
Pharmacokinetic Characterization and Tissue Distribution of Fusion Protein Therapeutics by Orthogonal Bioanalytical Assays and Minimal PBPK Modeling


Abstract
:1. Introduction
2. Results and Discussion
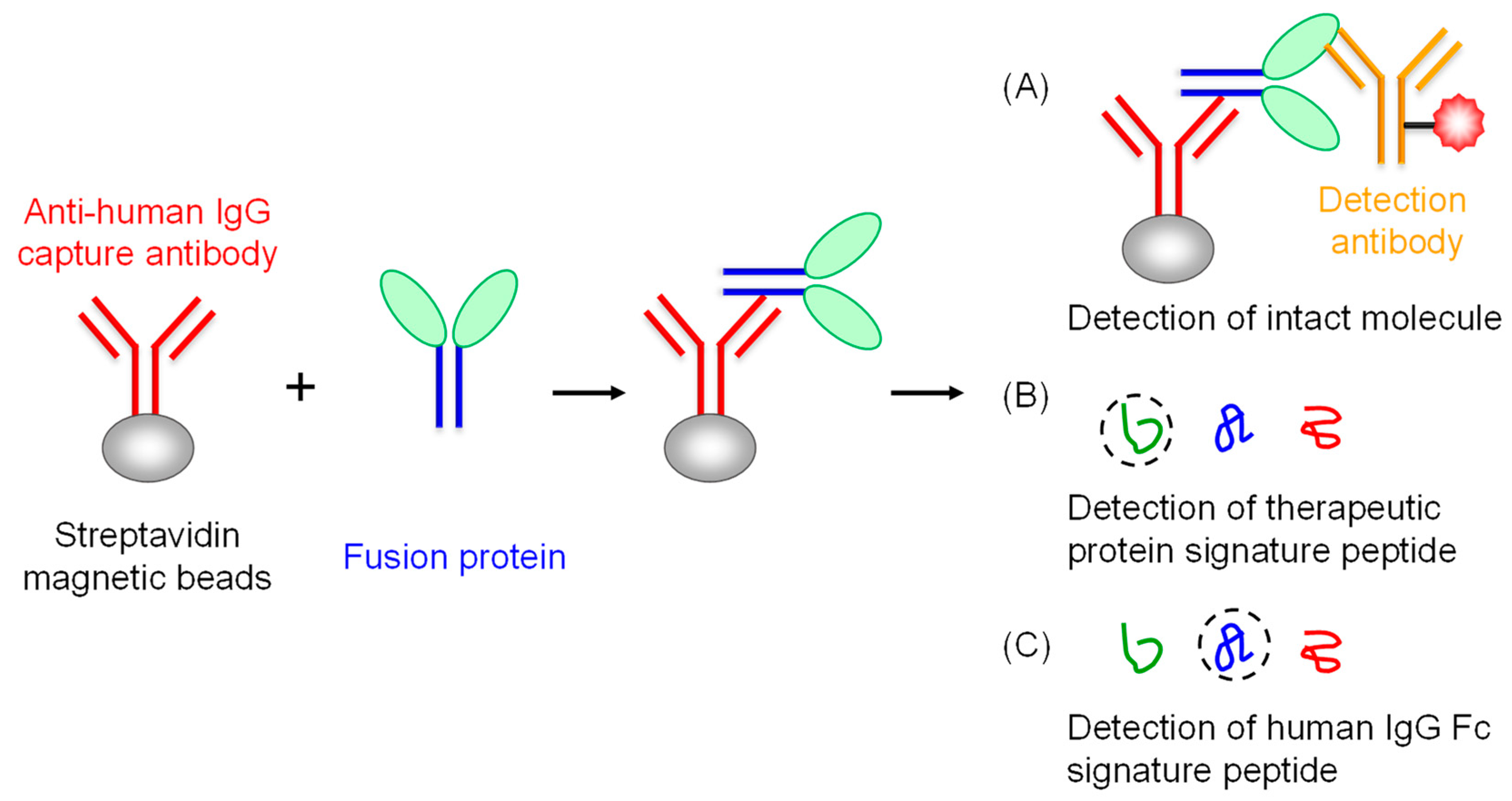
2.1. Strategy to Characterize the Pharmacokinetic Property of TFPs by LBA and IC-LC/MS
2.2. Selection of Signature Peptides to Quantify the Human IgG4 and Interferon Alpha
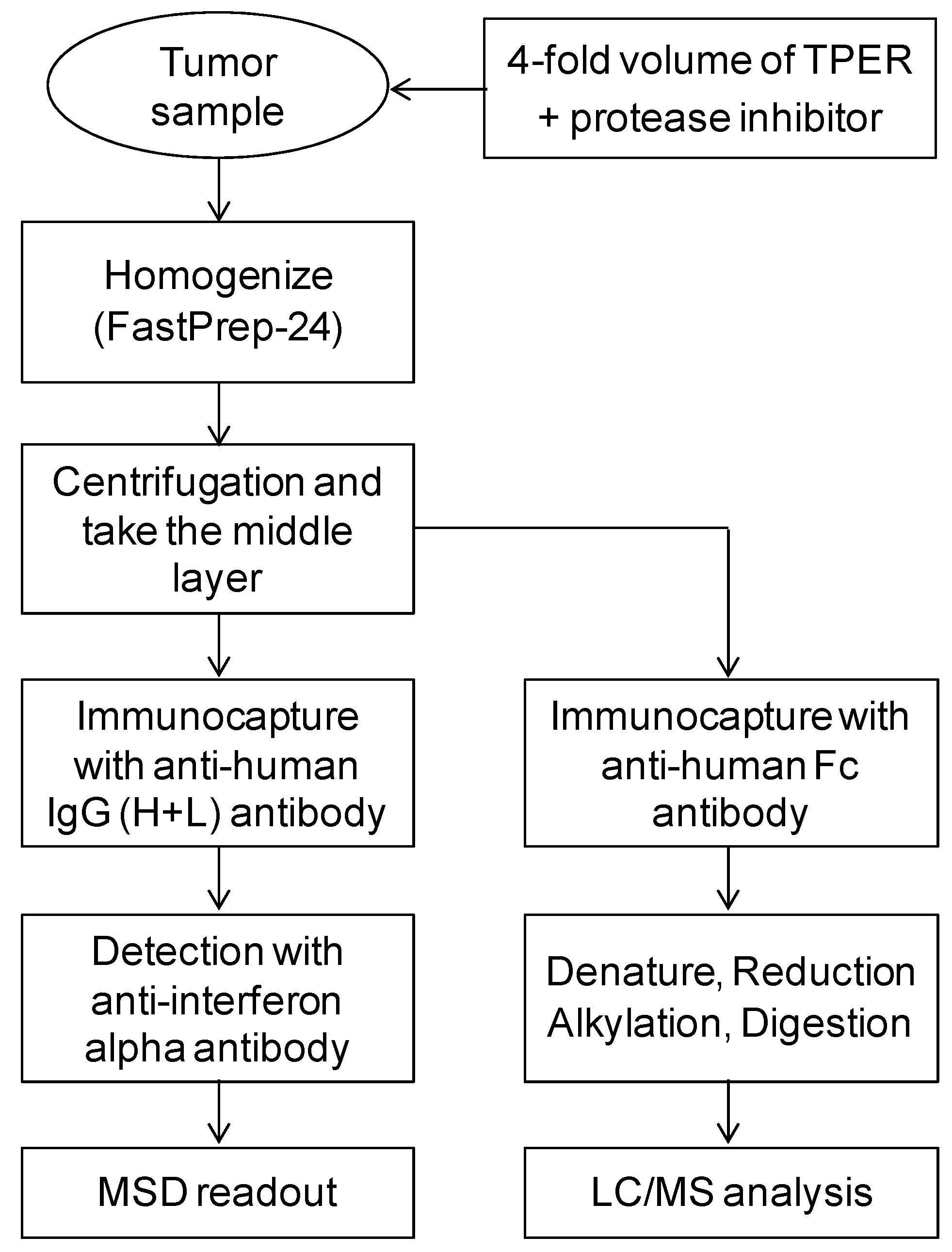
2.3. Workflow of Tumor Sample Preparation and Immunocapture for LBA and IC-LC/MS
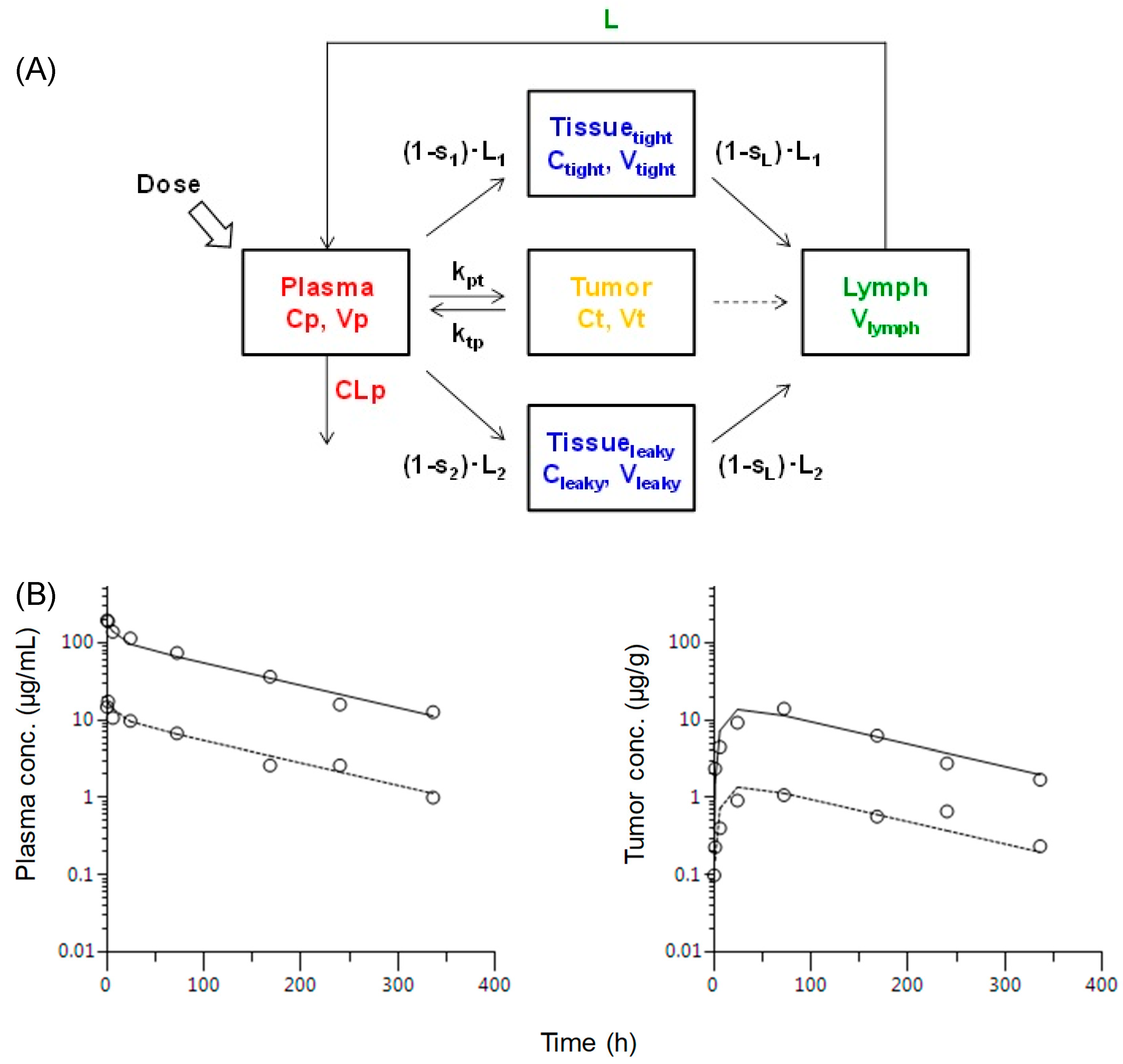
2.4. The Plasma and Tumor Concentration Versus Time Profile in Mice after a Single i.v. Administration of the TFP
2.5. Minimal PBPK Modeling to Describe the Relationship of Plasma and Tumor Pharmacokinetics of the TFP
3. Materials and Methods
3.1. Chemicals and Reagents
3.2. In Vivo Human Derived Xenograft Tumor Studies in Mice
3.3. Instrumentation and Experimental Conditions for Ligand Binding Assay
3.4. Sample Preparation Procedure for LC/MS
3.5. Method qualification
3.6. Instrumentation and Conditions for LC/MS Analysis
3.7. Pharmacokinetic Analysis
3.8. Statistics
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gillies, S.D.; Young, D.; Lo, K.M.; Roberts, S. Biological activity and in vivo clearance of antitumor antibody/cytokine fusion proteins. Bioconjug. Chem. 1993, 4, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Lobo, E.D.; Hansen, R.J.; Balthasar, J.P. Antibody pharmacokinetics and pharmacodynamics. J. Pharm. Sci. 2004, 93, 2645–2668. [Google Scholar] [CrossRef] [PubMed]
- Neubert, H.; Fountain, S.; King, L.; Clark, T.; Weng, Y.; O’Hara, D.M.; Li, W.; Leung, S.; Ray, C.; Palandra, J.; et al. Tissue bioanalysis of biotherapeutics and drug targets to support PK/PD. Bioanalysis 2012, 4, 2589–2604. [Google Scholar] [CrossRef] [PubMed]
- Abuqayyas, L.; Balthasar, J.P. Application of PBPK modeling to predict monoclonal antibody disposition in plasma and tissues in mouse models of human colorectal cancer. J. Pharm. Pharm. 2012, 39, 683–710. [Google Scholar] [CrossRef] [Green Version]
- Thurber, G.M.; Schmidt, M.M.; Wittrup, K.D. Factors determining antibody distribution in tumors. Trends Pharm. Sci. 2008, 29, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Shah, D.K.; Betts, A.M. Antibody biodistribution coefficients: inferring tissue concentrations of monoclonal antibodies based on the plasma concentrations in several preclinical species and human. MAbs 2013, 5, 297–305. [Google Scholar] [CrossRef]
- Hoofnagle, A.N.; Wener, M.H. The fundamental flaws of immunoassays and potential solutions using tandem mass spectrometry. J. Immunol. Methods 2009, 347, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Sleczka, B.G.; Mehl, J.T.; Shuster, D.J.; Lewis, K.E.; Moore, R.; Vuppugalla, R.; Rajendran, S.; D’Arienzo, C.J.; Olah, T.V. Quantification of human mAbs in mouse tissues using generic affinity enrichment procedures and LC-MS detection. Bioanalysis 2014, 6, 1795–1811. [Google Scholar] [CrossRef]
- Sugimoto, H.; Wei, D.; Dong, L.; Ghosh, D.; Chen, S.; Qian, M.G. Perspectives on potentiating immunocapture-LC-MS for the bioanalysis of biotherapeutics and biomarkers. Bioanalysis 2018, 10, 1679–1690. [Google Scholar] [CrossRef]
- Pearson, J.T.; Rock, D.A. Bioanalytical approaches to assess the proteolytic stability of therapeutic fusion proteins. Bioanalysis 2015, 7, 3035–3051. [Google Scholar] [CrossRef]
- Jones, H.; Rowland-Yeo, K. Basic concepts in physiologically based pharmacokinetic modeling in drug discovery and development. Cpt. Pharmacomet. Syst. Pharm. 2013, 2, e63. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Balthasar, J.P.; Jusko, W.J. Second-generation minimal physiologically-based pharmacokinetic model for monoclonal antibodies. J. Pharm. Pharm. 2013, 40, 597–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cilliers, C.; Guo, H.; Liao, J.; Christodolu, N.; Thurber, G.M. Multiscale Modeling of Antibody-Drug Conjugates: Connecting Tissue and Cellular Distribution to Whole Animal Pharmacokinetics and Potential Implications for Efficacy. Aaps. J. 2016, 18, 1117–1130. [Google Scholar] [CrossRef] [Green Version]
- Liebler, D.C.; Zimmerman, L.J. Targeted quantitation of proteins by mass spectrometry. Biochemistry 2013, 52, 3797–3806. [Google Scholar] [CrossRef] [PubMed]
- Hoofnagle, A.N.; Whiteaker, J.R.; Carr, S.A.; Kuhn, E.; Liu, T.; Massoni, S.A.; Thomas, S.N.; Townsend, R.R.; Zimmerman, L.J.; Boja, E.; et al. Recommendations for the Generation, Quantification, Storage, and Handling of Peptides Used for Mass Spectrometry-Based Assays. Clin. Chem. 2016, 62, 48–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furlong, M.T.; Zhao, S.; Mylott, W.; Jenkins, R.; Gao, M.; Hegde, V.; Tamura, J.; Tymiak, A.; Jemal, M. Dual universal peptide approach to bioanalysis of human monoclonal antibody protein drug candidates in animal studies. Bioanalysis 2013, 5, 1363–1376. [Google Scholar] [CrossRef] [PubMed]
- Merck&Co. IntronRA Product Label. Semin. Liver. Dis. 2008, 23, 23–28. [Google Scholar]
- Tibbitts, J.; Canter, D.; Graff, R.; Smith, A.; Khawli, L.A. Key factors influencing ADME properties of therapeutic proteins: A need for ADME characterization in drug discovery and development. MAbs 2016, 8, 229–245. [Google Scholar] [CrossRef] [Green Version]
- Harris, R.J. Processing of C-terminal lysine and arginine residues of proteins isolated from mammalian cell culture. J. Chromatogr. A 1995, 705, 129–134. [Google Scholar] [CrossRef]
- Santora, L.C.; Krull, I.S.; Grant, K. Characterization of recombinant human monoclonal tissue necrosis factor-alpha antibody using cation-exchange HPLC and capillary isoelectric focusing. Anal. Biochem. 1999, 275, 98–108. [Google Scholar] [CrossRef]
- Baxter, L.T.; Zhu, H.; Mackensen, D.G.; Jain, R.K. Physiologically based pharmacokinetic model for specific and nonspecific monoclonal antibodies and fragments in normal tissues and human tumor xenografts in nude mice. Cancer Res. 1994, 54, 1517–1528. [Google Scholar] [PubMed]
- Mager, D.E.; Jusko, W.J. General pharmacokinetic model for drugs exhibiting target-mediated drug disposition. J. Pharm. Pharm. 2001, 28, 507–532. [Google Scholar]
- Li, X.; Jusko, W.J.; Cao, Y. Role of Interstitial Fluid Turnover on Target Suppression by Therapeutic Biologics Using a Minimal Physiologically Based Pharmacokinetic Model. J. Pharm. Exp. 2018, 367, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, M.A.; Tseng, C.M.; Roskos, L.K. Elimination mechanisms of therapeutic monoclonal antibodies. Drug Discov. Today 2006, 11, 81–88. [Google Scholar] [CrossRef]
- Garg, A.; Balthasar, J.P. Physiologically-based pharmacokinetic (PBPK) model to predict IgG tissue kinetics in wild-type and FcRn-knockout mice. J. Pharm. Pharm. 2007, 34, 687–709. [Google Scholar] [CrossRef] [PubMed]
- Durocher, Y.; Perret, S.; Kamen, A. High-level and high-throughput recombinant protein production by transient transfection of suspension-growing human 293-EBNA1 cells. Nucleic Acids Res. 2002, 30, E9. [Google Scholar] [CrossRef]
- Sugimoto, H.; Ghosh, D.; Chen, S.; Smith, M.D.; Abu-Yousif, A.O.; Qian, M.G. Immunocapture-LC/MS-Based Target Engagement Measurement in Tumor Plasma Membrane. Anal. Chem. 2018, 90, 13564–13571. [Google Scholar] [CrossRef]
- Neubert, H.; Song, A.; Lee, A.; Wei, C.; Duggan, J.; Xu, K.; Woolf, E.; Evans, C.; Palandra, J.; Laterza, O.; et al. 2017 White Paper: rise of hybrid LBA/LCMS immunogenicity assays (Part 2: hybrid LBA/LCMS biotherapeutics, biomarkers & immunogenicity assays and regulatory agencies’ inputs). In Proceedings of the 11th Workshop on Recent Issues in Bioanalysis, Los Angeles, CA, USA, 3–7 April 2017; pp. 1895–1912. [Google Scholar]
Sample Availability: Samples are available from the authors. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assay Platform | Signature Peptide | Matrix | Nominal Conc. (μg/mL or g) | Intra-Assay | |||
|---|---|---|---|---|---|---|---|
| Average Conc. (μg/mL) | CV (%) | RE (%) | |||||
| LBA | - | Plasma | LQC | 3.00 | 2.79 | 8.1 | −7.0 |
| MQC | 30.0 | 32.3 | 12.1 | 7.6 | |||
| HQC | 240 | 278 | 12.9 | 15.6 | |||
| Tumor | LQC | 0.300 | 0.301 | 8.0 | 0.3 | ||
| MQC | 2.00 | 2.14 | 5.7 | 7.0 | |||
| HQC | 8.00 | 8.27 | 4.1 | 3.3 | |||
| IC-LC/MS | Human IgG4 | Plasma | LQC | 0.300 | 0.353 | 4.1 | 17.7 |
| MQC | 2.00 | 2.20 | 7.6 | 10.0 | |||
| HQC | 80.0 | 85.2 | 2.7 | 6.5 | |||
| Tumor | LQC | 0.300 | 0.316 | 8.2 | 5.2 | ||
| MQC | 2.00 | 1.98 | 2.3 | −0.8 | |||
| Interferon alpha | Plasma | LQC | 0.300 | 0.334 | 10.2 | 11.2 | |
| MQC | 2.00 | 2.18 | 5.4 | 9.1 | |||
| HQC | 80.0 | 88.1 | 4.1 | 10.1 | |||
| Tumor | LQC | 0.300 | 0.329 | 15.4 | 9.5 | ||
| MQC | 2.00 | 1.67 | 6.7 | −16.6 | |||
| AUC (h*μg/mL) | CL (mL/h/kg) | Cmax (μg/mL) | T 1/2 (h) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| IC-LC/MS | IC-LC/MS | IC-LC/MS | |||||||||
| Dosing | LBA | INFα | IgG4 | LBA | INFα | IgG4 | LBA | INFα | IgG4 | ||
| Plasma | IV 1 mg/kg | 1470 | 1600 | 1650 | 0.624 | 0.539 | 0.527 | 17.3 | 17.3 | 17.6 | 98.1 |
| IV 10 mg/kg | 16200 | 16000 | 16400 | 0.559 | 0.593 | 0.568 | 194 | 202 | 194 | 90.8 | |
| Tumor | IV 1 mg/kg | 229 | 227 | 168 | 2.31 | 1.93 | 1.57 | ||||
| IV 10 mg/kg | 2210 | 1730 | 1480 | 14.0 | 10.9 | 8.67 | |||||
| Parameter | Value | %CV | Unit | Description | Reference |
|---|---|---|---|---|---|
| L | 0.12 | mL/h | Total lymph flow | [12] | |
| ISF | 4.35 | mL | Total interstitial flow volume | [12] | |
| Kp | 0.156 | - | Tissue-to-plasma concentration ratio | Experimental data | |
| Vp | 1.74 | 6.5 | mL | Plasma volume | Fitted data |
| Vlymph | 1.7 | mL | Lymphatic volume | [12] | |
| Vtumor | 0.5 | mL | Tumor volume | Experimental data | |
| CLp | 0.0181 | 3.0 | mL/h | Clearance | Fitted data |
| kpt | 0.00269 | 0.85 | 1/h | Rate constant | Fitted data |
| ktp | 0.0602 | 2.6 | 1/h | Rate constant | Fitted data |
| S1 | 0.950 | - | Vascular reflection coefficients for Vtight | [12] | |
| S2 | 0.475 | 9.9 | - | Vascular reflection coefficients for Vleaky | Fitted data |
| SL | 0.2 | - | Lymphatic capillary reflection coefficients | [25] |
| Protein | Peptide | Q1 (m/z) | Q3 (m/z) | Fragment | DP (V) | EP (V) | CE (eV) | CXP (V) |
|---|---|---|---|---|---|---|---|---|
| Human IgG4 | SLSLSLGK | 403.0 (charge: 2) | 604.4 | y6 | 121 | 10 | 17 | 54 |
| SLSLSLG[K] | 407.0 (charge: 2) | 612.4 | y6 | 121 | 10 | 17 | 54 | |
| Interferon alpha | EDSILAVR | 451.8 (charge: 2) | 458.2 | y4 | 76 | 10 | 23 | 44 |
| EDSILAV[R] | 456.8 (charge: 2) | 468.2 | y4 | 76 | 10 | 23 | 44 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugimoto, H.; Chen, S.; Qian, M.G. Pharmacokinetic Characterization and Tissue Distribution of Fusion Protein Therapeutics by Orthogonal Bioanalytical Assays and Minimal PBPK Modeling. Molecules 2020, 25, 535. https://doi.org/10.3390/molecules25030535
Sugimoto H, Chen S, Qian MG. Pharmacokinetic Characterization and Tissue Distribution of Fusion Protein Therapeutics by Orthogonal Bioanalytical Assays and Minimal PBPK Modeling. Molecules. 2020; 25(3):535. https://doi.org/10.3390/molecules25030535
Chicago/Turabian StyleSugimoto, Hiroshi, Susan Chen, and Mark G. Qian. 2020. "Pharmacokinetic Characterization and Tissue Distribution of Fusion Protein Therapeutics by Orthogonal Bioanalytical Assays and Minimal PBPK Modeling" Molecules 25, no. 3: 535. https://doi.org/10.3390/molecules25030535