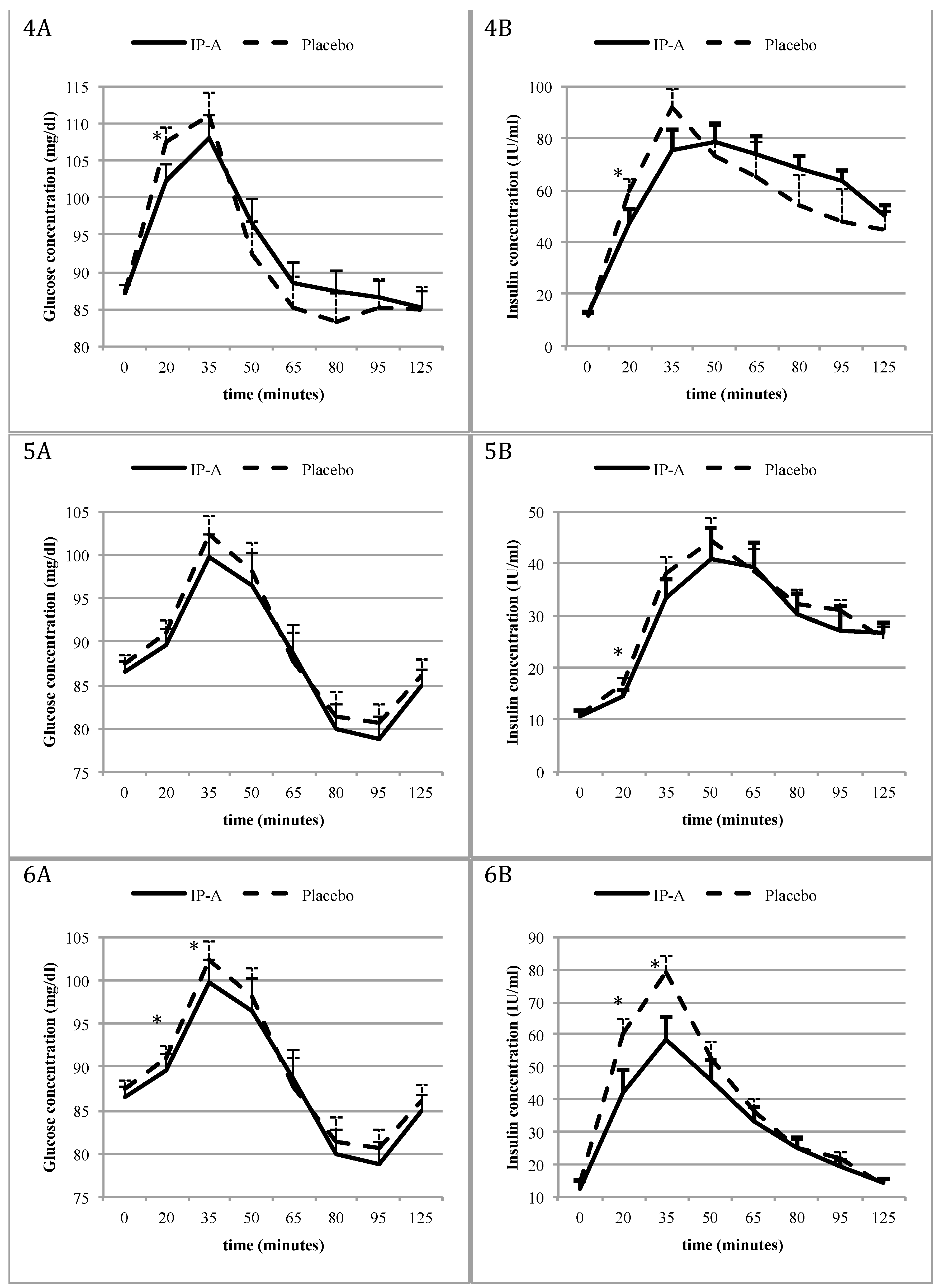
3.2. Effect of IP-A on Glucose and Insulin Levels Following Various High-GI/GL Meals (Study 2)
3.3. Effect of IP-A/IP-B on the Number of Hypoglycaemic Episodes
3.4. Safety of IP-A
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Makris, A.; Foster, G.D. Dietary approaches to the treatment of obesity. Psychiatr. Clin. N. Am. 2011, 34, 813–827. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M. Low-glycemic load diets: How does the evidence for prevention of disease measure up? J. Am. Diet. Assoc. 2010, 110, 1818–1819. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.B. High-glycemic index foods, hunger, and obesity: Is there a connection? Nutr. Rev. 2000, 58, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, J.L.; Gomis, R.; Hanefeld, M.; Josse, R.G.; Karasik, A.; Laakso, M. The STOP-NIDDM Trial: An international study on the efficacy of an alpha-glucosidase inhibitor to prevent type 2 diabetes in a population with impaired glucose tolerance: Rationale, design, and preliminary screening data. Study to Prevent Non-Insulin-Dependent Diabetes Mellitus. Diabetes Care 1998, 21, 1720–1725. [Google Scholar] [PubMed]
- Chiasson, J.L.; Josse, R.G.; Gomis, R.; Hanefeld, M.; Karasik, A.; Laakso, M. Acarbose for prevention of type 2 diabetes mellitus: The STOP-NIDDM randomised trial. Lancet 2002, 359, 2072–2077. [Google Scholar] [CrossRef]
- Chiasson, J.L.; Josse, R.G.; Gomis, R.; Hanefeld, M.; Karasik, A.; Laakso, M. Acarbose treatment and the risk of cardiovascular disease and hypertension in patients with impaired glucose tolerance: The STOP-NIDDM trial. JAMA 2003, 290, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, J.L.; Josse, R.G.; Gomis, R.; Hanefeld, M.; Karasik, A.; Laakso, M. STOP-NIDDM Trail Research Group. Acarbose for the prevention of Type 2 diabetes, hypertension and cardiovascular disease in subjects with impaired glucose tolerance: Facts and interpretations concerning the critical analysis of the STOP-NIDDM Trial data. Diabetologia 2004, 47, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Kapoor, R.; Thathola, A.; Srivastava, R.P. Nutritional quality of leaves of some genotypes of mulberry (Morus alba). Int. J. Food Sci. Nutr. 2006, 57, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Thabti, I.; Elfalleh, W.; Hannachi, H.; Ferchichi, A.; Campos, M.D.G. Identification and quantification of phenolic acids and flavonol glycosides in Tunisian Morus species by HPLC-DAD and HPLC–MS. J. Funct. Foods 2012, 4, 367–374. [Google Scholar] [CrossRef]
- Oku, T.; Yamada, M.; Nakamura, M.; Sadamori, N.; Nakamura, S. Inhibitory effects of extractives from leaves of Morus alba on human and rat small intestinal disaccharidase activity. Br. J. Nutr. 2006, 95, 933–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Layer, P.; Zinsmeister, A.R.; DiMagno, E.P. Effects of decreasing intraluminal amylase activity on starch digestion and postprandial gastrointestinal function in humans. Gastroenterology 1986, 91, 41–48. [Google Scholar] [CrossRef]
- Welsch, C.A.; Lachance, P.A.; Wasserman, B.P. Dietary phenolic compounds: Inhibition of Na+-dependent d-glucose uptake in rat intestinal brush border membrane vesicles. J. Nutr. 1989, 119, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Blum, J.; Lemaire, B.; Lafay, S. Effect of a green decaffeinated coffee extract on glyacemia. A Pilot Prospective Clinical Study. Nutr. Foods 2007, 6, 13–17. [Google Scholar]
- Kwon, O.; Eck, P.; Chen, S.; Corpe, C.P.; Lee, J.H.; Kruhlak, M.; Levine, M. Inhibition of the intestinal glucose transporter GLUT2 by flavonoids. FASEB J. 2007, 21, 366–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adisakwattana, S.; Ruengsamran, T.; Kampa, P.; Sompong, W. In vitro inhibitory effects of plant-based foods and their combinations on intestinal alpha-glucosidase and pancreatic alpha-amylase. BMC Complement. Altern. Med. 2012, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Banu, S.; Jabir, N.R.; Manjunath, N.C.; Khan, M.S.; Ashraf, G.M.; Kamal, M.A.; Tabrez, S. Reduction of post-prandial hyperglycemia by mulberry tea in type-2 diabetes patients. Saudi J. Biol. Sci. 2015, 22, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Udani, J.K.; Singh, B.B.; Barrett, M.L.; Preuss, H.G. Lowering the glycemic index of white bread using a white bean extract. Nutr. J. 2009, 8, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, K.L.; Clifford, M.N.; Morgan, L.M. Coffee acutely modifies gastrointestinal hormone secretion and glucose tolerance in humans: Glycemic effects of chlorogenic acid and caffeine. Am. J. Clin. Nutr. 2003, 78, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Sambol, N.C.; Chiang, J.; O’Conner, M.; Liu, C.Y.; Lin, E.T.; Goodman, A.M.; Benet, L.Z.; Karam, J.H. Pharmacokinetics and pharmacodynamics of metformin in healthy subjects and patients with noninsulin-dependent diabetes mellitus. J. Clin. Pharmacol. 1996, 36, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.S.; O’Keefe, J.H.; Jellinger, P. Postprandial dysmetabolism: The missing link between diabetes and cardiovascular events? Endocr. Pract. 2008, 14, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Bonora, E. Postprandial peaks as a risk factor for cardiovascular disease: Epidemiological perspectives. Int. J. Clin. Pract. Suppl. 2002, 129, 5–11. [Google Scholar]
- O’Keefe, J.H.; Bell, D.S. Postprandial hyperglycemia/hyperlipidemia (postprandial dysmetabolism) is a cardiovascular risk factor. Am. J. Cardiol. 2007, 100, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Kawahito, S.; Kitahata, H.; Oshita, S. Problems associated with glucose toxicity: Role of hyperglycemia-induced oxidative stress. World J. Gastroenterol. 2009, 15, 4137–4142. [Google Scholar] [CrossRef] [PubMed]
- Moghaddam, E.; Vogt, J.A.; Wolever, T.M. The effects of fat and protein on glycemic responses in nondiabetic humans vary with waist circumference, fasting plasma insulin, and dietary fiber intake. J. Nutr. 2006, 136, 2506–2511. [Google Scholar] [CrossRef] [PubMed]
- Guldstrand, M.C.; Simberg, C.L. High-fat diets: Healthy or unhealthy? Clin. Sci. 2007, 113, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Ahren, B. Insulin secretion and insulin sensitivity in relation to fasting glucose in healthy subjects. Diabetes Care 2007, 30, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Shanik, M.H.; Xu, Y.; Skrha, J.; Dankner, R.; Zick, Y.; Roth, J. Insulin resistance and hyperinsulinemia: Is hyperinsulinemia the cart or the horse? Diabetes Care 2008, 31 (Suppl. 2), S262–S268. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, T.; Allison, G.; Abbasi, F.; Lamendola, C.; Reaven, G. Prevalence of insulin resistance and associated cardiovascular disease risk factors among normal weight, overweight, and obese individuals. Metabolism 2004, 53, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Baltali, M.; Korkmaz, M.E.; Kiziltan, H.T.; Muderris, I.H.; Ozin, B.; Anarat, R. Association between postprandial hyperinsulinemia and coronary artery disease among non-diabetic women: A case control study. Int. J. Cardiol. 2003, 88, 215–221. [Google Scholar] [CrossRef]
- Brun, J.F.; Fedou, C.; Mercier, J. Postprandial reactive hypoglycemia. Diabetes Metab. 2000, 26, 337–351. [Google Scholar] [PubMed]
- Barrett, M.L.; Udani, J.K. A proprietary alpha-amylase inhibitor from white bean (Phaseolus vulgaris): A review of clinical studies on weight loss and glycemic control. Nutr. J. 2011, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, T.K.; Glavits, R.; Endres, J.R.; Palmer, P.A.; Clewell, A.E.; Murbach, T.S.; Hirka, G.; Pasics, I. A 28-Day Repeated Dose Toxicological Study of an Aqueous Extract of Morus Alba L. Int. J. Toxicol. 2016, 35, 683–691. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N) | Male/Female (n) | Age (years) | BMI (kg/m2) | |
|---|---|---|---|---|
| Study 1 | 32 | 19/13 | 26.7 ± 3.7 | 26.51 ± 1.6 |
| IP-A | 16 | 10/6 | 26.9 ± 3.6 | 26.4 ± 3.8 |
| IP-B | 16 | 9/7 | 26.4 ± 1.6 | 26.7 ± 1.7 |
| Study 2 (IP-A) | 150 | 67/83 | 28.2 ± 9.2 | 25.5 ± 3.0 |
| Meal 1 | 30 | 18/17 | 28.8 ± 9.6 | 25.6 ± 5.0 |
| Meal 2 | 30 | 12/18 | 26.3 ± 7.8 | 25.6 ± 2.3 |
| Meal 3 | 30 | 13/17 | 26.7 ± 8.2 | 25.2 ± 2.0 |
| Meal 4 | 30 | 13/17 | 29.2 ± 9.9 | 25.6 ± 2.3 |
| Meal 5 | 30 | 11/19 | 30.0 ± 9.8 | 25.6 ± 2.0 |
| Meal | Portion (g) | Energy (kcal) | Total Carbohydrate (g) | Total Protein (g) | Total Fat (g) | |
|---|---|---|---|---|---|---|
| Study 1 | White roll | 150 | 481 | 92.0 | 13.1 | 6.0 |
| Water | 200 | - | - | - | - | |
| Total | 481 | 92.0 | 13.1 | 6.0 | ||
| Study 2 (Meal 1) | Cola 1 | 400 | 168 | 42.4 | - | - |
| Corn puffs 2 | 50 | 179 | 40.0 | 3.5 | 0.5 | |
| Total | 347 | 82.4 | 3.5 | 0.5 | ||
| Study 2 (Meal 2) | Corn flakes 3 | 50 | 188 | 37.0 | 4.5 | 1.5 |
| Milk 4 | 400 | 272 | 42.0 | 12.0 | 6.0 | |
| Total | 460 | 79 | 16.5 | 7.5 | ||
| Study 2 (Meal 3) | Muffin 5 | 120 | 293 | 54.9 | 6.0 | 9.0 |
| Yogurt 6 | 300 | 219 | 36.0 | 8.7 | 4.8 | |
| Total | 512 | 90.9 | 14.7 | 13.8 | ||
| Study 2 (Meal 4) | Fries 7 | 200 | 598 | 74.0 | 6.8 | 30.0 |
| Ketchup 7 | 20 | 26 | 6.0 | 0.4 | 0.0 | |
| Total | 624 | 80.0 | 7.2 | 30.0 | ||
| Study 2 (Meal 5) | Macaroni & Cheese Dinner 8 | 58+ water | 220 | 41.0 | 6.0 | 3.0 |
| Total | 220 | 41.0 | 6.0 | 3.0 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamska-Patruno, E.; Billing-Marczak, K.; Orlowski, M.; Gorska, M.; Krotkiewski, M.; Kretowski, A. A Synergistic Formulation of Plant Extracts Decreases Postprandial Glucose and Insulin Peaks: Results from Two Randomized, Controlled, Cross-Over Studies Using Real-World Meals. Nutrients 2018, 10, 956. https://doi.org/10.3390/nu10080956
Adamska-Patruno E, Billing-Marczak K, Orlowski M, Gorska M, Krotkiewski M, Kretowski A. A Synergistic Formulation of Plant Extracts Decreases Postprandial Glucose and Insulin Peaks: Results from Two Randomized, Controlled, Cross-Over Studies Using Real-World Meals. Nutrients. 2018; 10(8):956. https://doi.org/10.3390/nu10080956
Chicago/Turabian StyleAdamska-Patruno, Edyta, Katarzyna Billing-Marczak, Marek Orlowski, Maria Gorska, Marcin Krotkiewski, and Adam Kretowski. 2018. "A Synergistic Formulation of Plant Extracts Decreases Postprandial Glucose and Insulin Peaks: Results from Two Randomized, Controlled, Cross-Over Studies Using Real-World Meals" Nutrients 10, no. 8: 956. https://doi.org/10.3390/nu10080956