
Serotype Distribution of Remaining Pneumococcal Meningitis in the Mature PCV10/13 Period: Findings from the PSERENADE Project

 , , , , , , , , , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Site Identification and Eligibility
2.2. Defining Serotype Categories
2.3. Analytic Model
3. Results
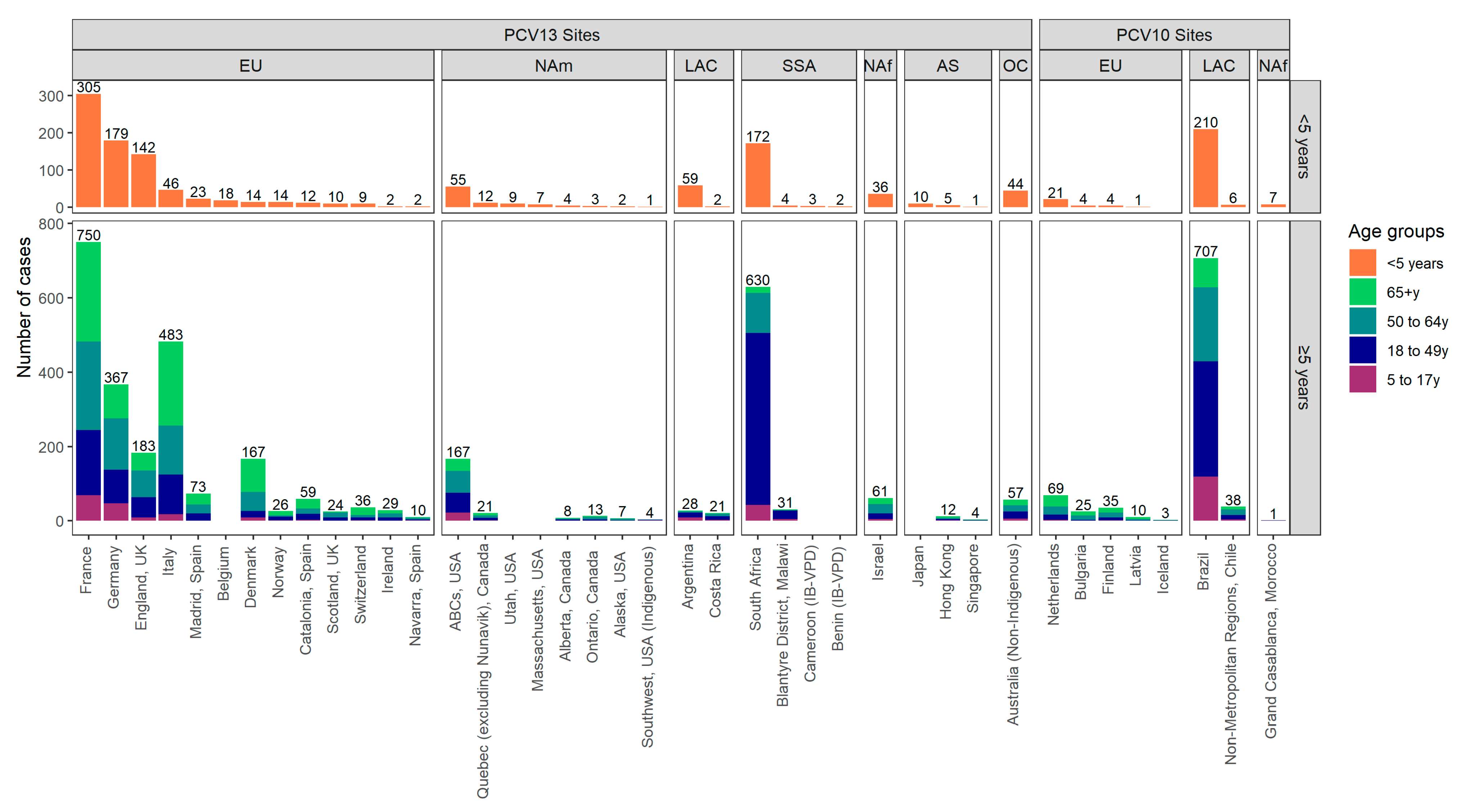
3.1. Data Included
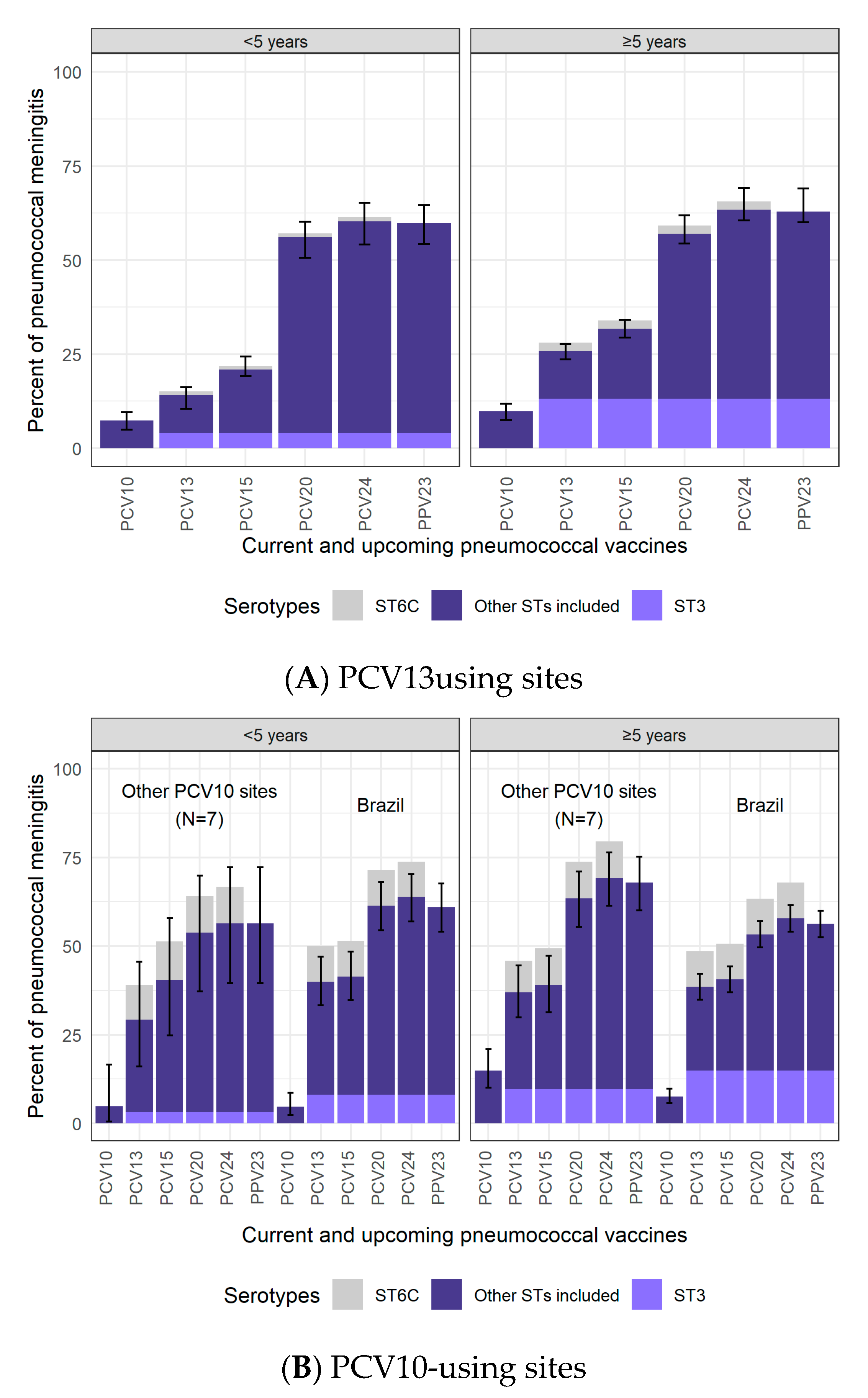
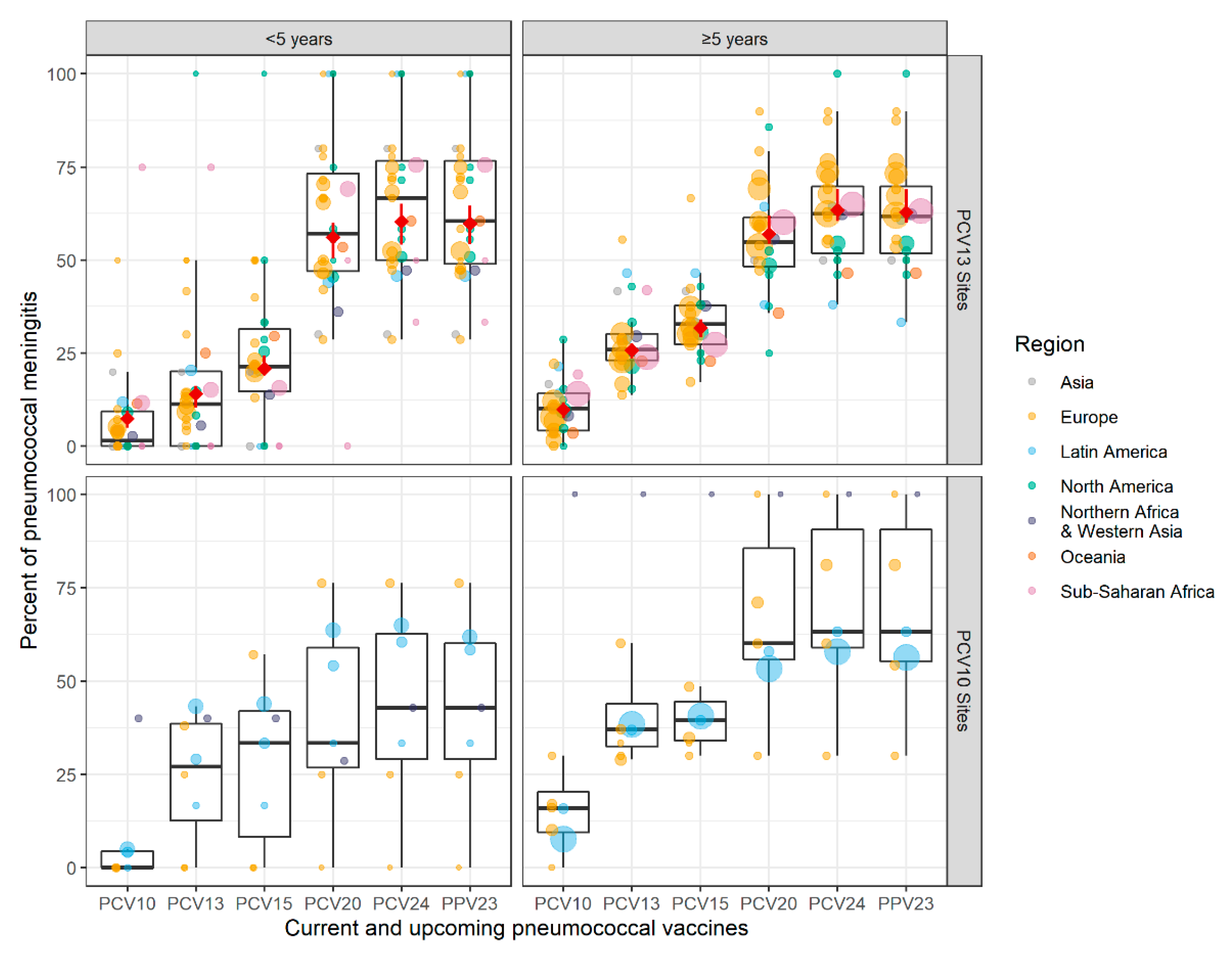
3.2. Pneumococcal Meningitis Due to Vaccine-Type Serotypes
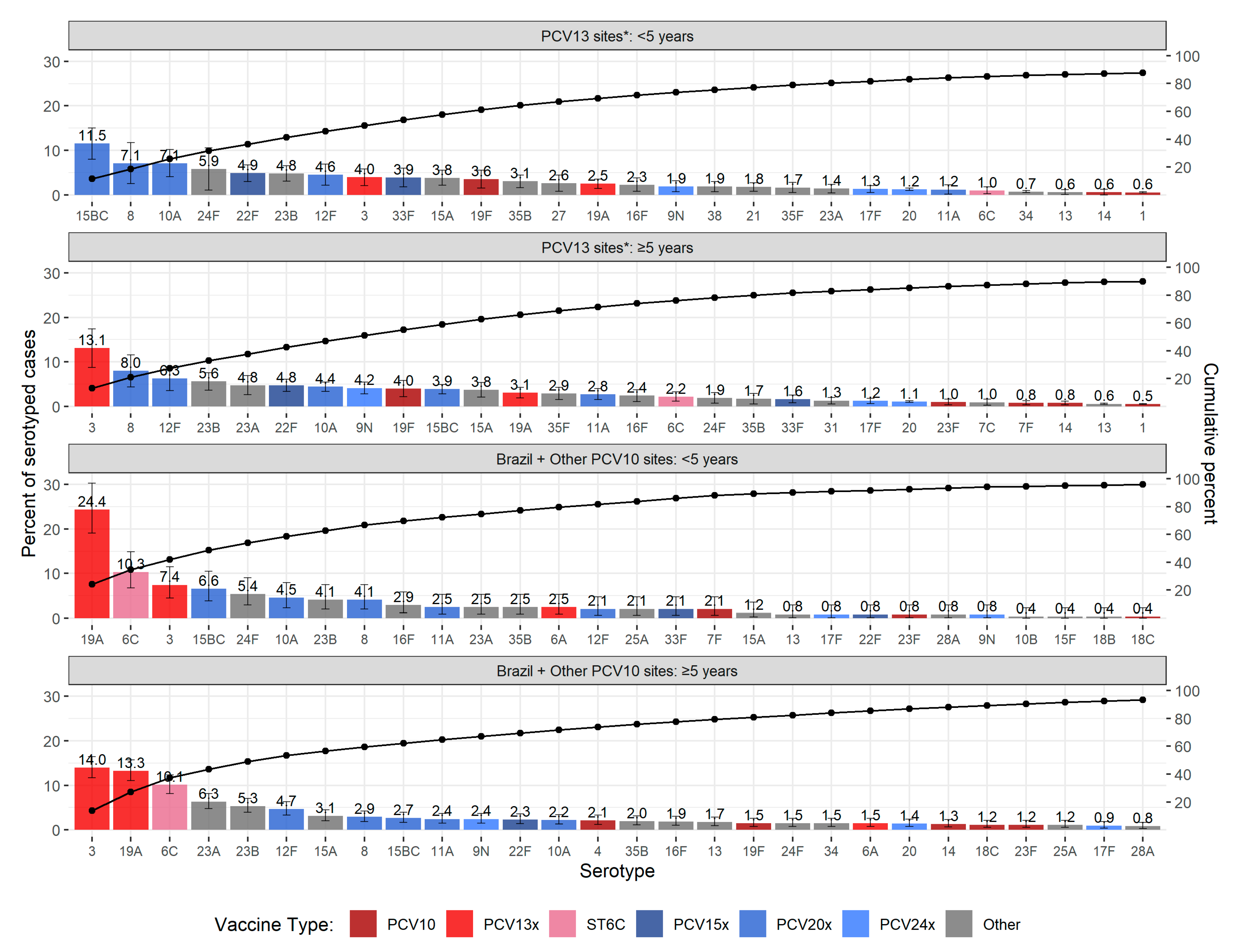
3.3. Serotype Distribution
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Affiliation |
|---|---|
| Zahin Amin-Chowdhury | Immunisation and Countermeasures Division, Public Health England, London NW9 5EQ, UK |
| Rita Born | Federal Office of Public Health, 3097 Liebefeld, Switzerland |
| Maria-Cristina C. Brandileone | National Laboratory for Meningitis and Pneumococcal Infections, Center of Bacteriology, Institute Adolfo Lutz (IAL), São Paulo 01246-902, Brazil |
| Dana Bruden | Arctic Investigations Program, Division of Preparedness and Emerging Infections, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention, Anchorage, AK 99508, USA |
| Carrie L. Byington | University of Utah Department of Pediatrics (emeritus), Salt Lake City, UT 84108, United States; University of California Health System, Oakland, CA 94607, USA |
| Claire Cameron | Public Health Scotland, Glasgow G2 6QE, UK |
| Jesús Castilla | Instituto de Salud Pública de Navarra—IdiSNA, 31003 Pamplona, Navarra, Spain; CIBER Epidemiología y Salud Pública, (CIBERESP), 28029 Madrid, Spain |
| Guanhao Chan | Singapore Ministry of Health, Communicable Diseases Division, Singapore 308442, Singapore |
| Kin-Hung Chow | Department of Microbiology and Carol Yu Centre for Infection, Queen Mary Hospital, The University of Hong Kong, Hong Kong SAR, China |
| Tine Dalby | Bacteria, Parasites and Fungi, Statens Serum Institut, DK-2300 Copenhagen S, Denmark |
| Kostas Danis | Santé Publique France, the French National Public Health Agency, Saint Maurice CEDEX, 94415 Paris, France |
| Linda de Gouveia | Centre for Respiratory Diseases and Meningitis, National Institute for Communicable Diseases of the National Health Laboratory Service, Sandringham, 2192 Johannesburg, South Africa |
| Sara de Miguel | Epidemiology Department, Dirección General de Salud Pública, 28009 Madrid, Spain |
| Geneviève Deceuninck | Quebec University Hospital Research Centre, Québec, QC G1V 4G2, Canada |
| Martina Del Manso | Department of Infectious Diseases, Italian National Institute of Health (Istituto Superiore di Sanità, ISS), 00161 Rome, Italy |
| Janepsy Díaz | Instituto de Salud Pública de Chile, 7780050 Santiago, Santiago Metropolitan, Chile |
| Elina Dimina | Centre for disease prevention and control of Latvia, 1005 Riga, Latvia |
| Helga Erlendsdottir | Department of Clinical Microbiology, Landspitali—The National University Hospital, Hringbraut, 101 Reykjavik, Iceland |
| Noga Givon-Lavi | Pediatric Infectious Disease Unit and Clinical Microbiology Laboratory, Soroka University Medical Center, Ben-Gurion University of the Negev, Beer-Sheva 8410501, Israel |
| James D. Kellner | Department of Pediatrics, University of Calgary, and Alberta Health Services, Calgary, AB T3B 6A8, Canada |
| Mirjam J. Knol | National Institute for Public Health and the Environment, 3721 MA Bilthoven, The Netherlands |
| Brigitte Lefebvre | Laboratoire de Santé Publique du Québec, Sainte-Anne-de-Bellevue, Quebec City, QC H9X 3R5, Canada |
| Jolita Mereckiene | HSE Health Protection Surveillance Centre, Mountjoy, D01 A4A3 Dublin, Ireland |
| Carmen Muñoz-Almagro | Molecular Microbiology Department, Hospital Sant Joan de Déu Research Institute, 08950 Esplugues de Llobregat, Barcelona, Spain; Medicine Department, Universitat Internacional de Catalunya, 08017 Barcelona, Spain; CIBER Epidemiología y Salud Pública (CIBERESP), 28029 Madrid, Spain |
| Daniela Napoli | Servicio de Bacteriología Clínica, Departamento de Bacteriología, INEI—ANLIS “Dr. Carlos G. Malbrán”, C1282 AFF Buenos Aires, Argentina |
| Néhémie Nzoyikorera | Department of Microbiology, Faculty of Medicine and Pharmacy, Hassan II University of Casablanca, Casablanca 20000, Morocco; Bacteriology-Virology and Hospital Hygiene Laboratory, Ibn Rochd University Hospital Centre, Casablanca 20250, Morocco |
| Stephen I. Pelton | Boston University Schools of Medicine and Public Health, Boston, MA 02118, USA |
| Kate Pennington | Communicable Disease Epidemiology and Surveillance Section, Office of Health Protection, Australian Government Department of Health, Canberra, ACT 2606, Australia |
| Tamara Pilishvili | National Center for Immunizations and Respiratory Diseases, Centers for Disease Control and Prevention, Atlanta, GA 30333, USA |
| Marie-Cecile Ploy | University Hospital Centre Limoges, Regional Observatories for Pneumococci, 87000 Limoges, France |
| Rodrigo Puentes | Instituto de Salud Pública de Chile, 7780050 Santiago, Santiago Metropolitan, Chile |
| Shigeru Suga | Infectious Disease Center and Department of Clinical Research, National Hospital Organization Mie Hospital, Tsu, Mie 514-0125, Japan |
| Catherine G. Sutcliffe | Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA |
| Todd D. Swarthout | NIHR Global Health Research Unit on Mucosal Pathogens, Division of Infection and Immunity, UCL, Bloomsbury, London WC1E 6BT, UK; Malawi-Liverpool-Wellcome Trust Clinical Research Programme, P.O. Box 30096, Chichiri, Blantyre 3, Malawi |
| Koh Cheng Thoon | KK Women’s and Children’s Hospital, Singapore 229899, Singapore |
| Maija Toropainen | Department of Health Security, Finnish Institute for Health and Welfare, 00271 Helsinki, Finland |
| Didrik F. Vestrheim | Department of Infection Control and Vaccine, Norwegian Institute of Public Health, 0456 Oslo, Norway |
| Anne von Gottberg | Centre for Respiratory Diseases and Meningitis, National Institute for Communicable Diseases of the National Health Laboratory Service, Sandringham, 2192 Johannesburg, South Africa; School of Pathology, Faculty of Health Sciences, University of the Witwatersrand, Braamfontein 2000, Johannesburg, South Africa |
| Toronto Invasive Bacterial Diseases Network | |
| WHO Invasive Bacterial Vaccine-Preventable Diseases (IB-VPD) Network |
| PSERENADE Technical Advisory Group |
| Thomas Cherian |
| William P. Hausdorff |
| Marc Lipsitch |
| Shabir A. Madhi |
| Elizabeth Miller |
| Catherine Satzke |
| Cynthia G. Whitney |
| World Health Organization |
| Katherine L. O’Brien |
| Jenny A. Walldorf |
| Johns Hopkins University |
| Yunfeng Cao |
| Peggy Gross |
| Donna Hesson |
| Marissa Hetrich |
| Ananya Kumar |
| Kate Perepezko |
| E. Wangeci Kagucia |
| Francesca Schiaffino Salazar |
| Jenna Sinkevitch |
| Daniel Stephens |
| Epiconcept |
| Camelia Savulescu |
| European Centre for Disease Prevention and Control |
| Edoardo Colzani |
| Pan American Health Organization |
| Lúcia Helena de Oliveira |
| Epidemiology Department, Dirección General de Salud Pública, Comunidad de Madrid, Madrid, Spain |
| Luis García Comas |
| Maria Ordobás Gavín |
| Department of Infectious Diseases, Italian National Institute of Health (Istituto Superiore di Sanità, ISS), Rome, Italy |
| Flavia Riccardo |
| Surveillance and Public Health Emergency Response, Public Health Agency of Catalonia, Barcelona, Spain |
| Sonia Broner |
| Conchita Izquierdo |
| Laboratoire du Centre Mère et Enfant Fondation Chantal Biya, Yaoundé, Cameroun |
| Angeline Boula |
| University of Parakou, Alibori in PARAKOU, Benin |
| Joseph Agossou |
| WHO Collaborating Centre for New Vaccines Surveillance, Medical Research Council Unit The Gambia at London School of Hygiene and Tropical Medicine, Banjul, The Gambia |
| Brenda A. Kwambana-Adams |
| Martin Antonio |
| Archibald Worwui |
| Peter S. Ndow |
| WHO Regional Office for Africa, Inter Country Support Team, Ouagadougou, Burkina Faso |
| Joseph Biey |
| Bernard Ntsama |
| WHO Regional Office for Africa, Inter Country Support Team, Libreville, Gabon |
| Gilson Paluku |
| Aboubacar N’DIAYE |
| WHO Country offices, Benin and Cameroon |
| Sentinel site surveillance teams and countries part of the African Pediatric Bacterial Meningitis Surveillance Network |
| Australian National Notifiable Diseases Surveillance data were provided by the Office of Health Protection, Australian Government Department of Health, on behalf of the Communicable Diseases Network Australia and the Enhanced Invasive Pneumococcal Disease Surveillance Working Group. |
References
- Wahl, B.; O’Brien, K.L.; Greenbaum, A.; Majumder, A.; Liu, L.; Chu, Y.; Lukšić, I.; Nair, H.; McAllister, D.A.; Campbell, H.; et al. Burden of Streptococcus Pneumoniae and Haemophilus Influenzae Type b Disease in Children in the Era of Conjugate Vaccines: Global, Regional, and National Estimates for 2000–2015. Lancet Glob. Health 2018, 6, e744–e757. [Google Scholar] [CrossRef] [Green Version]
- Johnson, H.L.; Deloria-Knoll, M.; Levine, O.S.; Stoszek, S.K.; Hance, L.F.; Reithinger, R.; Muenz, L.R.; O’Brien, K.L. Systematic Evaluation of Serotypes Causing Invasive Pneumococcal Disease among Children Under Five: The Pneumococcal Global Serotype Project. PLoS Med. 2010, 7, e1000348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Vaccine Access Center (IVAC), Johns Hopkins Bloomberg School of Public Health VIEW-Hub. Available online: https://view-hub.org (accessed on 29 December 2020).
- Lucero, M.; Dulalia, V.; Nillos, L.; Williams, G.; Parreño, R.; Nohynek, H.; Riley, I.; Makela, H. Pneumococcal Conjugate Vaccines for Preventing Vaccine-Type Invasive Pneumococcal Disease and Pneumonia with Consolidation on X-ray in Children under Two Years of Age. Cochrane Database Syst. Rev. 2004, 4, CD004977. [Google Scholar] [CrossRef]
- Cherian, T.; Cohen, M.; de Oliveira, L.; Farrar, J.L.; Goldblatt, D.; Knoll, M.; Moisi, J.C.; O’Brien, K.L.; Pilishvili, T.; Ramakrishnan, M.; et al. Pneumococcal Conjugate Vaccine (PCV) Review of Impact Evidence (PRIME): Summary of Findings from Systematic Review; Report to Strategic Advisory Group of Experts on Immunization (SAGE) of the World Health Organization; WHO: Geneva, Switzerland, 2017; Volume 1, pp. 1–215. [Google Scholar]
- Dagan, R. Relationship between Immune Response to Pneumococcal Conjugate Vaccines in Infants and Indirect Protection after Vaccine Implementation. Expert Rev. Vaccines 2019, 18, 641–661. [Google Scholar] [CrossRef] [PubMed]
- Feikin, D.R.; Kagucia, E.W.; Loo, J.D.; Link-Gelles, R.; Puhan, M.A.; Cherian, T.; Levine, O.S.; Whitney, C.G.; O’Brien, K.L.; Moore, M.R.; et al. Serotype-Specific Changes in Invasive Pneumococcal Disease after Pneumococcal Conjugate Vaccine Introduction: A Pooled Analysis of Multiple Surveillance Sites. PLoS Med. 2013, 10, e1001517. [Google Scholar] [CrossRef] [Green Version]
- Falkenhorst, G.; Remschmidt, C.; Harder, T.; Hummers-Pradier, E.; Wichmann, O.; Bogdan, C. Effectiveness of the 23-Valent Pneumococcal Polysaccharide Vaccine (PPV23) against Pneumococcal Disease in the Elderly: Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169368. [Google Scholar] [CrossRef]
- Franklin, K.; Ronveaux, O.; Fernandez, K.; Kwambana-Adams, B.; Lessa, F.C.; Soeters, H.M.; Copper, L.; Coldiron, M.E.; Mwenda, J.; Antonio, M.; et al. Pneumococcal Meningitis Outbreaks in Africa, 2000–2018: Systematic Literature Review and Meningitis Surveillance Database Analyses; Systematic Review Registration (PROSPERO) Number: 102614 (interim number); 2020. [Google Scholar]
- Merck Sharp & Dohme Corp. Merck Submits Applications for Licensure of V114, the Company’s Investigational 15-Valent Pneumococcal Conjugate Vaccine, for Use in Adults to the U.S. FDA and European Medicines Agency. Available online: https://www.merck.com/news/merck-submits-applications-for-licensure-of-v114-the-companys-investigational-15-valent-pneumococcal-conjugate-vaccine-for-use-in-adults-to-the-u-s-fda-and-european-medicines-agency/ (accessed on 10 December 2020).
- Pfizer. A Phase 3, Randomized, Open-Label Trial to Evaluate the Safety and Immunogenicity of a 20-Valent Pneumococcal Conjugate Vaccine in Adults 65 Years of Age and Older with Prior Pneumococcal Vaccination. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT03835975 (accessed on 20 December 2020).
- Skinner, J.; Kaufhold, R.; McGuinness, D. Immunogenicity of PCV24, a next Generation Pneumococcal Conjugate Vaccine. In Proceedings of the 11th International Symposium on Pneumococci and Pneumococcal Diseases, Melbourne, Australia, 15 April 2018. [Google Scholar]
- Affinivax. Affinivax Announces the Presentation of Phase 1 Clinical Data for Its MAPSTM Vaccine for Streptococcus Pneumoniae at IDWeek 2020. Available online: https://affinivax.com/press-release-october-21-2020/ (accessed on 10 December 2020).
- World Health Organization. Global Vaccine Action Plan: Defeating Meningitis by 2030 Meningitis Prevention and Control; World Health Organization Seventy-third World Health Assembly: Geneva, Switzerland, 2020; pp. 1–4. [Google Scholar]
- Deloria-Knoll, M.; Bennett, J.C.; Garcia Quesada, M.; Kagucia, E.W.; Peterson, M.E.; Feikin, D.R.; Cohen, A.L.; Hetrich, M.K.; Yangyupei, Y.; Sinkevitch, J.N.; et al. Global Landscape Review of Serotype-Specific Invasive Pneumococcal Disease Surveillance among Countries Using PCV10/13: The Pneumococcal Serotype Replacement and Distribution Estimation (PSERENADE) Project. Microorganisms 2021. [Google Scholar]
- World Health Organization. WHO-UNICEF Estimates of PCV3 Coverage. Available online: https://apps.who.int/immunization_monitoring/globalsummary/timeseries/tswucoveragepcv3.html (accessed on 30 December 2020).
- Merck Sharp & Dohme Corp. A Phase 3, Multicenter, Randomized, Double-Blind, Active Comparator-Controlled Study to Evaluate the Safety, Tolerability, and Immunogenicity of V114 in Healthy Adults 50 Years of Age or Older (PNEU-AGE). 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT03950622 (accessed on 20 December 2020).
- Pfizer. A Phase 3, Randomized, Double-Blind Trial to Evaluate the Safety and Immunogenicity of a 20-Valent Pneumococcal Conjugate Vaccine in Pneumococcal Vaccine-Naive Adults 18 Years of Age and Older. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT03760146 (accessed on 20 December 2020).
- van Selm, S.; vac Cann, L.M.; Kolkman, M.A.B.; van der Zeijst, B.A.M.; van Putten, J.P.M. Genetic Basis for the Structural Difference between Streptococcus Pneumoniae Serotype 15B and 15C Capsular Polysaccharides-PubMed. Infect. Immun. 2003, 71, 6192–6198. [Google Scholar] [CrossRef] [Green Version]
- Yee, T.W. Vector Generalized Linear and Additive Models; Springer Series in Statistics; Springer: New York, NY, USA, 2015; ISBN 978-1-4939-2817-0. [Google Scholar]
- Sings, H.L.; De Wals, P.; Gessner, B.D.; Isturiz, R.; Laferriere, C.; McLaughlin, J.M.; Pelton, S.; Schmitt, H.-J.; Suaya, J.A.; Jodar, L. Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine Against Invasive Disease Caused by Serotype 3 in Children: A Systematic Review and Meta-Analysis of Observational Studies. Clin. Infect. Dis. 2019, 68, 2135–2143, Corrigendum to: Clin. Infect. Dis. 2021, 1, 1–2, doi:10.1093/cid/ciaa1767. [Google Scholar] [CrossRef]
- Lapidot, R.; Shea, K.M.; Yildirim, I.; Cabral, H.J.; Pelton, S.I. Characteristics of Serotype 3 Invasive Pneumococcal Disease before and after Universal Childhood Immunization with PCV13 in Massachusetts. Pathogens 2020, 9, 396. [Google Scholar] [CrossRef]
- Ladhani, S.N.; Collins, S.; Djennad, A.; Sheppard, C.L.; Borrow, R.; Fry, N.K.; Andrews, N.J.; Miller, E.; Ramsay, M.E. Rapid Increase in Non-Vaccine Serotypes Causing Invasive Pneumococcal Disease in England and Wales, 2000–2017: A Prospective National Observational Cohort Study. Lancet Infect. Dis. 2018, 18, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Cooper, D.; Yu, X.; Sidhu, M.; Nahm, M.H.; Fernsten, P.; Jansen, K.U. The 13-Valent Pneumococcal Conjugate Vaccine (PCV13) Elicits Cross-Functional Opsonophagocytic Killing Responses in Humans to Streptococcus Pneumoniae Serotypes 6C and 7A. Vaccine 2011, 29, 7207–7211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iroh Tam, P.-Y.; Thielen, B.K.; Obaro, S.K.; Brearley, A.M.; Kaizer, A.M.; Chu, H.; Janoff, E.N. Childhood Pneumococcal Disease in Africa–A Systematic Review and Meta-Analysis of Incidence, Serotype Distribution, and Antimicrobial Susceptibility. Vaccine 2017, 35, 1817–1827. [Google Scholar] [CrossRef] [Green Version]
- De Wals, P. Commentary on Paradoxical Observations Pertaining to the Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Serotype 3 Streptococcus Pneumoniae Infections in Children. Vaccine 2018, 36, 5495–5496. [Google Scholar] [CrossRef]
- Andrews, N.J.; Waight, P.A.; Burbidge, P.; Pearce, E.; Roalfe, L.; Zancolli, M.; Slack, M.; Ladhani, S.N.; Miller, E.; Goldblatt, D. Serotype-Specific Effectiveness and Correlates of Protection for the 13-Valent Pneumococcal Conjugate Vaccine: A Postlicensure Indirect Cohort Study. Lancet Infect. Dis. 2014, 14, 839–846. [Google Scholar] [CrossRef]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Holtzman, C.; Harrison, L.H.; Zansky, S.M.; Rosen, J.B.; Reingold, A.; Scherzinger, K.; et al. Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine for Prevention of Invasive Pneumococcal Disease in Children in the USA: A Matched Case-Control Study. Lancet Respir. Med. 2016, 4, 399–406. [Google Scholar] [CrossRef]
- Harboe, Z.B.; Dalby, T.; Weinberger, D.M.; Benfield, T.; Mølbak, K.; Slotved, H.C.; Suppli, C.H.; Konradsen, H.B.; Valentiner-Branth, P. Impact of 13-Valent Pneumococcal Conjugate Vaccination in Invasive Pneumococcal Disease Incidence and Mortality. Clin. Infect. Dis. 2014, 59, 1066–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domínguez, Á.; Ciruela, P.; Hernández, S.; García-García, J.J.; Soldevila, N.; Izquierdo, C.; Moraga-Llop, F.; Díaz, A.; de Sevilla, M.F.; González-Peris, S.; et al. Effectiveness of the 13-Valent Pneumococcal Conjugate Vaccine in Preventing Invasive Pneumococcal Disease in Children Aged 7-59 Months. A Matched Case-Control Study. PLoS ONE 2017, 12, e0183191. [Google Scholar] [CrossRef]
- van der Linden, M.; Falkenhorst, G.; Perniciaro, S.; Fitzner, C.; Imöhl, M. Effectiveness of Pneumococcal Conjugate Vaccines (PCV7 and PCV13) against Invasive Pneumococcal Disease among Children under Two Years of Age in Germany. PLoS ONE 2016, 11, e0161257. [Google Scholar] [CrossRef]
- Deceuninck, G.; De Wals, P.; Boulianne, N.; De Serres, G. Effectiveness of Pneumococcal Conjugate Vaccine Using a 2+1 Infant Schedule in Quebec, Canada. Pediatr. Infect. Dis. J. 2010, 29, 546–549. [Google Scholar] [CrossRef]
- Savulescu, C.; Hanquet, G. PCV13 Effectiveness and Overall Effect of PCV10/13 Vaccination Programmes in Children under Five Years of Age: SpIDnet Multicentre Studies. In Proceedings of the ESCAIDE 2016 Parallel Session on Vaccine-Preventable Diseases, Stockholm, Sweden, 19 November 2016. [Google Scholar]
- Lodi, L.; Ricci, S.; Nieddu, F.; Moriondo, M.; Lippi, F.; Canessa, C.; Mangone, G.; Cortimiglia, M.; Casini, A.; Lucenteforte, E.; et al. Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Severe Invasive Disease Caused by Serotype 3 Streptococcus Pneumoniae in Italian Children. Vaccines 2019, 7, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peckeu, L.; van der Ende, A.; de Melker, H.E.; Sanders, E.A.M.; Knol, M.J. Impact and Effectiveness of the 10-Valent Pneumococcal Conjugate Vaccine on Invasive Pneumococcal Disease among Children under 5 Years of Age in the Netherlands. Vaccine 2021, 39, 431–437. [Google Scholar] [CrossRef]
- Hammitt, L.L.; Etyang, A.O.; Morpeth, S.C.; Ojal, J.; Mutuku, A.; Mturi, N.; Moisi, J.C.; Adetifa, I.M.; Karani, A.; Akech, D.O.; et al. Effect of Ten-Valent Pneumococcal Conjugate Vaccine on Invasive Pneumococcal Disease and Nasopharyngeal Carriage in Kenya: A Longitudinal Surveillance Study. Lancet 2019, 393, 2146–2154. [Google Scholar] [CrossRef] [Green Version]
- Rinta-Kokko, H.; Palmu, A.A.; Auranen, K.; Nuorti, J.P.; Toropainen, M.; Siira, L.; Virtanen, M.J.; Nohynek, H.; Jokinen, J. Long-Term Impact of 10-Valent Pneumococcal Conjugate Vaccination on Invasive Pneumococcal Disease among Children in Finland. Vaccine 2018, 36, 1934–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serum Institute of India. A New Pneumococcal Vaccine Is Here! Why This Matters. Available online: https://www.seruminstitute.com/news_pneumococcal_vaccine.php (accessed on 10 December 2020).
- Pfizer. U.S. FDA Accepts for Priority Review the Biologics License Application for Pfizer’s Investigational 20-Valent Pneumococcal Conjugate Vaccine for Adults 18 Years of Age and Older. Available online: https://investors.pfizer.com/investor-news/press-release-details/2020/U.S.-FDA-Accepts-for-Priority-Review-the-Biologics-License-Application-for-Pfizers-Investigational-20-valent-Pneumococcal-Conjugate-Vaccine-for-Adults-18-Years-of-Age-and-Older/default.aspx (accessed on 10 December 2020).
- Pfizer. Data from Pfizer’s Adult and Pediatric Clinical Trial Programs for 20-Valent Pneumococcal Conjugate Vaccine Presented at IDWeek 2020. Available online: https://investors.pfizer.com/investor-news/press-release-details/2020/Data-From-Pfizers-Adult-and-Pediatric-Clinical-Trial-Programs-for-20-Valent-Pneumococcal-Conjugate-Vaccine-Presented-at-IDWeek-2020/default.aspx (accessed on 10 December 2020).
- Soeters, H.M.; Kambiré, D.; Sawadogo, G.; Ouédraogo-Traoré, R.; Bicaba, B.; Medah, I.; Sangaré, L.; Ouédraogo, A.-S.; Ouangraoua, S.; Yaméogo, I.; et al. Impact of 13-Valent Pneumococcal Conjugate Vaccine on Pneumococcal Meningitis, Burkina Faso, 2016–2017. J. Infect. Dis. 2019, 220, S253–S262. [Google Scholar] [CrossRef] [PubMed]
- Ousmane, S.; Kobayashi, M.; Seidou, I.; Issaka, B.; Sharpley, S.; Farrar, J.L.; Whitney, C.G.; Ouattara, M. Characterization of Pneumococcal Meningitis before and after Introduction of 13-Valent Pneumococcal Conjugate Vaccine in Niger, 2010–2018. Vaccine 2020, 38, 3922–3929. [Google Scholar] [CrossRef]
- Bozio, C.H.; Abdul-Karim, A.; Abenyeri, J.; Abubakari, B.; Ofosu, W.; Zoya, J.; Ouattara, M.; Srinivasan, V.; Vuong, J.T.; Opare, D.; et al. Continued Occurrence of Serotype 1 Pneumococcal Meningitis in Two Regions Located in the Meningitis Belt in Ghana Five Years after Introduction of 13-Valent Pneumococcal Conjugate Vaccine. PLoS ONE 2018, 13, e0203205. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.C.; Hetrich, M.K.; Garcia Quesada, M.; Sinkevitch, J.N.; Deloria Knoll, M.; Feikin, D.R.; Zeger, S.L.; Kagucia, E.W.; Cohen, A.L.; Ampofo, K.; et al. Changes in Invasive Pneumococcal Disease Caused by Streptococcus Pneumoniae Serotype 1 Following Introduction of PCV10 and PCV13: Findings from the PSERENADE Project. Microorganisms 2021, 9, 696. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia Quesada, M.; Yang, Y.; Bennett, J.C.; Hayford, K.; Zeger, S.L.; Feikin, D.R.; Peterson, M.E.; Cohen, A.L.; Almeida, S.C.G.; Ampofo, K.; et al. Serotype Distribution of Remaining Pneumococcal Meningitis in the Mature PCV10/13 Period: Findings from the PSERENADE Project. Microorganisms 2021, 9, 738. https://doi.org/10.3390/microorganisms9040738
Garcia Quesada M, Yang Y, Bennett JC, Hayford K, Zeger SL, Feikin DR, Peterson ME, Cohen AL, Almeida SCG, Ampofo K, et al. Serotype Distribution of Remaining Pneumococcal Meningitis in the Mature PCV10/13 Period: Findings from the PSERENADE Project. Microorganisms. 2021; 9(4):738. https://doi.org/10.3390/microorganisms9040738
Chicago/Turabian StyleGarcia Quesada, Maria, Yangyupei Yang, Julia C. Bennett, Kyla Hayford, Scott L. Zeger, Daniel R. Feikin, Meagan E. Peterson, Adam L. Cohen, Samanta C. G. Almeida, Krow Ampofo, and et al. 2021. "Serotype Distribution of Remaining Pneumococcal Meningitis in the Mature PCV10/13 Period: Findings from the PSERENADE Project" Microorganisms 9, no. 4: 738. https://doi.org/10.3390/microorganisms9040738