
Introduction, Spread and Impact of the SARS-CoV-2 Omicron Variants BA.1 and BA.2 in Cyprus

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection and Next-Generation Sequencing
2.2. Lineage Assignment and Mutation Analysis
2.3. Phylogenetic Analysis
3. Results and Discussion
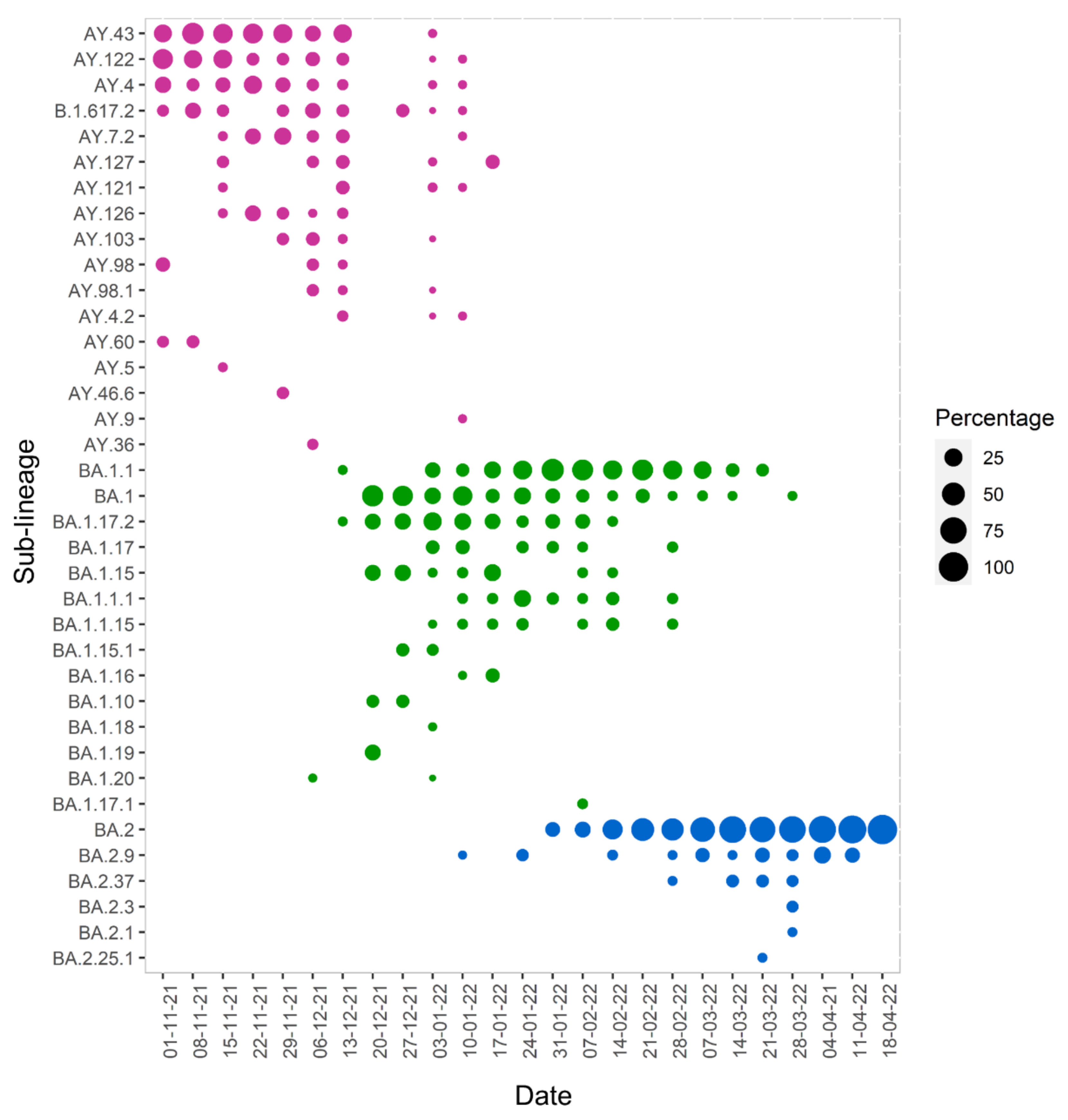
3.1. Lineage Analysis
3.2. Mutation Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Muth, D.; Niemeyer, D.; Drosten, C. Hosts and Sources of Endemic Human Coronaviruses. Adv Virus Res. 2018, 100, 163–188. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Wunderink, R.G. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology 2018, 23, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Grunewald, M.; Perlman, S. Coronaviruses: An Updated Overview of Their Replication and Pathogenesis. Methods Mol. Biol. 2020, 2203, 1–29. [Google Scholar] [CrossRef]
- Sanjuán, R.; Nebot, M.R.; Chirico, N.; Mansky, L.M.; Belshaw, R. Viral mutation rates. J. Virol. 2010, 84, 9733–9748. [Google Scholar] [CrossRef]
- Robson, F.; Khan, K.S.; Le, T.K.; Paris, C.; Demirbag, S.; Barfuss, P.; Rocchi, P.; Ng, W.L. Coronavirus RNA Proofreading: Molecular Basis and Therapeutic Targeting. Mol. Cell 2020, 79, 710–727. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Zhou, J.; Ye, Q. The Global Epidemic of the SARS-CoV-2 Delta Variant, Key Spike Mutations and Immune Escape. Front. Immunol. 2021, 12, 751778. [Google Scholar] [CrossRef]
- Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 12 July 2022).
- Saxena, S.K.; Kumar, S.; Ansari, S.; Paweska, J.T.; Maurya, V.K.; Tripathi, A.K.; Abdel-Moneim, A.S. Characterization of the novel SARS-CoV-2 Omicron (B.1.1.529) variant of concern and its global perspective. J. Med. Virol. 2022, 94, 1738–1744. [Google Scholar] [CrossRef]
- Alkhatib, M.; Salpini, R.; Carioti, L.; Ambrosio, F.A.; D’Anna, S.; Duca, L.; Costa, G.; Bellocchi, M.C.; Piermatteo, L.; Artese, A.; et al. Update on SARS-CoV-2 Omicron Variant of Concern and Its Peculiar Mutational Profile. Microbiol. Spectr. 2022, 10, e02732-21. [Google Scholar] [CrossRef]
- Nikolaidis, M.; Papakyriakou, A.; Chlichlia, K.; Markoulatos, P.; Oliver, S.G.; Amoutzias, G.D. Comparative Analysis of SARS-CoV-2 Variants of Concern, Including Omicron, Highlights Their Common and Distinctive Amino Acid Substitution Patterns, Especially at the Spike ORF. Viruses 2022, 14, 707. [Google Scholar] [CrossRef]
- Mallapaty, S. Where did Omicron come from? Three key theories. Nature 2022, 602, 26–28. [Google Scholar] [CrossRef]
- Chaguza, C.; Hahn, A.M.; Petrone, M.E.; Zhou, S.; Ferguson, D.; Breban, M.I.; Pham, K.; Peña-Hernández, M.A.; Castaldi, C.; Hill, V.; et al. Accelerated SARS-CoV-2 intrahost evolution leading to distinct genotypes during chronic infection. medRxiv 2022. [Google Scholar] [CrossRef]
- Sievers, C.; Zacher, B.; Ullrich, A.; Huska, M.; Fuchs, S.; Buda, S.; Haas, W.; Diercke, M.; an der Heiden, M.; Kröger, S. SARS-CoV-2 Omicron variants BA.1 and BA.2 both show similarly reduced disease severity of COVID-19 compared to Delta, Germany, 2021 to 2022. Eurosurveillance 2022, 27, 2200396. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Chu, H.; Yuen, K. Pathogenicity of SARS-CoV-2 Omicron. Clin. Transl. Med. 2022, 12, 693–699. [Google Scholar] [CrossRef]
- Stålcrantz, J.; Kristoffersen, A.B.; Bøås, H.; Veneti, L.; Seppälä, E.; Aasand, N.; Hungnes, O.; Kvåle, R.; Bragstad, K.; Buanes, E.A.; et al. Milder disease trajectory among COVID-19 patients hospitalised with the SARS-CoV-2 Omicron variant compared with the Delta variant in Norway. Scand. J. Public Health 2022, 50, 140349482211085. [Google Scholar] [CrossRef]
- Lin, S.; Chen, Z.; Zhang, X.; Wen, A.; Yuan, X.; Yu, C.; Yang, J.; He, B.; Cao, Y.; Lu, G. Characterization of SARS-CoV-2 Omicron spike RBD reveals significantly decreased stability, severe evasion of neutralizing-antibody recognition but unaffected engagement by decoy ACE2 modified for enhanced RBD binding. Signal Transduct. Target. Ther. 2022, 7, 56. [Google Scholar] [CrossRef]
- Evans, J.P.; Zeng, C.; Qu, P.; Faraone, J.; Zheng, Y.M.; Carlin, C.; Bednash, J.S.; Zhou, T.; Lozanski, G.; Mallampalli, R.; et al. Neutralization of SARS-CoV-2 Omicron sub-lineages BA.1, BA.1.1, and BA.2. Cell Host Microbe. 2022, 30, 1093–1102.e3. [Google Scholar] [CrossRef]
- Richter, J.; Fanis, P.; Tryfonos, C.; Koptides, D.; Krashias, G.; Bashiardes, S.; Hadjisavvas, A.; Loizidou, M.; Oulas, A.; Alexandrou, D.; et al. Molecular epidemiology of SARS-CoV-2 in Cyprus. PLoS ONE 2021, 16, e0248792. [Google Scholar] [CrossRef]
- Oulas, A.; Richter, J.; Zanti, M.; Tomazou, M.; Michailidou, K.; Christodoulou, K.; Christodoulou, C.; Spyrou, G.M. In depth analysis of Cyprus-specific mutations of SARS-CoV-2 strains using computational approaches. BMC Genom. Data 2021, 22, 48. [Google Scholar] [CrossRef]
- Rambaut, A.; Holmes, E.C.; O’Toole, Á.; Hill, V.; McCrone, J.T.; Ruis, C.; du Plessis, L.; Pybus, O.G. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat. Microbiol. 2020, 5, 1403–1407. [Google Scholar] [CrossRef]
- Mercatelli, D.; Triboli, L.; Fornasari, E.; Ray, F.; Giorgi, F.M. Coronapp: A web application to annotate and monitor SARS-CoV-2 mutations. J. Med. Virol. 2021, 93, 3238–3245. [Google Scholar] [CrossRef]
- Wickham, H. Ggplot2, Elegant Graphics for Data Analysis, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Minh, B.Q.; Schmidt, H.A.; Chernomor, O.; Schrempf, D.; Woodhams, M.D.; Von Haeseler, A.; Lanfear, R. IQ-TREE 2, New Models and Efficient Methods for Phylogenetic Inference in the Genomic Era. Mol. Biol. Evol. 2020, 37, 1530–1534. [Google Scholar] [CrossRef]
- Darriba, D.; Taboada, G.L.; Doallo, R.; Posada, D. JModelTest 2: More models, new heuristics and parallel computing. Nat. Methods 2012, 9, 772. [Google Scholar] [CrossRef]
- Letunic, I.; Bork, P. Interactive Tree of Life (iTOL) v5, an online tool for phylogenetic tree display and annotation. Nucleic Acids Res. 2021, 49, W293–W296. [Google Scholar] [CrossRef]
- Lambrou, A.S.; Shirk, P.; Steele, M.K.; Paul, P.; Paden, C.R.; Cadwell, B.; Reese, H.E.; Aoki, Y.; Hassell, N.; Caravas, J.; et al. Genomic Surveillance for SARS-CoV-2 Variants: Predominance of the Delta (B.1.617.2) and Omicron (B.1.1.529) Variants—United States, June 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 206–211. [Google Scholar] [CrossRef]
- Singh, U.B.; Deb, S.; Chaudhry, R.; Bala, K.; Rani, L.; Gupta, R.; Kumari, L.; Ahmed, J.; Gaurav, S.; Perumalla, S.; et al. SARS-CoV-2 Omicron Variant Wave in India: Advent, Phylogeny and Evolution. bioRxiv 2022. [Google Scholar] [CrossRef]
- Fonager, J.; Bennedbæk, M.; Bager, P.; Wohlfahrt, J.; Ellegaard, K.M.; Ingham, A.C.; Edslev, S.M.; Stegger, M.; Sieber, R.N.; Lassauniere, R.; et al. Molecular epidemiology of the SARS-CoV-2 variant Omicron BA.2 sub-lineage in Denmark, 29 November 2021 to 2 January 2022. Eurosurveillance 2022, 27, 2200181. [Google Scholar] [CrossRef]
- Majeed, A. London is an important barometer for the omicron wave in the United Kingdom. BMJ 2022, 376, 42. [Google Scholar] [CrossRef]
- Gangavarapu, K.; Latiff, A.A.; Mullen, J.L.; Alkuzweny, M.; Hufbauer, E.; Tsueng, G.; Haag, E.; Zeller, M.; Aceves, C.M.; Zaiets, K.; et al. Outbreak.info genomic reports: Scalable and dynamic surveillance of SARS-CoV-2 variants and mutations. medRxiv 2022. [Google Scholar] [CrossRef]
- Matsvay, A.; Klink, G.V.; Safina, K.R.; Nabieva, E.; Garushyants, S.K.; Biba, D.; Bazykin, G.A.; Mikhaylov, I.M.; Say, A.V.; Zakamornaya, A.I.; et al. Genomic epidemiology of SARS-CoV-2 in Russia reveals recurring cross-border transmission throughout 2020. medRxiv 2021. [Google Scholar] [CrossRef]
- Morobe, J.M.; Didon, D.; Pool, B.; Lambisia, A.W.; Makori, T.; Mohammed, K.S.; de Laurent, Z.R.; Ndwiga, L.; Mburu, M.W.; Moraa, E.; et al. Genomic Epidemiology of SARS-CoV-2 in Seychelles, 2020–2021. Viruses 2022, 14, 1318. [Google Scholar] [CrossRef] [PubMed]
- Plante, J.A.; Liu, Y.; Liu, J.; Xia, H.; Johnson, B.A.; Lokugamage, K.G.; Zhang, X.; Muruato, A.E.; Zou, J.; Fontes-Garfias, C.R.; et al. Spike mutation D614G alters SARS-CoV-2 fitness. Nature 2021, 592, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, J.; Johnson, B.A.; Xia, H.; Ku, Z.; Schindewolf, C.; Widen, S.G.; An, Z.; Weaver, S.C.; Menachery, V.D.; et al. Delta spike P681R mutation enhances SARS-CoV-2 fitness over Alpha variant. Cell Rep. 2022, 39, 110829. [Google Scholar] [CrossRef] [PubMed]
- Meng, B.; Abdullahi, A.; Ferreira, I.A.T.M.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 usage by SARS-CoV-2 Omicron impacts infectivity and fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef]
- Zhao, H.; Lu, L.; Peng, Z.; Chen, L.L.; Meng, X.; Zhang, C.; Ip, J.D.; Chan, W.M.; Chu, A.W.H.; Chan, K.H.; et al. SARS-CoV-2 Omicron variant shows less efficient replication and fusion activity when compared with Delta variant in TMPRSS2-expressed cells. Emerg. Microbes Infect. 2022, 11, 277–283. [Google Scholar] [CrossRef]
- Starr, T.N.; Greaney, A.J.; Dingens, A.S.; Bloom, J.D. Complete map of SARS-CoV-2 RBD mutations that escape the monoclonal antibody LY-CoV555 and its cocktail with LY-CoV016. Cell Rep. Med. 2021, 2, 100255. [Google Scholar] [CrossRef]
- Le Bert, N.; Tan, A.; Kunasegaran, K.; Chia, A.; Tan, N.; Chen, Q.; Hang, S.K.; Qui, M.D.; Chan, B.S.; Low, J.G.; et al. Mutations of SARS-CoV-2 variants of concern escaping Spike-specific T cells. bioRxiv 2022. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, T.; Fang, Y.; Liu, J.; Ye, Q.; Ding, L. SARS-CoV-2 spike L452R mutation increases Omicron variant fusogenicity and infectivity as well as host glycolysis. Signal Transduct. Target. Ther. 2022, 7, 76. [Google Scholar] [CrossRef]
- Kimura, I.; Yamasoba, D.; Tamura, T.; Nao, N.; Oda, Y.; Mitoma, S.; Ito, J.; Nasser, H.; Zahradnik, J.; Uriu, K.; et al. Virological characteristics of the novel SARS-CoV-2 Omicron variants including BA.2.12.1, BA.4 and BA.5. bioRxiv 2022, 28. [Google Scholar] [CrossRef]
- Davies, M.A.; Morden, E.; Rosseau, P.; Arendse, J.; Bam, J.L.; Boloko, L.; Cloete, K.; Cohen, C.; Chetty, N.; Dane, P.; et al. Outcomes of laboratory-confirmed SARS-CoV-2 infection during resurgence driven by Omicron lineages BA.4 and BA.5 compared with previous waves in the Western Cape Province, South Africa. medRxiv 2022, 13. [Google Scholar] [CrossRef]
- Arora, P.; Kempf, A.; Nehlmeier, I.; Schulz, S.R.; Cossmann, A.; Stankov, M.V.; Jäck, H.M.; Behrens, G.M.; Pöhlmann, S.; Hoffmann, M. Augmented neutralisation resistance of emerging omicron subvariants BA.2.12.1, BA.4, and BA.5. Lancet Infect. Dis. 2022, 22, 1117–1118. [Google Scholar] [CrossRef]
- Ren, S.-Y.; Wang, W.-B.; Gao, R.-D.; Zhou, A.-M. Omicron variant (B.1.1.529) of SARS-CoV-2, Mutation, infectivity, transmission, and vaccine resistance. World J. Clin. Cases 2022, 10, 1–11. [Google Scholar] [CrossRef]
- Lu, L.; Mok, B.W.Y.; Chen, L.; Chan, J.M.C.; Tsang, O.T.Y.; Lam, B.H.S.; Chuang, V.W.M.; Chu, A.W.H.; Chan, W.M.; Ip, J.D.; et al. Neutralization of SARS-CoV-2 Omicron variant by sera from BNT162b2 or Coronavac vaccine recipients. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Hoffmann, M.; Krüger, N.; Schulz, S.; Cossmann, A.; Rocha, C.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.S.; Winkler, M.S.; et al. The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Cell 2022, 185, 447–456.e11. [Google Scholar] [CrossRef]
- Gupta, D.; Sharma, P.; Singh, M.; Kumar, M.; Ethayathulla, A.S.; Kaur, P. Structural and functional insights into the spike protein mutations of emerging SARS-CoV-2 variants. Cell Mol. Life Sci. 2021, 78, 7967–7989. [Google Scholar] [CrossRef]
- Grabowski, F.; Kochańczyk, M.; Lipniacki, T. The Spread of SARS-CoV-2 Variant Omicron with a Doubling Time of 2.0-3.3 Days Can Be Explained by Immune Evasion. Viruses 2022, 14, 294. [Google Scholar] [CrossRef]
- Liu, Y.; Yu, Y.; Zhao, Y.; He, D. Reduction in the infection fatality rate of Omicron variant compared with previous variants in South Africa. Int. J. Infect. Dis. 2022, 120, 146–149. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Hong, V.X.; Patel, M.M.; Kahn, R.; Lipsitch, M.; Tartof, S.Y. Clinical outcomes associated with SARS-CoV-2 Omicron (B.1.1.529) variant and BA.1/BA.1.1 or BA.2 subvariant infection in southern California. Nat. Med. 2022. [Google Scholar] [CrossRef]
- Planas, D.; Saunders, N.; Maes, P.; Guivel-Benhassine, F.; Planchais, C.; Buchrieser, J.; Bolland, W.H.; Porrot, F.; Staropoli, I.; Lemoine, F.; et al. Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature 2022, 602, 671–675. [Google Scholar] [CrossRef]
- Takashita, E.; Kinoshita, N.; Yamayoshi, S.; Sakai-Tagawa, Y.; Fujisaki, S.; Ito, M.; Iwatsuki-Horimoto, K.; Chiba, S.; Halfmann, P.; Nagai, H.; et al. Efficacy of Antibodies and Antiviral Drugs against COVID-19 Omicron Variant. N. Engl. J. Med. 2022, 386, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Bálint, G.; Vörös-Horváth, B.; Széchenyi, A. Omicron: Increased transmissibility and decreased pathogenicity. Signal Transduct. Target. Ther. 2022, 7, 151. [Google Scholar] [CrossRef] [PubMed]
- Hui, K.P.; Ho, J.C.; Cheung, M.C.; Ng, K.C.; Ching, R.H.; Lai, K.L.; Kam, T.T.; Gu, H.; Sit, K.Y.; Hsin, M.K.; et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature 2022, 603, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Han, J.; Zhang, Y.; He, J.; Yu, W.; Zhang, X.; Wu, J.; Zhang, S.; Kong, Y.; Guo, Y.; et al. SARS-CoV-2 Omicron Variant: Epidemiological Features, Biological Characteristics, and Clinical Significance. Front. Immunol. 2022, 13, 2010. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| WHO Label | Lineage | Sub-Lineage | Number | % of VOC |
|---|---|---|---|---|
| Delta | B.1.617.2 | AY.43 | 45 | 24.3% |
| AY.122 | 29 | 15.7% | ||
| AY.4 | 21 | 11.4% | ||
| B.1.617.2 | 18 | 9.7% | ||
| AY.7.2 | 14 | 7.6% | ||
| AY.127 | 13 | 7.0% | ||
| AY.121 | 9 | 4.9% | ||
| AY.126 | 7 | 3.8% | ||
| AY.103 | 7 | 3.8% | ||
| AY.98 | 6 | 3.2% | ||
| AY.98.1 | 5 | 2.7% | ||
| AY.4.2 | 4 | 2.2% | ||
| AY.60 | 2 | 1.1% | ||
| AY.36 | 2 | 1.1% | ||
| AY.5 | 1 | 0.5% | ||
| AY.46.6 | 1 | 0.5% | ||
| AY.9 | 1 | 0.5% | ||
| Total | 185 | |||
| Omicron | BA.1 | BA.1.1 | 81 | 30.5% |
| BA.1 | 59 | 22.2% | ||
| BA.1.17.2 | 49 | 18.4% | ||
| BA.1.17 | 20 | 7.5% | ||
| BA.1.15 | 16 | 6.0% | ||
| BA.1.1.1 | 12 | 4.5% | ||
| BA.1.1.15 | 11 | 4.1% | ||
| BA.1.15.1 | 6 | 2.3% | ||
| BA.1.16 | 3 | 1.1% | ||
| BA.1.10 | 2 | 0.8% | ||
| BA.1.18 | 2 | 0.8% | ||
| BA.1.19 | 2 | 0.8% | ||
| BA.1.20 | 2 | 0.8% | ||
| BA.1.17.1 | 1 | 0.4% | ||
| Total | 266 | |||
| Omicron | BA.2 | BA.2 | 133 | 83.1% |
| BA.2.9 | 15 | 9.4% | ||
| BA.2.37 | 8 | 5.0% | ||
| BA.2.3 | 2 | 1.3% | ||
| BA.2.1 | 1 | 0.6% | ||
| BA.2.25.1 | 1 | 0.6% | ||
| Total | 160 |
| Position | SNP | Delta | BA.1 | BA.2 | ||
|---|---|---|---|---|---|---|
| 21595 | S1 | SP | V11V | 2.7% | 12.4% | 0.0% |
| 21618 | NTD | T19I | 0.0% | 0.0% | 98.1% | |
| 21618 | T19R | 100.0% | 0.0% | 0.0% | ||
| 21762 | A67V | 0.0% | 100.0% | 6.8% | ||
| 21846 | T95I | 39.5% | 92.1% | 6.8% | ||
| 21987 | G142D | 99.5% | 0.0% | 100.0% | ||
| 22200 | V213G | 0.0% | 0.0% | 100.0% | ||
| 22578 | RBD | G339D | 0.0% | 92.1% | 100.0% | |
| 22599 | R346K | 0.0% | 38.3% | 0.0% | ||
| 22673 | S371L | 0.0% | 99.6% | 0.0% | ||
| 22674 | S371F | 0.0% | 0.4% | 100.0% | ||
| 22679 | S373P | 0.0% | 100.0% | 100.0% | ||
| 22686 | S375F | 0.0% | 100.0% | 100.0% | ||
| 22688 | T376A | 0.0% | 0.4% | 100.0% | ||
| 22775 | D405N | 0.0% | 0.4% | 100.0% | ||
| 22786 | R408S | 0.0% | 0.4% | 100.0% | ||
| 22792 | I410I | 0.5% | 0.0% | 11.2% | ||
| 22813 | K417N | 0.0% | 100.0% | 100.0% | ||
| 22882 | RBM | N440K | 0.0% | 100.0% | 100.0% | |
| 22898 | G446S | 0.0% | 100.0% | 0.0% | ||
| 22917 | L452R | 100.0% | 0.0% | 0.0% | ||
| 22992 | S477N | 0.0% | 98.5% | 100.0% | ||
| 22995 | T478K | 100.0% | 98.5% | 100.0% | ||
| 23013 | E484A | 0.0% | 98.5% | 100.0% | ||
| 23040 | Q493R | 0.0% | 98.5% | 100.0% | ||
| 23048 | G496S | 0.0% | 98.5% | 0.0% | ||
| 23055 | Q498R | 0.0% | 98.5% | 100.0% | ||
| 23063 | N501Y | 0.0% | 98.5% | 100.0% | ||
| 23075 | Y505H | 0.0% | 98.5% | 100.0% | ||
| 23202 | T547K | 0.0% | 95.1% | 0.0% | ||
| 23403 | D614G | 100.0% | 99.2% | 100.0% | ||
| 23525 | H655Y | 0.5% | 90.6% | 95.7% | ||
| 23599 | N679K | 0.0% | 86.5% | 94.4% | ||
| 23604 | P681H | 0.0% | 86.1% | 93.8% | ||
| 23604 | P681R | 53.5% | 0.0% | 0.0% | ||
| 23664 | S2 | A701V | 0.0% | 17.7% | 0.0% | |
| 23854 | N764K | 0.0% | 100.0% | 100.0% | ||
| 23948 | FP | D796Y | 0.0% | 100.0% | 100.0% | |
| 24130 | N856K | 0.0% | 97.0% | 0.6% | ||
| 24410 | HR1 | D950N | 100.0% | 0.0% | 0.0% | |
| 24424 | Q954H | 0.0% | 100.0% | 100.0% | ||
| 24469 | N969K | 0.0% | 100.0% | 100.0% | ||
| 24503 | L981F | 0.0% | 100.0% | 0.0% | ||
| 25000 | D1146D | 0.0% | 100.0% | 100.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, J.; Koptides, D.; Tryfonos, C.; Alexandrou, D.; Christodoulou, C. Introduction, Spread and Impact of the SARS-CoV-2 Omicron Variants BA.1 and BA.2 in Cyprus. Microorganisms 2022, 10, 1688. https://doi.org/10.3390/microorganisms10091688
Richter J, Koptides D, Tryfonos C, Alexandrou D, Christodoulou C. Introduction, Spread and Impact of the SARS-CoV-2 Omicron Variants BA.1 and BA.2 in Cyprus. Microorganisms. 2022; 10(9):1688. https://doi.org/10.3390/microorganisms10091688
Chicago/Turabian StyleRichter, Jan, Dana Koptides, Christina Tryfonos, Denise Alexandrou, and Christina Christodoulou. 2022. "Introduction, Spread and Impact of the SARS-CoV-2 Omicron Variants BA.1 and BA.2 in Cyprus" Microorganisms 10, no. 9: 1688. https://doi.org/10.3390/microorganisms10091688