
Efficacy of Sonic-Powered and Manual Toothbrushes on Plaque-Induced Gingivitis in Pregnant Women: A Randomized Controlled Trial
 , , , ,
, , , ,
Abstract
:1. Introduction
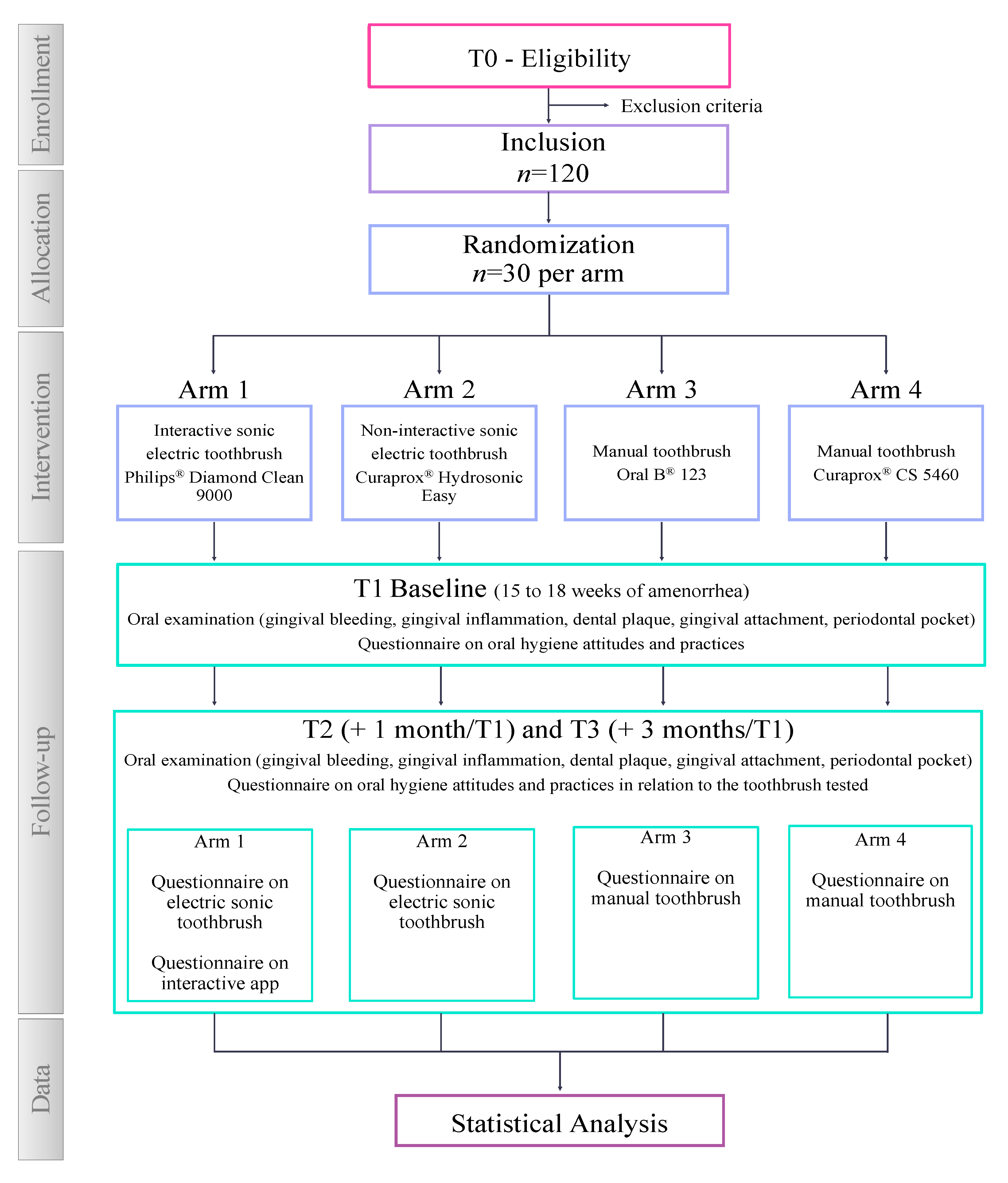
2. Experimental Design
2.1. Trial Design
2.2. Study Setting
2.3. Study Population
2.3.1. Eligibility Criteria
2.3.2. Exclusion Criteria
2.4. Materials Description
2.5. Interventions
2.6. Outcomes
2.6.1. Primary Outcome Measures
2.6.2. Secondary Outcome Measures
2.7. Timeline of Participant
2.7.1. Pre-Screening and Eligibility Assessment (T0)
2.7.2. Inclusion, Oral Examination and Questionnaire (T1)
- (i)
- Bleeding on probing (BOP): Dichotomous gingival index reporting the presence/absence of bleeding on probing after 30 s (0 = absence of bleeding after 30 s, and 1 = presence bleeding after 30 s). Four sites are recorded per tooth (mesio-buccal, disto-buccal, mesio-palatine and disto-palatine) [30,31].
- (ii)
- Gingivitis score (Gingival Index, GI): Measured through visual observation from 0 to 3 (0 = no inflammation; 1 = slight change, slight inflammation in color and little change in texture; 2 = moderate, moderate inflammation, redness, edema and hypertrophy, tendency to bleed on probing; 3 = severe, marked redness, inflammation and hypertrophy; tendency to spontaneous bleeding). Gingivitis score = sum of GI scores divided by number of total sites [32].
- (iii)
- Dental plaque score (Rustogi Modified Navy Plaque Index, RMNPI): According to the Navy plaque index modified by Rustogi et al., the presence of plaque deposits is sought on the vestibular and lingual surfaces of the teeth. Each tooth face is divided into 9 areas to which a dichotomous score is assigned (0 = absence of plaque; 1 = presence of plaque). Thus, for each tooth, 18 measurements are carried out. This index makes it possible to detect minimal differences at the partial level of the marginal/interproximal zones, or at the total level of the oral cavity [33].
- (iv)
- Probing pocket depth (PPD) score: Measure indicating the distance separating the top of the marginal gingiva from the bottom of the periodontal pocket. The measurement is expressed in millimeters. Four sites are recorded per tooth (mesio-buccal, disto-buccal, mesio-palatine and disto-palatine) [34].
- (v)
- Clinical Attachment Loss (CAL) score: Addition of PPD and recession height, which is the distance separating the enamel–cementum junction from the bottom of the pocket. Four sites are recorded per tooth (mesio-buccal, disto-buccal, mesio-palatine and disto-palatine) [31].
2.7.3. Follow-Up Visits (T2 and T3)
2.8. Ethics Statement
2.9. Sample Size
3. Procedure
3.1. Recruitment
3.2. Allocation of Interventions
3.2.1. Allocation
3.2.2. Blinding
3.3. Data Collection, Management and Analysis
3.3.1. Data Collection Methods
3.3.2. Data Management
3.3.3. Data Analysis Methods
4. Expected Results
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Available online: https://www.who.int/publications-detail-redirect/9789241549912 (accessed on 23 August 2023).
- Wu, M.; Chen, S.-W.; Jiang, S.-Y. Relationship between Gingival Inflammation and Pregnancy. Mediators Inflamm. 2015, 2015, 623427. [Google Scholar] [CrossRef] [PubMed]
- Bett, J.V.S.; Batistella, E.Â.; Melo, G.; Munhoz, E.d.A.; Silva, C.A.B.; Guerra, E.N.d.S.; Porporatti, A.L.; De Luca Canto, G. Prevalence of Oral Mucosal Disorders during Pregnancy: A Systematic Review and Meta-Analysis. J. Oral. Pathol. Med. 2019, 48, 270–277. [Google Scholar] [CrossRef]
- Carrillo-de-Albornoz, A.; Figuero, E.; Herrera, D.; Bascones-Martínez, A. Gingival Changes during Pregnancy: II. Influence of Hormonal Variations on the Subgingival Biofilm. J. Clin. Periodontol. 2010, 37, 230–240. [Google Scholar] [CrossRef]
- Geurs, N.C.; Jeffcoat, M.K.; Tanna, N.; Geisinger, M.L.; Parry, S.; Biggio, J.R.; Doyle, M.J.; Grender, J.M.; Gerlach, R.W.; Reddy, M.S. A Randomized Controlled Clinical Trial of Prenatal Oral Hygiene Education in Pregnancy-Associated Gingivitis. J. Midwifery Womens Health 2023, 68, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Lieske, B.; Makarova, N.; Jagemann, B.; Walther, C.; Ebinghaus, M.; Zyriax, B.-C.; Aarabi, G. Inflammatory Response in Oral Biofilm during Pregnancy: A Systematic Review. Nutrients 2022, 14, 4894. [Google Scholar] [CrossRef]
- Gare, J.; Kanoute, A.; Meda, N.; Viennot, S.; Bourgeois, D.; Carrouel, F. Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7194. [Google Scholar] [CrossRef] [PubMed]
- Murakami, S.; Mealey, B.L.; Mariotti, A.; Chapple, I.L.C. Dental Plaque-Induced Gingival Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S17–S27. [Google Scholar] [CrossRef] [PubMed]
- Saini, R.; Saini, S.; Saini, S.R. Periodontitis: A Risk for Delivery of Premature Labor and Low-Birth-Weight Infants. J. Nat. Sci. Biol. Med. 2010, 1, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Nannan, M.; Xiaoping, L.; Ying, J. Periodontal Disease in Pregnancy and Adverse Pregnancy Outcomes: Progress in Related Mechanisms and Management Strategies. Front. Med. 2022, 9, 963956. [Google Scholar] [CrossRef]
- Zi, M.Y.H.; Longo, P.L.; Bueno-Silva, B.; Mayer, M.P.A. Mechanisms Involved in the Association between Periodontitis and Complications in Pregnancy. Front. Public Health 2015, 2, 290. [Google Scholar] [CrossRef]
- Van der Weijden, F.A.; Slot, D.E. Efficacy of Homecare Regimens for Mechanical Plaque Removal in Managing Gingivitis a Meta Review. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S77–S91. [Google Scholar] [CrossRef] [PubMed]
- Sälzer, S.; Graetz, C.; Dörfer, C.E.; Slot, D.E.; Van der Weijden, F.A. Contemporary Practices for Mechanical Oral Hygiene to Prevent Periodontal Disease. Periodontol. 2000 2020, 84, 35–44. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Taccardi, D.; Scribante, A. Home Oral Care of Periodontal Patients Using Antimicrobial Gel with Postbiotics, Lactoferrin, and Aloe Barbadensis Leaf Juice Powder vs. Conventional Chlorhexidine Gel: A Split-Mouth Randomized Clinical Trial. Antibiotics 2022, 11, 118. [Google Scholar] [CrossRef] [PubMed]
- Ikawa, T.; Mizutani, K.; Sudo, T.; Kano, C.; Ikeda, Y.; Akizuki, T.; Kobayashi, H.; Izumi, Y.; Iwata, T. Clinical Comparison of an Electric-Powered Ionic Toothbrush and a Manual Toothbrush in Plaque Reduction: A Randomized Clinical Trial. Int. J. Dent. Hyg. 2021, 19, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Ccahuana-Vasquez, R.A.; Adam, R.; Conde, E.; Grender, J.M.; Cunningham, P.; Goyal, C.R.; Qaqish, J. A 5-Week Randomized Clinical Evaluation of a Novel Electric Toothbrush Head with Regular and Tapered Bristles versus a Manual Toothbrush for Reduction of Gingivitis and Plaque. Int. J. Dent. Hyg. 2019, 17, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Mylonopoulou, I.-M.; Pepelassi, E.; Madianos, P.; Halazonetis, D.J. A Randomized, 3-Month, Parallel-Group Clinical Trial to Compare the Efficacy of Electric 3-Dimensional Toothbrushes vs Manual Toothbrushes in Maintaining Oral Health in Patients with Fixed Orthodontic Appliances. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Yaacob, M.; Worthington, H.V.; Deacon, S.A.; Deery, C.; Walmsley, A.D.; Robinson, P.G.; Glenny, A.-M. Powered versus Manual Toothbrushing for Oral Health. Cochrane Database Syst. Rev. 2014, 2014, CD002281. [Google Scholar] [CrossRef]
- Grender, J.; Adam, R.; Zou, Y. The Effects of Oscillating-Rotating Electric Toothbrushes on Plaque and Gingival Health: A Meta-Analysis. Am. J. Dent. 2020, 33, 3–11. [Google Scholar] [PubMed]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef]
- Scheerman, J.F.M.; van Meijel, B.; van Empelen, P.; Verrips, G.H.W.; van Loveren, C.; Twisk, J.W.R.; Pakpour, A.H.; van den Braak, M.C.T.; Kramer, G.J.C. The Effect of Using a Mobile Application (“WhiteTeeth”) on Improving Oral Hygiene: A Randomized Controlled Trial. Int. J. Dent. Hyg. 2020, 18, 73–83. [Google Scholar] [CrossRef]
- The Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030). Available online: https://www.who.int/publications-detail-redirect/A71-19 (accessed on 23 August 2023).
- Enabulele, J.; Ibhawoh, L. Resident Obstetricians’ Awareness of the Oral Health Component in Management of Nausea and Vomiting in Pregnancy. BMC Pregnancy Childbirth 2014, 14, 388. [Google Scholar] [CrossRef]
- Radwan-Oczko, M.; Hirnle, L.; Szczepaniak, M.; Duś-Ilnicka, I. How Much Do Pregnant Women Know about the Importance of Oral Health in Pregnancy? Questionnaire-Based Survey. BMC Pregnancy Childbirth 2023, 23, 348. [Google Scholar] [CrossRef] [PubMed]
- Thomassen, T.M.J.A.; Van der Weijden, F.G.A.; Slot, D.E. The Efficacy of Powered Toothbrushes: A Systematic Review and Network Meta-Analysis. Int. J. Dent. Hyg. 2022, 20, 3–17. [Google Scholar] [CrossRef]
- Ramseier, C.A.; Petitat, C.; Trepp, S.; Lang, N.P.; Eick, S.; Adam, R.; Ccahuana-Vasquez, R.A.; Barker, M.L.; Timm, H.; Klukowska, M.; et al. Clinical Parameters and Oral Fluid Biomarkers in Gingivitis Subjects Using an Electric Toothbrush with Irrigator vs a Manual Toothbrush Alone over 8 Weeks: A Randomised Controlled Clinical Trial. Oral. Health Prev. Dent. 2021, 19, 137–147. [Google Scholar] [CrossRef]
- Grender, J.; Goyal, C.R.; Qaqish, J.; Timm, H.; Adam, R. A 12-Week Randomized Controlled Trial Comparing a Novel Electric Toothbrush With an Extra Gentle Brush Head to a Manual Toothbrush for Plaque and Gingivitis Reduction. Compend. Contin. Educ. Dent. 2022, 43, f20–f29. [Google Scholar] [PubMed]
- Chan, A.-W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 Explanation and Elaboration: Guidance for Protocols of Clinical Trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S173–S182. [Google Scholar] [CrossRef]
- Newbrun, E. Indices to Measure Gingival Bleeding. J. Periodontol. 1996, 67, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Borgnakke, W.S.; Albandar, J.M. 15—Measurement and Distribution of Periodontal Diseases. In Burt and Eklund’s Dentistry, Dental Practice, and the Community, 7th ed.; Mascarenhas, A.K., Okunseri, C., Dye, B.A., Eds.; W.B. Saunders: St. Louis, MO, USA, 2021; pp. 171–188. ISBN 978-0-323-55484-8. [Google Scholar]
- Löe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Rustogi, K.N.; Curtis, J.P.; Volpe, A.R.; Kemp, J.H.; McCool, J.J.; Korn, L.R. Refinement of the Modified Navy Plaque Index to Increase Plaque Scoring Efficiency in Gumline and Interproximal Tooth Areas. J. Clin. Dent. 1992, 3, C9–C12. [Google Scholar]
- Listgarten, M.A. Periodontal Probing: What Does It Mean? J. Clin. Periodontol. 1980, 7, 165–176. [Google Scholar] [CrossRef]


{kind=link}
| Arm | Arm 1 | Arm 2 | Arm 3 | Arm 4 |
|---|---|---|---|---|
| Product name | Diamond Clean 9000 Sonicare | Hydrosonic Easy | Oral-B® 123 | CS 5460 |
| Type of toothbrush | Interactive sonic | Non-interactive sonic | Manual | Manual |
| Bristles hardness | Soft | Ultra-soft | Medium | Ultra-soft |
| Filaments Material, diameter | Nylon, <0.18 mm | Curen®, 0.1 mm | Not available | Curen®, 0.1 mm |
| Manufacturer Name (city, country) | Philips® (Suresnes, France) | Curaden® (Kriens, Switzerland) | Procter & Gamble® (Asnières-sur-Seine, France) | Curaden® (Kriens, Switzerland) |
| Date of Pregnancy Procedures/Visits | Timeline | |||
|---|---|---|---|---|
| T0 | T1 | T2 | T3 | |
| 15–18 Weeks a | +1 Month/T1 | +3 Months/T1 | ||
| Pre-screening | X | |||
| Eligibility screening | X | |||
| Informed consent | X | |||
| Questionnaires | X | X | X | |
| Oral hygiene attitudes and practices b | X | |||
| Oral hygiene attitudes and practices in relation to toothbrushes tested c | X | X | ||
| Acceptability of the toothbrush d | X | X | ||
| Oral examination | X | X | X | |
| Bleeding on probing | X | X | X | |
| Gingival Index | X | X | X | |
| Plaque Index | X | X | X | |
| Probing Pocket Depth | X | X | X | |
| Clinical Attachment Loss | X | X | X | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clément, C.; Bourgeois, D.; Vitiello, F.; Perrier, H.; Tabary, A.; Carrouel, F. Efficacy of Sonic-Powered and Manual Toothbrushes on Plaque-Induced Gingivitis in Pregnant Women: A Randomized Controlled Trial. Methods Protoc. 2023, 6, 99. https://doi.org/10.3390/mps6050099
Clément C, Bourgeois D, Vitiello F, Perrier H, Tabary A, Carrouel F. Efficacy of Sonic-Powered and Manual Toothbrushes on Plaque-Induced Gingivitis in Pregnant Women: A Randomized Controlled Trial. Methods and Protocols. 2023; 6(5):99. https://doi.org/10.3390/mps6050099
Chicago/Turabian StyleClément, Céline, Denis Bourgeois, Flavia Vitiello, Herve Perrier, Ariane Tabary, and Florence Carrouel. 2023. "Efficacy of Sonic-Powered and Manual Toothbrushes on Plaque-Induced Gingivitis in Pregnant Women: A Randomized Controlled Trial" Methods and Protocols 6, no. 5: 99. https://doi.org/10.3390/mps6050099