Epidemiology and Outcomes of Bloodstream Infections in HIV-Patients during a 13-Year Period

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
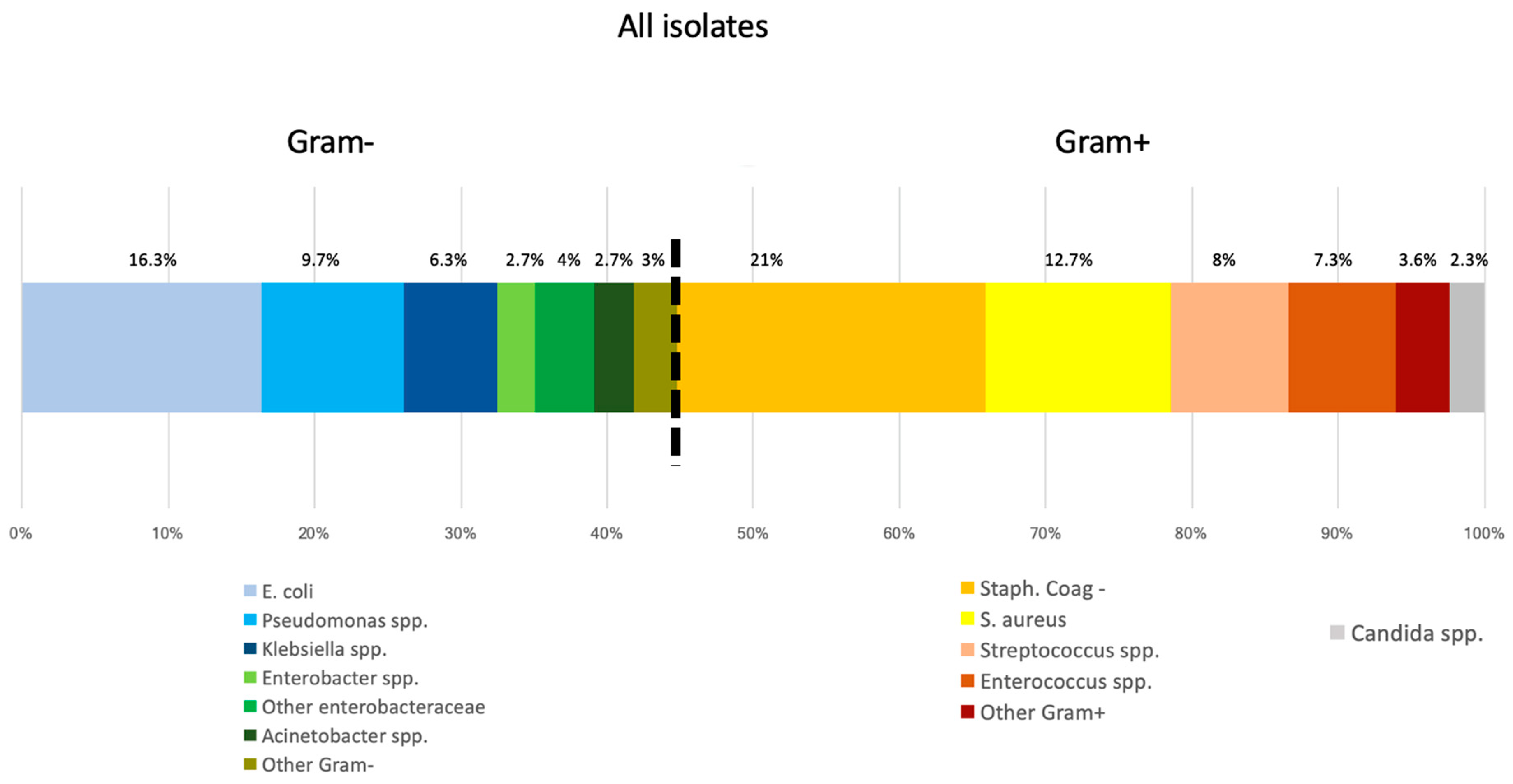
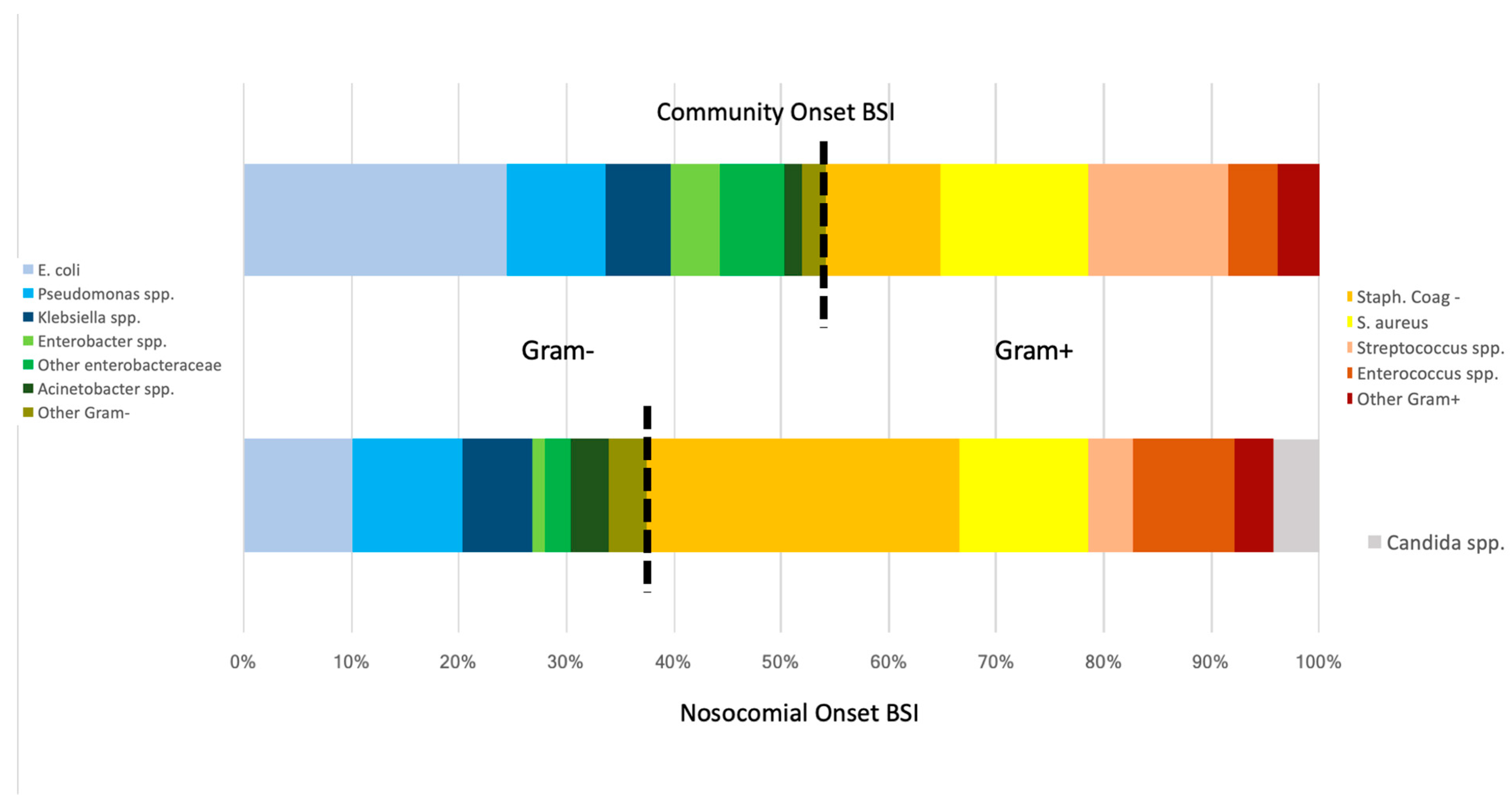
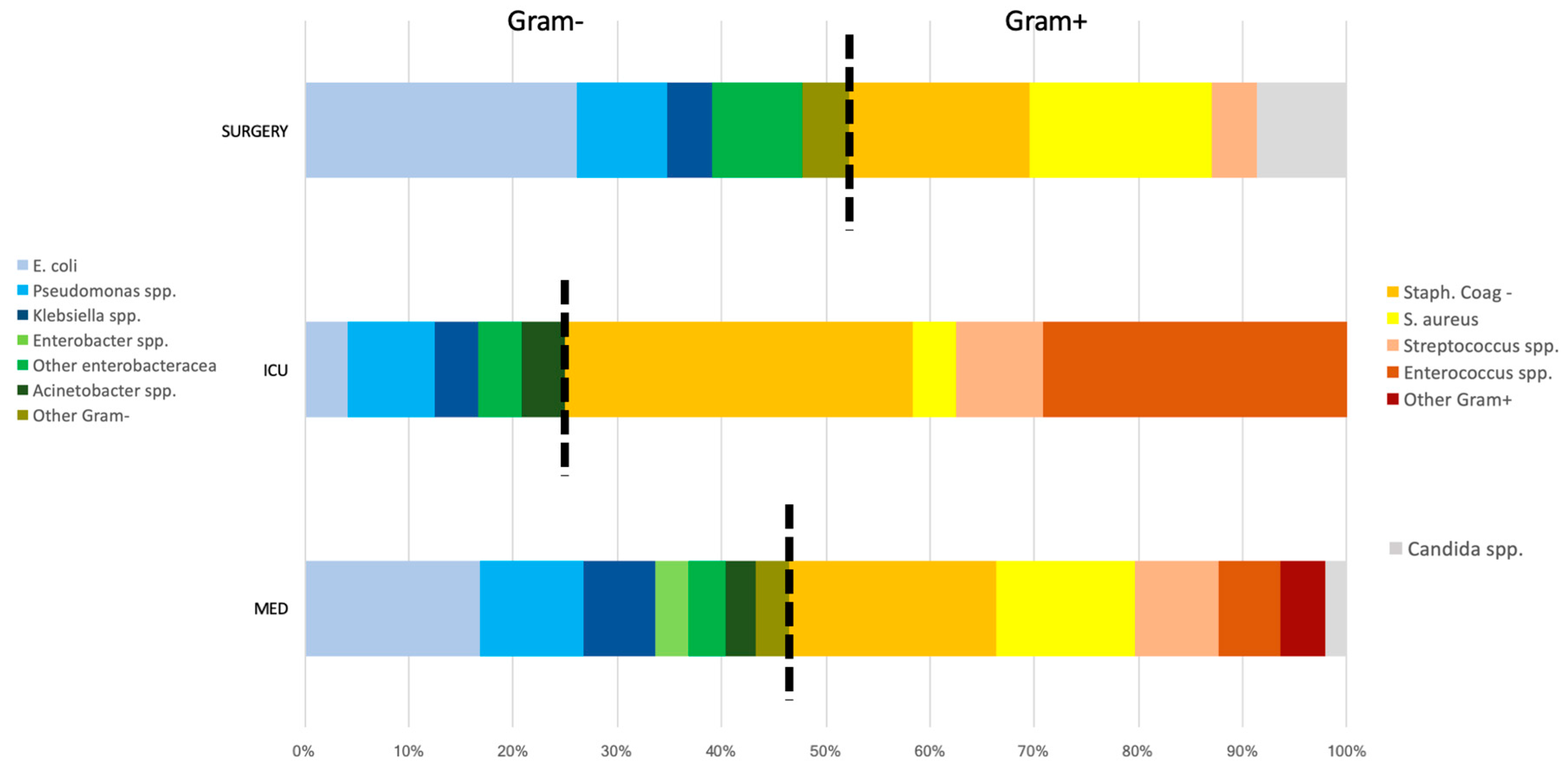
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Meynard, J.-L.; Guiguet, M.; Fonquernie, L.; Lefebvre, B.; Lalande, V.; Honore, I.; Meyohas, M.-C.; Girard, P.-M. Impact of highly active antiretroviral therapy on the occurrence of bacteraemia in HIV-infected patients and their epidemiologic characteristics. HIV Med. 2003, 4, 127–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japiassú, A.M.; Amâncio, R.T.; Mesquita, E.C.; Medeiros, D.M.; Bernal, H.B.; Nunes, E.P.; Luz, P.M.; Grinsztejn, B.; Bozza, F.A. Sepsis is a major determinant of outcome in critically ill HIV/AIDS patients. Crit. Care 2010, 14, R152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mrus, J.M.; Braun, L.; Yi, M.S.; Linde-Zwirble, W.T.; Johnston, J.A. Impact of HIV/AIDS on care and outcomes of severe sepsis. Crit. Care 2005, 9, R623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huson, M.A.M.; Stolp, S.M.; van der Poll, T.; Grobusch, M.P. Community-acquired bacterial bloodstream infections in HIV-infected patients: A systematic review. Clin. Infect. Dis. 2014, 58, 79–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taramasso, L.; Tatarelli, P.; Di Biagio, A. Bloodstream infections in HIV-infected patients. Virulence 2016, 7, 320–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrosillo, N.; Viale, P.; Nicastri, E.; Arici, C.; Bombana, E.; Casella, A.; Cristini, F.; De Gennaro, M.; Dodi, F.; Gabbuti, A.; et al. Nosocomial bloodstream infections among human immunodeficiency virus-infected patients: Incidence and risk factors. Clin. Infect. Dis. 2002, 34, 677–685. [Google Scholar] [CrossRef] [Green Version]
- Uhlenkott, M.C.; Buskin, S.E.; Kahle, E.M.; Barash, E.; Aboulafia, D.M. Causes of death in the era of highly active antiretroviral therapy: A retrospective analysis of a hybrid hematology-oncology and HIV practice and the Seattle/King county adult/adolescent spectrum of HIV-related diseases project. Am. J. Med. Sci. 2008, 336, 217–223. [Google Scholar] [CrossRef]
- Ortega, M.; Almela, M.; Soriano, A.; Marco, F.; Martínez, J.A.; Muñoz, A.; Peñarroja, G.; Mensa, J. Bloodstream infections among human immunodeficiency virus-infected adult patients: Epidemiology and risk factors for mortality. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 969–976. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Available online: https://aidsinfo.nih.gov/guidelines (accessed on 12 June 2020).
- Prabaker, K.; Weinstein, R.A. Trends in antimicrobial resistance in intensive care units in the United States. Curr. Opin Crit. Care 2011, 17, 472–479. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control Surveillance of Antimicrobial Resistance in Europe 2018. 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2018 (accessed on 12 June 2020).
- ECDC. ECDC Country Visit to Italy to Discuss Antimicrobial Resistance Issues; European Centre for Disease Prevention and Control (ECDC): Solna, Sweden, 2017; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/AMR-country-visit-Italy.pdf (accessed on 12 June 2020).
- European Centre for Disease Prevention and Control. An Agency of the European Union ECDC Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in Acute Care Hospitals; European Centre for Disease Prevention and Control (ECDC): Solna, Sweden, 2013; Available online: https://www.ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/healthcare-associated-infections-antimicrobial-use-PPS (accessed on 12 June 2020).
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Afessa, B.; Morales, I.; Weaver, B. Bacteremia in hospitalized patients with human immunodeficiency virus: A prospective, cohort study. BMC Infect. Dis. 2001, 1, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agenzia sanitaria e. Sociale Regionale Emilia ROmagna Sorveglianza dell’Antibioticoresistenza e USO di Antibiotici Sistemici in Emilia-Romagna. Available online: https://assr.regione.emilia-romagna.it/pubblicazioni/rapporti-documenti/antibioticoresistenza-rer-2018 (accessed on 12 June 2020).
- Furuno, J.P.; Johnson, J.K.; Schweizer, M.L.; Uche, A.; Stine, O.C.; Shurland, S.M.; Forrest, G.N. Community-associated methicillin-resistant Staphylococcus aureus bacteremia and endocarditis among HIV patients: A cohort study. BMC Infect. Dis. 2011, 11, 298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazzaretti, C.; Borghi, V.; Franceschini, E.; Guaraldi, G.; Mussini, C. Engagement and retention in care of patients diagnosed with HIV infection and enrolled in the Modena HIV Surveillance Cohort. J. Int. AIDS Soc. 2012, 15, 18393. [Google Scholar] [CrossRef]
- Musiime, V.; Cook, A.; Bakeera-Kitaka, S.; Vhembo, T.; Lutakome, J.; Keishanyu, R.; Prendergast, A.J.; Lubwama, S.; Robertson, V.; Hughes, P.; et al. Bacteremia, causative agents and antimicrobial susceptibility among HIV-1-infected children on antiretroviral therapy in Uganda and Zimbabwe. Pediatr. Infect. Dis. J. 2013, 32, 856–862. [Google Scholar] [CrossRef]
- Grant, A.D.; Djomand, G.; Smets, P.; Kadio, A.; Coulibaly, M.; Kakou, A.; Maurice, C.; Whitaker, J.P.; Sylla-Koko, F.; Bonard, D.; et al. Profound immunosuppression across the spectrum of opportunistic disease among hospitalized HIV-infected adults in Abidjan, Côte d’Ivoire. AIDS 1997, 11, 1357–1364. [Google Scholar] [CrossRef]
- Meremo, A.; Mshana, S.E.; Kidenya, B.R.; Kabangila, R.; Peck, R.; Kataraihya, J.B. High prevalence of Non-typhoid salmonella bacteraemia among febrile HIV adult patients admitted at a tertiary Hospital, North-Western Tanzania. Int Arch. Med. 2012, 5, 28. [Google Scholar] [CrossRef]
- Mayanja, B.N.; Todd, J.; Hughes, P.; Van der Paal, L.; Mugisha, J.O.; Atuhumuza, E.; Tabuga, P.; Maher, D.; Grosskurth, H. Septicaemia in a population-based HIV clinical cohort in rural Uganda, 1996-2007: Incidence, aetiology, antimicrobial drug resistance and impact of antiretroviral therapy. Trop. Med. Int. Health 2010, 15, 697–705. [Google Scholar] [CrossRef]
- Bartoletti, M.; Giannella, M.; Caraceni, P.; Domenicali, M.; Ambretti, S.; Tedeschi, S.; Verucchi, G.; Badia, L.; Lewis, R.E.; Bernardi, M.; et al. Epidemiology and outcomes of bloodstream infection in patients with cirrhosis. J. Hepatol. 2014, 61, 51–58. [Google Scholar] [CrossRef]
- Trecarichi, E.M.; Pagano, L.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Caira, M.; Spadea, A.; Busca, A.; et al. Current epidemiology and antimicrobial resistance data for bacterial bloodstream infections in patients with hematologic malignancies: An Italian multicentre prospective survey. Clin. Microbiol. Infect. 2015, 21, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Islas-Muñoz, B.; Volkow-Fernández, P.; Ibanes-Gutiérrez, C.; Villamar-Ramírez, A.; Vilar-Compte, D.; Cornejo-Juárez, P. Bloodstream infections in cancer patients. Risk factors associated with mortality. Int. J. Infect. Dis. 2018, 71, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Silva, M.; Marra, A.R.; Pereira, C.A.P.; Medina-Pestana, J.O.; Camargo, L.F.A. Bloodstream infection after kidney transplantation: Epidemiology, microbiology, associated risk factors, and outcome. Transplantation 2010, 90, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Salute, M. della Linee Guida Italiane Sull’utilizzo dei Farmaci Antiretrovirali e Sulla Gestione Diagnostico-Clinica Delle Persone con Infezione da HIV-1-anno 2017. Available online: http://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=2696 (accessed on 12 June 2020).
- EACS European AIDS Clinical Society EACS European AIDS Clinical Society, HIV GUIDELINES 2018. 2018. Available online: https://www.eacsociety.org/guidelines/eacs-guidelines/eacs-guidelines.html (accessed on 12 June 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total (263 Obs) | Non MDR Isolate (169 Obs) | MDR Isolate (94 Obs) | p Value |
|---|---|---|---|---|
| Age, median (IQR) | 46 (40–52) | 46 (41–52) | 45 (40–52) | 0.625 |
| Male sex, n (%) | 175 (66.5) | 114 (67) | 61 (65) | 0.673 |
| Year of event, n (%) | 0.188 | |||
| Before 2008 | 105 (40) | 62 (36.7) | 43 (45.7) | |
| 2009–2013 | 94 (35.7) | 67 (39.6) | 27 (28.7) | |
| After 2014 | 64 (24.3) | 40 (23.7) | 24 (25.5) | |
| Hospital acquired, n (%) | 137 (52) | 71 (42) | 66 (70) | <0.001 |
| Years of HIV *, median (IQR) | 14 (7–22) | 15 (8–23) | 11 (4–19) | 0.021 |
| Years of cART **, median (IQR) | 5 (0–10) | 5 (0–10) | 5 (0–9) | 0.944 |
| CD4/CD8 ratio ***, median (IQR) | 0.38 (0.13–0.64) | 0.41 (0.14–0.66) | 0.24 (0.10–0.60) | 0.133 |
| CD4 count ***, cell/μL, median (IQR) | 207 (73–385) | 216 (84–396) | 186 (45–344) | 0.356 |
| CD4 count < 200/μL at event ***, n (%) | 83 (47.4) | 52 (45) | 31 (52) | 0.417 |
| HIV RNA > 100.000 copies/mL at event ***, n (%) | 23 (13.3) | 12 (10.8) | 11 (17.7) | 0.198 |
| HIV RNA > 10.000 copies/mL at event ***, n (%) | 44 (25.4) | 28 (25.2) | 16 (25.8) | 0.933 |
| HIV RNA < 200 copies/mL at event ***, n (%) | 113 (65.3) | 75 (67) | 38 (61) | 0.406 |
| Type of isolate, n (%) | 0.061 | |||
| Gram negative | 119 (45.2) | 82 (48.5) | 37 (49.4) | |
| Gram positive | 139 (52.8) | 82 (48.5) | 57 (60.6) | |
| Fungi | 5 (2) | 5 (3) | 0 (0) | |
| Death, n (%) | 83 (31.6) | 41 (24.3) | 42 (44.7) | <0.001 |
| Gram negative | 39 (32.8) | 20 (24.4) | 19 (51.4) | 0.004 |
| Gram positive | 43 (30.9) | 20 (24.4) | 23 (40.4) | 0.045 |
| Fungi | 1 (20) | 1 (20) | 0 (0) | - |
| Polymicrobial, n (%) | 24 (9.1) | 15 (8.9) | 9 (9.6) | 0.854 |
| Central venous associated bacteremia, n (%) | 72 (27.4) | 34 (20.1) | 38 (40.4) | <0.001 |
| Gram negative | 26 (36.1) | 14 (41.2) | 12 (31.6) | 0.183 |
| Gram positive | 44 (61.1) | 18 (52.9) | 26 (68.4) | |
| Fungi | 2 (2.8) | 2 (5.9) | 0 (0) | |
| ICU | 9 (40.9) | 5 (14.7) | 4 (10.5) | 0.849 |
| Surgery | 6 (26.1) | 3 (8.8) | 3 (7.9) | |
| Medicine | 57 (26.2) | 26 (76.5) | 31 (81.6) |
| Variables | Total Population (258 Obs) | Gram Negative (119 Obs) | Gram Positive (139 Obs) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | Std. Err. | p Value | 95% CI | OR | Std. Err. | p Value | 95% CI | IRR | Std. Err. | p Value | 95% CI | |
| Age | 1.04 | 0.02 | 0.009 | 1.01–1.07 | 1.08 | 0.03 | 0.004 | 1.02–1.14 | 1.02 | 0.01 | 0.249 | 0.99–1.06 |
| Male sex | 1.15 | 0.36 | 0.639 | 0.63–2.11 | 0.56 | 0.24 | 0.187 | 0.24–1.32 | 2.29 | 1.03 | 0.066 | 0.95–5.55 |
| Years of c-ART | 1.12 | 0.03 | 0.001 | 1.06–1.19 | 1.10 | 0.04 | 0.006 | 1.03–1.18 | 1.13 | 0.05 | 0.004 | 1.04–1.24 |
| Years of HIV | 1.02 | 0.16 | 0.331 | 0.98–1.05 | 1.03 | 0.02 | 0.176 | 0.99–1.08 | 1.00 | 0.02 | 0.872 | 0.95–1.04 |
| CD4 count < 200 at event | 0.67 | 0.23 | 0.255 | 0.34–1.33 | 1.09 | 0.55 | 0.859 | 0.41–2.94 | 0.39 | 0.19 | 0.050 | 0.16–1.00 |
| HIV-RNA < 200 copies/mL at event | 0.96 | 0.34 | 0.912 | 0.48–1.85 | 1.04 | 0.54 | 0.932 | 0.38–2.89 | 0.91 | 0.43 | 0.844 | 0.36–2.29 |
| HIV-RNA > 100.000 copies/mL at event | 0.64 | 0.35 | 0.410 | 0.22–1.83 | 0.43 | 0.36 | 0.317 | 0.08–2.25 | 0.73 | 0.52 | 0.657 | 0.18–2.93 |
| HIV-RNA > 10.000 copies/mL at event | 0.78 | 0.31 | 0.538 | 0.36–1.70 | 0.50 | 0.32 | 0.278 | 0.14–1.74 | 1.00 | 0.50 | 0.997 | 0.37–2.68 |
| Hospital ward | ||||||||||||
| ICU | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Surgery | 0.32 | 0.20 | 0.075 | 0.09–1.12 | 1.04 | 0.13 | 0.072 | 0.01–1.22 | 0.16 | 0.19 | 0.118 | 0.02–1.58 |
| Medicines | 0.44 | 0.20 | 0.078 | 0.18–1.09 | 1.09 | 0.12 | 0.048 | 0.01–1.00 | 0.56 | 0.31 | 0.295 | 0.19–1.65 |
| CVC-associated bacteremia | 1.16 | 0.32 | 0.582 | 0.68–2.00 | 0.94 | 0.41 | 0.892 | 0.40–2.22 | 1.28 | 0.49 | 0.521 | 0.60–2.72 |
| MDR isolate | 2.46 | 0.65 | 0.001 | 1.46–4.13 | 3.37 | 1.41 | 0.004 | 1.48–7.65 | 2.12 | 0.78 | 0.041 | 1.03–4.34 |
| ESBL isolate | 1.83 | 0.63 | 0.077 | 0.94–3.59 | 1.57 | 0.61 | 0.249 | 0.73–3.37 | - | - | - | - |
| CRKP isolate | 5.22 | 2.99 | 0.004 | 1.70–16.08 | 4.02 | 2.18 | 0.010 | 1.39–11.65 | - | - | - | - |
| MRSA isolate | 3.48 | 2.22 | 0.051 | 1.00–12.15 | - | - | - | - | 3.66 | 2.18 | 0.061 | 0.94–12.01 |
| A | Unadjusted (258 Obs) | Adjusted for Age (258 Obs) | Adjusted for Age, Ward and CD4 Count * (172 Obs) | ||||||
| OR | 95%CI | p Value | OR | 95%CI | p Value | OR | 95%CI | p Value | |
| MDR isolate | 2.49 | 1.49–4.17 | 0.001 | 2.55 | 1.50–4.34 | 0.001 | 2.22 | 1.12–4.41 | 0.023 |
| Age | 1.04 | 1.01–1.07 | 0.009 | 1.04 | 1.00–1.07 | 0.046 | |||
| B | Unadjusted (258 Obs) | Adjusted for Age (258 Obs) | Adjusted for Age, Ward and CD4 Count * (172 Obs) | ||||||
| OR | 95%CI | p Value | OR | 95%CI | p Value | OR | 95%CI | p Value | |
| CRKP isolate | 5.22 | 1.70–16.08 | 0.004 | 4.45 | 1.39–14.22 | 0.012 | 1.84 | 0.46–7.39 | 0.388 |
| Age | 1.03 | 1.00–1.06 | 0.035 | 1.03 | 1.00–1.07 | 0.074 | |||
| C | Unadjusted (258 Obs) | Adjusted for Age (258 Obs) | Adjusted for Age, Ward and CD4 Count * (172 Obs) | ||||||
| OR | 95%CI | p Value | OR | 95%CI | p Value | OR | 95%CI | p Value | |
| CRKP isolate | 5.22 | 1.70–16.08 | 0.004 | 4.45 | 1.39–14.22 | 0.012 | 1.84 | 0.46–7.39 | 0.388 |
| Age | 1.03 | 1.00–1.06 | 0.035 | 1.03 | 1.00–1.07 | 0.074 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franceschini, E.; Santoro, A.; Menozzi, M.; Bacca, E.; Venturelli, C.; Zona, S.; Bedini, A.; Digaetano, M.; Puzzolante, C.; Meschiari, M.; et al. Epidemiology and Outcomes of Bloodstream Infections in HIV-Patients during a 13-Year Period. Microorganisms 2020, 8, 1210. https://doi.org/10.3390/microorganisms8081210
Franceschini E, Santoro A, Menozzi M, Bacca E, Venturelli C, Zona S, Bedini A, Digaetano M, Puzzolante C, Meschiari M, et al. Epidemiology and Outcomes of Bloodstream Infections in HIV-Patients during a 13-Year Period. Microorganisms. 2020; 8(8):1210. https://doi.org/10.3390/microorganisms8081210
Chicago/Turabian StyleFranceschini, E., Antonella Santoro, Marianna Menozzi, Erica Bacca, Claudia Venturelli, Stefano Zona, Andrea Bedini, Margherita Digaetano, Cinzia Puzzolante, Marianna Meschiari, and et al. 2020. "Epidemiology and Outcomes of Bloodstream Infections in HIV-Patients during a 13-Year Period" Microorganisms 8, no. 8: 1210. https://doi.org/10.3390/microorganisms8081210