
Complicated Streptococcus agalactiae Sepsis with/without Meningitis in Young Infants and Newborns: The Clinical and Molecular Characteristics and Outcomes

 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and GBS Isolates
2.2. Definition
2.3. Capsular Serotyping and MLST
2.4. Antimicrobial Susceptibility Testing
2.5. Statistical Analysis
3. Results
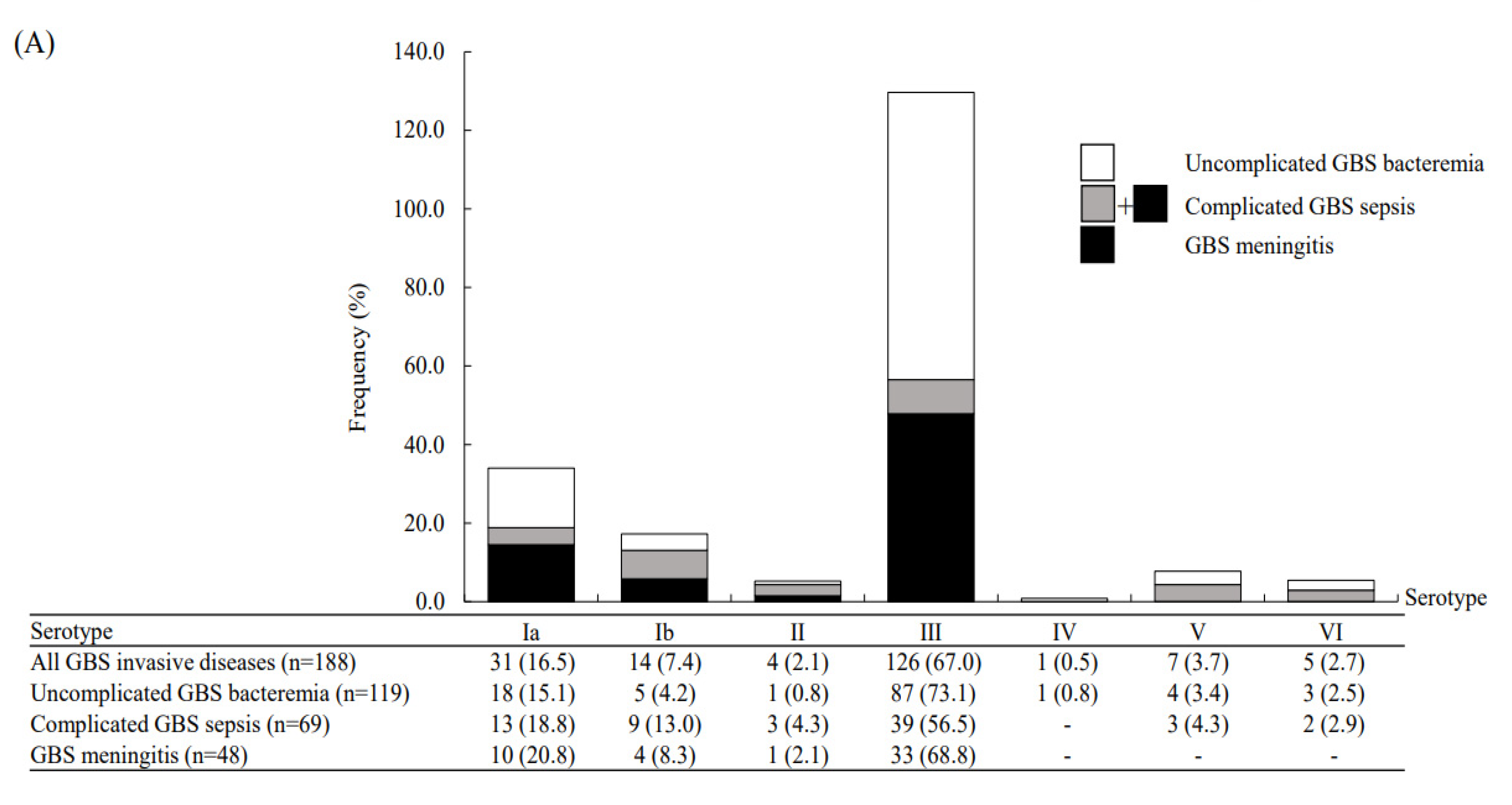
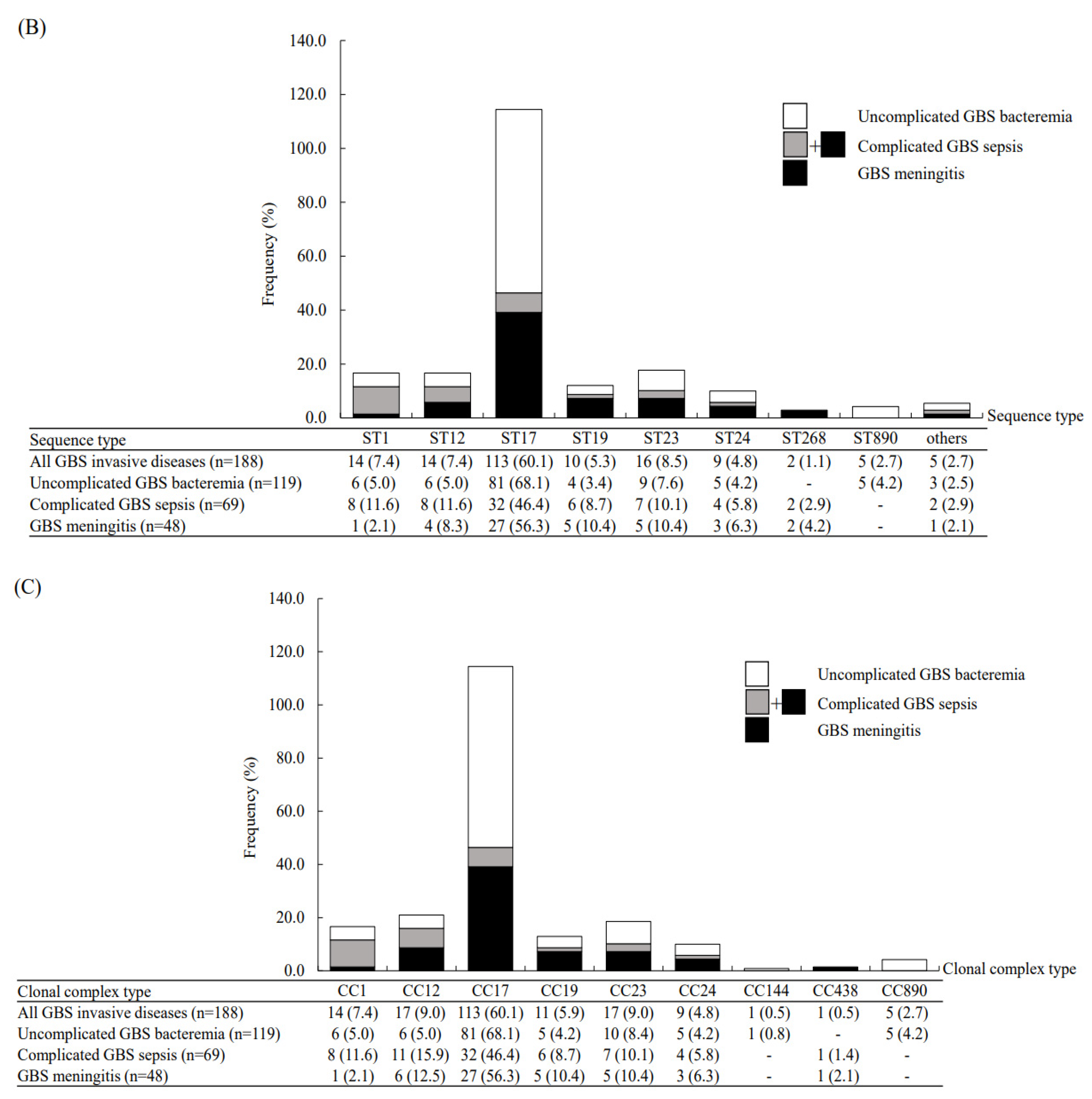
3.1. Complicated GBS Sepsis versus Uncomplicated GBS Bacteremia
3.2. Antimicrobial Susceptibility Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ouchenir, L.; Renaud, C.; Khan, S.; Bitnun, A.; Boisvert, A.A.; McDonald, J.; Bowes, J.; Brophy, J.; Barton, M.; Ting, J.; et al. The epidemiology, management, and outcomes of bacterial meningitis in infants. Pediatrics 2017, 140, e20170476. [Google Scholar] [CrossRef] [Green Version]
- Hasbun, R.; Wootton, S.H.; Rosenthal, N.; Balada-Llasat, J.M.; Chung, J.; Duff, S.; Bozzette, S.; Zimmer, L.; Ginocchio, C.C. Epidemiology of meningitis and encephalitis in infants and children in the United States, 2011–2014. Pediatr. Infect. Dis. J. 2019, 38, 37–41. [Google Scholar] [CrossRef]
- Romain, A.S.; Cohen, R.; Plainvert, C.; Joubrel, C.; Béchet, S.; Perret, A.; Tazi, A.; Poyart, C.; Levy, C. Clinical and laboratory features of group B streptococcus meningitis in infants and newborns: Study of 848 cases in France, 2001–2014. Clin. Infect. Dis. 2018, 66, 857–864. [Google Scholar] [CrossRef]
- Nanduri, S.A.; Petit, S.; Smelser, C.; Apostol, M.; Alden, N.B.; Harrison, L.H.; Lynfield, R.; Vagnone, P.S.; Burzlaff, K.; Spina, N.L.; et al. Epidemiology of invasive early-onset and late-onset Group B Streptococcal disease in the United States, 2006 to 2015, multistate laboratory and population-based surveillance. JAMA Pediatr. 2019, 173, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Mu, X.; Ji, W.; Yuan, C.; He, P.; Zhang, Y.; Huang, Y.; Li, J.; Chen, J.; Zhong, H.; et al. Epidemiology of invasive group B streptococcal disease in infants from urban area of South China, 2011–2014. BMC Infect. Dis. 2018, 18, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edmond, K.M.; Kortsalioudaki, C.; Scott, S.; Schrag, S.J.; Zaidi, A.K.M.; Cousens, S.; Heath, P. Group B streptococcal disease in infants aged younger than 3 months: Systemic review and meta-analysis. Lancet 2012, 379, 547–556. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.H.; Hsu, J.F.; Chu, S.M.; Lien, R.; Huang, H.R.; Chiang, M.C.; Fu, R.H.; Lee, C.W.; Huang, Y.C. Incidence, clinical characteristics and risk factors for adverse outcome in neonates with late-onset sepsis. Pediatr. Infect. Dis. J. 2014, 33, e7–e13. [Google Scholar] [CrossRef]
- Hsu, J.F.; Chu, S.M.; Huang, Y.C.; Lien, R.; Huang, H.R.; Lee, C.W.; Chiang, M.C.; Fu, R.H.; Tsai, M. Predictors of clinical and microbiological treatment failure in neonatal bloodstream infections. Clin. Microbiol. Infect. 2015, 21, 482.e9–482.e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.H.; Lee, C.W.; Chu, S.M.; Lee, I.T.; Lien, R.; Huang, H.R.; Chiang, M.C.; Fu, R.H.; Hsu, R.F.; Huang, Y.C. Infectious complications and morbidities after neonatal bloodstream infections: An observational cohort study. Medicine 2016, 95, e3078. [Google Scholar] [CrossRef]
- Hsu, M.H.; Hsu, J.F.; Kuo, H.C.; Lai, M.Y.; Chiang, M.C.; Lin, Y.J.; Huang, H.R.; Chu, S.M.; Tsai, M.H. Neurological complications in young infants with acute bacterial meningitis. Front. Neurol. 2018, 9, 903. [Google Scholar] [CrossRef]
- Kohli-Lynch, M.; Russell, N.J.; Seale, A.C.; Dangor, Z.; Tann, C.J.; Baker, C.J.; Bartlett, L.; Cutland, C.; Gravette, M.G.; Heath, P.T.; et al. Neurodevelopmental impairment in children after Group B Streptococcus disease worldwide: Systemic review and meta-analysis. Clin. Infect. Dis. 2017, 65, S190–S199. [Google Scholar] [CrossRef] [PubMed]
- Peros, T.; van Schuppen, J.; Bohte, A.; Hodiamont, C.; Aronica, E.; de Haan, T. Neonatal bacterial meningitis versus ventriculitis: A cohort-based overview of clinical characteristics, microbiology and imaging. Eur. J. Pediatr. 2020, 179, 1969–1977. [Google Scholar] [CrossRef] [PubMed]
- Nakwa, F.L.; Lala, S.G.; Madhi, S.A.; Dangor, Z. Neurodevelopmental impairment at 1 year of age in infants with previous invasive Group B Streptococci sepsis and meningitis. Pediatr. Infect. Dis. J. 2020, 39, 794–798. [Google Scholar] [CrossRef]
- Coon, E.R.; Srivastava, R.; Stoddard, G.; Wilkes, J.; Pavia, A.T.; Shah, S.S. Shortened IV antibiotic course for uncomplicated, late-onset Group B Streptococcal bacteremia. Pediatrics 2018, 142, e20180345. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.H.; Hsu, J.F.; Lai, M.Y.; Lin, L.C.; Chu, S.M.; Huang, H.R.; Chiang, M.C.; Fu, R.H.; Lu, J.J. Molecular characteristics and antimicrobial resistance of Group B Streptococcus Strains causing invasive disease in neonates and adults. Front. Microbiol. 2019, 10, 264. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Zhu, C.; Liu, X.; Ma, D.; Song, C.; Zhou, L.; Wang, Z.; Ou, Y.; Ma, W.; Shi, X.; et al. The etiology of acute meningitis and encephalitis syndromes in a sentinel pediatric hospital, Shenzhen, China. BMC Infect. Dis. 2019, 19, 560. [Google Scholar] [CrossRef]
- Erickson, T.A.; Munoz, F.M.; Troisi, C.L.; Nolan, M.S.; Hasbun, R.; Brown, E.L.; Murray, K.O. The epidemiology of meningitis in infants under 90 days of age in a large pediatric hospital. Microorganisms 2021, 9, 526. [Google Scholar] [CrossRef] [PubMed]
- African Neonatal Sepsis Trial (AFRINEST) Group; Tshefu, A.; Lokangaka, A.; Ngaima, S.; Engmann, C.; Esamai, F.; Gisore, P.; Ayede, A.I.; Falade, A.G.; Adejuyigbe, E.A.; et al. Simplified antibiotic regimens compared with injectable procaine benzylpenicilin plus gentamicin for treatment of neonates and young infants with clinical signs of possible series bacterial infection when referral is not possible: A randomized, open-label, equivalent trial. Lancet 2015, 385, 1767–1776. [Google Scholar]
- Obiero, C.W.; Mturi, N.; Mwarumba, S.; Ngari, M.; Newton, C.; Boele van Hensbroek, M.; Berkley, J.A. Clinical features to distinguish meningitis among young infants at a rural Kenyan hospital. Arch. Dis. Child. 2021, 106, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Vergnano, S.; Buttery, J.; Cailes, B.; Chandrasekaran, R.; Chiappini, E.; Clark, E.; Cutland, C.; Dourado de Andrade, S.; Esteve-Jaramillo, A.; Guinazu, J.R.; et al. Neonatal infections: Case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2016, 34, 6038–6046. [Google Scholar] [CrossRef] [Green Version]
- Jim, K.K.; Brouwer, M.C.; van der Ende, A.; van de Beek, D. Subdural emphyme in bacterial meningitis. Neurology 2012, 79, 2133–2139. [Google Scholar] [CrossRef]
- Tien, N.; Ho, C.M.; Lin, H.J.; Shih, M.C.; Ho, M.W.; Lin, H.C.; Lin, H.S.; Chang, C.C.; Lu, J.J. Multilocus sequencing typing of invasive group B streptococcus in central area of Taiwan. J. Microbiol. Immunol. Infect. 2011, 44, 430–434. [Google Scholar] [CrossRef] [Green Version]
- Manning, S.D.; Springman, A.C.; Lehotzky, E.; Lewis, M.A.; Whittam, T.S.; Davies, H.D. Multilocus sequence types associated with neonatal group B streptococcal sepsis and meningitis in Canada. J. Clin. Microbiol. 2009, 47, 1143–1148. [Google Scholar] [CrossRef] [Green Version]
- Matuschek, E.; Ahman, J.; Webster, C.; Kahlmeter, G. Antimicrobial susceptibility testing of colistin-evolution of seven commercial MIC products against standard broth microdilution for Escherichia coli, Klebsiella pneumonia, Pseudomonas aeruginosa, and Acinetobacter spp. Clin. Microbiol. Infect. 2018, 24, 865–870. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, Twenty-Fourth Informational Supplement, M100-S24; SLCI: Wayne, MI, USA, 2014. [Google Scholar]
- Bekker, V.; Bijlsma, M.W.; van de Beek, D.; Kuijpers, T.W.; van der Ende, A. Incidence of invasive group B streptococcal disease and pathogen genotype distribution in newborn babies in the Netherlands over 25 years: A nationwide surveillance study. Lancet. Infect. Dis. 2014, 14, 1083–1089. [Google Scholar] [CrossRef]
- Zurn, K.; Lander, F.; Hufnagel, M.; Monecke, S.; Berner, R. Microaray analysis of Group B Streptococci causing invasive neonatal early and late-onset infection. Pediatr. Infect. Dis. J. 2020, 39, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Hartley, J.; Li, Y.; Kunkel, L.; Crowcroft, N.S. The burden of infant group B streptococcal infections in Ontario: Analysis of administrative data to estimate the potential benefits of new vaccines. Hum. Vaccin. Immunother. 2019, 15, 193–202. [Google Scholar] [CrossRef]
- Lo, C.W.; Liu, H.C.; Lee, C.C.; Lin, C.L.; Chen, C.L.; Jeng, M.J.; Chiu, C.H. Serotype distribution and clinical correlation of Streptococcus agalactiae causing invasive disease in infants and children in Taiwan. J. Microbiol. Immunol. Infect. 2019, 52, 578–584. [Google Scholar] [CrossRef]
- Ali, M.M.; Woldeamanuel, Y.; Woldetsadik, D.A.; Chaka, T.E.; Fenta, D.A.; Dinberu, M.T.; Weldetensaye, E.K.; Ismael, S.J.; Tadesse, B.T. Prevalence of group B streptococcus among pregnant women and newborns at Hawassa University comprehensive specialized hospital, Hawassa, Ethiopia. BMC Infect. Dis. 2019, 19, 325. [Google Scholar] [CrossRef] [PubMed]
- Horvath-Puho, E.; van Kassel, M.N.; Goncalves, B.P.; de Gier, B.; Procter, S.R.; Paul, P.; van der Ende, A.; Sogarrd, K.K.; Hahne, S.J.M.; Chandna, J.; et al. Mortality, neurodevelopmental impairments, and economic outcomes after invasive group B streptococcal disease in early infancy in Denmark and the Netherlands: A national matched cohort study. Lancet Child Adolesc. Health 2021, 5, 398–407. [Google Scholar] [CrossRef]
- Lohrmann, F.; Berg, A.; Wicker, E.; Imm, A.; Krause, G.; Zurn, K.; Berner, R.; Hufnagel, M.; Lander, F. Prevalence of capsular serotype, pilus island distribution, and antibiotic resistance in pediatric and adult invasive group B streptococcus isolates: Data from a nationwide prospective surveillance study in Germany. Pediatr. Infect. Dis. J. 2021, 40, 76–82. [Google Scholar] [CrossRef]
- Kadambari, S.; Trotter, C.L.; Heath, P.T.; Goldacre, M.J.; Pollard, A.J.; Goldacre, R. Group B streptococcal disease in England (1998–2017): A population-based observational study. Clin. Infect. Dis. 2021, 72, e791–e798. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.Y.; Wang, D.Y.; Li, H.T.; Liu, J.M. Screening-based and risk-based strategy for the prevention of early-onset Group B Streptococcus/Non-group B Streptococcus sepsis in the neonates: A systemic review and meta-analysis. Pediatr. Infect. Dis. J. 2020, 39, 740–748. [Google Scholar] [CrossRef]
- Keij, F.M.; Achten, N.B.; Tramper-Stranders, G.A.; Allegaert, K.; van Rossum, A.M.C.; Reiss, I.K.M.; Kornelisse, R.F. Stratified management for bacterial infections in late preterm and term neonates: Current strategies and future opportunities toward precision medicine. Front. Pediatr. 2021, 9, 590969. [Google Scholar] [CrossRef] [PubMed]
- Armistead, B.; Oler, E.; Adams Waldorf, K.; Rajagopal, L. The double life of group B Streptococcus: Asymptomatic colonizer and potent pathogen. J. Mol. Biol. 2019, 431, 2914–2931. [Google Scholar] [CrossRef] [PubMed]
- Gofton, T.E.; Young, G.B. Sepsis-associated encephalopathy. Nat. Rev. Neurol. 2012, 8, 557–566. [Google Scholar] [CrossRef]
- Chu, S.M.; Hsu, J.F.; Lee, C.W.; Reyin, L.; Huang, H.R.; Chiang, M.C.; Fu, R.H.; Tsai, M.H. Neurological complications after neonatal bacteremia: The clinical characteristics, risk factors and outcomes. PLoS ONE 2014, 9, e105294. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Zhai, Q.; Ooi, K.; Cao, Y.; Qiao, Z. Risk factors for hydrocephalus in neonatal purulent meningitis: A single-center retrospective analysis. J. Child Neurol. 2021, 36, 491–497. [Google Scholar] [CrossRef]
- Lin, C.H.; Lin, W.D.; Chou, I.C.; Lee, I.C.; Hong, S.Y. Epilepsy and neurodevelopmental outcomes in children with etiologically diagnosed central nervous system infections: A retrospective cohort study. Front. Neurol. 2019, 10, 528. [Google Scholar] [CrossRef]
- Pappas, A.; Adams-Chapman, I.; Shankaran, S.; McDonald, S.A.; Stoll, B.J.; Laptook, A.R.; Carlo, W.A.; Van Meurs, K.P.; Hintz, S.R.; Carlson, M.D.; et al. Neurodevelopmental and behavioral outcomes in extremely premature neonates with ventriculomegaly in the absence of periventricular intraventricular hemorrhage. JAMA Pediatr. 2018, 172, 32–42. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, W.J.; Zhu, L.; Xu, L.J.; Guo, C.; Zhang, X.H.; Liu, Q.H.; Ma, L. Emergence of invasive serotype Ib sequence type 10 group B streptococcus disease in Chinese infants is driven by a tetracycline-sensitive clone. Front. Cell Infect. Microbiol. 2021, 11, 642455. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.; Liu, H.; Madhi, S.A.; Cunnington, M.; Zhang, Z.; Dangor, Z.; Zhou, H.; Mu, X.; Jin, Z.; Wang, A.; et al. Clinical and molecular epidemiology of invasive group B streptococcus disease among infants, China. Emerg. Infect. Dis. 2019, 25, 2021–2030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Ma, L.; Zhu, L.; Zhou, X.H.; Xu, L.J.; Guo, C.; Meng, J.H.; Zhang, X.H.; Liu, Q.H.; Huang, R. Molecular characterization of pathogenic group B streptococcus from a tertiary hospital in Shanxi, China: High incidence of sequence type 10 strains in infants/pregnant women. J. Microbiol. Immunol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | All Cases (Total n = 188) | Complicated GBS Infections with/without Meningitis (Total n = 69) | Uncomplicated GBS Bacteremia (Total n = 119) | p Values |
|---|---|---|---|---|
| Gestational age (week), median (IQR) | 38.0 (36.3–39.0) | 38.0 (36.0–39.0) | 39.0 (37.0–40.0) | 0.049 |
| Birth body weight (g), median (IQR) | 2885.0 (2551–3235) | 2750.0 (2490–3120) | 2960.0 (2640–3305) | 0.039 |
| Gender, (male/female, n/%) | 81 (43.1)/107 (56.9) | 31 (44.9)/38 (55.1) | 50 (42.0)/69 (58.0) | 0.761 |
| Birth by NSD/Cesarean section, n (%) | 130 (69.1)/58 (30.9) | 45 (65.2)/24 (34.8) | 85 (71.4)/34 (28.6) | 0.414 |
| 5 min Apgar score < 7, n (%) | 12 (6.4) | 6 (8.7) | 6 (5.0) | 0.362 |
| Premature rupture of membrane, n (%) | 35 (18.6) | 20 (29.0) | 15 (12.6) | 0.007 |
| Onset of GBS bacteremia (day), median (IQR) | 25.5 (9.3–53.8) | 18.0 (2.0–32.5) | 30.0 (15.0–56.0) | 0.001 |
| Early-onset sepsis (≤7 days), n (%) | 44 (23.4) | 26 (37.7) | 18 (15.1) | 0.002 |
| Late-onset sepsis (8–90 days), n (%) | 133 (70.7) | 40 (58.0) | 93 (78.2) | 0.002 |
| Very late-onset sepsis (>90 days), n (%) | 11 (5.9) | 3 (4.3) | 8 (6.7) | 0.142 |
| Clinical features *, n (%) | ||||
| Fever (≥38.3 ℃) | 153 (81.4) | 49 (71.0) | 104 (87.4) | 0.007 |
| Apnea, bradycardia and/or cyanosis | 67 (35.6) | 54 (78.3) | 13 (10.9) | <0.001 |
| Ventilator requirement | <0.001 | |||
| Room air or nasal canuala | 124 (66.0) | 23 (33.3) | 101 (84.9) | |
| Non-invasive ventilator (N-CPAP and N-IMV) | 18 (9.6) | 3 (4.3) | 15 (12.6) | |
| Intubation | 37 (19.7) | 34 (49.3) | 3 (2.5) | |
| High-frequency oscillatory ventilator | 9 (4.8) | 9 (13.0) | 0 (0) | |
| Abdominal distension and/or vomiting | 71 (37.8) | 40 (58.0) | 31 (26.1) | <0.001 |
| Hypoglycemia | 22 (11.7) | 13 (18.8) | 9 (7.6) | 0.032 |
| Hypotension | 34 (18.1) | 33 (47.8) | 1 (0.8) | <0.001 |
| Severe sepsis | 39 (33.1) | 39 (56.5) | 0 (0) | <0.001 |
| Disseminated intravascular coagulopathy | 13 (6.9) | 13 (18.8) | 0 (0) | <0.001 |
| Requirement of blood transfusion ** | 88 (46.8) | 38 (55.1) | 50 (42.0) | 0.096 |
| Laboratory data at onset of GBS bacteremia, n (%) | ||||
| Leukocytosis (WBC > 20,000/L) | 110 (58.5) | 35 (50.7) | 75 (63.0) | 0.125 |
| Leukopenia (WBC < 4000/L) | 41 (21.8) | 24 (34.8) | 17 (14.3) | 0.002 |
| Shift to left in WBC (immature > 20%) | 23 (12.2) | 11 (15.9) | 12 (10.1) | 0.255 |
| Anemia (hemoglobin level < 11.5 g/dL) | 97 (51.6) | 38 (55.1) | 59 (49.6) | 0.545 |
| Thrombocytopenia (platelet < 150,000/μL) | 31 (16.5) | 24 (34.8) | 7 (5.9) | <0.001 |
| Metabolic acidosis | 27 (14.4) | 23 (33.3) | 4 (3.4) | <0.001 |
| Coagulopathy | 30 (16.0) | 27 (39.1) | 3 (2.5) | <0.001 |
| C-reactive protein (mg/dL), median (IQR) | 40.7 (10.8–104.0) | 83.2 (21.7–167.9) | 20.4 (7.0–57.6) | <0.001 |
| Neurological Complications, Sequelae and Death | Neonates with Complicated GBS Sepsis and Meningitis (n = 48) | Neonates with Severe Sepsis and/or Septic Shock (n = 21) |
|---|---|---|
| Any neurological complications | 37 (77.8) | 8 (38.1) |
| Seizure | 22 (45.8) | 5 (23.8) |
| Subdural effusion | 16 (33.3) | 1 (4.8) |
| Increased intracranial pressure | 12 (25.0) | 7 (33.3) |
| Ventriculomegaly | 17 (35.4) | 0 (0) |
| Hydrocephalus | 6 (12.5) | 1 (4.8) |
| Encephalomalacia | 6 (12.5) | 0 (0) |
| Subependymal hemorrhage | 5 (10.4) | 2 (9.5) |
| Intraventricular hemorrhage | 4 (8.3) | 4 (19.0) |
| Ventriculitis | 4 (8.3) | 0 (0) |
| Periventricular leukomalacia | 1 (2.1) | 1 (4.8) |
| Infarction | 5 (10.4) | 0 (0) |
| Subdural empyema or abscess | 2 (4.2) | 0 (0) |
| Brain atrophy | 1 (2.1) | 0 (0) |
| Discharge with neurological sequelae | 17 (35.4) | 4 (19.0) |
| Final in-hospital mortality | 7 (14.6) | 12 (57.1) |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | |
| Preterm birth (GA < 37 weeks) | 2.52 (1.19–5.31) | 0.015 | 0.70 (0.24–2.08) | 0.525 |
| Septic shock | 20.7 (8.41–50.97) | <0.001 | 1.40 (0.32–6.11) | 0.654 |
| Respiratory failure (requirement of intubation) | 24.75 (10.23–59.91) | <0.001 | 14.97 (3.31–67.79) | <0.001 |
| Type III/CC-17 GBS isolates | 0.24 (0.12–0.50) | <0.001 | ||
| Type Ib/CC-12 GBS isolates | 5.92 (1.92–18.24) | 0.002 | 2.11 (0.45–9.88) | 0.344 |
| Early-onset sepsis | 3.84 (1.81–8.15) | <0.001 | 1.70 (0.70–2.42) | 0.570 |
| Leukopenia (WBC count < 5000 cells/μL) | 2.41 (1.12–5.22) | 0.025 | 0.77 (0.23–2.52) | 0.660 |
| Anemia (hemoglobin level < 11.5 mg/dL) | 1.35 (0.67–2.74) | 0.401 | ||
| Thrombocytopenia (platelet count < 150,000/μL) | 13.8 (5.65–33.68) | <0.001 | 6.19 (1.88–20.33) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.; Chu, S.-M.; Wang, H.-C.; Yang, P.-H.; Huang, H.-R.; Chiang, M.-C.; Fu, R.-H.; Tsai, M.-H.; Hsu, J.-F. Complicated Streptococcus agalactiae Sepsis with/without Meningitis in Young Infants and Newborns: The Clinical and Molecular Characteristics and Outcomes. Microorganisms 2021, 9, 2094. https://doi.org/10.3390/microorganisms9102094
Lin C, Chu S-M, Wang H-C, Yang P-H, Huang H-R, Chiang M-C, Fu R-H, Tsai M-H, Hsu J-F. Complicated Streptococcus agalactiae Sepsis with/without Meningitis in Young Infants and Newborns: The Clinical and Molecular Characteristics and Outcomes. Microorganisms. 2021; 9(10):2094. https://doi.org/10.3390/microorganisms9102094
Chicago/Turabian StyleLin, Chih, Shih-Ming Chu, Hsiao-Chin Wang, Peng-Hong Yang, Hsuan-Rong Huang, Ming-Chou Chiang, Ren-Huei Fu, Ming-Horng Tsai, and Jen-Fu Hsu. 2021. "Complicated Streptococcus agalactiae Sepsis with/without Meningitis in Young Infants and Newborns: The Clinical and Molecular Characteristics and Outcomes" Microorganisms 9, no. 10: 2094. https://doi.org/10.3390/microorganisms9102094