
Volatile Organic Compounds, Bacterial Airway Microbiome, Spirometry and Exercise Performance of Patients after Surgical Repair of Congenital Diaphragmatic Hernia

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Clinical Examination
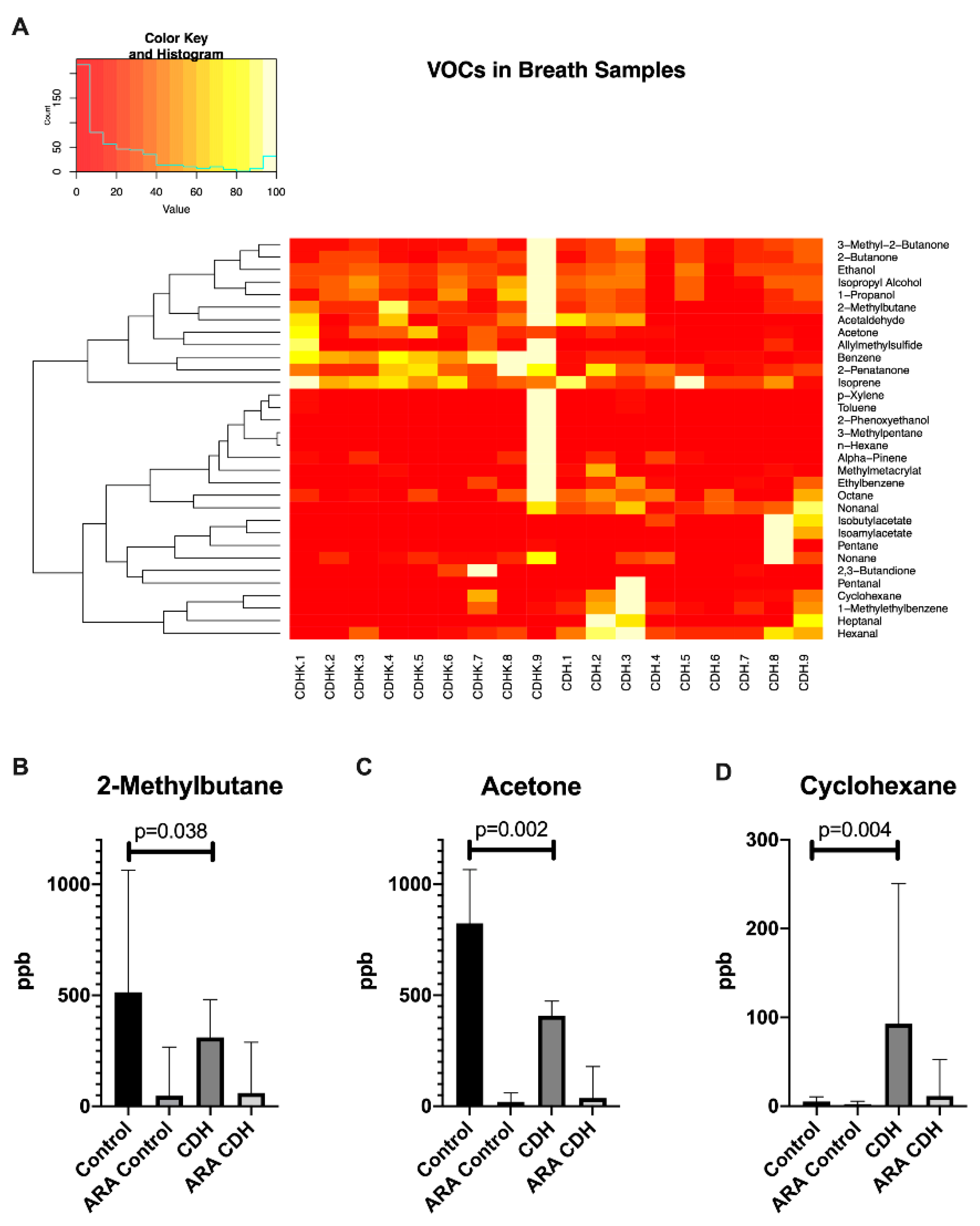
2.2. Breath VOC Profile
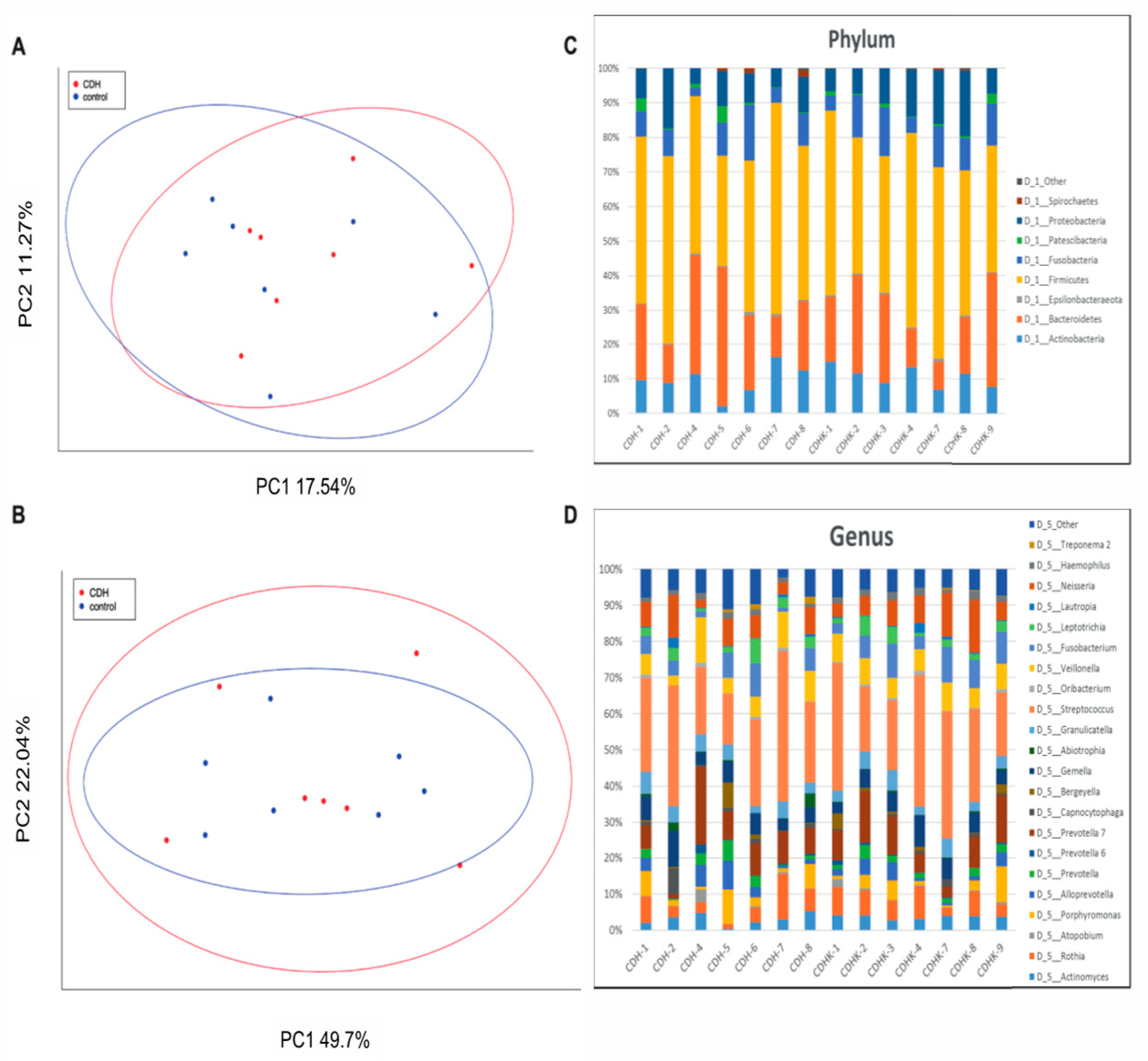
2.3. 16S Based Airway Microbiome
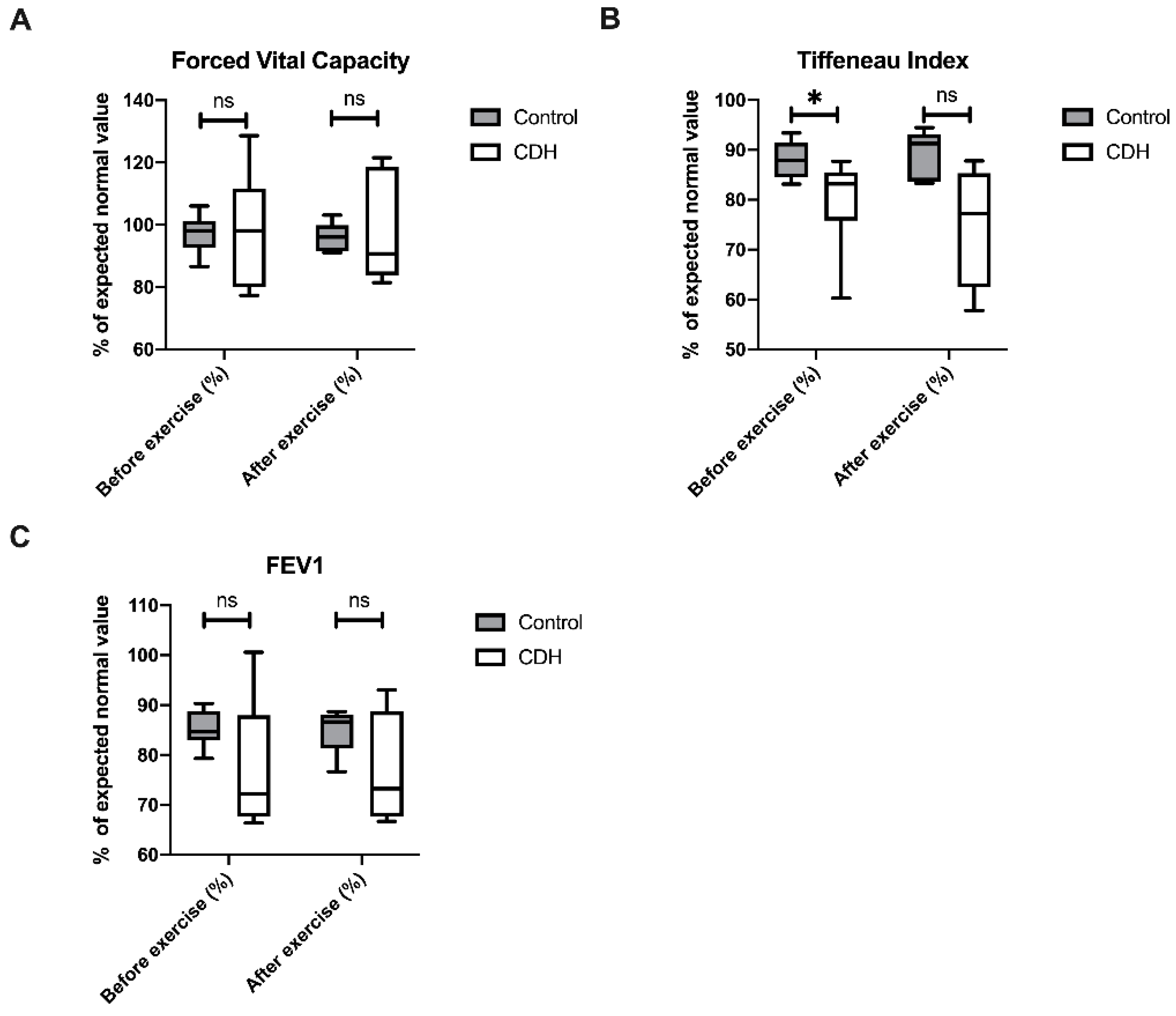
2.4. Spirometry
2.5. Spiroergometry
3. Discussion
4. Materials and Methods
4.1. Clinical Examination
4.2. Breath VOC Sampling
4.3. Breath VOC Analysis
4.4. 16S Based Airway Microbiome
4.5. Spirometry
4.6. Spiroergometry
4.7. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Registration
Sample Availability
References
- Flemmer, A.W.; Jani, J.C.; Bergmann, F.; Muensterer, O.J.; Gallot, D.; Hajek, K.; Sugawara, J.; Till, H.; Deprest, J. Lung tissue mechanics predict lung hypoplasia in a rabbit model for congenital diaphragmatic hernia. Pediatr. Pulmonol. 2007, 42, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Zalla, J.M.; Stoddard, G.J.; Yoder, B.A. Improved mortality rate for congenital diaphragmatic hernia in the modern era of management: 15year experience in a single institution. J. Pediatr. Surg. 2015, 50, 524–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skari, H.; Bjornland, K.; Haugen, G.; Egeland, T.; Emblem, R. Congenital diaphragmatic hernia: A meta-analysis of mortality factors. J. Pediatr. Surg. 2000, 35, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Bohn, D. Congenital Diaphragmatic Hernia. Am. J. Respir. Crit. Care Med. 2002, 166, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Bojanić, K.; Grizelj, R.; Dilber, D.; Saric, D.; Vuković, J.; Pianosi, P.T.; Driscoll, D.J.; Weingarten, T.N.; Pritišanac, E.; Schroeder, D.R.; et al. Cardiopulmonary exercise performance is reduced in congenital diaphragmatic hernia survivors. Pediatr. Pulmonol. 2016, 51, 1320–1329. [Google Scholar] [CrossRef]
- Bagolan, P.; Casaccia, G.; Crescenzi, F.; Nahom, A.; Trucchi, A.; Giorlandino, C. Impact of a current treatment protocol on outcome of high-risk congenital diaphragmatic hernia. J. Pediatr. Surg. 2004, 39, 313–318. [Google Scholar] [CrossRef]
- Peetsold, M.G.; Heij, H.A.; Nagelkerke, A.F.; Ijsselstijn, H.; Tibboel, D.; Quanjer, P.H.; Gemke, R.J.B.J. Pulmonary function and exercise capacity in survivors of congenital diaphragmatic hernia. Eur. Respir. J. 2009, 34, 1140–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trachsel, D.; Selvadurai, H.; Bohn, D.; Langer, J.C.; Coates, A.L. Long-term pulmonary morbidity in survivors of congenital diaphragmatic hernia. Pediatr. Pulmonol. 2005, 39, 433–439. [Google Scholar] [CrossRef]
- Basek, P.; Bajrami, S.; Straub, D.; Moeller, A.; Baenziger, O.; Wildhaber, J.; Bernet, V. The pulmonary outcome of long-term survivors after congenital diaphragmatic hernia repair. Swiss Med Wkly. 2008, 138, 173–179. [Google Scholar]
- Brar, T.; Nagaraj, S.; Mohapatra, S. Microbes and asthma. Curr. Opin. Pulm. Med. 2012, 18, 14–22. [Google Scholar] [CrossRef]
- Boutin, S.; Graeber, S.Y.; Weitnauer, M.; Panitz, J.; Stahl, M.; Clausznitzer, D.; Kaderali, L.; Einarsson, G.; Tunney, M.M.; Elborn, J.S.; et al. Comparison of Microbiomes from Different Niches of Upper and Lower Airways in Children and Adolescents with Cystic Fibrosis. PLoS ONE 2015, 10, e0116029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, A.; Beck, J.M.; Schloss, P.D.; Campbell, T.B.; Crothers, K.; Curtis, J.L.; Flores, S.C.; Fontenot, A.P.; Ghedin, E.; Huang, L.; et al. Comparison of the respiratory microbiome in healthy nonsmokers and smokers. Am. J. Respir. Crit. Care Med. 2013, 187, 1067–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gischler, S.J.; van der Cammen-van Zijp, M.H.M.; Mazer, P.; Madern, G.C.; Bax, N.M.; De Jongste, J.C.; Van Dijk, M.; Tibboel, D.; Ijsselstijn, H. A prospective comparative evaluation of persistent respiratory morbidity in esophageal atresia and congenital diaphragmatic hernia survivors. J. Pediatr. Surg. 2009, 44, 1683–1690. [Google Scholar] [CrossRef] [Green Version]
- van der Cammen-van Zijp, M.H.M.; Gischler, S.J.; Mazer, P.; Van Dijk, M.; Tibboel, D.; Ijsselstijn, H. Motor-function and exercise capacity in children with major anatomical congenital anomalies: An evaluation at 5years of age. Early Hum. Dev. 2010, 86, 523–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marven, S.S.; Smith, C.M.; Claxton, D.; Chapman, J.; Davies, H.A.; Primhak, R.A.; Powell, C.V.E. Pulmonary function, exercise performance, and growth in survivors of congenital diaphragmatic hernia. Arch. Dis. Child. 1998, 78, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Miekisch, W.; Schubert, J.; Nöldge-Schomburg, G. Diagnostic potential of breath analysis—focus on volatile organic compounds. Clin. Chim. Acta 2004, 347, 25–39. [Google Scholar] [CrossRef]
- Van De Kant, K.D.; Van Der Sande, L.J.T.M.; Jöbsis, Q.; Van Schayck, O.C.P.; Dompeling, E. Clinical use of exhaled volatile organic compounds in pulmonary diseases: A systematic review. Respir. Res. 2012, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Trefz, P.; Obermeier, J.; Lehbrink, R.; Schubert, J.K.; Miekisch, W.; Fischer, D.-C. Exhaled volatile substances in children suffering from type 1 diabetes mellitus: Results from a cross-sectional study. Sci. Rep. 2019, 9, 15707–15709. [Google Scholar] [CrossRef]
- Trefz, P.; Rösner, L.; Hein, D.; Schubert, J.K.; Miekisch, W. Evaluation of needle trap micro-extraction and automatic alveolar sampling for point-of-care breath analysis. Anal. Bioanal. Chem. 2013, 405, 3105–3115. [Google Scholar] [CrossRef]
- Obermeier, J.; Trefz, P.; Happ, J.; Schubert, J.K.; Staude, H.; Fischer, D.-C.; Miekisch, W. Exhaled volatile substances mirror clinical conditions in pediatric chronic kidney disease. PLoS ONE 2017, 12, e0178745. [Google Scholar] [CrossRef]
- Barker, M.; Hengst, M.; Schmid, J.; Buers, H.-J.; Mittermaier, B.; Klemp, D.; Koppmann, R. Volatile organic compounds in the exhaled breath of young patients with cystic fibrosis. Eur. Respir. J. 2006, 27, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Schubert, R.; Schwoebel, H.; Mau-Moeller, A.; Behrens, M.; Fuchs, P.; Sklorz, M.; Schubert, J.K.; Bruhn, S.; Miekisch, W. Metabolic monitoring and assessment of anaerobic threshold by means of breath biomarkers. Metabolomics 2012, 8, 1069–1080. [Google Scholar] [CrossRef]
- Oguma, T.; Nagaoka, T.; Kurahashi, M.; Kobayashi, N.; Yamamori, S.; Tsuji, C.; Takiguchi, H.; Niimi, K.; Tomomatsu, H.; Tomomatsu, K.; et al. Clinical contributions of exhaled volatile organic compounds in the diagnosis of lung cancer. PLoS ONE 2017, 12, e0174802. [Google Scholar] [CrossRef]
- Zhou, Y.; Chen, E.; Wu, X.; Hu, Y.; Ge, H.; Xu, P.; Zou, Y.; Jin, J.; Wang, P.; Ying, K. Rational lung tissue and animal models for rapid breath tests to determine pneumonia and pathogens. Am. J. Transl. Res. 2017, 9, 5116–5126. [Google Scholar] [PubMed]
- Turchetta, A.; Fintini, D.; Cafiero, G.; Calzolari, A.; Giordano, U.; Cutrera, R.; Morini, F.; Braguglia, A.; Bagolan, P. Physical activity, fitness, and dyspnea perception in children with congenital diaphragmatic hernia. Pediatr. Pulmonol. 2011, 46, 1000–1006. [Google Scholar] [CrossRef] [PubMed]
- Zaccara, A.; Turchetta, A.; Calzolari, A.; Iacobelli, B.; Nahom, A.; Lucchetti, M.; Bagolan, P.; Rivosecchi, M.; Coran, A. Maximal oxygen consumption and stress performance in children operated on for congenital diaphragmatic hernia. J. Pediatr. Surg. 1996, 31, 1092–1095. [Google Scholar] [CrossRef]
- Politis, M.D.; Bermejo-Sánchez, E.; Canfield, M.A.; Contiero, P.; Cragan, J.D.; Dastgiri, S.; De Walle, H.E.; Feldkamp, M.L.; Nance, A.; Groisman, B.; et al. Prevalence and mortality in children with congenital diaphragmatic hernia: A multicountry study. Ann. Epidemiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Bergmann, A.; Steffens, M.; Trefz, P.; Ziller, M.; Miekisch, W.; Schubert, J.S.; Köhler, H.; Reinhold, P. Impact of food intake on in vivo VOC concentrations in exhaled breath assessed in a caprine animal model. J. Breath Res. 2015, 9, 047113. [Google Scholar] [CrossRef]
- Fischer, S.; Trefz, P.; Bergmann, A.; Steffens, M.; Ziller, M.; Miekisch, W.; Schubert, J.S.; Köhler, H.; Reinhold, P. Physiological variability in volatile organic compounds (VOCs) in exhaled breath and released from faeces due to nutrition and somatic growth in a standardized caprine animal model. J. Breath Res. 2015, 9, 027108. [Google Scholar] [CrossRef]
- Windhaber, J.; Steinbauer, M.; Castellani, C.; Singer, G.; Till, H.; Schober, P. Do Anthropometric and Aerobic Parameters Predict a Professional Career for Adolescent Skiers? Int. J. Sports Med. 2019, 40, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Skrabal, F.; Pichler, G.P.; Penatzer, M.; Steinbichl, J.; Hanserl, A.-K.; Leis, A.; Loibner, H. The Combyn™ ECG: Adding haemodynamic and fluid leads for the ECG. Part II: Prediction of total body water (TBW), extracellular fluid (ECF), ECF overload, fat mass (FM) and “dry” appendicular muscle mass (AppMM). Med. Eng. Phys. 2017, 44, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Oertel, P.; Bergmann, A.; Fischer, S.; Trefz, P.; Küntzel, A.; Reinhold, P.; Köhler, H.; Schubert, J.; Miekisch, W. Evaluation of needle trap micro-extraction and solid-phase micro-extraction: Obtaining comprehensive information on volatile emissions from in vitro cultures. Biomed. Chromatogr. 2018, 32, e4285. [Google Scholar] [CrossRef] [PubMed]
- Traxler, S.; Bischoff, A.-C.; Saß, R.; Trefz, P.; Gierschner, P.; Brock, B.; Schwaiger, T.; Karte, C.; Blohm, U.; Schröder, C.; et al. VOC breath profile in spontaneously breathing awake swine during Influenza A infection. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Trefz, P.; Koehler, H.; Klepik, K.; Möbius, P.; Reinhold, P.; Schubert, J.K.; Miekisch, W. Volatile Emissions from Mycobacterium avium subsp. paratuberculosis Mirror Bacterial Growth and Enable Distinction of Different Strains. PLoS ONE 2013, 8, e76868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettigrew, M.M.; Gent, J.F.; Kong, Y.; Wade, M.; Gansebom, S.; Bramley, A.M.; Jain, S.; Arnold, S.L.R.; McCullers, J.A. Association of sputum microbiota profiles with severity of community-acquired pneumonia in children. BMC Infect. Dis. 2016, 16, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klymiuk, I.; Bilgilier, C.; Stadlmann, A.; Thannesberger, J.; Kastner, M.-T.; Högenauer, C.; Püspök, A.; Biowski-Frotz, S.; Schrutka-Kölbl, C.; Thallinger, G.G.; et al. The Human Gastric Microbiome Is Predicated upon Infection with Helicobacter pylori. Front. Microbiol. 2017, 8, 2508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenna, P.; Hoffmann, C.; Minkah, N.; Aye, P.P.; Lackner, A.; Liu, Z.; Lozupone, C.A.; Hamady, M.; Knight, R.; Bushman, F.D. The Macaque Gut Microbiome in Health, Lentiviral Infection, and Chronic Enterocolitis. PLoS Pathog. 2008, 4, e20. [Google Scholar] [CrossRef] [Green Version]
- Callahan, B.J.; Mcmurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [Green Version]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CDH | Control | Age | Gender | Muscle Mass | Body Fat | VOCs | Pulmonary Microbiome | Spirometry Before Ex. | Spiroergometry | Spirometry After Ex. |
|---|---|---|---|---|---|---|---|---|---|---|
| CDH-1 | CDHK-7 | 12 | m | X | X | X | X | X | X | X |
| CDH-2 | CDHK-8 | 9 | m | X | X | X | X | X | 01 | 01 |
| CDH-3 | CDHK-6 | 8 | m | X | X | X | 01 | X | 01 | 01 |
| CDH-4 | CDHK-9 | 13 | m | X | X | X | X | X | X | X |
| CDH-5 | CDHK-2 | 9 | f | X | X | X | X | X | X | X |
| CDH-6 | CDHK-4 | 12 | f | X | X | X | X | X | X | X |
| CDH-7 | CDHK-3 | 6 | m | 01 | X | X | X | X | 01 | 01 |
| CDH-8 | CDHK-1 | 13 | m | X | X | X | X | X | X | X |
| CDH-9 | CDHK-5 | 7 | f | 02 | 02 | X | 02 | 02 | 02 | 02 |
| Parameter | Control Group | CDH Group | p-Value |
|---|---|---|---|
| Height (cm) | 137.0 (39.5) | 142.5 (36.5) | 0.673 |
| Body weight (kg) | 30.0 (28.4) | 36.4 (30.5) | 0.673 |
| BMI (kg/m2) | 16.0 (5.0) | 18.0 (4.7) | 0.888 |
| Appendicular muscle mass (kg/m2) | 5.6 (3.6) | 5.3 (2.8) | 0.805 |
| Body fat (%) | 5.3 (2.8) | 6.0 (15.0) | 0.442 |
| Parameter | Control Group | CDH Group | p-Value |
|---|---|---|---|
| Relative Performance Capacity (%) | 118.0 (27.0) | 108.0 (33.0) | 0.095 |
| VO2max/kg (mL/kg/min) | 46.7 (12.3) | 42.3 (9.6) | 0.222 |
| Pmax/kg (W/kg) | 3.4 (1.0) | 3.3 (0.8) | 0.310 |
| O2 Pulse (mL) | 12.1 (7.3) | 10.2 (7.6) | 1.0 |
| RER | 1.2 (0.2) | 1.2 (0.1) | 0.841 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Warncke, G.; Singer, G.; Windhaber, J.; Schabl, L.; Friehs, E.; Miekisch, W.; Gierschner, P.; Klymiuk, I.; Eber, E.; Zeder, K.; et al. Volatile Organic Compounds, Bacterial Airway Microbiome, Spirometry and Exercise Performance of Patients after Surgical Repair of Congenital Diaphragmatic Hernia. Molecules 2021, 26, 645. https://doi.org/10.3390/molecules26030645
Warncke G, Singer G, Windhaber J, Schabl L, Friehs E, Miekisch W, Gierschner P, Klymiuk I, Eber E, Zeder K, et al. Volatile Organic Compounds, Bacterial Airway Microbiome, Spirometry and Exercise Performance of Patients after Surgical Repair of Congenital Diaphragmatic Hernia. Molecules. 2021; 26(3):645. https://doi.org/10.3390/molecules26030645
Chicago/Turabian StyleWarncke, Gert, Georg Singer, Jana Windhaber, Lukas Schabl, Elena Friehs, Wolfram Miekisch, Peter Gierschner, Ingeborg Klymiuk, Ernst Eber, Katarina Zeder, and et al. 2021. "Volatile Organic Compounds, Bacterial Airway Microbiome, Spirometry and Exercise Performance of Patients after Surgical Repair of Congenital Diaphragmatic Hernia" Molecules 26, no. 3: 645. https://doi.org/10.3390/molecules26030645