
Escherichia coli Is Overtaking Group B Streptococcus in Early-Onset Neonatal Sepsis
 , , , ,
, , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical and Microbiological Practices
2.3. Definitions
- Intrapartum antibiotic prophylaxis: intrapartum antibiotics administered for multiple reasons (e.g., GBS prophylaxis, suspected chorioamnionitis, maternal fever).
- Adequate IAP: penicillin, ampicillin, or cefazolin administered at least 4 h prior to delivery.
- Prolonged ROM: rupture of membranes ≥ 18 h before delivery.
- Pre-term neonates: neonates born at <37 weeks gestation.
- Late pre-term and full-term: neonates born at 34–36 and ≥37 weeks, respectively.
- Very low birth weight (VLBW) neonates: BW < 1500 g.
- Asymptomatic bacteraemia: positive blood culture obtained due to maternal RFs for EOS in an infant who remained asymptomatic.
- Pneumonia: positive blood culture associated with respiratory distress syndrome and a characteristic radiographic appearance [9].
- Brain lesions: lesions confirmed by brain ultrasound or magnetic resonance imaging (MRI) in a newborn with clinical indications.
- Severe disease: any of the following: apnoea at onset; need for fluid resuscitation, catecholamine support, mechanical ventilation, or exchange transfusion; pneumonia; meningitis; brain lesions at hospital discharge; death.
- EOS-related death: death occurring within the first 7 postnatal days.
2.4. Statistical Analysis
3. Results
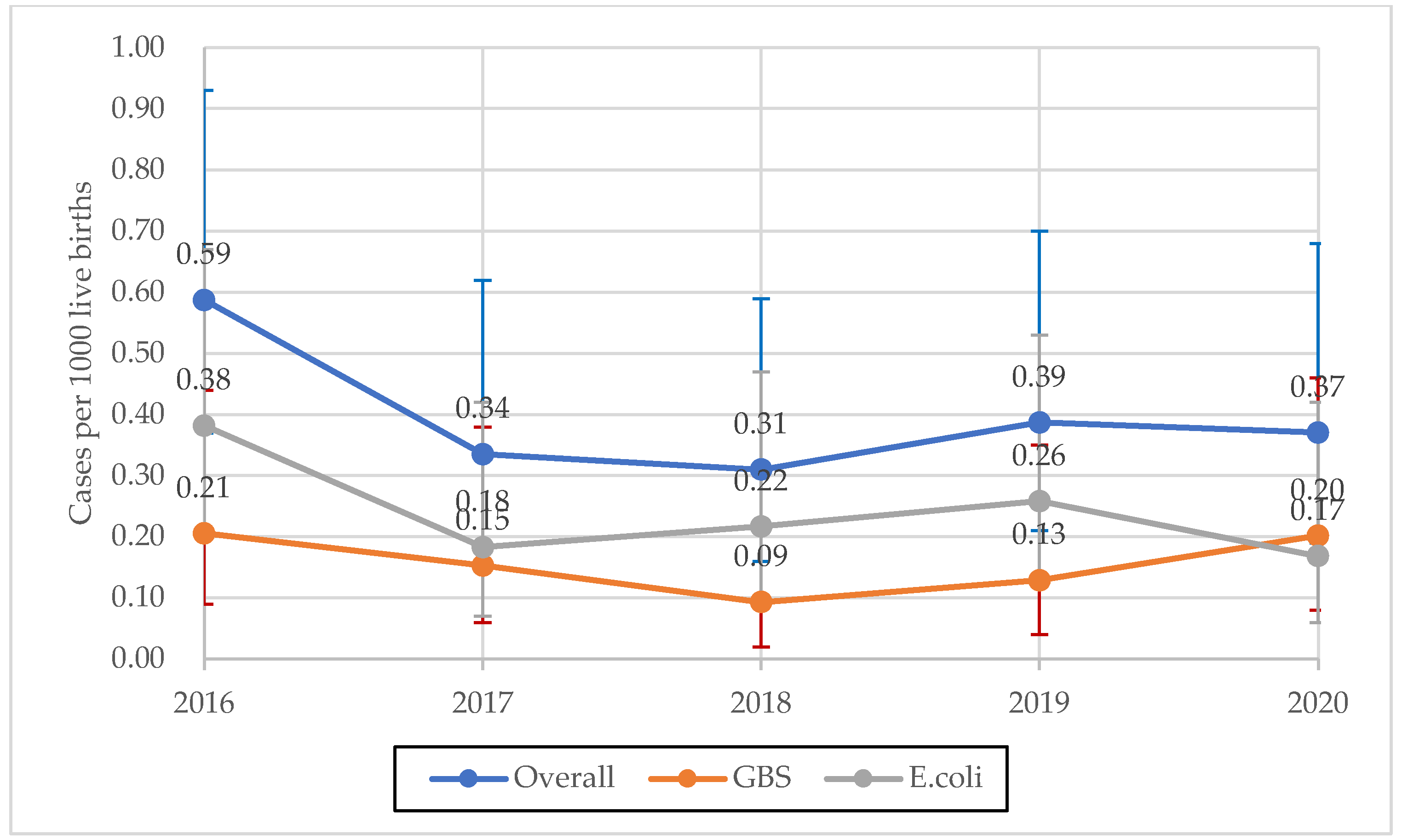
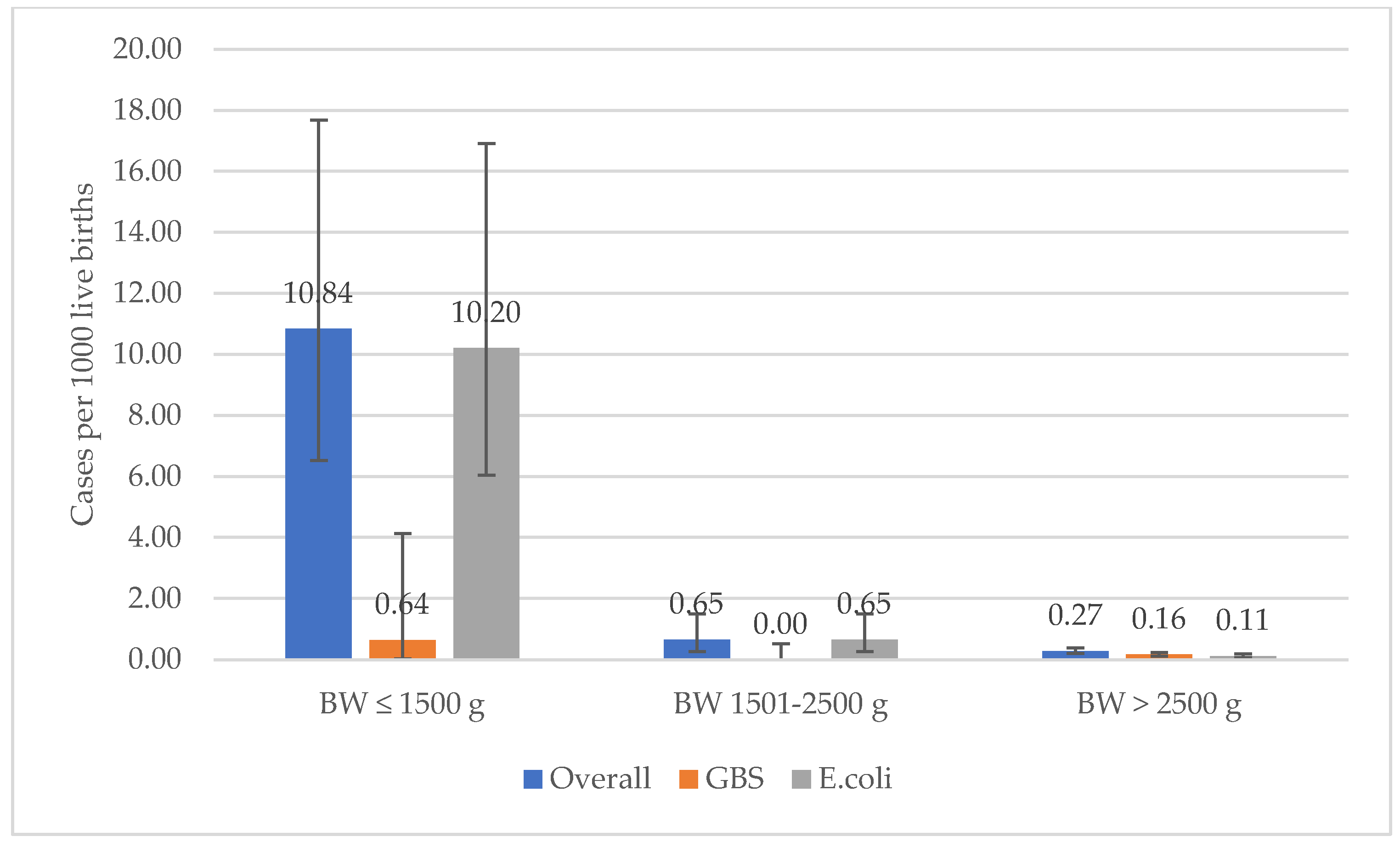
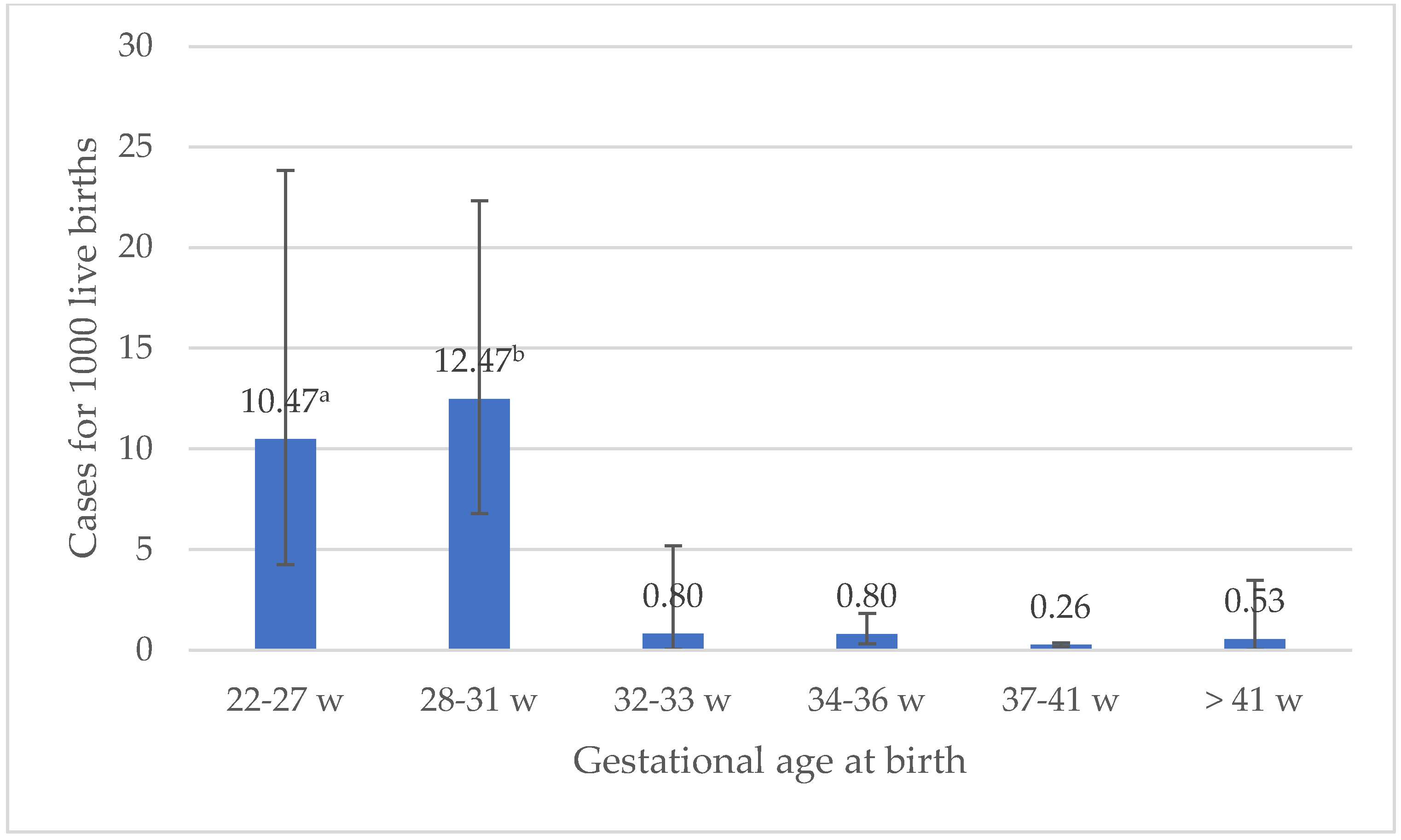
3.1. Overall and Pathogen Specific Incidence Rates, According to BW and GA
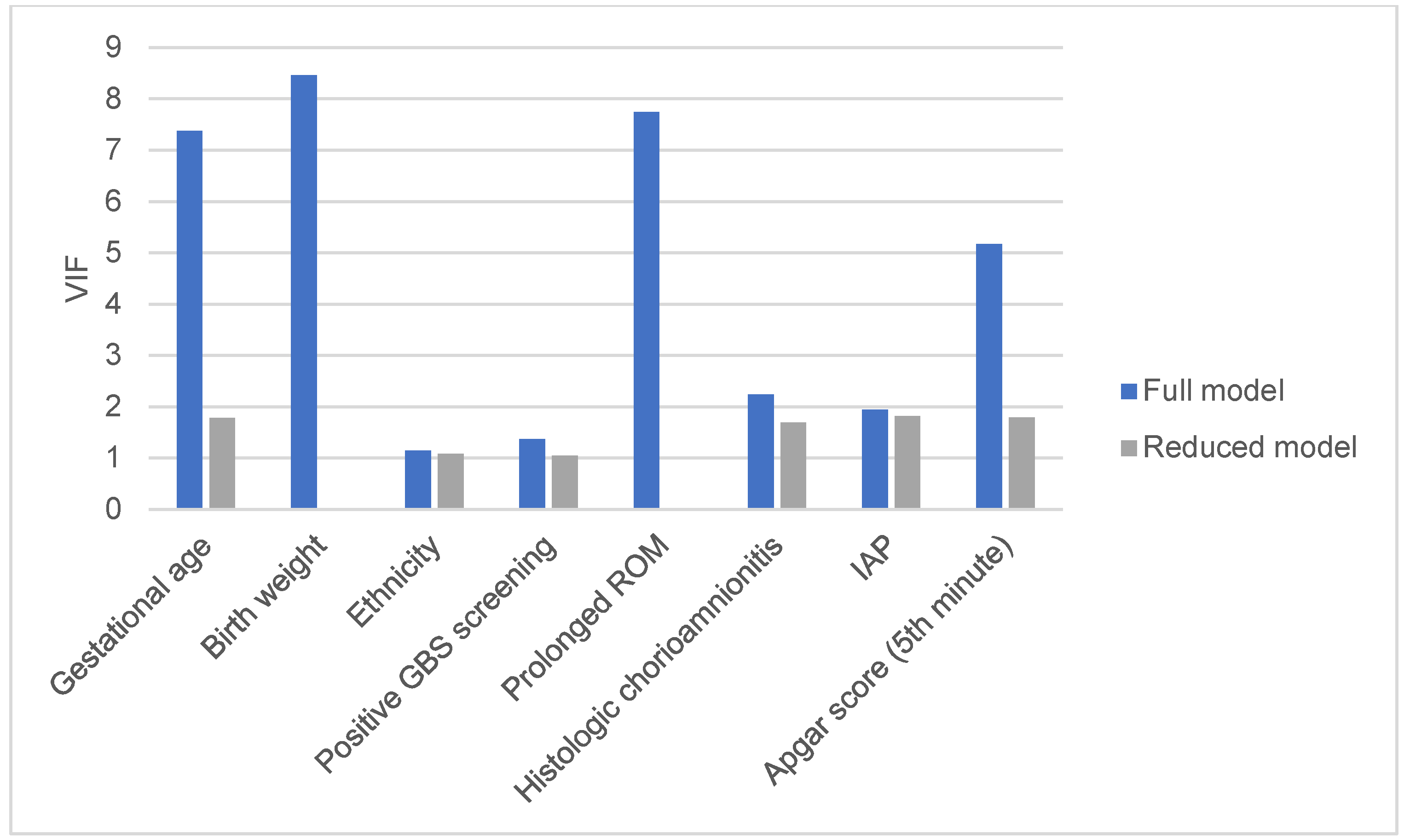
3.2. Factors Associated with Severe Disease
3.3. Antimicrobial Susceptibility
3.4. Comparison with Previous Emilia-Romagna Surveillance Reports
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bizzarro, M.J.; Raskind, C.; Baltimore, R.S.; Gallagher, P.G. Seventy-Five Years of Neonatal Sepsis at Yale: 1928–2003. Pediatrics 2005, 116, 595–602. [Google Scholar] [CrossRef]
- Bizzarro, M.J.; Dembry, L.-M.; Baltimore, R.S.; Gallagher, P.G. Changing Patterns in Neonatal Escherichia Coli Sepsis and Ampicillin Resistance in the Era of Intrapartum Antibiotic Prophylaxis. Pediatrics 2008, 121, 689–696. [Google Scholar] [CrossRef]
- Schrag, S.J.; Farley, M.M.; Petit, S.; Reingold, A.; Weston, E.J.; Pondo, T.; Hudson Jain, J.; Lynfield, R. Epidemiology of Invasive Early-Onset Neonatal Sepsis, 2005 to 2014. Pediatrics 2016, 138, e20162013. [Google Scholar] [CrossRef]
- Singh, T.; Barnes, E.H.; Isaacs, D. Australian Study Group for Neonatal Infections Early-Onset Neonatal Infections in Australia and New Zealand, 2002–2012. Arch. Dis. Child.-Fetal Neonatal Ed. 2019, 104, F248–F252. [Google Scholar] [CrossRef]
- Stoll, B.J.; Puopolo, K.M.; Hansen, N.I.; Sánchez, P.J.; Bell, E.F.; Carlo, W.A.; Cotten, C.M.; D’Angio, C.T.; Kazzi, S.N.J.; Poindexter, B.B.; et al. Early-Onset Neonatal Sepsis 2015 to 2017, the Rise of Escherichia Coli, and the Need for Novel Prevention Strategies. JAMA Pediatr. 2020, 174, e200593. [Google Scholar] [CrossRef]
- Weston, E.J.; Pondo, T.; Lewis, M.M.; Martell-Cleary, P.; Morin, C.; Jewell, B.; Daily, P.; Apostol, M.; Petit, S.; Farley, M.; et al. The Burden of Invasive Early-Onset Neonatal Sepsis in the United States, 2005–2008. Pediatr. Infect. Dis. J. 2011, 30, 937–941. [Google Scholar] [CrossRef]
- Bizzarro, M.J.; Shabanova, V.; Baltimore, R.S.; Dembry, L.-M.; Ehrenkranz, R.A.; Gallagher, P.G. Neonatal Sepsis 2004–2013: The Rise and Fall of Coagulase-Negative Staphylococci. J. Pediatr. 2015, 166, 1193–1199. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Sánchez, P.J.; Faix, R.G.; Poindexter, B.B.; Van Meurs, K.P.; Bizzarro, M.J.; Goldberg, R.N.; Frantz, I.D.; Hale, E.C.; et al. Early Onset Neonatal Sepsis: The Burden of Group B Streptococcal and E. coli Disease Continues. Pediatrics 2011, 127, 817–826. [Google Scholar] [CrossRef]
- Berardi, A.; Baroni, L.; Bacchi Reggiani, M.L.; Ambretti, S.; Biasucci, G.; Bolognesi, S.; Capretti, M.G.; Carretto, E.; Ciccia, M.; Fiorini, V.; et al. The Burden of Early-Onset Sepsis in Emilia-Romagna (Italy): A 4-Year, Population-Based Study. J. Matern.-Fetal Neonatal Med. 2016, 29, 3126–3131. [Google Scholar] [CrossRef]
- Giannoni, E.; Agyeman, P.K.A.; Stocker, M.; Posfay-Barbe, K.M.; Heininger, U.; Spycher, B.D.; Bernhard-Stirnemann, S.; Niederer-Loher, A.; Kahlert, C.R.; Donas, A.; et al. Neonatal Sepsis of Early Onset, and Hospital-Acquired and Community-Acquired Late Onset: A Prospective Population-Based Cohort Study. J. Pediatr. 2018, 201, 106–114.e4. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.; Fanaroff, A.A.; Wright, L.L.; Carlo, W.A.; Ehrenkranz, R.A.; Lemons, J.A.; Donovan, E.F.; Stark, A.R.; Tyson, J.E.; et al. Changes in Pathogens Causing Early-Onset Sepsis in Very-Low-Birth-Weight Infants. N. Engl. J. Med. 2002, 347, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Cordero, L.; Rau, R.; Taylor, D.; Ayers, L.W. Enteric Gram-Negative Bacilli Bloodstream Infections: 17 Years’ Experience in a Neonatal Intensive Care Unit. Am. J. Infect. Control 2004, 32, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Daley, A.J.; Isaacs, D. Australasian Study Group for Neonatal Infections Ten-Year Study on the Effect of Intrapartum Antibiotic Prophylaxis on Early Onset Group B Streptococcal and Escherichia Coli Neonatal Sepsis in Australasia. Pediatr. Infect. Dis. J. 2004, 23, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.; Peake, K.; Morris, A.J.; McCowan, L.M.; Battin, M.R. Escherichia Coli: A Growing Problem in Early Onset Neonatal Sepsis. Aust. N. Z. J. Obstet. Gynaecol. 2004, 44, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Higgins, R.D.; Fanaroff, A.A.; Duara, S.; Goldberg, R.; Laptook, A.; Walsh, M.; Oh, W.; Hale, E.; et al. Very Low Birth Weight Preterm Infants with Early Onset Neonatal Sepsis: The Predominance of Gram-Negative Infections Continues in the National Institute of Child Health and Human Development Neonatal Research Network, 2002–2003. Pediatr. Infect. Dis. J. 2005, 24, 635–639. [Google Scholar] [CrossRef]
- Towers, C.V.; Briggs, G.G. Antepartum Use of Antibiotics and Early-Onset Neonatal Sepsis: The next 4 Years. Am. J. Obstet. Gynecol. 2002, 187, 495–500. [Google Scholar] [CrossRef]
- Towers, C.V.; Carr, M.H.; Padilla, G.; Asrat, T. Potential Consequences of Widespread Antepartal Use of Ampicillin. Am. J. Obstet. Gynecol. 1998, 179, 879–883. [Google Scholar] [CrossRef]
- Joseph, T.A.; Pyati, S.P.; Jacobs, N. Neonatal Early-Onset Escherichia Coli Disease. The Effect of Intrapartum Ampicillin. Arch. Pediatr. Adolesc. Med. 1998, 152, 35–40. [Google Scholar] [CrossRef]
- Karlowicz, M.G.; Buescher, E.S.; Surka, A.E. Fulminant Late-Onset Sepsis in a Neonatal Intensive Care Unit, 1988–1997, and the Impact of Avoiding Empiric Vancomycin Therapy. Pediatrics 2000, 106, 1387–1390. [Google Scholar] [CrossRef]
- Mayor-Lynn, K.; González-Quintero, V.H.; O’Sullivan, M.J.; Hartstein, A.I.; Roger, S.; Tamayo, M. Comparison of Early-Onset Neonatal Sepsis Caused by Escherichia Coli and Group B Streptococcus. Am. J. Obstet. Gynecol. 2005, 192, 1437–1439. [Google Scholar] [CrossRef]
- Cohen-Wolkowiez, M.; Moran, C.; Benjamin, D.K.; Cotten, C.M.; Clark, R.H.; Benjamin, D.K.; Smith, P.B. Early and Late Onset Sepsis in Late Preterm Infants. Pediatr. Infect. Dis. J. 2009, 28, 1052–1056. [Google Scholar] [CrossRef] [PubMed]
- Ficara, M.; Pietrella, E.; Spada, C.; Della Casa Muttini, E.; Lucaccioni, L.; Iughetti, L.; Berardi, A. Changes of Intestinal Microbiota in Early Life. J. Matern.-Fetal Neonatal Med. 2020, 33, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Zeissig, S.; Blumberg, R.S. Life at the Beginning: Perturbation of the Microbiota by Antibiotics in Early Life and Its Role in Health and Disease. Nat. Immunol. 2014, 15, 307–310. [Google Scholar] [CrossRef]
- Berardi, A.; Lugli, L.; Baronciani, D.; Creti, R.; Rossi, K.; Ciccia, M.; Gambini, L.; Mariani, S.; Papa, I.; Serra, L.; et al. Group B Streptococcal Infections in a Northern Region of Italy. Pediatrics 2007, 120, e487–e493. [Google Scholar] [CrossRef] [PubMed]
- Schrag, S.; Gorwitz, R.; Fultz-Butts, K.; Schuchat, A. Prevention of Perinatal Group B Streptococcal Disease. Revised Guidelines from CDC. MMWR Recomm. Rep. 2002, 51, 1–22. [Google Scholar] [PubMed]
- Verani, J.R.; McGee, L.; Schrag, S.J. Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC) Prevention of Perinatal Group B Streptococcal Disease--Revised Guidelines from CDC, 2010. MMWR Recomm. Rep. 2010, 59, 1–36. [Google Scholar]
- Creti, R.; Imperi, M.; Berardi, A.; Lindh, E.; Alfarone, G.; Pataracchia, M.; Recchia, S. The Italian Network On Neonatal And Infant Gbs Infections, null Invasive Group B Streptococcal Disease in Neonates and Infants, Italy, Years 2015–2019. Microorganisms 2021, 9, 2579. [Google Scholar] [CrossRef]
- Ganatra, H.A.; Stoll, B.J.; Zaidi, A.K.M. International Perspective on Early-Onset Neonatal Sepsis. Clin. Perinatol. 2010, 37, 501–523. [Google Scholar] [CrossRef]
- Berardi, A.; Lugli, L.; Baronciani, D.; Rossi, C.; Ciccia, M.; Creti, R.; Gambini, L.; Mariani, S.; Papa, I.; Tridapalli, E.; et al. Group B Streptococcus Early-Onset Disease in Emilia-Romagna: Review after Introduction of a Screening-Based Approach. Pediatr. Infect Dis. J. 2010, 29, 115–121. [Google Scholar] [CrossRef]
- Berardi, A.; Di Fazzio, G.; Gavioli, S.; Di Grande, E.; Groppi, A.; Papa, I.; Piccinini, G.; Simoni, A.; Tridapalli, E.; Volta, A.; et al. Universal Antenatal Screening for Group B Streptococcus in Emilia-Romagna. J. Med. Screen 2011, 18, 60–64. [Google Scholar] [CrossRef]
- Berardi, A.; Rossi, C.; Bacchi Reggiani, M.L.; Bastelli, A.; Capretti, M.G.; Chiossi, C.; Fiorini, V.; Gambini, L.; Gavioli, S.; Lanari, M.; et al. An Area-Based Study on Intrapartum Antibiotic Prophylaxis for Preventing Group B Streptococcus Early-Onset Disease: Advances and Limitations. J. Matern. Fetal. Neonatal. Med. 2017, 30, 1739–1744. [Google Scholar] [CrossRef] [PubMed]
- Berardi, A.; Lugli, L.; Rossi, C.; Guidotti, I.; Lanari, M.; Creti, R.; Perrone, E.; Biasini, A.; Sandri, F.; Volta, A.; et al. Impact of Perinatal Practices for Early-Onset Group B Streptococcal Disease Prevention. Pediatr. Infect Dis. J. 2013, 32, e265–e271. [Google Scholar] [CrossRef] [PubMed]
- López Sastre, J.B.; Fernández Colomer, B.; Coto Cotallo, G.D.; Ramos Aparicio, A. Grupo de Hospitales Castrillo Trends in the Epidemiology of Neonatal Sepsis of Vertical Transmission in the Era of Group B Streptococcal Prevention. Acta Paediatr. 2005, 94, 451–457. [Google Scholar] [CrossRef]
- Ohlsson, A.; Shah, V.S. Intrapartum Antibiotics for Known Maternal Group B Streptococcal Colonization. Cochrane Database Syst. Rev. 2014, 6, CD007467. [Google Scholar] [CrossRef]
- Cailes, B.; Kortsalioudaki, C.; Buttery, J.; Pattnayak, S.; Greenough, A.; Matthes, J.; Bedford Russell, A.; Kennea, N.; Heath, P.T. neonIN network Epidemiology of UK Neonatal Infections: The NeonIN Infection Surveillance Network. Arch Dis. Child Fetal Neonatal Ed. 2018, 103, F547–F553. [Google Scholar] [CrossRef]
- Johansson Gudjónsdóttir, M.; Elfvin, A.; Hentz, E.; Adlerberth, I.; Tessin, I.; Trollfors, B. Changes in Incidence and Etiology of Early-Onset Neonatal Infections 1997-2017 - a Retrospective Cohort Study in Western Sweden. BMC Pediatr. 2019, 19, 490. [Google Scholar] [CrossRef] [PubMed]
- Bekker, V.; Bijlsma, M.W.; van de Beek, D.; Kuijpers, T.W.; van der Ende, A. Incidence of Invasive Group B Streptococcal Disease and Pathogen Genotype Distribution in Newborn Babies in the Netherlands over 25 Years: A Nationwide Surveillance Study. Lancet Infect. Dis. 2014, 14, 1083–1089. [Google Scholar] [CrossRef]
- WHO. Regional Office for Europe and European Centre for Disease Prevention and Control. In Surveillance of Antimicrobial Resistance in Europe, 2020 Data; Executive Summary; WHO Regional Office for Europe: Copenhagen, Denmark, 2021. [Google Scholar]
- Puopolo, K.M.; Benitz, W.E.; Zaoutis, T.E. Committee on Fetus and Newborn; Committee on Infectious Diseases Management of Neonates Born at ≥35 0/7 Weeks’ Gestation with Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics 2018, 142, e20182894. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Benitz, W.E.; Zaoutis, T.E. Committee on Fetus and Newborn; Committee on Infectious Diseases Management of Neonates Born at ≤34 6/7 Weeks’ Gestation with Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics 2018, 142, e20182896. [Google Scholar] [CrossRef]
- Flannery, D.D.; Akinboyo, I.C.; Mukhopadhyay, S.; Tribble, A.C.; Song, L.; Chen, F.; Li, Y.; Gerber, J.S.; Puopolo, K.M. Antibiotic Susceptibility of Escherichia Coli Among Infants Admitted to Neonatal Intensive Care Units Across the US From 2009 to 2017. JAMA Pediatr. 2021, 175, 168–175. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Clinical Characteristics | Overall (GBS and E. coli; n = 64) | E. coli (n = 39) | Missing | GBS (n = 25) | Missing | p a |
|---|---|---|---|---|---|---|
| Positive antenatal GBS screening b, n (%) | 11 (20%) | 3 (9%) | - | 8 (36%) | - | 0.04 |
| Vaginal delivery, n (%) | 40 (63%) | 20 (51%) | - | 20 (80%) | - | 0.03 |
| Prolonged ROM, n (%) | 25 (39%) | 19 (49%) | 5 | 6 (24%) | 8 | 0.05 |
| Median duration of ROM, hours, (IQR) | 17 (2–60) | 20 (1–158) | 8 | 9 (4–19) | 8 | 0.02 |
| Maternal intrapartum temperature ≥ 38 °C, n (%) | 17 (27%) | 10 (26%) | 1 | 7 (28%) | - | 0.99 |
| Maternal GBS bacteriuria, n (%) | 6 (9%) | 5 (14%) | 4 | 1 (5%) | 5 | 0.40 |
| Prior infant with GBS disease, n (%) | 0 (0%) | - | - | 0% (0%) | - | - |
| Clinical chorioamnionitis c, n (%) | 7 (11%) | 4 (13%) | 7 | 3 (14%) | 4 | 0.99 |
| Placental analysis performed, n (%) | 30 (47%) | 21 (64%) | 18 | 9 (38%) | 16 | 0.05 |
| Histological chorioamnionitis, n (%) | 18 (67%) | 15 (47%) | 7 | 3 (14%) | 3 | 0.02 |
| IAP exposure d, n (%) | 36 (56%) | 27 (69%) | - | 9 (36%) | - | 0.009 |
| Adequate IAP, n (%) | 20 (31%) | 18 (47%) | 1 | 2 (8%) | 1 | 0.002 |
| Median birth weight, g (IQR) | 2930 (1365–3479) | 2235 (1120–3100) | - | 3400 (3035–3842) | - | 0.001 |
| Birth weight < 1500 g, n (%) | 17 (27%) | 16 (41%) | - | 1 (4%) | - | <0.001 |
| Median gestational age, weeks (IQR) | 38 (30–38) | 35 (29–39) | - | 40 (39–40) | - | 0.001 |
| Preterm neonates (<37 weeks gestation), n (%) | 25 (39%) | 22 (56%) | - | 3 (12%) | - | 0.001 |
| Asymptomatic bacteraemia, n (%) | 13 (20%) | 6 (15%) | - | 7 (28%) | - | 0.22 |
| Culture-proven meningitis e, n (%) | 2 (7%) | 1 (6%) | - | 1 (7%) | - | 0.99 |
| Pneumonia, n (%) | 9 (14%) | 3 (8%) | - | 6 (24%) | - | 0.14 |
| Median length of hospital stay, d (IQR) | 12 (9–30) | 35 (29–39) | 5 | 10 (8–15) | 1 | 0.001 |
| Brain lesions at discharge from hospital, n (%) | 3 (5%) | 3 (8%) | - | 0 (0%) | - | 0.28 |
| Case fatalities, n (%) | 5 (8%) | 4 (10%) | - | 1 (4%) | - | 0.64 |
| Characteristic | Univariable Analysis OR (95% CI) | p | Multi-Variable Analysis a | p |
|---|---|---|---|---|
| Pathogen (E. coli) | 1.49 (0.54–4.08) | 0.44 | ||
| Gestational age | 0.92 (0.84–1.01) | 0.06 | 0.95 (0.80–1.13) | 0.56 |
| Birth weight | 1.00 (0.99–1.00) | 0.12 | ||
| Ethnicity | 0.17 (0.02–1.59) | 0.12 | 0.60 (0.04–9.36) | 0.72 |
| Sex | 0.88 (0.33–2.36) | 0.80 | ||
| Twin pregnancy | 1.00 (0.06–16.71) | 1.00 | ||
| Maternal age | 1.02 (0.94–1.11) | 0.63 | ||
| Positive GBS screening | 0.37 (0.09–1.45) | 0.15 | 0.58 (0.09–3.76) | 0.56 |
| GBS bacteriuria | 1.04 (0.19–5.68) | 0.96 | ||
| Intrapartum fever ≥38 °C | 0.64 (0.21–1.98) | 0.44 | ||
| Prolonged ROM | 0.29 (0.10–0.85) | 0.02 | ||
| Caesarean Section | 1.00 (0.36–2.75) | 0.95 | ||
| Clinical chorioamnionitis | 0.53 (0.11–2.64) | 0.44 | ||
| Histologic chorioamnionitis | 2.91 (0.86–9.86) | 0.09 | 2.24 (0.30–17.04) | 0.44 |
| IAP | 0.46 (0.17–1.26) | 0.13 | 0.12 (0.02–0.76) | 0.03 |
| Adequate IAP | 0.61 (0.21–1.79) | 0.61 | ||
| Apgar score (5th minute) | 0.76 (0.59–1.00) | 0.05 | 0.65 (0.37–1.17) | 0.15 |
| Ampicillin resistance | 1.56 (0.53–4.56) | 0.42 | ||
| Gentamicin resistance | 0.84 (0.11–6.67) | 0.87 | ||
| Resistance to first-line antibiotics a | 0.97 (0.13–7.33) | 0.97 |
| VIF (Full Model) | VIF (Reduced Model) | |
|---|---|---|
| Gestational age | 7.37 | 1.78 |
| Birth weight | 8.46 | // |
| Ethnicity | 1.15 | 1.08 |
| Positive GBS screening | 1.37 | 1.05 |
| Prolonged ROM | 7.74 | // |
| Histologic chorioamnionitis | 2.24 | 1.69 |
| IAP | 1.94 | 1.81 |
| Apgar score (5th minute) | 5.17 | 1.79 |
| Susceptibility/Number of Isolates Tested (%) a | ||||||||
|---|---|---|---|---|---|---|---|---|
| Pathogens | Amikacin | Ampicillin | Cefotaxime | Clindamycin | Erythromycin | Gentamicin | Meropenem | Vancomycin |
| GBS | - | 24/24 (100%) | 6/6 (100%) | 15/22 (68%) | 11/15 (73%) | - | - | 22/22 (100%) |
| E. coli | 39/39 (100%) | 10/33 (30%) | 34/37 (92%) | - | - | 35/39 (90%) | 33/33 (100%) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miselli, F.; Cuoghi Costantini, R.; Creti, R.; Sforza, F.; Fanaro, S.; Ciccia, M.; Piccinini, G.; Rizzo, V.; Pasini, L.; Biasucci, G.; et al. Escherichia coli Is Overtaking Group B Streptococcus in Early-Onset Neonatal Sepsis. Microorganisms 2022, 10, 1878. https://doi.org/10.3390/microorganisms10101878
Miselli F, Cuoghi Costantini R, Creti R, Sforza F, Fanaro S, Ciccia M, Piccinini G, Rizzo V, Pasini L, Biasucci G, et al. Escherichia coli Is Overtaking Group B Streptococcus in Early-Onset Neonatal Sepsis. Microorganisms. 2022; 10(10):1878. https://doi.org/10.3390/microorganisms10101878
Chicago/Turabian StyleMiselli, Francesca, Riccardo Cuoghi Costantini, Roberta Creti, Francesca Sforza, Silvia Fanaro, Matilde Ciccia, Giancarlo Piccinini, Vittoria Rizzo, Lorena Pasini, Giacomo Biasucci, and et al. 2022. "Escherichia coli Is Overtaking Group B Streptococcus in Early-Onset Neonatal Sepsis" Microorganisms 10, no. 10: 1878. https://doi.org/10.3390/microorganisms10101878