
Patterns of Presentation of Drug-Resistant Tuberculosis in Nigeria: A Retrospective File Review

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Setting
2.2.1. DR-TB Model in Nigeria
2.2.2. DRTB Case Finding and Diagnostic Coverage
2.2.3. DR-TB Treatment Coverage in Nigeria
2.3. Inclusion and Exclusion
2.4. Data Analysis
3. Results
3.1. Socio-Demographic and Clinical Characteristics of the Participants
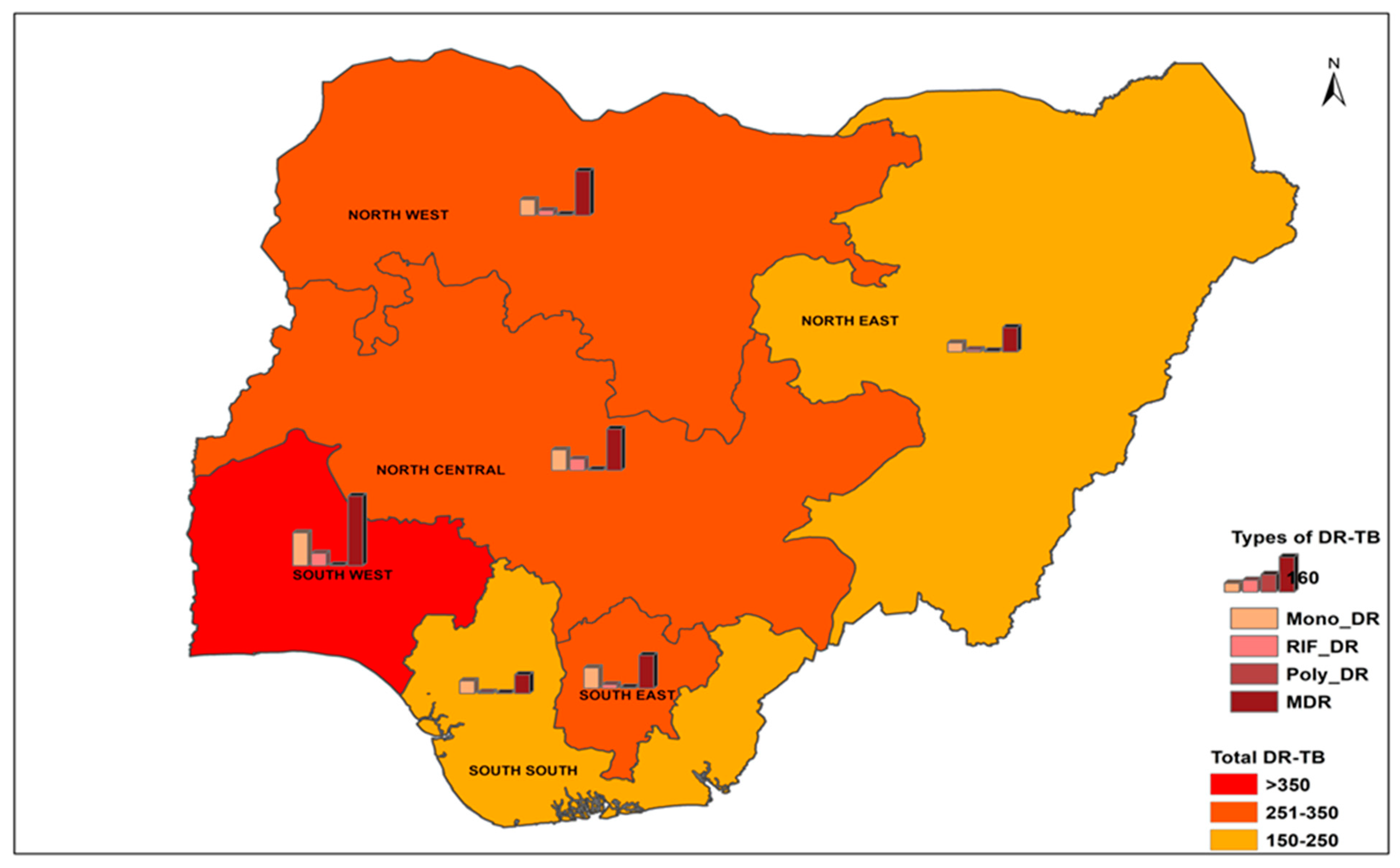
3.1.1. Pattern of Presentation of Bacteriologically Confirmed DR-TB Cases in Nigeria (2010–2016)
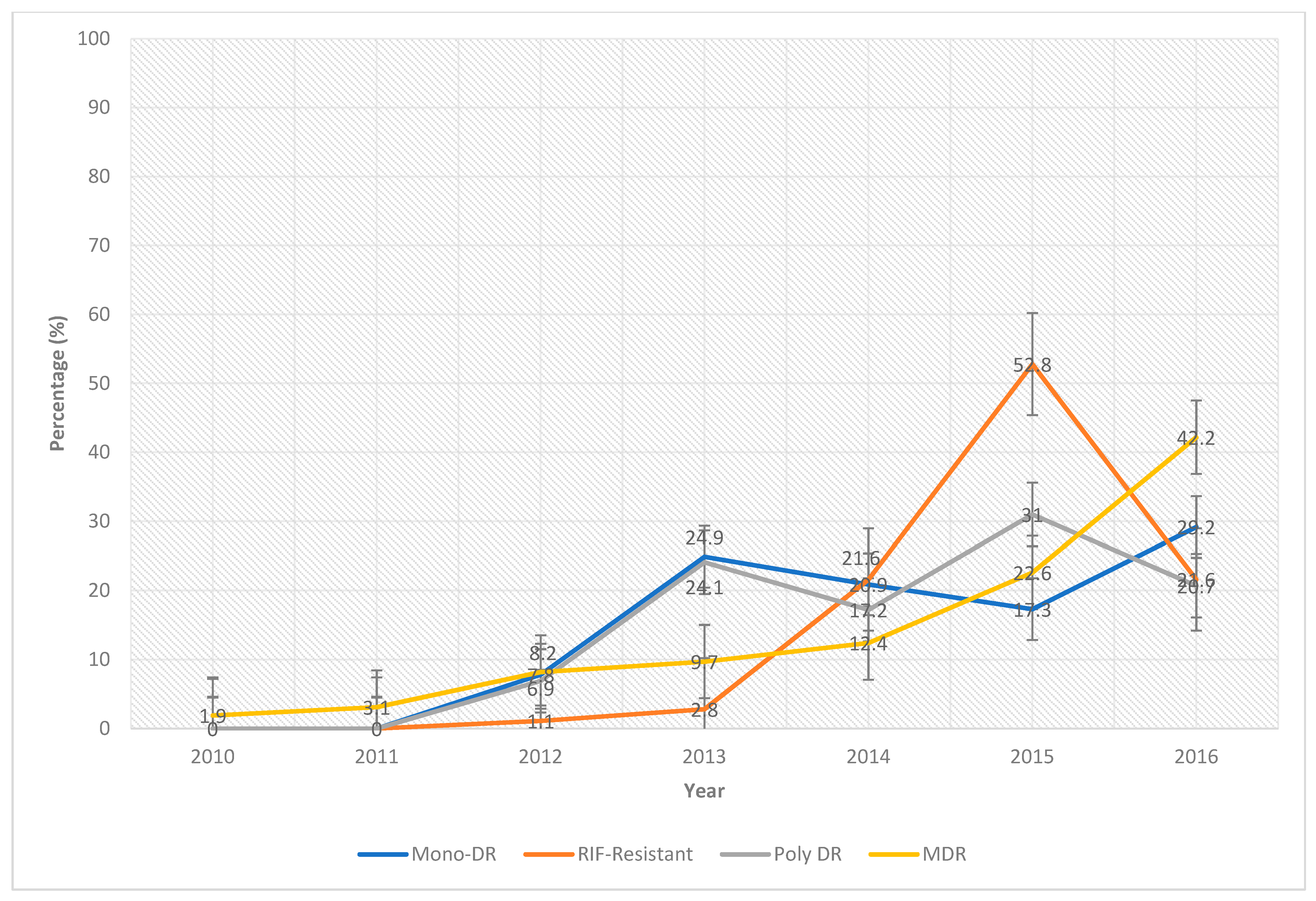
3.1.2. Trend of the Pattern of Presentation of Laboratory-Confirmed DR-TB Cases by Year (2010–2016)
4. Discussion
5. Strengths and Weaknesses
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Control: WHO Report 2018; World Health Organisation: Geneva, Switzerland, 2018. [Google Scholar]
- Federal Ministry of Health [FMOH], Department of Public Health. National TB and Leprosy Control Programme Annual Report, 2018; National TB and Leprosy Control Programme: Abuja, Nigeria, 2018. [Google Scholar]
- Federal Ministry of Health. The National Strategic Plan for Tuberculosis Control: Towards Universal Access to Prevention, Diagnosis and Treatment, 2015–2020; National Tuberculosis and Leprosy Control Programme, Department of Public Health, Federal Ministry of Health: Abuja, Nigeria, 2015; pp. 1–201. [Google Scholar]
- Kabir, M.; Obasanya, O.; Van der Grinten, E. National Tuberculosis and Leprosy Control Programme, Workers Manual, 5th ed.; Federal Ministry of Health: Abuja, Nigeria, 2010; pp. 1–64.
- Lamikanra, A. Essential Microbiology; Amkra Books: Lagos, Nigeria, 2010; pp. 395–404. [Google Scholar]
- Wang, L.; Zhang, H.; Ruan, Y.; Chin, D.P.; Xia, Y.; Cheng, S.; Chen, M.; Zhao, Y.; Jiang, S.; Du, X.; et al. Tuberculosis prevalence in China, 1990–2010; a longitudinal analysis of national survey data. Lancet 2014, 383, 2057–2064. [Google Scholar] [CrossRef]
- Lönnroth, K.; Castro, K.G.; Chakaya, J.M.; Chauhan, L.S.; Floyd, K.; Glaziou, P.; Raviglione, M.C. Tuberculosis control and elimination 2010–50: Cure, care, and social development. Lancet 2010, 375, 1814–1829. [Google Scholar] [CrossRef]
- WHO. Treatment of tuberculosis: Guidelines; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Boakye-Appiah, J.K.; Steinmetz, A.R.; Pupulampu, P.; Ofori-Yirenkyi, S.; Tetteh, I.; Frimpong, M.; Oppong, P.; Opare-Sem, O.; Norman, B.R.; Stienstra, Y.; et al. High prevalence of multidrug-resistant tuberculosis among patients with rifampicin resistance using GeneXpert Mycobacterium tuberculosis/rifampicin in Ghana. Int. J. Mycobacteriol. 2016, 5, 226–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drobniewski, F.A.; Wilson, S.M. The rapid diagnosis of isoniazid and rifampicin resistance in Mycobacterium tuberculosis a molecular story. J. Med. Microbiol. 1998, 47, 189–196. [Google Scholar] [CrossRef] [Green Version]
- Cavusoglu, C.; Hilmioglu, S.; Guneri, S.; Bilgic, A. Characterization of rpoB mutations in rifampin-resistant clinical isolates of Mycobacterium tuberculosis from Turkey by DNA sequencing and line probe assay. J. Clin. Microbiol. 2002, 40, 4435–4438. [Google Scholar] [CrossRef] [Green Version]
- Glasauer, S.; Altmann, D.; Hauer, B.; Brodhun, B.; Haas, W.; Perumal, N. First-line tuberculosis drug resistance patterns and associated risk factors in Germany, 2008–2017. PLoS ONE 2019, 14, e0217597. [Google Scholar] [CrossRef] [Green Version]
- Van Deun, A.; Barrera, L.; Bastian, I.; Fattorini, L.; Hoffmann, H.; Kam, K.M.; Rigouts, L.; Rüsch-Gerdes, S.; Wright, A. Mycobacterium tuberculosis strains with highly discordant rifampin susceptibility test results. J. Clin. Microbiol. 2009, 47, 3501–3506. [Google Scholar] [CrossRef] [Green Version]
- Rigouts, L.; Gumusboga, M.; de Rijk, W.B.; Nduwamahoro, E.; Uwizeye, C.; de Jong, B.; Van Deun, A. Rifampin resistance missed in automated liquid culture system for Mycobacterium tuberculosis isolates with specific rpoB mutations. J. Clin. Microbiol. 2013, 51, 2641–2645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.E.; Kurbatova, E.V.; Cavanaugh, J.S.; Cegielski, J.P. Global isoniazid resistance patterns in rifampin-resistant and rifampin-susceptible tuberculosis. Int. J. Tuberc. Lung Dis. 2011, 16, 203–205. [Google Scholar] [CrossRef] [Green Version]
- Toma, M.M. Determinants of Retreatment with First Line Anti Tuberculosis Drugs in Smear Positive Patients in Adamawa State, October 2012–June 2013. Master’s Thesis, Ahmadu Bello University, Zaria, Nigeria, 2014. [Google Scholar]
- WHO. Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis. 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK247413/ (accessed on 21 April 2022).
- Liu, Z.; Zhang, M.; Wang, J.; Chen, S.; Wu, B.; Zhou, L.; Pan, A.; Wang, W.; Wang, X. Longitudinal Analysis of Prevalence and Risk Factors of Rifampicin-Resistant Tuberculosis in Zhejiang, China. BioMed Res. Int. 2020, 2020, 3159482. [Google Scholar] [CrossRef] [Green Version]
- Omisore, N.O.; Oyewole, M.O.; Akinkunmi, E.O. Multi Drug Resistant Mycobacterium Tuberculosis in Adamawa State, Nigeria. Afr. J. Infect. Dis. 2018, 13, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Boonrod, T.; Ingsrisawang, L.; Pungrassami, P.; Sengsong, S.; Bromnavej, A.; Waseewiwat, P.; Sreevijit, N.; Bunsanong, B.; Bunsin, C. Drug resistance patterns of Mycobacterium tuberculosis complex and risk factors associated with multidrug-resistant tuberculosis in the upper southern part of Thailand. Epidemiol. Biostat. Public Health 2019, 16. [Google Scholar] [CrossRef]
- Elzinga, G.; Raviglione, M.C.; Maher, D. Scale up: Meeting targets in global tuberculosis control. Lancet 2004, 363, 814–819. [Google Scholar] [CrossRef]
- Afshari, M.; Aarabi, M.; Parsaee, M.; Nezammahalleh, A.; Moosazadeh, M. Determinant factors of drug resistant tuberculosis in Iran, a case control study. Clin. Epidemiol. Glob. Health 2019, 7, 322–324. [Google Scholar] [CrossRef] [Green Version]
- Nagaraja, C.; Shashibhushan, B.L.; Sagar, C.; Asif, M.; Manjunath, P.H. Manjunath Resistance pattern in drug-resistant pulmonary tuberculosis. J. Post Grad. Med. 2011, 57, 181–183. [Google Scholar] [CrossRef]
- Sharma, S.K.; Kumar, S.; Saha, P.; George, N.; Arora, S.; Gupta, D.; Singh, U.; Hanif, M.; Vashisht, R. Prevalance of multidrug-resistant tuberculosis among category II pulmonary tuberculosis patients. Indian J. Med. Res. 2011, 133, 312–315. [Google Scholar] [PubMed]
- Tatar, D.; Senol, G.; Cosar, D.; Ozacar, R.; Halilcolar, H. Patterns of drug resistance in pulmonary tuberculosis cases in the Izmir district, Turkey. New Microbiol. 2009, 32, 31–37. [Google Scholar] [PubMed]
- Daniel, O.; Osman, E. Prevalence and Risk Factors Associated with Drug Resistant TB in South West, Nigeria. Asian Pac. J. Trop. Med. 2011, 4, 148–151. [Google Scholar] [CrossRef]
- Gaude, G.S.; Praveenkumar; Hattiholli, J. Drug resistance patterns among pulmonary tuberculosis patients in a tertiary care hospital in northern Karnataka. J. Med. Trop. 2015, 17, 81–86. [Google Scholar] [CrossRef]
- Li, Q.; Zhao, G.; Wu, L.; Lu, M.; Liu, W.; Wu, Y.; Wang, L.; Wang, K.; Qian, H.-Z.; Xie, L. Prevalence and patterns of drug resistance among pulmonary tuberculosis patients in Hangzhou, China. Antimicrob. Resist. Infect. Control 2018, 7, 61. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Union against Tuberculosis and Lung Disease. Anti-Tuberculosis Drug Resistance in the World: 4th Global Report. Available online: https://www.who.int/publications/i/item/9789241563611 (accessed on 15 June 2020).
- Abdella, K.; Abdissa, K.; Kebede, W.; Abebe, G. Drug resistance patterns of Mycobacterium tuberculosis complex and associated factors among retreatment cases around Jimma, Southwest Ethiopia. BMC Public Health 2015, 15, 599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, M.; Roy, N.; Banerjee, R.; Kishore, J.; Jakhar, A. Determinants of Drug Resistance in Previously-Treated Pulmonary Tuberculosis Patients Registered at a Chest Clinic in South Delhi, India. Cureus 2019, 11, e5541. [Google Scholar] [CrossRef] [Green Version]
- Baya, B.; Achenbach, C.J.; Kone, B.; Toloba, Y.; Dabitao, D.K.; Diarra, B.; Goita, D.; Diabaté, S.; Maiga, M.; Soumare, D.; et al. Clinical risk factors associated with multidrug-resistant tuberculosis (MDR-TB) in Mali. Int. J. Infect. Dis. 2019, 81, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rifat, M.; Hall, J.; Oldmeadow, C.; Husain, A.; Hinderaker, S.G.; Milton, A.H. Factors related to previous tuberculosis treatment of patients with multidrug-resistant tuberculosis in Bangladesh. BMJ Open 2015, 5, e008273. [Google Scholar] [CrossRef] [Green Version]
- Gler, M.T.; Macalintal, L.E.; Raymond, L.; Guilatco, R.; Quelapio, M.I.D.; Tupasi, T.E. Multidrug-resistant tuberculosis among previously treated patients in the Philippines. Int. J. Tuberc. Lung Dis. 2011, 15, 652–656. [Google Scholar] [CrossRef]
- Espinal, M.A.; Laserson, K.; Camacho, M.; Fusheng, Z.; Kim, S.J.; Tlali, E.; Smith, I.; Suarez, P.; Antunes, M.L.; George, A.G.; et al. Determinants of drug-resistant tuberculosis: Analysis of 11 countries. Int. J. Tuberc. Lung Dis. 2001, 5, 887–893. [Google Scholar]
- Villegas, L.; Otero, L.; Sterling, T.R.; Huaman, M.A.; Van der Stuyft, P.; Gotuzzo, E.; Seas, C. Prevalence, risk factors, and treatment outcomes of isoniazid- and rifampicin- mono-resistant pulmonary tuberculosis in Lima, Peru. PLoS ONE 2016, 11, e0152933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prach, L.M.; Pascopella, L.; Barry, P.M.; Flood, J.; Porco, T.C.; Hopewell, P.C.; Metcalfe, J.Z. Rifampin monoresistant tuberculosis and HIV comorbidity in California, 1993–2008. Aids 2013, 27, 2615–2622. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Frequency (n) | Percentage (%) |
|---|---|---|
| Sex (n = 2555) | ||
| Male | 1710 | 66.93 |
| Female | 845 | 33.07 |
| Age (yrs.) (n = 2555) | ||
| ≤20 | 201 | 7.87 |
| 21–30 | 687 | 26.89 |
| 31–40 | 899 | 35.19 |
| 41–50 | 465 | 18.20 |
| 51–60 | 196 | 7.67 |
| 60+ | 107 | 4.19 |
| Patient group # (n = 2476) | ||
| New | 567 | 22.90 |
| Previously treated | 1909 | 77.10 |
| No of previous treatment # (n = 823) | ||
| 1 | 302 | 36.70 |
| 2 | 411 | 49.94 |
| 3+ | 110 | 13.37 |
| DR-TB category # (n = 1897) | ||
| Mono-DR | 527 | 27.78 |
| RIF Resistant | 176 | 9.28 |
| Poly-DR | 29 | 1.53 |
| MDR | 1165 | 61.41 |
| Zone current address # (n = 2438) | ||
| NE | 221 | 9.06 |
| NC | 400 | 16.41 |
| NW | 368 | 15.09 |
| SS | 354 | 14.52 |
| SE | 195 | 8.00 |
| SW | 900 | 36.92 |
| HIV Status # (n= 1303) | ||
| Positive | 305 | 23.41 |
| Negative | 998 | 76.59 |
| Mono-DR | RIF-Resistant | Poly DR | MDR | df | χ2 (p-Value) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n(%) | 95% CI | n(%) | 95% CI | n(%) | 95% CI | n(%) | 95% CI | |||
| Sex | ||||||||||
| Male | 349 (66.22) | 62.08–70.13 | 120 (68.18) | 60.75–74.99 | 18 (62.07) | 42.26–79.31 | 801 (68.76) | 66.04–71.35 | 3 | 3.31 (0.511) |
| Female | 178 (33.78) | 29.87–37.92 | 56 (31.82) | 25.01–39.25 | 11 (37.93) | 20.69–57.74 | 364 (31.24) | 28.65–33.96) | ||
| Age (yrs.) | ||||||||||
| ≤20 | 36 (6.83) | 4.97–9.31 | 12 (6.82) | 3.57–11.61 | 2 (6.90) | 0.85–22.77 | 99 (8.50) | 7.03–10.24 | 15 | 14.80 (0.466) |
| 21–30 | 161 (30.55) | 26.77–34.61 | 41 (23.30) | 17.27–30.25 | 7 (24.14) | 10.30–43.54 | 307 (26.35) | 23.90–28.96 | ||
| 31–40 | 177 (33.59) | 29.69–37.72 | 64 (36.36) | 29.26–43.94 | 12 (41.38) | 23.52–61.06 | 414 (35.54) | 32.84–38.33 | ||
| 41–50 | 86 (16.32) | 13.41–19.72 | 33 (18.75) | 13.27–25.31 | 4 (13.79) | 3.89–31.66 | 214 (18.37) | 16.25–20.70 | ||
| 51–60 | 42 (7.97) | 5.95–10.60 | 18 (10.23) | 6.17–15.68 | 1 (3.45) | 0.09–17.76 | 92 (7.90) | 6.48–9.59 | ||
| 60+ | 25 (4.74) | 3.23–6.91 | 8 (4.55) | 1.98–8.76 | 3 (10.34) | 2.19–27.35 | 39 (3.35) | 2.46–4.54 | ||
| Patient group | ||||||||||
| New | 109 (20.76) | 17.51–24.44 | 46 (26.14) | 19.81–33.28 | 6 (20.69) | 7.99–39.72 | 253 (21.81) | 19.53–24.28 | 3 | 3.24 (0.366) |
| Previously treated | 416 (79.24) | 75.56–82.49 | 130 (73.86) | 66.72–80.19 | 23 (79.31) | 60.28–92.01 | 907 (78.19) | 75.72–80.47 | ||
| No of previous treatment | ||||||||||
| 1 | 80 (35.40) | 29.17–42.01 | 37 (59.68) | 46.45–71.95 | 2 (14.29) | 1.78–42.81 | 113 (32.47) | 27.77–37.56 | 6 | 36.39 (0.001) * |
| 2 | 118 (52.21) | 45.49–58.88) | 25 (40.32) | 28.05–53.55 | 11 (78.57) | 49.20–95.34 | 166 (47.70) | 42.51–52.95 | ||
| 3+ | 28 (12.39) | 8.39–17.41 | - | - | 1 (7.14) | 0.18–33.87 | 69 (19.83) | 15.98–24.34 | ||
| Zone current address | ||||||||||
| NE | 42 (8.09) | 6.04–10.76 | 11 (6.47) | 3.27–11.28 | 5 (17.24) | 5.85–35.77 | 114 (10.57) | 8.87–12.54 | 15 | 98.26 (0.001) * |
| NC | 74 (14.26) | 11.51–17.53 | 24 (14.12) | 9.26–20.27 | 6 (20.69) | 7.99–39.72 | 207 (19.18) | 16.95–21.64 | ||
| NW | 96 (18.50) | 15.39–22.06 | 53 (31.18) | 24.30–38.72 | 5 (17.24) | 5.85–35.77 | 193 (17.89) | 15.72–20.29 | ||
| SS | 96 (18.50) | 15.39–22.06 | 18 (10.59) | 6.40–16.22 | 6 (20.69) | 7.99–39.72 | 154 (14.27) | 12.31–16.49 | ||
| SE | 58 (11.18) | 8.74–14.18 | 6 (3.53) | 1.31–7.52 | 3 (10.34) | 2.19–27.35 | 87 (8.06) | 6.58–9.84 | ||
| SW | 153 (29.48) | 25.72–33.54 | 58 (34.12) | 1.31–41.77 | 4 (13.79) | 3.89–31.66 | 324 (30.03) | 27.37–32.83 | ||
| HIV Status (n= 1303) | ||||||||||
| Positive | 60 (23.26) | 18.24–28.90 | 27 (24.77) | 17.0–33.96 | 6 (42.86) | 17.66–71.14 | 120 (22.60) | 19.25–26.35 | 3 | 3.26 (0.353) |
| Negative | 198 (76.74) | 71.10–81.76 | 82 (75.23) | 66.04–83.0 | 8 (57.14) | 28.86–82.34 | 411 (77.40) | 73.65–80.75 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oladimeji, O.; Othman, Y.; Oladimeji, K.E.; Atiba, B.P.; Adepoju, V.A.; Odugbemi, B.A. Patterns of Presentation of Drug-Resistant Tuberculosis in Nigeria: A Retrospective File Review. Microbiol. Res. 2022, 13, 609-619. https://doi.org/10.3390/microbiolres13030043
Oladimeji O, Othman Y, Oladimeji KE, Atiba BP, Adepoju VA, Odugbemi BA. Patterns of Presentation of Drug-Resistant Tuberculosis in Nigeria: A Retrospective File Review. Microbiology Research. 2022; 13(3):609-619. https://doi.org/10.3390/microbiolres13030043
Chicago/Turabian StyleOladimeji, Olanrewaju, Yasir Othman, Kelechi Elizabeth Oladimeji, Bamidele Paul Atiba, Victor Abiola Adepoju, and Babatunde Adeniran Odugbemi. 2022. "Patterns of Presentation of Drug-Resistant Tuberculosis in Nigeria: A Retrospective File Review" Microbiology Research 13, no. 3: 609-619. https://doi.org/10.3390/microbiolres13030043