
Dental Applications of Carbon Nanotubes
by
 , and
, and
Marco A. Castro-Rojas
1, 
Yadira I. Vega-Cantu
1,*,
Geoffrey A. Cordell
2,3 and
Aida Rodriguez-Garcia
1,4,* 1
Tecnologico de Monterrey, Escuela de Ingeniería y Ciencias, Ave. Eugenio Garza Sada 2501, Monterrey 64849, NL, Mexico
2
Natural Products Inc., Evanston, IL 60202, USA
3
Department of Pharmaceutics, College of Pharmacy, University of Florida, Gainesville, FL 32610, USA
4
Universidad Autónoma de Nuevo León, Facultad de Ciencias Biológicas, Instituto de Biotecnología, San Nicolás de los Garza 66455, NL, Mexico
*
Authors to whom correspondence should be addressed.
Molecules 2021, 26(15), 4423; https://doi.org/10.3390/molecules26154423
Submission received: 5 June 2021
/
Revised: 5 July 2021
/
Accepted: 15 July 2021
/
Published: 22 July 2021
(This article belongs to the Special Issue Nanomaterials for Biomedical Application)
Abstract
:Glass ionomer cements and resin-based composites are promising materials in restorative dentistry. However, their limited mechanical properties and the risk of bulk/marginal fracture compromise their lifespan. Intensive research has been conducted to understand and develop new materials that can mimic the functional behavior of the oral cavity. Nanotechnological approaches have emerged to treat oral infections and become a part of scaffolds for tissue regeneration. Carbon nanotubes are promising materials to create multifunctional platforms for dental applications. This review provides a comprehensive survey of and information on the status of this state-of-the-art technology and describes the development of glass ionomers reinforced with carbon nanotubes possessing improved mechanical properties. The applications of carbon nanotubes in drug delivery and tissue engineering for healing infections and lesions of the oral cavity are also described. The review concludes with a summary of the current status and presents a vision of future applications of carbon nanotubes in the practice of dentistry.
1. Introduction
The profound scientific, technological, and engineering impacts of the Fourth Industrial Revolution, also referred to as “Industry 4.0”, are being experienced across many aspects of society [1]. One series of outcomes relates to the dramatic changes occurring in the creation and conduct of research, with significant growth appearing in completely new areas, and the development of innovative research initiatives in underexplored areas to address specific societal and healthcare needs [2]. This ongoing evolutionary process is shifting many facets of human practices into a new era: the era of nanotechnology, the art and science of materials engineering at a scale of less than 100 nm [3]. “Nano” is a prefix derived from the ancient Greek word “nános”, which means “dwarf”. It refers to 1 billionth part of a particular physical size. Therefore, one nanometer represents 1 billionth (1 × 10−9) of a meter [4]. In the past 15 years, research on nanotechnology has revolutionized many diverse medical and dental research outcomes by seeking new strategies and more effective ways to apply the principles of bioengineering, cell-transplantation, and drug delivery to construct biological substitutes to maintain and restore the functions of diseased and compromised tissues [5].
The many applications of nanotechnology have led to significant improvements in healthcare in general medicine and in dentistry in particular. One aspect that has encouraged new advances in dentistry is the development and utilization of innovative nanomaterials in oral health practices [6]. As an example, biomimetic nanotechnology emulates the structure of dental enamel and the surrounding tissues to promote and achieve remineralization. The remineralization process focuses on restoring the amelogenin-based peptides, together with hydroxyapatite, to recover the hardness of the tooth [7]. These improvements in dentistry are represented by the development of a toothpaste comprising nanosized carbonate apatite, which effectively seals dentin tubules, promoting the management of dental sensitivity [8]. The aims of nanotechnology are to analyze structures, understand the physical properties, and create functional constructs through direct action on the existing framework [9]. Similar to nanomedicine, the use of nanotechnology in dentistry, known as “nanodentistry”, promotes the achievement of near-optimum oral health through the use of nanomaterials (including in tissue engineering and drug delivery systems) as integral approaches to dental restorations [10].
The aim of this review is to present relevant aspects regarding the use of nanotechnology in the development of dental restorative materials such as glass ionomer cements (GICs), and to discuss the influence of carbon nanotubes in drug delivery systems and tissue engineering for dental applications currently and in the future.
2. Carbon Nanotubes in Dentistry
Of all the elements in nature, carbon has the unique ability to exist in several different forms and structures, from carbon black to diamonds, with the resulting diverse applications. One of these scaffolds is the formation of nanotubes [11].
2.1. Characteristics of Carbon Nanotubes
Carbon nanotubes (CNTs) comprise a hollow, cylindrical structure of a hexagonal network of carbon atoms, measuring from several nanometers to a few microns. Various forms of this material can be produced using different techniques, including electric arc discharge, laser ablation, catalytic decomposition of hydrocarbons, electrolysis, synthesis from bulk polymers, and low-temperature solid pyrolysis, among others [12]. Carbon atoms in nanotubes are exclusively sp2-hybridized and are arranged in a hexagonal lattice. The resulting material has a high surface area, a small diameter, and high curvature. These characteristics contribute to their many unique properties through van der Walls, π-π stacking, and hydrophobic interactions. CNTs can be modified to increase solubility and modulate the inclusion of functional groups for specific biomedical applications [13].
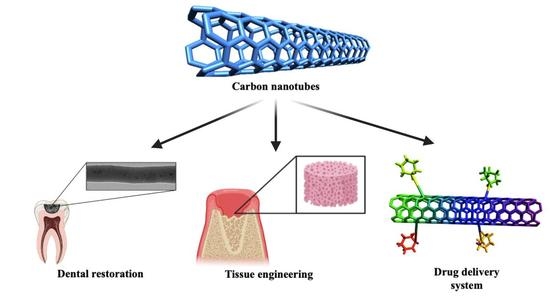
In the past two decades, significant research has examined the development and application of carbon nanotubes in dentistry due to the mechanical (among other) properties that they exhibit. In this aspect, they are excellent candidates to act as a reinforcement for dental materials, for use as scaffolds, and for targeted drug delivery systems [14]. The ability to modulate these properties enhances the utility and the clinical performance of the nanocomposite material.
Despite these positive attributes, there is a limit to the loading of CNTs that can be added as a filler or reinforcement to polymers or other materials. This phenomenon occurs because of the agglomeration of CNTs. This is a major challenge in their use and is usually addressed through chemical functionalization which increases dispersion of CNTs and consequently leads to lower agglomeration. This effectively provides a higher loading capacity for the matrix, with benefits regarding the enhanced mechanical properties of the final composite [15]. Loading optimization for CNTs in the composite matrix is carried out with the aim of maximizing the efficiency of stress transfer to the matrix interface of the CNT. Variables such as interfacial stress transfer, aspect ratio, dispersion, and alignment, as well as the type of synthesis, modulate the effectiveness of the reinforcement [16].
2.2. Single-Wall and Multiple-Wall Carbon Nanotubes
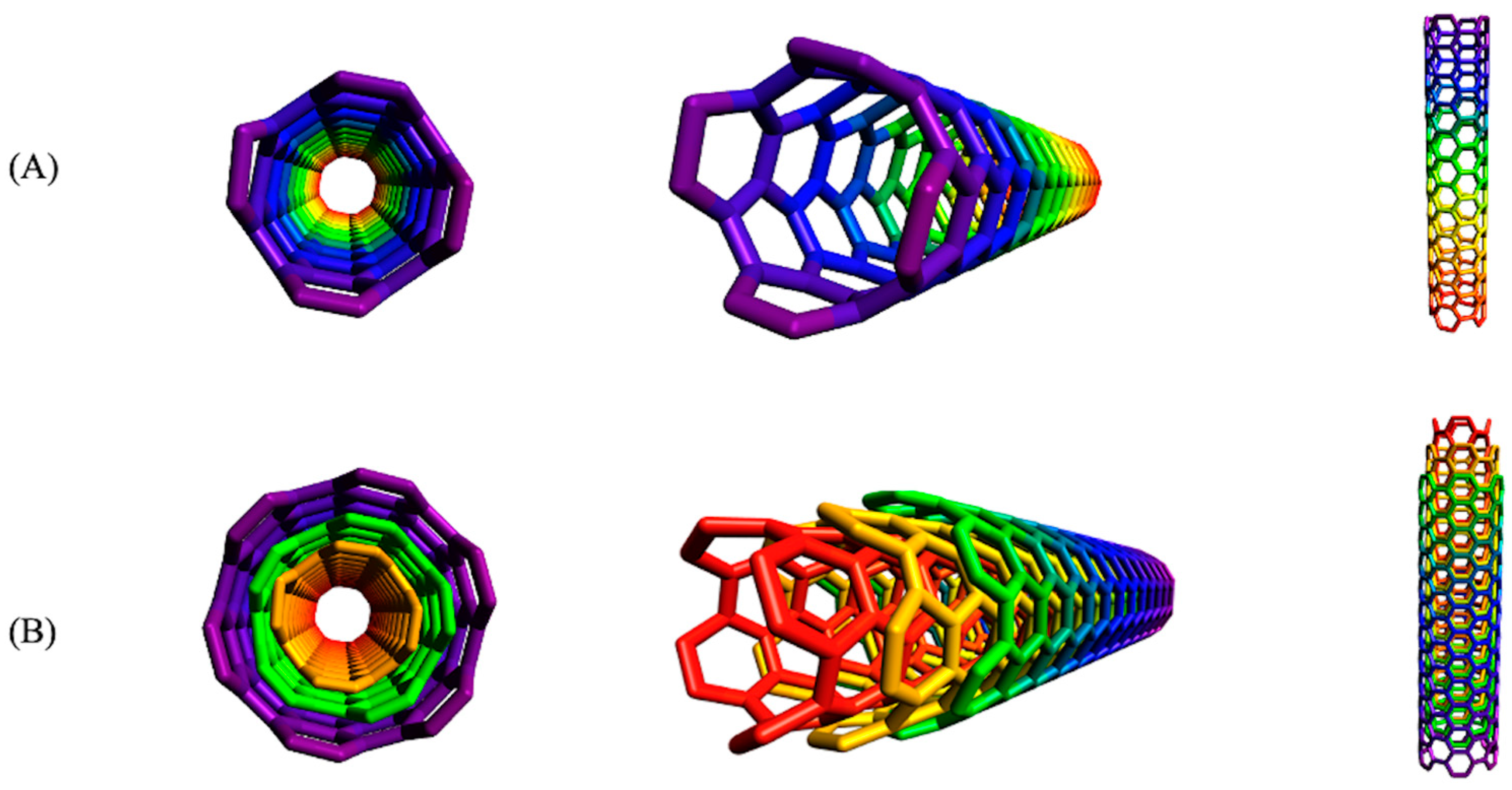
Both single- and multi-walled CNTs are available. Single-walled carbon nanotubes (SWCNTs) have a diameter between 0.4 and 2 nm, while that of multi-walled carbon nanotubes (MWCNTs) can vary between 2 and 100 nm. Lengths can extend to several millimeters long, a characteristic which depends entirely on the method of synthesis [17]. Figure 1 shows the respective arrangements of the carbon atoms in SWCNTs and MWCNTs. The angle of graphene rolling produces carbon nanotubes in three different formats: the achiral chair type (two sides of the hexagon oriented perpendicular to the axis of the CNT), the achiral zigzag type (two sides of the hexagon oriented parallel the axis of the CNT), and the chiral type (any pair of sides of the hexagon oriented at an angle different from 0 or 90° to the axis of the CNT). The different synthetic approaches do not mitigate the prevalent possibility of defects appearing in the nanotubes, such as Stone–Wales defects (90° change in π-π orientation), a pair of 5–7 rings, sp3-hybridized defects, and vacancies (absence of a carbon atom in the six membered rings) [18].
2.3. Applications of Carbon Nanotubes in Dentistry
The specific applications of CNTs and their versatility depend on their individual properties, including morphology, size, and arrangement. In consequence, MWCNTs have emerged as promising candidates for delivery systems due to the high loading capacity provided by their greater surface area and their ability to interact with cellular membranes [19]. Additionally, their excellent mechanical and electrical properties indicate them as good candidates for use as fillers and as osteogenic scaffolds for bone proliferation and bone formation [20]. Indeed, carbon nanotubes used as fillers exhibited good performance in reinforcement at concentrations of 10 vol%, due to the load transfer on the interfacial bonding of the reinforced material and the CNTs [21].
The utilization of endogenous bioactive materials stimulates a diversity of biological interactions and elicits a cascade of responses from the living tissue [22]. To be effective in the oral cavity, a bioactive material must show characteristics which embrace the control of microbial infection, the strengthening of teeth, and have bio-promoting effects. These include control of inflammation, remineralization of teeth, and/or promotion of tissue regeneration [23]. In dentistry, these exogenous materials can be used in permanent restorations, for example as pulp-capping materials, for dentinal tubule occlusion, for scaffolding, and to promote tooth remineralization [24]. One example of bioactivity is the remineralization of initial caries lesions, where the dentin and enamel beneath the restoration can benefit significantly from the promotion of biomineralization, providing adhesion is not compromised [25].
3. Dental Restorative Materials
The lifespan of dental restorations is limited and inherently depends on different factors, including the type of dentition (primary or permanent teeth), size, site, function of the restoration, and the composition of the dental material [26]. With recent scientific advances and an enhanced understanding of the caries process, minimal intervention procedures are performed to maintain the majority of the natural tissue, thereby providing increased life expectancy of the restoration [27].
One of the most important goals in contemporary dentistry is to reduce the failure rate of dental restorations due to bulk/marginal fractures and ameliorate the risk of secondary caries, thereby minimizing the need for a replacement restoration, with the consequent further destruction of tooth tissues [28]. Secondary caries represents one of the main issues leading to the accumulation of biofilm and consequently restoration failure [29]. Some authors claim that the rate of secondary caries in dental restorations may be as high as 50–60% due to the lack of resistance and adhesion of the dental material to tooth tissues, producing microleakage and promoting a high level of deleterious microbial activity [30].
Several materials have been introduced in dentistry as fillers and restorative materials to improve the treatment of both carious and non-carious lesions. With the evolution of dentistry and the emphasis on personal oral care practices, patients have a greater desire to maintain their natural teeth, which leads to an increase in the rate of dental restorations [31]. Restorative dental materials must embrace three fundamental characteristics to deal with tissue failure: (i) adhesion to the tooth tissues, (ii) appropriate mechanical properties, similar to dentin and enamel, and (iii) a wide range of color options [32]. New synthetic materials must overcome the challenge of the continuously moist environment of the oral cavity, and must withstand the effects of masticatory forces, variation of temperature, pH, microbial and enzymatic attacks, and be resistant to color changes from the exogenous materials present in foods (chlorophylls, anthocyanins, carotenoids, synthetic dyes, etc.). Bite forces may vary depending on the tooth location and the particular individual, for which values are in the range of 100 to 500 Newtons [33,34].
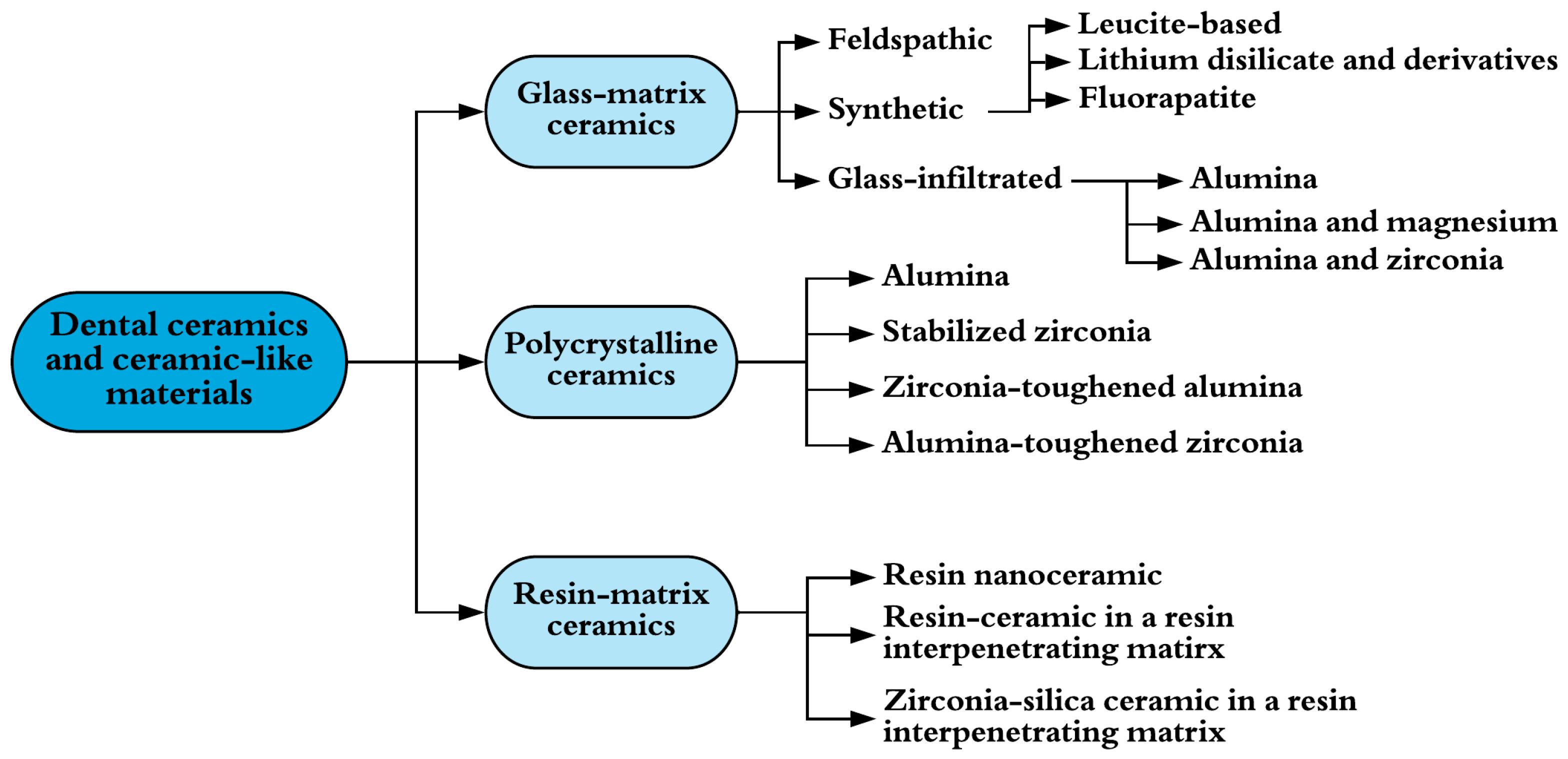
Traditionally, dental amalgam has been used for dental restoration [35]. This material is formed through the reaction of a powdered alloy, composed of silver, tin, and copper, with mercury. The resulting malleable mass is used as a dental restorative. Despite its history of use in the restoration of posterior teeth, this material suffers from several negative characteristics. The most important one is that this material does not adhere to the dental tissues and requires the sacrifice of caries-free tissue to provide the required mechanical retention [36]. Toxicity for humans, the potential for environmental contamination, and esthetic issues have increased concerns with the continued use of this material, leading to research developments for alternative restorative materials [37]. Ceramic materials have found wide use in restorative dentistry and are classified into three groups: glass-matrix ceramics, polycrystalline ceramics, and resin-matrix ceramics (Figure 2), as proposed by Gracis et al. [38].
In addition to these materials, there are several dental restorative materials which employ resin composites. These were developed to replace lost or decayed tooth structure, attending to demands for better esthetic appearance and minimizing the hazards of using mercury in dental amalgams. Although these resin-based composites are widely used for restorations due to their color similarity to natural teeth, and for cavities subjected to low level stress [39,40,41], their use is limited due to issues with mechanical strength, wear resistance, polymerization shrinkage, and color stability. The main benefit in comparison with other materials is the cost of the preparation, which makes them more affordable for patients [42].
3.1. Characteristics of Glass Ionomer Cements
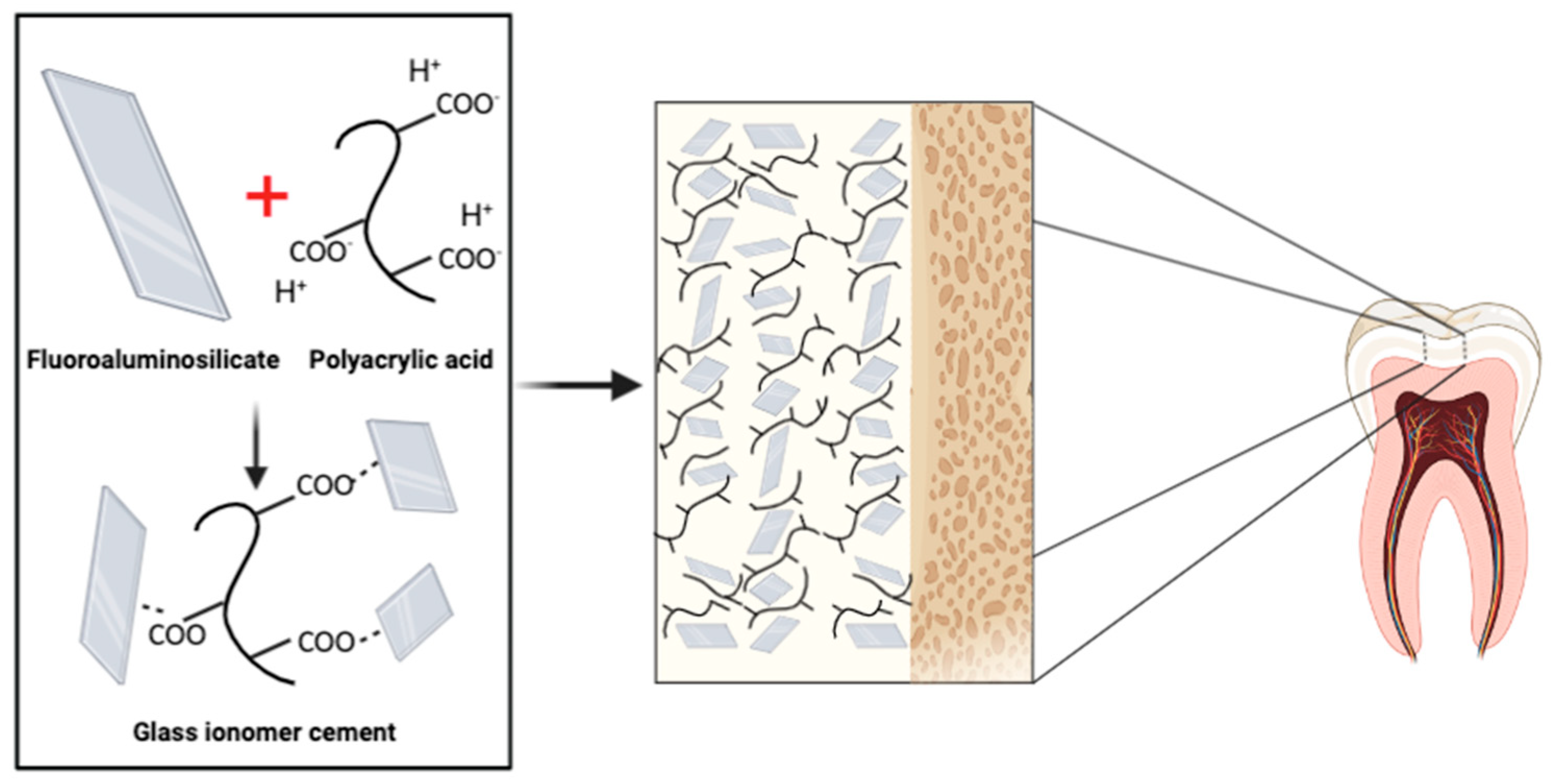
Glass ionomer cements (GICs) are dental materials that display attractive properties for use as restorative and luting materials. They were introduced in 1972 by Wilson and Kent as a “new translucent dental filling material” and consist of three basic components: a polymeric water-soluble acid, a basic (ion-leachable) glass, and water [14]. This type of material produces different properties from a powdered fluoroaminosilicate, such as strength, rigidity, and fluoride release. It also takes advantage of the biocompatibility and adhesive characteristics of the polyalkenoic acid component [38,42]. Glass ionomer cements can be classified as shown in Table 1.
Glass ionomer cements (GICs) are formed as the result of an acid–base reaction. The acid attacks and degrades the alumina-silicate glass, releasing cations of calcium and aluminum. Chelation of cations occurs between the carboxylate groups and the polyalkenoic acid chains form a cross-linked structure (Figure 3) [14].
The mechanical resistance of the GIC material is a key factor to provide good performance of restoration for the patient. This requires consideration of the composition and mechanical properties of the natural tooth since enamel and dentin have different mechanical properties (Table 2). It was reported that the coefficient of thermal expansion of GICs is similar to that of human dentin, thereby reducing the possibility of marginal leakage and restoration failure [50].
3.2. Benefits and Applications of Glass Ionomers in Dental Restorations
Currently, GICs are widely used in several dental applications, including full dental restorations, fissure sealants, luting agents, liners, and bases, and as endodontic sealers due their unique properties in comparison with other conventional materials [52]. These properties include chemical adhesion to enamel and dentin in the presence of wetness, high biocompatibility, resistance to microleakage, favorable thermal expansion and contraction, good marginal integrity, fluoride release, and stability at high humidity [53].
The need for replacement restorations typically arises due to the development of secondary caries at the interface of a restoration and tooth tissue. Bacteria present in the human oral micro-environment, including Streptococcus mutans, Actinomyces spp., and Lactobacillus spp., are the main microorganisms responsible for development of dental biofilm [14]. In addition, inherent surface unevenness of glass ionomers increases the surface area and provides niches for biofilm formation. GICs are considered to be cariostatic and antibacterial materials due to fluoride release [28] and their strong bonding to tooth tissues. However, the physical properties of these materials limit their use for posterior tooth restoration [54]. An interesting strategy would be to develop dental materials with selective antimicrobial activity for dominant oral pathogens through the incorporation of nano-delivered natural compounds derived from plants or microorganisms. This could be especially impactful for the creation of novel restorative materials.
3.3. Major Drawbacks of Using Glass Ionomers
Even though the glass ionomer cements possess many attractive characteristics, they present significant disadvantages in practice, including poor hydrolytic stability, low flexural strength, poor fracture toughness, and limited durability [55]. In addition, there are clinical limitations, including prolonged setting reaction time, dehydration, and the rough texture, which can reduce the final mechanical properties of the restoration after setting [56]. To overcome these clinical constraints and provide enhanced performance for the patient, further improvements are required, particularly to enhance mechanical strength. The use of resin-modified GICs has been proposed as one approach to correct partially the composition issue, to enhance the physical properties of the material, and to reduce fluoride ion release. When this release does occur, mineralization of the tissue is reduced, and the probability of restoration failure is higher [57].
3.4. Nanotechnology in Glass Ionomers
Research for new materials with improved clinical performance has been continuous and has led to achievements of nanotechnology in dental material manufacturing. These new materials are established as “nanobiomaterials” and exhibit enhanced properties and efficiency in comparison with formative bulk materials [58]. To overcome mechanical and biological constraints of GICs, several nanomaterials, including hydroxyapatite, silica, zirconia, graphene, and silver nanoparticles, have been incorporated into GICs. Introduction of nanohydroxyapatite and silica into GICs resulted in improvements in mechanical properties (hardness and compressive and flexural strength) and maintained a sustained fluoride release [59]. When alumina/zirconia and hydroxyapatite were added to the GIC, antibacterial activity and biocompatibility were increased [60]. Among various nanomaterials, graphene has been used to reduce biofilm formation and to increase the wear resistance of dental composites [11].
The influence of multi-walled carbon nanotubes (MWCNTs) in reinforced glass ionomer cements with respect to their chemical, thermal, and mechanical properties for specific use as a posterior restorative material was examined by Goyal et al. [61]. Concentrations of 0%, 1%, and 2% w/w of MWCNTs were added as a reinforcement agent, obtaining a dark-colored material, which limits its application only to posterior teeth. An enhancement of mechanical properties of the material was reported as a hardness increase from 2.19 MPa to 5.70 MPa with the addition of 2% w/w of MWCNTs. This particular composition also tolerated higher wear forces better than the other two compositions [61].
The esthetic appearance of restorative materials is very important for all patients and is why GICs are widely used in the restoration of primary teeth. Color stability tests must therefore be conducted on new materials to determine if they will meet the requirements of the individual patient. The incorporation of carbon nanotubes into glass ionomer cements has led to enhanced color stability profiles compared with other reinforcement materials such as silver nanoparticles [62]. Based on these considerations of color stability this material can be used effectively in posterior restorations, especially for primary teeth where esthetic requirements and color stability are less clinically significant [63].
4. Carbon Nanotubes in Guided Bone Regeneration (GBR)
Currently evolving targets are shifting towards the development of biofunctional materials which prevent disease and/or actively promote tissue regeneration. In the instance of a bone defect, guided bone regeneration (GBR) is now a widely used technique which deploys an occlusive membrane to seal the area of the bone defect to physically prevent the incursion of non-osteogenic cells into defects [64]. This artificial barrier also serves as a scaffold which fosters osteogenic cells to stimulate bone formation at a higher rate than the surrounding connective tissue and prevents infection when used in dental implants. Requirements for an ideal material used in GBR include: (i) biodegradability; (ii) biocompatibility to promote integration with the tissue and avoid inflammatory responses; (iii) mechanical strength; and (iv) porosity to be partially occlusive to avoid epithelial cell flow and fibroblast of the soft tissue, and allow the diffusion of oxygen, nutrients, and bioactive substances [65].
Innovation of artificial scaffold materials to sustain bone cell proliferation and growth, and to enhance incrementally or replace bone tissue, is a primary goal in bone bioengineering [66]. In support of this biological and clinical outcome, CNTs have been explored for the stimulation of bone regeneration and to provide an alternative permanent mechanical function. It was observed that neutrally charged CNTs have the ability to sustain both osteoblast proliferation and bone forming functions, and they showed promising biocompatibility with osteoblast cells [67].
Research studying the effects of the surface functionalization of CNTs in nanocomposites for dental implants, such as hydroxyapatite, zirconia, and titanium, has fostered a greater understanding of the chemical groups that can promote osteoblast proliferation [68]. In addition, carbon nanotubes combined with hydroxyapatite demonstrated cytocompatibility, with more than 200% cell viability and compressive strength in the range of 13 to 29 MPa. This combination is considered an attractive bone-filling material [69].
4.1. Mechanical Properties of Nanofiber Polymeric Membranes Reinforced with Carbon Nanotubes
Microcracks in bone are the natural response of the tissue to excessive applied mechanical loads. With the introduction of carbon nanotubes as scaffolds the reinforced bone tissue is more resistant to the development and growth of fissures due to better load distribution, dispersal of the crack growth, and a decrease in the stress intensity near the fissure tip [70]. The addition of different functional groups, including amino, phosphate, and carboxylic acid moieties, can dramatically change the physical, mechanical, and biological properties of CNTs with respect to bone growth. This functionalization will depend entirely on the specific needs of the load (drugs, antigens, genes, etc.). Functionalization also assists in CNT biodegradability through the introduction of structural defects which leads to the improved intrusion of oxidative enzymes to enhance the degradation of CNTs [71]. Interaction of carbon nanotubes with tissue environment is modulated by tailoring the functional groups at the surface, as this determines the charge density and the overall net polarity. The result is that a charged surface obtained through chemical modification may be more hydrophilic, in contrast to the initial, electrically neutral surface [68].
The use of CNTs as fillers in the reinforcement of scaffold materials is affected by four parameters: (i) their extent of dispersion in the matrix, (ii) their aspect ratio, (iii) their alignment, and (iv) the interfacial stress transfer. Their distribution allows the material to have a uniform performance and higher superficial area, while the alignment of the nanotubes is reflected in their improved mechanical strength, and stress transfer allows the matrix to carry higher loads without cracking [16]. Maximization of the load transfer is achieved by incrementing towards a larger aspect ratio. Measurement of these improvements is possible using microindentation, which consists of applying a specific force using a diamond indenter to measure the declinations of enamel rods and dental tubules [72]. The interaction between the polymer and the CNT is particularly important in order to transfer the external stress forces to the CNTs, thereby enabling the matrix to bear higher loads [73].
In addition to this application, the use of these materials for dentin surface modification showed selective coating of the surface of the dentin and cementum by adhering to the collagen fibers exposed from these surfaces [74]. Hahn et al. reported the ability of carbon nanotubes to improve mechanical properties, such as hardness and elastic modulus, when CNTs are added to a hydroxyapatite coating, resulting in an adhesion strength ranging from 27.3 to 29.0 MPa [75]. Similarly, Marrs et al. studied the application of CNTs for the reinforcement of a bone cement based on polymethylmethacrylate (PMMA). The result was an enhancement in mechanical properties with peaks of performance observed with concentrations of 2% wt. The product showed a flexural strength of 90.6 MPa and a bending modulus of 3528 MPa [76]. Bonding, esthetic, mechanical, and physical properties of restorative dental materials have been greatly improved. Although these materials show excellent clinical response, investigations to achieve performance similar to the attributes of natural teeth continue as an ongoing process [77].
Scaffolds for bone tissue engineering applications containing polycaprolactone (PCL) have been widely used. PCL is a hydrophobic semicrystalline polymer whose crystallinity decreases with the increment of molecular weight. This material has good solubility and a low melting point (59–64 °C) [78]. It is a biodegradable and bioactive material and has been considered as a possible substitute for bone tissue due to its unique properties. However, the application of PCL for this purpose is limited by its weak mechanical properties. This disadvantage can be addressed through the production of polymeric nanofiber composites formed through electrospinning processes [79]. The resulting polymer is easily synthesized and processed and can be molded precisely into diverse shapes which are easily modified due to the viscoelastic properties and the low melting temperature. A clinically important characteristic of modified and electrospun PCL is that it can be functionalized with active molecules such as drugs or bone growth stimulating factors [80]. Previous studies have also shown that PCL reinforced with CNTs exhibited improved physicochemical, biological, and mechanical properties, for example through the increment in elastic modulus and tensile stress as well as conductivity, while they did not exhibit cytotoxicity [70,71].
4.2. Effect of Carbon Nanotubes on Cells
The cytotoxicity of CNTs has been widely studied. It was demonstrated that the cytotoxicity of CNTs depends on the relationship with length, diameter, and the presence of functional groups. To mitigate toxicity, many efforts have been made to modify the surface properties of CNTs. For instance, Ketabi et al. studied the reinforcement of nanofibers of polycaprolactone with multiple-wall carbon nanotubes for odontoblast cell interactions [81]. In the same way, Flores-Cedillo et al. reinforced polycaprolactone with MWCNTs for use as scaffolds in bone tissue regeneration, thereby developing materials with improved physicochemical, biological, and mechanical properties, such as increased elastic modulus and tensile stress, as well as conductivity. While they did not exhibit cytotoxicity, it was concluded that the application of an electric field to the carbon nanotubes does not promote alignment or dispersion [42].
The diameter of carbon nanotubes provides them the capacity to inactivate bacteria such as E. coli. Direct contact of the bacteria with the material causes cell membrane damage and subsequently cell death. Differences in toxicity lie in the diameter of the tube and the surface area available for interaction. Kang et al. demonstrated that single-wall CNTs were more toxic for bacteria than multi-walled CNTs through oxidative stress. To quantify the molecular response of the bacteria with the CNT gene expression, DNA microarray analyses were performed [82].
A recent study investigated the influence of coating biopolymer nanofibers with CNTs on cells [83]. It was demonstrated that these scaffolds could modulate different interactions of the cells and tissues that allow bone healing and regeneration, reduce inflammatory signals, and promote angiogenesis. The in vitro study demonstrated accelerated adhesion and osteogenic differentiation, while the in vivo results showed an increase of bone forming cells with higher bone mineral density, confirming the potential use in bone regeneration and healing processes [83].
4.3. Preparation of Polymeric Membranes Reinforced with Carbon Nanotubes
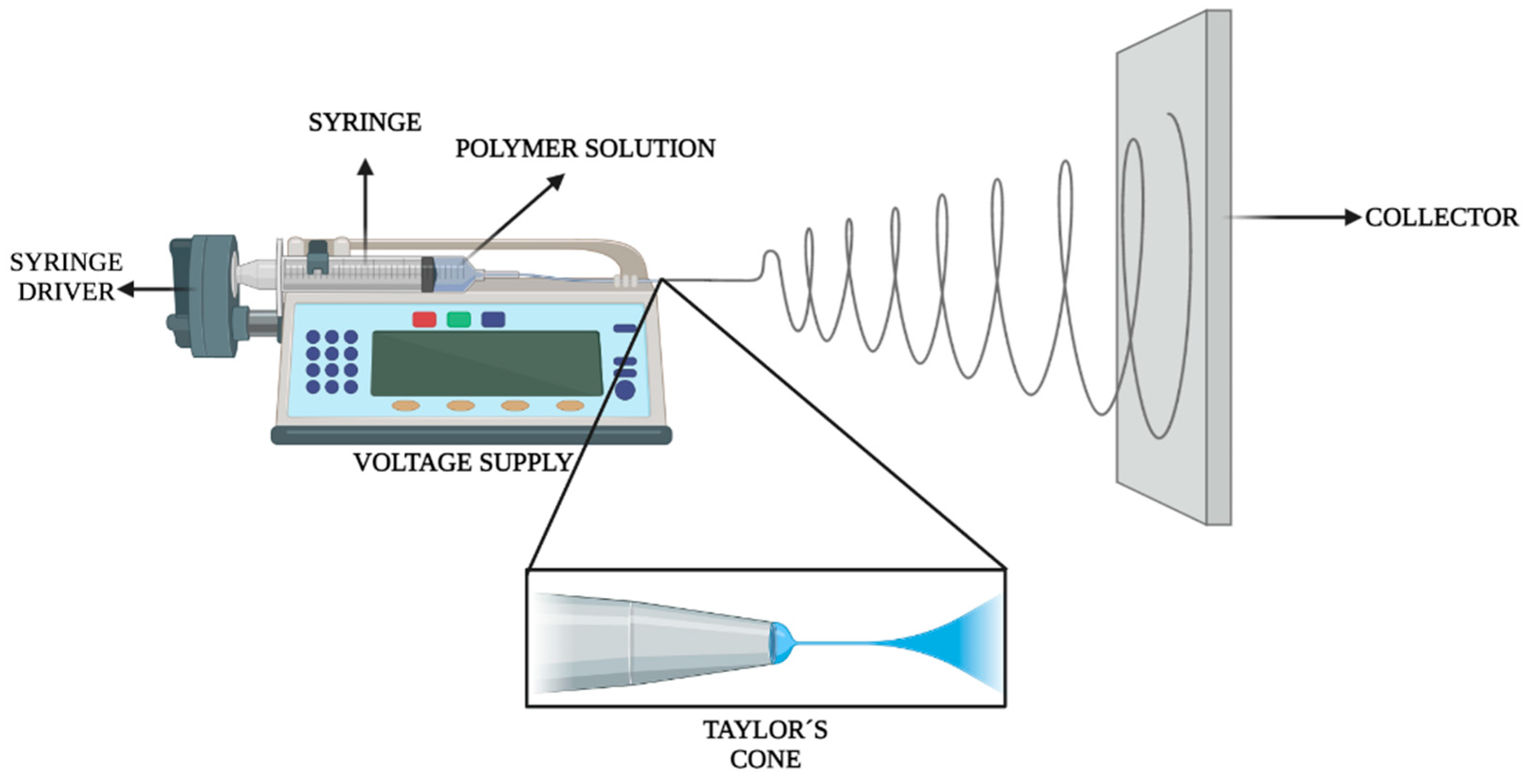
The most common method to prepare polymeric membranes is through electrospinning, a process which was introduced in the 1930s to produce polymeric fibers from several nanometers to a few micrometers [84]. Electrospinning, as illustrated in Figure 4, is based on the dispersion of a polymer in an appropriate solvent, which is then introduced into a glass syringe. The polymeric solution is pumped through the syringe to which is applied a high voltage (25 kV, positive pole), while the collector acts as the negative pole. Due to the voltage difference that exists between the tip of the needle and the collector, the polymeric material becomes stretched thereby forming a Taylor´s cone, which provides polymeric fibers ranging from 30 nm to 1 μm in diameter [85]. The resulting membranes can be used for many different applications, including fine filtration, scaffolds for tissue engineering, and drug delivery systems.
The synthesis and characterization of nylon-6 fibers using electrospinning, with and without the reinforcement of carbon nanotubes, demonstrated the significant influence of CNTs and how the concentration of CNTs (2.5, 5.0, 10.0, and 20.0%) affected mechanical properties such as flexural strength, volumetric polymerization shrinkage, and elastic modulus, with the best values obtained for concentrations of 2.5 and 5.0% of CNTs. The highest value for flexural strength was reported as 106.0 MPa for a 5% concentration with an elastic modulus of 201.0 MPa [86]. Polystyrene/MWCNT nano fibers showed an increase in Young’s modulus of 22% compared with untreated polystyrene [87]. The preparation of nanofibers of polyurethane/MWCNTs showed an enhancement in the tensile strength compared with the bulk material [80]. Strength of polymeric nanofibers prepared through electrospinning is due to the differently adopted conformations of the polymer chains and the microstructure and is enhanced through interfacial linking forces between matrix and nanofillers, mainly due to the specific surface area of the nanofibers [88].
5. Carbon Nanotubes in Drug Delivery Systems
Modifications in drug delivery systems have a profound effect on the bioavailability and pharmacokinetics of medicinal agents and represent a widely researched area of drug development. Currently, studies are taking advantage of the special properties of carbon nanotubes. Major improvements in targeted drug delivery systems include a reduction in drug dosage, retiming of drug distribution to obtain the same results, and reducing the side effects from the current delivery methods [89]. Carbon nanotubes provide an opportunity to introduce a high loading capacity and the ability to be easily taken up by the cells. It has been stated that a carbon nanotube with a diameter of 80 nm can accommodate approximately 5 million drug molecules, thereby by serving as a nanocontainer [90].
Although there are many available delivery systems their success is limited due to low protein loading, size control, and toxicity; carbon nanotubes are studied for use in biological systems based on their ability to penetrate cell membranes, their sustained capacity, and their distribution within cells [19]. MWCNTs have the capacity for high protein loading and stability under biological conditions [19].
The commonly suggested mechanism of interaction between carbon nanotubes and cellular membranes is through receptor-mediated endocytosis. The uptake mechanism arises from surface interactions of the media with the carbon nanotubes, an interaction regarded as the most important for cell internalization [91].
6. Conclusions and Future Applications
This review demonstrates the highly successful impact of carbon nanotubes in dentistry. The continuous development of new materials for oral applications, including for functional dental restorations, demands the provision of new composites with enhanced physical, chemical, and mechanical properties to deal with the clinical needs prevalent in the oral cavity. Furthermore, dental composites are expected to exhibit a wide range of desired characteristics, including biocompatibility, adhesion to tooth tissues, and color stability, as well as the delivery of biological agents for prevention and treatment.
Because the physicochemical and mechanical properties of carbon nanotubes are tunable, it is anticipated that their incorporation into dental materials will increase their use in dentistry, leading to new and more effective functional applications. These potential advancements could lead to the development of new materials for caries prevention with the use of functionalized carbon nanotubes as drug delivery systems, as well as biomimetic scaffolds that imitate the extracellular matrix for tissue engineering. In addition, carbon nanotubes hold great potential for the development of dental materials with interesting properties, including bioactivity, as a delivery system for agents with antimicrobial and tissue-regenerative properties. Undoubtedly, they will provide innovative platforms for a wide range of future studies which will improve oral care.
Author Contributions
Conceptualization, A.R.-G.; methodology, A.R.-G.; software, M.A.C.-R.; writing—original draft preparation, M.A.C.-R., G.A.C. and A.R.-G.; writing—review and editing, G.A.C. and A.R.-G.; supervision, A.R.-G.; project administration, A.R.-G.; funding acquisition, Y.I.V.-C. All authors have read and agreed to the published version of the manuscript.
Funding
The authors would like to acknowledge the financial support of Universidad Autónoma de Nuevo León, Grant No. SA1550-21. Additional support for funding and publishing in an open access journal was provided by Tecnológico de Monterrey. This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The Graphical Abstract and each of the Figures were created by M.A.C.-R. using BioRender software through a licensed subscription.
Conflicts of Interest
The authors declare no real or perceived conflict of interest.
References
- Morrar, R.; Arman, H.; Mousa, S. The Fourth Industrial Revolution (Industry 4.0): A social innovation perspective. Technol. Innov. Manag. Rev. 2017, 7, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Maynard, A.D. Navigating the Fourth Industrial Revolution. Nat. Nanotechnol. 2015, 10, 1005–1006. [Google Scholar] [CrossRef]
- AlKahtani, R.N. The implications and applications of nanotechnology in dentistry: A review. Saudi Dent. J. 2018, 30, 107–116. [Google Scholar] [CrossRef]
- Schleyer, T.L. Nanodentistry. Fact or fiction? J. Am. Dent. Assoc. 2000, 131, 1567–1568. [Google Scholar] [CrossRef]
- Kanaparthy, R.; Kanaparthy, A. The changing face of dentistry: Nanotechnology. Int. J. Nanomed. 2011, 6, 2799–2804. [Google Scholar] [CrossRef] [Green Version]
- Mok, Z.H.; Proctor, G.; Thanou, M. Emerging nanomaterials for dental treatments. Emerg. Top. Life Sci. 2021, 4, 613–625. [Google Scholar] [CrossRef]
- Ge, J.; Cui, F.Z.; Wang, X.M.; Feng, H.L. Property variations in the prism and the organic sheath within enamel by nanoindentation. Biomaterials 2005, 26, 3333–3339. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kwon, H.K.; Kim, B.I. Effect of dentinal tubule occlusion by dentifrice containing nano-carbonate apatite. J. Oral Rehabil. 2008, 35, 847–853. [Google Scholar] [CrossRef]
- Ozak, S.T.; Ozkan, P. Nanotechnology and dentistry. Eur. J. Dent. 2013, 7, 145–151. [Google Scholar] [CrossRef]
- Freitas, R.A. Molecular robots and other high-tech possibilities. J. Am. Dent. Assoc. 2000, 131, 1559–1565. [Google Scholar] [CrossRef]
- Hirsch, A. The era of carbon allotropes. Nat. Mater. 2010, 9, 868–871. [Google Scholar] [CrossRef]
- Journet, C.; Bernard, C.; Lyon, U.; Bernier, P. Production of carbon nanotubes. Artic. Appl. Phys. A 1998. [Google Scholar] [CrossRef]
- Gao, Z.; Varela, J.A.; Groc, L.; Lounis, B.; Cognet, L. Toward the suppression of cellular toxicity from single-walled carbon nanotubes. Biomater. Sci. 2016, 4, 230–244. [Google Scholar] [CrossRef] [Green Version]
- Kleverlaan, C.J.; Van Duinen, R.N.B.; Feilzer, A.J. Mechanical properties of glass ionomer cements affected by curing methods. Dent. Mater. 2004, 20, 45–50. [Google Scholar] [CrossRef]
- Bonilla-Represa, V.; Abalos-Labruzzi, C.; Herrera-Martinez, M.; Guerrero-Pérez, M.O. Nanomaterials in dentistry: State of the art and future challenges. Nanomaterials 2020, 10, 1770. [Google Scholar] [CrossRef]
- Coleman, J.N.; Khan, U.; Gun’ko, Y.K. Mechanical reinforcement of polymers using carbon nanotubes. Adv. Mater. 2006, 18, 689–706. [Google Scholar] [CrossRef]
- Bekyarova, E.; Ni, Y.; Malarkey, E.B.; Montana, V.; McWilliams, J.L.; Haddon, R.C.; Parpura, V. Applications of carbon nanotubes in biotechnology and biomedicine. J. Biomed. Nanotechnol. 2006, 1, 3–17. [Google Scholar] [CrossRef] [Green Version]
- Maniecki, T.; Shtyka, O.; Mierczynski, P.; Ciesielski, R.; Czylkowska, A.; Leyko, J.; Mitukiewicz, G.; Dubkov, S.; Gromov, D. Carbon nanotubes: Properties, synthesis, and application. Fibre Chem. 2018, 50, 297–300. [Google Scholar] [CrossRef]
- Kechagioglou, P.; Andriotis, E.; Papagerakis, P.; Papagerakis, S. Multiwalled carbon nanotubes for dental applications. In Methods in Molecular Biology; Humana Press Inc.: Totowa, NJ, USA, 2019; Volume 1922, pp. 121–128. [Google Scholar]
- McIntyre, R.A. Common nano-materials and their use in real world applications. Sci. Prog. 2012, 95, 1–22. [Google Scholar] [CrossRef]
- Andrews, R.; Weisenberger, M.C. Carbon nanotube polymer composites. Curr. Opin. Solid State Mater. Sci. 2004, 8, 31–37. [Google Scholar] [CrossRef]
- Garchitorena, M.I.; Garchitorena, M.I. Vidrios bioactivos en odontología restauradora. Odontoestomatologia 2019, 21, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Imazato, S.; Kohno, T.; Tsuboi, R.; Thongthai, P.; Xu, H.H.K.; Kitagawa, H. Cutting-edge filler technologies to release bio-active components for restorative and preventive dentistry. Dent. Mater. J. 2020, 39, 69–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernando, D.; Attik, N.; Pradelle-Plasse, N.; Jackson, P.; Grosgogeat, B.; Colon, P. Bioactive glass for dentin remineralization: A systematic review. Mater. Sci. Eng. C 2017, 76, 1369–1377. [Google Scholar] [CrossRef]
- Vallittu, P.K.; Boccaccini, A.R.; Hupa, L.; Watts, D.C. Bioactive dental materials—Do they exist and what does bioactivity mean? Dent. Mater. 2018, 34, 693–694. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, B.; Treasure, E.; Dummer, P.; Dunstan, F.; Gilmour, A.; Jones, R.; Phillips, C.; Stevens, J.; Rees, J.; Richmond, S. Challenges with studies investigating longevity of dental restorations—A critique of a systematic review. J. Dent. 2001, 29, 155–161. [Google Scholar] [CrossRef]
- Tyas, M.J.; Anusavice, K.J.; Frencken, J.E.; Mount, G.J. Minimal intervention dentistry—A review: FDI Commission Project 1-97. Int. Dent. J. 2000, 50, 1–12. [Google Scholar] [CrossRef]
- Xie, D.; Weng, Y.; Guo, X.; Zhao, J.; Gregory, R.L.; Zheng, C. Preparation and evaluation of a novel glass-ionomer cement with antibacterial functions. Dent. Mater. 2011, 27, 487–496. [Google Scholar] [CrossRef]
- Poole, S.F.; Pitondo-Silva, A.; Oliveira-Silva, M.; Moris, I.C.M.; Gomes, E.A. Influence of different ceramic materials and surface treatments on the adhesion of Prevotella intermedia. J. Mech. Behav. Biomed. Mater. 2020, 111, 104010. [Google Scholar] [CrossRef]
- Fan, C.; Chu, L.; Rawls, H.R.; Norling, B.K.; Cardenas, H.L.; Whang, K. Development of an antimicrobial resin-a pilot study. Dent. Mater. 2011, 27, 322–328. [Google Scholar] [CrossRef]
- Matis, B.A.; Cochran, M.J.; Carlson, T.J.; Guba, C.; Eckert, G.J. A three-year clinical evaluation of two dentin bonding agents. J. Am. Dent. Assoc. 2004, 135, 451–457. [Google Scholar] [CrossRef]
- Rekow, E.D.; Bayne, S.C.; Carvalho, R.M.; Steele, J.G. What constitutes an ideal dental restorative material? Adv. Dent. Res. 2013, 25, 18–23. [Google Scholar] [CrossRef]
- Raadsheer, M.C.; Van Eijden, T.M.G.J.; Van Ginkel, F.C.; Prahl-Andersen, B. Contribution of jaw muscle size and craniofacial morphology to human bite force magnitude. J. Dent. Res. 1999, 78, 31–42. [Google Scholar] [CrossRef]
- Khan, A.S.; Khan, M.; Rehman, I.U. Nanoparticles, properties, and applications in glass ionomer cements. In Nanobiomaterials in Clinical Dentistry; Elsevier Inc.: Amsterdam, The Netherlands, 2012; pp. 93–108. ISBN 9781455731275. [Google Scholar]
- Ramesh, B.; Kulvinder, K.W.; Aseem, P.; Anil, C. Dental amalgam: An update. Compend. Contin. Educ. Dent. 2010, 13, 204–208. [Google Scholar] [CrossRef]
- Lynch, C.D.; Frazier, K.B.; McConnell, R.J.; Blum, I.R.; Wilson, N.H.F. State-of-the-art techniques in operative dentistry: Contemporary teaching of posterior composites in UK and Irish dental schools. Br. Dent. J. 2010, 3, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Fleming, G.J.; Burke, F.J.; Watson, D.J.; Owen, F.J. Materials for restoration of primary teeth: I. Conventional materials and early glass ionomers. Dent. Update 2001, 28, 486–491. [Google Scholar] [CrossRef]
- Gracis, S.; Thompson, V.; Ferencz, J.; Silva, N.; Bonfante, E. A new classification system for all-ceramic and ceramic-like restorative materials. Int. J. Prosthodont. 2015, 28, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Marghalani, H.Y. Resin-based dental composite materials. In Handbook of Bioceramics and Biocomposites; Springer International Publishing: Berlin, Germany, 2016; pp. 357–405. [Google Scholar] [CrossRef]
- Gallo, M.; Abouelleil, H.; Chenal, J.M.; Adrien, J.; Lachambre, J.; Colon, P.; Maire, E. Polymerization shrinkage of resin-based composites for dental restorations: A digital volume correlation study. Dent. Mater. 2019, 35, 1654–1664. [Google Scholar] [CrossRef]
- Opdam, N.J.M.; Van De Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.D.N.J.M.; Van Dijken, J.W. Longevity of posterior composite restorations: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef]
- Flores-Cedillo, M.L.; Alvarado-Estrada, K.N.; Pozos-Guillén, A.J.; Murguía-Ibarra, J.S.; Vidal, M.A.; Cervantes-Uc, J.M.; Rosales-Ibáñez, R.; Cauich-Rodríguez, J.V. Multiwall carbon nanotubes/polycaprolactone scaffolds seeded with human dental pulp stem cells for bone tissue regeneration. J. Mater. Sci. Mater. Med. 2016, 27, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Browning, W.D. The benefits of glass ionomer self-adhesive materials in restorative dentistry. Compend. Contin. Educ. Dent. 2006, 27, 308–314. [Google Scholar]
- Croll, T.P.; Nicholson, J.W. Glass ionomer cements in pediatric dentistry: Review of the literature. Pediatric Dent. 2002, 24, 423–429. [Google Scholar]
- Zhao, J.; Xie, D. A novel hyperbranched poly(acrylic acid) for improved resin-modified glass-ionomer restoratives. Dent. Mater. 2011, 27, 478–486. [Google Scholar] [CrossRef]
- Tarasingh, P.; Sharada Reddy, J.; Suhasini, K.; Hemachandrika, I. Comparative evaluation of antimicrobial efficacy of resin-modified glass ionomers, compomers and giomers—An in vitro study. J. Clin. Diagn. Res. 2015, 9, ZC85–ZC87. [Google Scholar] [CrossRef]
- Williams, J.A.; Billington, R.W.; Pearson, G.J. The comparative strengths of commercial glass-ionomer cements with and without metal additions. Br. Dent. J. 1992, 172, 279–282. [Google Scholar] [CrossRef]
- Yap, A.U.J.; Pek, Y.S.; Cheang, P. Physico-mechanical properties of a fast-set highly viscous GIC restorative. J. Oral Rehabil. 2003, 30, 1–8. [Google Scholar] [CrossRef]
- Gautam, C.; Joyner, J.; Gautam, A.; Rao, J.; Vajtai, R. Zirconia based dental ceramics: Structure, mechanical properties, biocompatibility and applications. Dalton Trans. 2016, 45, 19194–19215. [Google Scholar] [CrossRef]
- Zhang, Y.-R.; Du, W.; Zhou, X.-D.; Yu, H.-Y. Review of research on the mechanical properties of the human tooth. Int. J. Oral Sci. 2014, 6, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholson, J.W.; Sidhu, S.K.; Czarnecka, B. Enhancing the Mechanical Properties of Glass-Ionomer Dental Cements: A Review. Materials 2020, 13, 2510. [Google Scholar] [CrossRef] [PubMed]
- Tüzüner, T.; Dimkov, A.; Nicholson, J.W. The effect of antimicrobial additives on the properties of dental glass-ionomer cements: A review. Acta Biomater. Odontol. Scand. 2019, 5, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garoushi, S.; Vallittu, P.; Lassila, L. Hollow glass fibers in reinforcing glass ionomer cements. Dent. Mater. 2017, 33, e86–e93. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, S.K. Glass-ionomer cement restorative materials: A sticky subject? Aust. Dent. J. 2011, 56, 23–30. [Google Scholar] [CrossRef]
- Baig, M.S.; Fleming, G.J.P. Conventional glass-ionomer materials: A review of the developments in glass powder, polyacid liquid and the strategies of reinforcement. J. Dent. 2015, 43, 897–912. [Google Scholar] [CrossRef]
- Knight, G.M. The benefits and limitations of glass-ionomer cements and their use in contemporary dentistry. In Glass-Ionomers in Dentistry; Springer: Cham, Switzerland, 2016; pp. 57–79. ISBN 978-3-319-22625-5. [Google Scholar]
- Sidhu, S.K.; Watson, T.F. Resin-modified glass-ionomer materials. Part 1: Properties. Dent. Update 1995, 22, 429–432. [Google Scholar] [PubMed]
- Kerezoudi, C.; Samanidou, V.F.; Palaghias, G. Nanobiomaterials in restorative dentistry. In Nanobiomaterials in Dentistry: Applications of Nanobiomaterials; Elsevier Inc.: Oxford, UK, 2016; Volume 11, pp. 107–132. ISBN 9780323428903. [Google Scholar]
- Moheet, I.A.; Luddin, N.; Ab Rahman, I.; Masudi, S.M.; Kannan, T.P.; Abd Ghani, N.R.N. Evaluation of mechanical properties and bond strength of nano-hydroxyapatite-silica added glass ionomer cement. Ceram. Int. 2018, 44, 9899–9906. [Google Scholar] [CrossRef]
- Thampi, V.A.; Prabhu, M.; Kavitha, K.; Manivasakan, P.; Prabu, P.; Rajendran, V.; Shankar, S.; Kulandaivelu, P. Hydroxyapatite, alumina/zirconia, and nanobioactive glass cement for tooth-restoring applications. Ceram. Int. 2014, 40, 14355–14365. [Google Scholar] [CrossRef]
- Goyal, M.; Sharma, K. Novel multi-walled carbon nanotube reinforced glass-ionomer cements for dental restorations. Mater. Today Proc. 2020, 37, 3035–3037. [Google Scholar] [CrossRef]
- Sun, L.; Yan, Z.; Duan, Y.; Zhang, J.; Liu, B. Improvement of the mechanical, tribological and antibacterial properties of glass ionomer cements by fluorinated graphene. Dent. Mater. 2018, 34, e115–e127. [Google Scholar] [CrossRef]
- Pani, S.C.; Aljammaz, M.T.; Alrugi, A.M.; Aljumaah, A.M.; Alkahtani, Y.M.; Alkhuraif, A. Color stability of glass ionomer cement after reinforced with two different nanoparticles. Int. J. Dent. 2020. [Google Scholar] [CrossRef]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef]
- de Moura, N.K.; Martins, E.F.; Oliveira, R.L.M.S.; de Brito Siqueira, I.A.W.; Machado, J.P.B.; Esposito, E.; Amaral, S.S.; de Vasconcellos, L.M.R.; Passador, F.R.; de Sousa Trichês, E. Synergistic effect of adding bioglass and carbon nanotubes on poly(lactic acid) porous membranes for guided bone regeneration. Mater. Sci. Eng. C 2020, 117, 111327. [Google Scholar] [CrossRef]
- Taton, T.A. Boning up on biology. Nature 2001, 412, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Zanello, L.P.; Zhao, B.; Hu, H.; Haddon, R.C. Bone cell proliferation on carbon nanotubes. Nano Lett. 2006, 6, 562–567. [Google Scholar] [CrossRef]
- Teh, S.J.; Lai, C.W. Carbon nanotubes for dental implants. In Applications of Nanocomposite Materials in Dentistry; Elsevier: Duxford, UK, 2018; pp. 93–105. ISBN 9780128137598. [Google Scholar]
- Gholami, F.; Noor, A.F.M. Hydroxyapatite reinforced with multi-walled carbon nanotubes and bovine serum albumin for bone substitute applications. AIP Conf. Proc. 2016, 1791, 20045. [Google Scholar] [CrossRef] [Green Version]
- Pourakbar Saffar, K.; Sudak, L.J.; Federico, S. A biomechanical evaluation of CNT-grown bone. J. Biomed. Mater. Res. Part A 2016, 104, 465–475. [Google Scholar] [CrossRef]
- Bianco, A.; Kostarelos, K.; Prato, M. Making carbon nanotubes biocompatible and biodegradable. Chem. Commun. 2011, 47, 10182–10188. [Google Scholar] [CrossRef] [PubMed]
- Miura, J.; Maeda, Y.; Nakai, H.; Zako, M. Multiscale analysis of stress distribution in teeth under applied forces. Dent. Mater. 2009, 25, 67–73. [Google Scholar] [CrossRef]
- Bhattacharya, M.; Seong, W.J. Carbon nanotube-based materials-preparation, biocompatibility, and applications in dentistry. In Nanobiomaterials in Clinical Dentistry, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 41–76. ISBN 9780128158869. [Google Scholar]
- Sagadevan, S.; Periasamy, M. Recent trends in nanobiosensors and their applications—A review. Rev. Adv. Mater. Sci. 2014, 36, 62–69. [Google Scholar]
- Hahn, B.D.; Lee, J.M.; Park, D.S.; Choi, J.J.; Ryu, J.; Yoon, W.H.; Lee, B.K.; Shin, D.S.; Kim, H.E. Mechanical and in vitro biological performances of hydroxyapatite-carbon nanotube composite coatings deposited on Ti by aerosol deposition. Acta Biomater. 2009, 5, 3205–3214. [Google Scholar] [CrossRef]
- Marrs, B.; Andrews, R.; Rantell, T.; Pienkowski, D. Augmentation of acrylic bone cement with multiwall carbon nanotubes. J. Biomed. Mater. Res. Part A 2006, 77, 269–276. [Google Scholar] [CrossRef]
- Imazato, S.; Kitagawa, H.; Tsuboi, R.; Kitagawa, R.; Thongthai, P.; Sasaki, J. Non-biodegradable polymer particles for drug delivery: A new technology for “bio-active” restorative materials. Dent. Mater. J. 2017, 36, 524–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, L.; Pei, X.; He, R.; Wan, Q.; Wang, J. Multiwall carbon nanotubes/polycaprolactone composites for bone tissue engineering application. Colloids Surf. B Biointerfaces 2012, 93, 226–234. [Google Scholar] [CrossRef]
- Kim, J.J.; Bae, W.J.; Kim, J.M.; Kim, J.J.; Lee, E.J.; Kim, H.W.; Kim, E.C. Mineralized polycaprolactone nanofibrous matrix for odontogenesis of human dental pulp cells. J. Biomater. Appl. 2014, 28, 1069–1078. [Google Scholar] [CrossRef]
- Stutz, C.; Strub, M.; Clauss, F.; Huck, O.; Schulz, G.; Gegout, H.; Benkirane-Jessel, N.; Bornert, F.; Kuchler-Bopp, S. A new polycaprolactone-based biomembrane functionalized with BMP-2 and stem cells improves maxillary bone regeneration. Nanomaterials 2020, 10, 1774. [Google Scholar] [CrossRef]
- Ketabi, M.A.; Shahnavazi, M.; Fekrazad, R.; Tondnevis, F.; Keshvari, H.; Raz, M.; Sadeghi, A.; Abolhasani, M.M. Synthesis and in vitro characterization of carbon nano tube-polycaprolactone composite scaffold for odontoblast cell interaction. In Key Engineering Materials; Trans Tech Publications Ltd.: Zurich, Switzerland, 2017; Volume 720, pp. 114–119. [Google Scholar]
- Kang, S.; Herzberg, M.; Rodrigues, D.F.; Elimelech, M. Antibacterial effects of carbon nanotubes: Size does matter! Langmuir 2008, 24, 6409–6413. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.D.; Kim, T.H.; Mandakhbayar, N.; Singh, R.K.; Jang, J.H.; Lee, J.H.; Kim, H.W. Coating biopolymer nanofibers with carbon nanotubes accelerates tissue healing and bone regeneration through orchestrated cell- and tissue-regulatory responses. Acta Biomater. 2020, 108, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.M.; Yilgor, I.; Yilgor, E.; Erman, B. Electrospinning of polyurethane fibers. Polymer 2002, 43, 3303–3309. [Google Scholar] [CrossRef]
- Uyar, T.; Çökeliler, D.; Doʇan, M.; Koçum, I.C.; Karatay, O.; Denkbaş, E.B. Electrospun nanofiber reinforcement of dental composites with electromagnetic alignment approach. Mater. Sci. Eng. C 2016, 62, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.L.S.; Tribst, J.P.M.; Dal Piva, A.M.O.; Souza, A.C.O. In vitro evaluation of multi-walled carbon nanotube reinforced nanofibers composites for dental application. Int. J. Polym. Mater. Polym. Biomater. 2020, 69, 1015–1022. [Google Scholar] [CrossRef]
- Sanchez-Garcia, M.D.; Lagaron, J.M.; Hoa, S.V. Effect of addition of carbon nanofibers and carbon nanotubes on properties of thermoplastic biopolymers. Compos. Sci. Technol. 2010, 70, 1095–1105. [Google Scholar] [CrossRef]
- Li, X.; Liu, W.; Sun, L.; Aifantis, K.E.; Yu, B.; Fan, Y.; Feng, Q.; Cui, F.; Watari, F. Resin composites reinforced by nanoscaled fibers or tubes for dental regeneration. BioMed Res. Int. 2014, 2014, 1–14. [Google Scholar] [CrossRef]
- Singh, B.G.P.; Baburao, C.; Pispati, V.; Pathipati, H.; Muthy, N.; Prassana, S.R.V.; Rathode, B.G. Carbon nanotubes. A novel drug delivery system. Int. J. Res. Pharm. Chem. 2012, 2, 523–532. [Google Scholar]
- Hilder, T.A.; Hill, J.M. Modeling the loading and unloading of drugs into nanotubes. Small 2009, 5, 300–308. [Google Scholar] [CrossRef]
- Jin, H.; Heller, D.A.; Sharma, R.; Strano, M.S. Size-dependent cellular uptake and expulsion of single-walled carbon nanotubes: Single particle tracking and a generic uptake model for nanoparticles. ACS Nano 2009, 3, 149–158. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The 2 arrangements of the carbon atoms in (A) SWCNTs and (B) MWCNTs.

Figure 2.
Classification system of ceramic and ceramic-like materials used in dentistry. Adapted from [38].
Figure 2.
Classification system of ceramic and ceramic-like materials used in dentistry. Adapted from [38].

Figure 3.
Basic composition of a glass ionomer cement (GIC) and its interaction with a tooth.

Figure 4.
Illustration of the electrospinning method.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Classification and characteristics of the glass ionomer cements.
| Classification | Characteristics and Use | Reference |
|---|---|---|
| Type I | Luting cements with low fill thickness and rapid setting. Used for the cementation of inlays, crowns, fixed partial dentures, and orthodontic appliances. | [43] |
| Type II | Restorations with particles larger than Type I. | [43] |
| Type II-1 | Considered as esthetic cements available for conventional and resin-modified presentations. | [43] |
| Type II-2 | Reinforced cement for esthetic applications. | [43] |
| Type III | Lining cements and fissure sealants with low viscosity and rapid setting. | [43] |
| Based on composition | Derived from an organic acid and a glass component referred to as acid-base reaction cements. | [44] |
| Resin-modified GICs | Contains an ion-leachable glass, a water-soluble polymeric acid, an organic monomer, and an initiator system. | [45] |
| Polyacid-modified composite resin | Light-polymerized composite resin restoratives with ion-leachable glass particles and an anhydrous polyalkenoic acid. | [46] |
| Metal-reinforced GICs | Mixture of a conventional powder with the addition of a range of metallic powders, such as silver alloys, gold, palladium, and titanium dioxide. | [47] |
| High-viscosity GICs | Have a high powder–liquid ratio and fast setting properties. | [48] |
| Zirconia-reinforced GICs | Contain zirconium oxide, glass powder, tartaric acid (1–10%), polyacrylic acid (20–50%), and deionized water. | [49] |
Table 2.
Mechanical properties of enamel and dentin. Retrieved from [51].
Table 2.
Mechanical properties of enamel and dentin. Retrieved from [51].
| Tooth Tissue | Property | Value |
|---|---|---|
| Hardness | 2.0–3.5 GPa * | |
| Enamel | Young’s modulus | 80–120 GPa |
| Fracture toughness | 0.67–3.93 MPa m1/2 | |
| Hardness | 0.3–0.7 GPa | |
| Dentin | Young´s modulus | 10–40 GPa |
| Fracture toughness | 1.1–2.3 MPa m1/2 ** |
* GPa indicates gigapascals; ** MPa indicates megapascals. Fracture toughness is expressed in units of stress times the square root of crack length: MPa m1/2.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Castro-Rojas, M.A.; Vega-Cantu, Y.I.; Cordell, G.A.; Rodriguez-Garcia, A. Dental Applications of Carbon Nanotubes. Molecules 2021, 26, 4423. https://doi.org/10.3390/molecules26154423
AMA Style
Castro-Rojas MA, Vega-Cantu YI, Cordell GA, Rodriguez-Garcia A. Dental Applications of Carbon Nanotubes. Molecules. 2021; 26(15):4423. https://doi.org/10.3390/molecules26154423
Chicago/Turabian StyleCastro-Rojas, Marco A., Yadira I. Vega-Cantu, Geoffrey A. Cordell, and Aida Rodriguez-Garcia. 2021. "Dental Applications of Carbon Nanotubes" Molecules 26, no. 15: 4423. https://doi.org/10.3390/molecules26154423