
Loop-Mediated Isothermal Amplification as Point-of-Care Testing for EGFR-Mutated Lung Adenocarcinoma

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
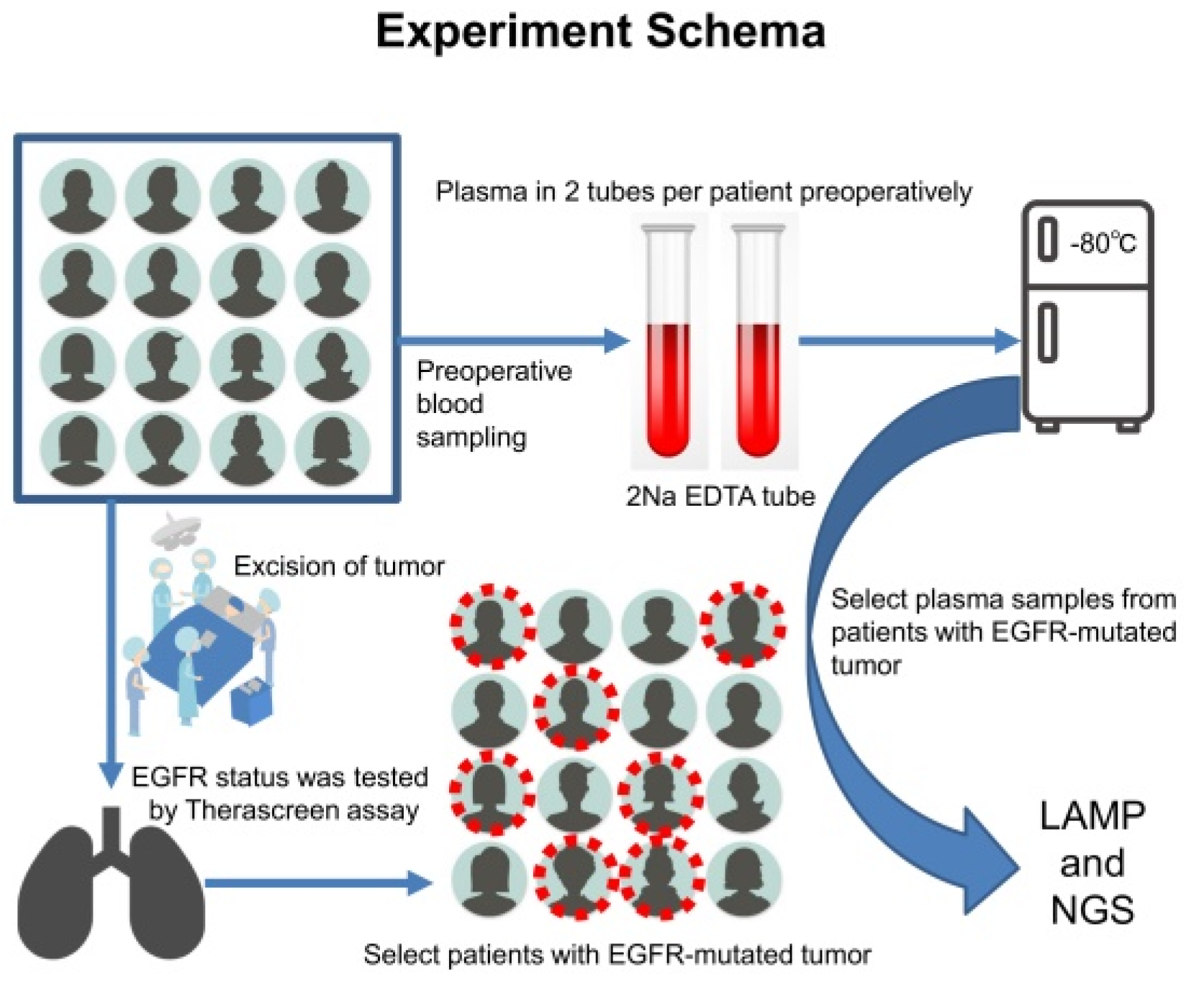
2.1. Study Design
2.2. Plasma Samples and DNA Extraction
2.3. Pathological Diagnosis and Therascreen qPCR Mutation Analysis
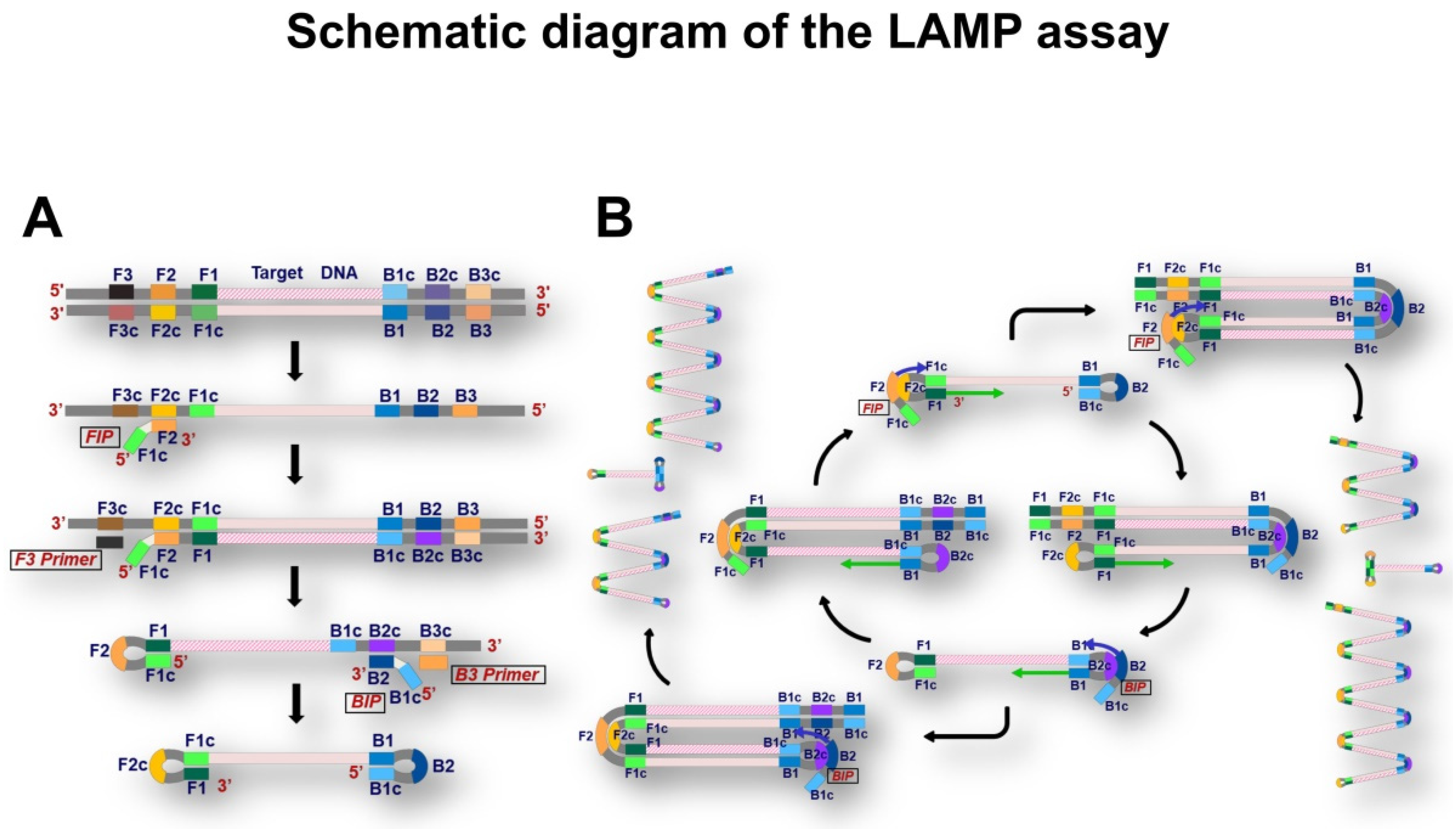
2.4. LAMP Mutation Analysis
2.5. Next-Generation Sequencing
2.6. Statistical Analysis
3. Results
3.1. Examination of the Efficacy of EGFR-LAMP Liquid Biopsy
3.2. Characteristics of Patients with EGFR-Mutated Adenocarcinoma
3.3. Amount of cfDNA Extracted from Plasma Samples
3.4. Therascreen EGFR PCR Mutation Analysis for Resected or Biopsied Tumors
3.5. Comparison of Results of the LAMP and the NGS Assays
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.Y.; Park, K.; Kim, S.W.; Lee, D.H.; Kim, H.Y.; Kim, H.T.; Ahn, M.J.; Yun, T.; Ahn, J.S.; Suh, C.; et al. First-SIGNAL: First-line single-agent iressa versus gemcitabine and cisplatin trial in never-smokers with adenocarcinoma of the lung. J. Oncol. 2012, 30, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Yang, J.C.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.L.; Zhou, C.; Hu, C.P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- The Japanese Lung Cancer Society: Guidelines of Lung Cancer. Available online: https://www.haigan.gr.jp/modules/guideline/index.php?content_id=3 (accessed on 29 December 2021).
- Hanna, N.H.; Robinson, A.G.; Temin, S.; Baker, S., Jr.; Brahmer, J.R.; Ellis, P.M.; Gaspar, L.E.; Haddad, R.Y.; Hesketh, P.J.; Jain, D.; et al. Therapy for Stage IV Non-Small-Cell Lung Cancer with Driver Alterations: ASCO and OH (CCO) Joint Guideline Update. J. Clin. Oncol. 2021, 39, 1040–1091. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalemkerian, G.P.; Narula, N.; Kennedy, E.B.; Biermann, W.A.; Donington, J.; Leighl, N.B.; Lew, M.; Pantelas, J.; Ramalingam, S.S.; Reck, M.; et al. Molecular Testing Guideline for the Selection of Patients With Lung Cancer for Treatment With Targeted Tyrosine Kinase Inhibitors: American Society of Clinical Oncology Endorsement of the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 911–919. [Google Scholar] [CrossRef] [PubMed]
- The Japan Lung Cancer Society, Guidance of Examinations of EGFR Mutations for Patients with Lung Cancer ver5.0. Available online: https://www.haigan.gr.jp/modules/tebiki/index.php?content_id=5 (accessed on 29 December 2021).
- The Japan Lung Cancer Society, Guidance of Examinations of ALK Fusion Gene for Patients with Lung Cancer ver3.1. Available online: https://www.haigan.gr.jp/modules/tebiki/index.php?content_id=9 (accessed on 29 December 2021).
- The Japan Lung Cancer Society, Guidance of Examinations of ROS1 Fusion Gene for Patients with Lung Cancer ver1.0. Available online: https://www.haigan.gr.jp/modules/tebiki/index.php?content_id=7 (accessed on 29 December 2021).
- The Japan Lung Cancer Society, Guidance of Examinations of BRAF Mutations for Patients with Lung Cancer ver1.0. Available online: https://www.haigan.gr.jp/modules/tebiki/index.php?content_id=4 (accessed on 29 December 2021).
- Takano, C.; Kuramochi, Y.; Seki, M.; Kim, D.W.; Omagari, D.; Sasano, M.; Chang, B.; Ohnishi, M.; Kim, E.J.; Fuwa, K.; et al. Molecular serotype-specific identification of Streptococcus pneumoniae using loop-mediated isothermal amplification. Sci. Rep. 2019, 9, 19823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quyen, T.L.; Nordentoft, S.; Vinayaka, A.C.; Ngo, T.A.; Engelsmenn, P.; Sun, Y.; Madsen, M.; Bang, D.D.; Wolff, A. A Sensitive, Specific and Simple Loop Mediated Isothermal Amplification Method for Rapid Detection of Campylobacter spp. in Broiler Production. Front. Microbiol. 2019, 10, 2443. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Y.; Jiao, W.; Li, J.; Quan, S.; Sun, L.; Wang, Y.; Qi, X.; Wang, X.; Shen, A. Development of loop-mediated isothermal amplification coupled with nanoparticle-based lateral flow biosensor assay for Mycoplasma pneumoniae detection. AMB Express 2019, 9, 196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, K.; Horita, N.; Yamamoto, M.; Tsukahara, T.; Nagakura, H.; Tashiro, K.; Shibata, Y.; Watanabe, H.; Nakashima, K.; Ushio, R.; et al. Diagnostic test accuracy of loop-mediated isothermal amplification assay for Mycobacterium tuberculosis: Systematic review and meta-analysis. Sci. Rep. 2016, 6, 39090. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bustin, S.A.; Nolan, T. RT-qPCR Testing of SARS-CoV-2: A Primer. Int. J. Mol. Sci. 2020, 21, 3004. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Wu, X.; Wan, Z.; Li, Y.; Zuo, L.; Qin, J.; Jin, X.; Zhang, C. Development of a Novel Reverse Transcription Loop-Mediated Isothermal Amplification Method for Rapid Detection of SARS-CoV-2. Virol. Sin. 2020, 35, 344–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, G.S.; Ku, K.; Baek, S.H.; Kim, S.J.; Kim, S.I.; Kim, B.T.; Maeng, J.S. Development of Reverse Transcription Loop-Mediated Isothermal Amplification Assays Targeting Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). J. Mol. Diagn. 2020, 22, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Xiao, H.; Zhang, Q. Systematic review: Comparison of Xpert MTB/RIF, LAMP and SAT methods for the diagnosis of pulmonary tuberculosis. Tuberculosis (Edinb.) 2016, 96, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Aryan, E.; Makvandi, M.; Farajzadeh, A.; Huygen, K.; Alvandi, A.H.; Gouya, M.M.; Sadrizadeh, A.; Romano, M. Clinical value of IS6110-based loop-mediated isothermal amplification for detection of Mycobacterium tuberculosis complex in respiratory specimens. J. Infect. 2013, 66, 487–493. [Google Scholar] [CrossRef] [PubMed]
- The Use of Loop-Mediated Isothermal Amplification (TB-LAMP) for the Diagnosis of Pulmonary Tuberculosis: Policy Guidance; World Health Organization: Geneva, Switzerland, 2016. [PubMed]
- WHO Consolidated Guidelines on Tuberculosis: Module 3: Diagnosis—Rapid Diagnostics for Tuberculosis Detection [Internet]; World Health Organization: Geneva, Switzerland, 2020. [PubMed]
- García-Basteiro, A.L.; DiNardo, A.; Saavedra, B.; Silva, D.R.; Palmero, D.; Gegia, M.; Migliori, G.B.; Duarte, R.; Mambuque, E.; Centis, R.; et al. Point of care diagnostics for tuberculosis. Pulmonology 2018, 24, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Takahashi, N.; Matsui, A.; Michiyuki, S.; Yamauchi, Y.; Shimizu, Y.; Hoshi, E.; Sakao, Y.; Kawamura, M. Comparative study of the loop-mediated isothermal amplification method and the QIAGEN therascreen PCR kit for the detection of EGFR mutations in non-small cell lung cancer. J. Thorac. Dis. 2021, 13, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Lucci, A.; Ignatiadis, M.; Jeffrey, S.S. Cell-free circulating tumor DNA profiling in cancer management. Trends Mol. Med. 2021, 27, 1014–1015. [Google Scholar] [CrossRef] [PubMed]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrba, L.; Oshiro, M.M.; Kim, S.S.; Garland, L.L.; Placencia, C.; Mahadevan, D.; Nelson, M.A.; Futscher, B.W. DNA methylation biomarkers discovered in silico detect cancer in liquid biopsies from non-small cell lung cancer patients. Epigenetics 2020, 15, 419–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, D.; Tiirikainen, M. Diagnostic Power of DNA Methylation Classifiers for Early Detection of Cancer. Trends Cancer 2020, 6, 78–81. [Google Scholar] [CrossRef] [PubMed]
- The Japanese Society of Pathology, Regulations for Handling Pathological Tissue Specimens for Genomic Medicine. Available online: http://pathology.or.jp/genome_med/pdf/textbook.pdf (accessed on 29 December 2021).
- Vallée, A.; Le Loupp, A.G.; Denis, M.G. Efficiency of the Therascreen® RGQ PCR kit for the detection of EGFR mutations in non-small cell lung carcinomas. Clin. Chim. Acta 2014, 15, 429. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, S.; Saito, Y.; Matsui, A.; Takahashi, N.; Ikeya, T.; Hoshi, E.; Shimizu, Y.; Yasuda, M. A novel loop-mediated isothermal amplification method for efficient and robust detection of EGFR mutations. Int. J. Oncol. 2020, 56, 743–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Non-Small Cell Lung Cancer Version 1.2022-December 7, 2021. Available online: https://www2.tri-kobe.org/nccn/guideline/lung/english/non_small.pdf (accessed on 29 December 2021).
- ISO 22870:2006. Point-of-Care Testing (POCT)-Requirements for Quality and Competence. Available online: https://www.iso.org/standard/35173.html (accessed on 29 December 2021).
- Augustine, R.; Hasan, A.; Das, S.; Ahmed, R.; Mori, Y.; Notomi, T.; Kevadiya, B.D.; Thakor, A.S. Loop-Mediated Isothermal Amplification (LAMP): A Rapid, Sensitive, Specific, and Cost-Effective Point-of-Care Test for Coronaviruses in the Context of COVID-19 Pandemic. Biology 2020, 9, 182. [Google Scholar] [CrossRef] [PubMed]
- Asaka, S.; Yoshizawa, A.; Saito, K.; Kobayashi, Y.; Yamamoto, H.; Negishi, T.; Nakata, R.; Matsuda, K.; Yamaguchi, A.; Honda, T. Rapid point-of-care testing for epidermal growth factor receptor gene mutations in patients with lung cancer using cell-free DNA from cytology specimen supernatants. Int. J. Oncol. 2018, 52, 2110–2118. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) |
|---|---|
| Age, years | 68.7 ± 8.4 |
| Sex | |
| Male | 20 (29.2) |
| Female | 31 (70.8) |
| Smoking Status | |
| Never smoker | 22 (43.1) |
| Former smoker | 23 (45.1) |
| Current smoker | 6 (11.8) |
| Subtype of adenocarcinoma | |
| Papillary predominant | 45 (88.0) |
| Lepidic predominant | 4 (8.0) |
| Micropapillary predominant | 1 (2.0) |
| Solid predominant | 1 (2.0) |
| Pathological stage | |
| pIA1 | 12 (24.0) |
| pIA2 | 21 (41.0) |
| pIA3 | 6 (12.0) |
| pIB | 2 (4.0) |
| pIIB | 3 (6.0) |
| pIIIA | 4 (8.0) |
| pIIIB | 1 (2.0) |
| pIVA | 1 (2.0) |
| pIVB | 1 (2.0) |
| Number | Percentage (%) | |
|---|---|---|
| Del 19 | 27 | 52.9 |
| L858R | 18 | 35.3 |
| Ins 20 | 2 | 3.9 |
| Ex 19 del + Ins 20 | 2 | 3.9 |
| Del 19 + G719X | 1 | 2.0 |
| G719X + Ex 18 | 1 | 2.0 |
| Total | 51 | 100 |
| Tumor | Plasma | ||||
|---|---|---|---|---|---|
| p-Stage | Therascreen | LAMP | LAMP | NGS | |
| Case 1 | IVB | L858R | L858R | L858R | L858R |
| Case 2 | IIIA | L858R | negative | negative | L858R |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, Y.; Matsui, A.; Michiyuki, S.; Morooka, H.; Ibi, T.; Yamauchi, Y.; Takahashi, N.; Shimizu, Y.; Ikeya, T.; Hoshi, E.; et al. Loop-Mediated Isothermal Amplification as Point-of-Care Testing for EGFR-Mutated Lung Adenocarcinoma. Micromachines 2022, 13, 897. https://doi.org/10.3390/mi13060897
Saito Y, Matsui A, Michiyuki S, Morooka H, Ibi T, Yamauchi Y, Takahashi N, Shimizu Y, Ikeya T, Hoshi E, et al. Loop-Mediated Isothermal Amplification as Point-of-Care Testing for EGFR-Mutated Lung Adenocarcinoma. Micromachines. 2022; 13(6):897. https://doi.org/10.3390/mi13060897
Chicago/Turabian StyleSaito, Yuichi, Atsuka Matsui, Satoru Michiyuki, Hiroaki Morooka, Takayuki Ibi, Yoshikane Yamauchi, Nobumasa Takahashi, Yoshihiko Shimizu, Tomohiko Ikeya, Eishin Hoshi, and et al. 2022. "Loop-Mediated Isothermal Amplification as Point-of-Care Testing for EGFR-Mutated Lung Adenocarcinoma" Micromachines 13, no. 6: 897. https://doi.org/10.3390/mi13060897