Interpretation of Multivariate Association Patterns between Multicollinear Physical Activity Accelerometry Data and Cardiometabolic Health in Children—A Tutorial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Statistical Analyses
3. Results
3.1. Children’s Characteristics
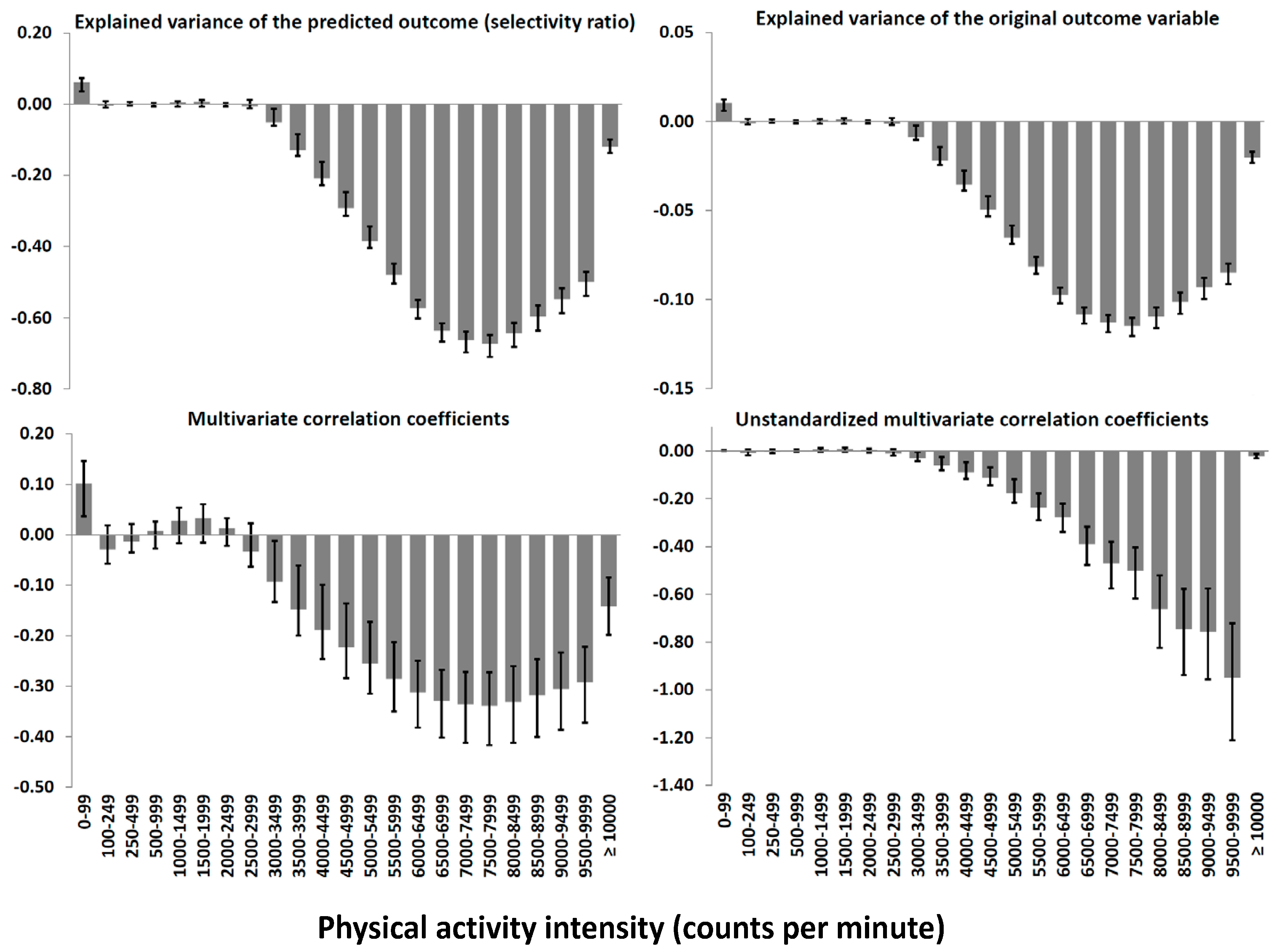
3.2. The Multivariate Association Pattern Displayed Using Different Statistics
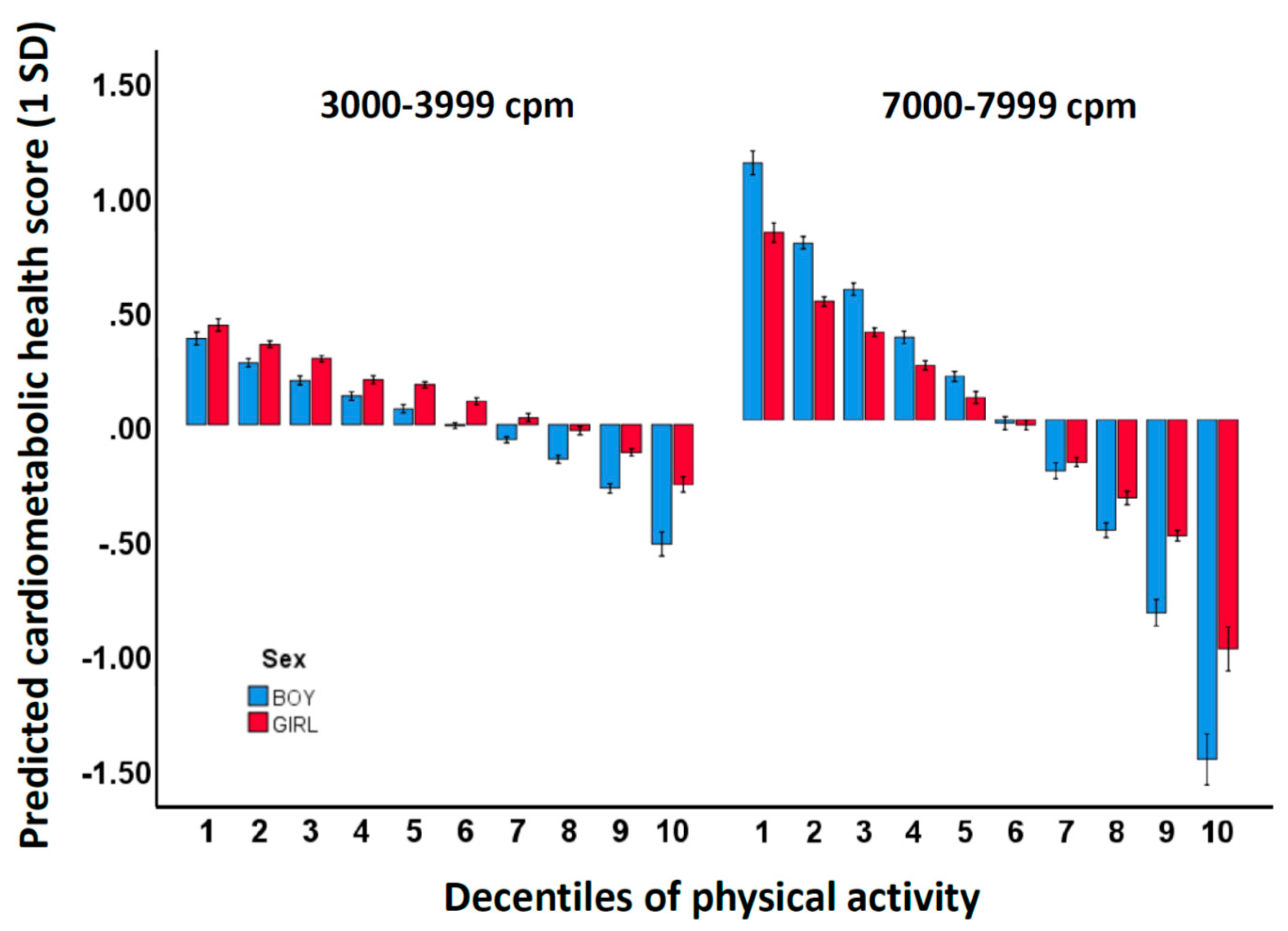
3.3. Prediction of Cardiometabolic Health across Decentiles of PA
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef] [PubMed]
- van der Ploeg, H.P.; Hillsdon, M. Is sedentary behaviour just physical inactivity by another name? Int. J. Behav. Nutr. Phys. Act. 2017, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Aadland, E.; Kvalheim, O.M.; Anderssen, S.A.; Resaland, G.K.; Andersen, L.B. The multivariate physical activity signature associated with metabolic health in children. Int. J. Behav. Nutr. Phys. Act. 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Pedisic, Z. Measurement issues and poor adjustments for physical activity and sleep undermine sedentary behaviour research—The focus should shift to the balance between sleep, sedentary behaviour, standing and activity. Kinesiology 2014, 46, 135–146. [Google Scholar]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Bahavioral Sciences, 3rd ed.; Routledge: New York, NY, USA, 2003. [Google Scholar]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Connor Gorber, S.; Kho, M.E.; Sampson, M.; et al. Combinations of physical activity, sedentary behaviour and sleep: Relationships with health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S283–S293. [Google Scholar] [CrossRef] [PubMed]
- Mekary, R.A.; Willett, W.C.; Hu, F.B.; Ding, E.L. Isotemporal Substitution Paradigm for Physical Activity Epidemiology and Weight Change. Am. J. Epidemiol. 2009, 170, 519–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, B.H.; Anderssen, S.A.; Andersen, L.B.; Hildebrand, M.; Kolle, E.; Steene-Johannessen, J.; Kriemler, S.; Page, A.S.; Puder, J.J.; Reilly, J.J.; et al. Cross-Sectional Associations of Reallocating Time Between Sedentary and Active Behaviours on Cardiometabolic Risk Factors in Young People: An International Children’s Accelerometry Database (ICAD) Analysis. Sports Med. 2018, 48, 2401–2412. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined Effects of Time Spent in Physical Activity, Sedentary Behaviors and Sleep on Obesity and Cardio-Metabolic Health Markers: A Novel Compositional Data Analysis Approach. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Stanford, T.E.; Martin-Fernandez, J.A.; Pedisic, Z.; Maher, C.A.; Lewis, L.K.; Hron, K.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; et al. Compositional data analysis for physical activity, sedentary time and sleep research. Stat. Methods Med. Res. 2018, 27, 3726–3738. [Google Scholar] [CrossRef]
- Aadland, E.; Andersen, L.B.; Anderssen, S.A.; Resaland, G.K.; Kvalheim, O.M. Associations of volumes and patterns of physical activity with metabolic health in children: A multivariate pattern analysis approach. Prev. Med. 2018, 115, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Aadland, E.; Kvalheim, O.M.; Anderssen, S.A.; Resaland, G.K.; Andersen, L.B. The Triaxial Physical Activity Signature Associated with Metabolic Health in Children. Med. Sci. Sports Exerc. 2019. [Google Scholar] [CrossRef]
- Rajalahti, T.; Kvalheim, O.M. Multivariate data analysis in pharmaceutics: A tutorial review. Int. J. Pharm. 2011, 417, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Madsen, R.; Lundstedt, T.; Trygg, J. Chemometrics in metabolomics—A review in human disease diagnosis. Anal. Chim. Acta 2010, 659, 23–33. [Google Scholar] [CrossRef]
- Rajalahti, T.; Kroksveen, A.C.; Arneberg, R.; Berven, F.S.; Vedeler, C.A.; Myhr, K.M.; Kvalheim, O.M. A multivariate approach to reveal biomarker signatures for disease classification: Application to mass spectral profiles of cerebrospinal fluid from patients with multiple sclerosis. J. Proteome Res. 2010, 9, 3608–3620. [Google Scholar] [CrossRef] [PubMed]
- Wold, S.; Ruhe, A.; Wold, H.; Dunn, W.J., III. The collinearity problem in linear-regression—The partial least-squares (PLS) approach to generalized inverses. Siam J. Sci. Stat. Comput. 1984, 5, 735–743. [Google Scholar] [CrossRef]
- Rajalahti, T.; Arneberg, R.; Berven, F.S.; Myhr, K.M.; Ulvik, R.J.; Kvalheim, O.M. Biomarker discovery in mass spectral profiles by means of selectivity ratio plot. Chemom. Intell. Lab. Syst. 2009, 95, 35–48. [Google Scholar] [CrossRef]
- Rajalahti, T.; Arneberg, R.; Kroksveen, A.C.; Berle, M.; Myhr, K.-M.; Kvalheim, O.M. Discriminating Variable Test and Selectivity Ratio Plot: Quantitative Tools for Interpretation and Variable (Biomarker) Selection in Complex Spectral or Chromatographic Profiles. Anal. Chem. 2009, 81, 2581–2590. [Google Scholar] [CrossRef] [PubMed]
- Resaland, G.K.; Moe, V.F.; Aadland, E.; Steene-Johannessen, J.; Glosvik, Ø.; Andersen, J.R.; Kvalheim, O.M.; McKay, H.A.; Anderssen, S.A. Active Smarter Kids (ASK): Rationale and design of a cluster-randomized controlled trial investigating the effects of daily physical activity on children’s academic performance and risk factors for non-communicable diseases. BMC Public Health 2015, 15, 709. [Google Scholar] [CrossRef]
- Resaland, G.K.; Aadland, E.; Moe, V.F.; Aadland, K.N.; Skrede, T.; Stavnsbo, M.; Suominen, L.; Steene-Johannessen, J.; Glosvik, Ø.; Andersen, J.R.; et al. Effects of physical activity on schoolchildren’s academic performance: The Active Smarter Kids (ASK) cluster-randomized controlled trial. Prev. Med. 2016, 91, 322–328. [Google Scholar] [CrossRef]
- John, D.; Freedson, P. ActiGraph and Actical physical activity monitors: A peek under the hood. Med. Sci. Sports Exerc. 2012, 44, S86–S89. [Google Scholar] [CrossRef]
- Froberg, A.; Berg, C.; Larsson, C.; Boldemann, C.; Raustorp, A. Combinations of Epoch Durations and Cut-Points to Estimate Sedentary Time and Physical Activity Among Adolescents. Meas. Phys. Educ. Exerc. Sci. 2017, 21, 154–160. [Google Scholar] [CrossRef]
- Aadland, E.; Andersen, L.B.; Anderssen, S.A.; Resaland, G.K. A comparison of 10 accelerometer non-wear time criteria and logbooks in children. BMC Public Health 2018, 18, 9. [Google Scholar] [CrossRef] [PubMed]
- Aadland, E.; Andersen, L.B.; Skrede, T.; Ekelund, U.; Anderssen, S.A.; Resaland, G.K. Reproducibility of Objectively Measured Physical Activity and Sedentary Time over Two Seasons in Children; Comparing a Day-by-Day and a Week-by-Week Approach. PLoS ONE 2017, 12, e0189304. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of Accelerometer Cut Points for Predicting Activity Intensity in Youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Aadland, E.; Terum, T.; Mamen, A.; Andersen, L.B.; Resaland, G.K. The Andersen aerobic fitness test: Reliability and validity in 10-year-old children. PLoS ONE 2014, 9, e110492. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Andersen, L.B.; Harro, M.; Sardinha, L.B.; Froberg, K.; Ekelund, U.; Brage, S.; Anderssen, S.A. Physical activity and clustered cardiovascular risk in children: A cross-sectional study (The European Youth Heart Study). Lancet 2006, 368, 299–304. [Google Scholar] [CrossRef]
- Kvalheim, O.M.; Karstang, T.V. Interpretation of latent-variable regression-models. Chemom. Intell. Lab. Syst. 1989, 7, 39–51. [Google Scholar] [CrossRef]
- Kvalheim, O.M.; Arneberg, R.; Grung, B.; Rajalahti, T. Determination of optimum number of components in partial least squares regression from distributions of the root-mean-squared error obtained by Monte Carlo resampling. J. Chemom. 2018. [Google Scholar] [CrossRef]
- Cain, K.L.; Sallis, J.F.; Conway, T.L.; Van Dyck, D.; Calhoon, L. Using accelerometers in youth physical activity studies: A review of methods. J. Phys. Activity Health 2013, 10, 437–450. [Google Scholar] [CrossRef]
- Ekelund, U.; Luan, J.A.; Sherar, L.B.; Esliger, D.W.; Griew, P.; Cooper, A.; International Children’s Accelerometry Database (ICAD) collaborators. Moderate to Vigorous Physical Activity and Sedentary Time and Cardiometabolic Risk Factors in Children and Adolescents. JAMA 2012, 307, 704–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarp, J.; Andersen, L.B.; Ostergaard, L. Quantification of underestimation of physical activity during cycling to school when using accelerometry. J. Phys. Activity Health 2015, 12, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Crouter, S.E.; Churilla, J.R.; Bassett, D.R. Estimating energy expenditure using accelerometers. Eur. J. Appl. Physiol. 2006, 98, 601–612. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 841) | Boys (n = 424) | Girls (n = 417) | p between Groups | |
|---|---|---|---|---|
| Demography | ||||
| Age (years) | 10.2 (0.3) | 10.2 (0.3) | 10.2 (0.3) | 0.803 |
| Anthropometry | ||||
| Body mass (kg) | 37.0 (8.1) | 36.8 (7.8) | 37.2 (8.3) | 0.641 |
| Height (cm) | 142.9 (6.7) | 143.1 (6.7) | 142.6 (6.8) | 0.197 |
| BMI (kg/m2) | 18.0 (3.0) | 17.9 (2.9) | 18.1 (3.1) | 0.218 |
| Overweight and obese (%) | 20.8 | 20.0 | 21.5 | 0.583 |
| Waist circumference (cm) | 61.9 (7.5) | 62.2 (7.3) | 61.6 (7.7) | 0.169 |
| Waist:height (ratio) | 0.43 (0.05) | 0.43 (0.05) | 0.43 (0.05) | 0.322 |
| Indices of cardiometabolic health | ||||
| Andersen test (m) | 898 (103) | 925 (112) | 871 (85) | <0.001 |
| Systolic blood pressure (mmHg) | 105.2 (8.4) | 105.3 (8.2) | 105.2 (8.6) | 0.612 |
| Diastolic blood pressure (mmHg) | 57.7 (6.2) | 57.4 (6.0) | 58.1 (6.3) | 0.180 |
| Total cholesterol (mmol/l) | 4.46 (0.69) | 4.46 (0.70) | 4.46 (0.68) | 0.976 |
| LDL-cholesterol (mmol/l) | 2.51 (0.64) | 2.50 (0.65) | 2.53 (0.62) | 0.570 |
| HDL-cholesterol (mmol/l) | 1.59 (0.35) | 1.63 (0.34) | 1.55 (0.35) | 0.001 |
| Total:HDL-cholesterol (ratio) | 2.91 (0.71) | 2.82 (0.66) | 2.99 (0.74) | 0.001 |
| Triglyceride (mmol/l) | 0.78 (0.38) | 0.72 (0.31) | 0.84 (0.42) | <0.001 |
| Glucose (mmol/l) | 4.98 (0.32) | 5.02 (0.31) | 4.94 (0.33) | 0.001 |
| Insulin (pmol/l) | 7.91 (4.29) | 7.05 (3.48) | 8.33 (4.83) | <0.001 |
| HOMA (index) | 1.71 (0.98) | 1.54 (0.83) | 1.89 (1.09) | <0.001 |
| Composite score (1SD) * | 0.00 (1.00) | 0.00 (0.93) | 0.00 (1.07) | - |
| Physical activity | ||||
| Wear time (min/day) | 795 (56) | 799 (59) | 791 (54) | 0.032 |
| Overall physical activity (cpm) | 708 (272) | 754 (296) | 660 (235) | <0.001 |
| SED (min/day) | 597 (56) | 593 (59) | 601 (53) | <0.001 |
| LPA (min/day) | 122 (22) | 124 (23) | 120 (21) | 0.065 |
| MPA (min/day) | 37 (10) | 39 (10) | 35 (8) | <0.001 |
| VPA (min/day) | 39 (15) | 43 (16) | 35 (12) | <0.001 |
| MVPA (min/day) | 76 (23) | 82 (24) | 70 (19) | <0.001 |
| Guideline amount (%) | 74 | 80 | 68 | <0.001 |
| Physical Activity Intensity (cpm) | Unstandardized Multivariate Regression Coefficients |
|---|---|
| 0–99 | 0.0018 |
| 100–999 | −0.0038 |
| 1000–1999 | 0.0068 |
| 2000–2999 | −0.0034 |
| 3000–3999 | −0.0453 |
| 4000–4999 | −0.1005 |
| 5000–5999 | −0.2070 |
| 6000–6999 | −0.3337 |
| 7000–7999 | −0.4857 |
| 8000–8999 | −0.7040 |
| 9000–9999 | −0.8522 |
| ≥10000 | −0.0217 |
| Physical Activity Intensity (cpm) | Decentiles of 3000–3999 cpm | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean | |
| Boys | |||||||||||
| 0–99 | 660 | 628 | 624 | 604 | 583 | 590 | 564 | 566 | 566 | 545 | 593 |
| 100–999 | 60.5 | 65.2 | 65.8 | 69.0 | 69.7 | 73.4 | 71.4 | 71.9 | 77.2 | 77.8 | 70.2 |
| 1000–1999 | 34.0 | 38.8 | 39.5 | 42.5 | 43.1 | 44.1 | 46.1 | 46.7 | 50.9 | 52.7 | 43.9 |
| 2000–2999 | 19.6 | 22.7 | 24.1 | 26.3 | 27.6 | 28.3 | 30.3 | 32.2 | 35.4 | 38.6 | 28.5 |
| 3000–3999 | 12.2 | 14.5 | 16.2 | 17.7 | 19.0 | 20.6 | 21.9 | 23.8 | 26.6 | 32.0 | 20.5 |
| 4000–4999 | 7.3 | 9.1 | 10.3 | 11.4 | 12.1 | 13.4 | 14.2 | 15.6 | 16.7 | 21.2 | 13.1 |
| 5000–5999 | 4.6 | 5.8 | 6.5 | 7.4 | 7.7 | 8.6 | 8.9 | 9.7 | 10.1 | 12.4 | 8.2 |
| 6000–6999 | 3.4 | 4.2 | 4.8 | 5.5 | 5.5 | 6.2 | 6.3 | 6.9 | 7.2 | 8.2 | 5.8 |
| 7000–7999 | 2.28 | 2.74 | 3.14 | 3.66 | 4.06 | 4.06 | 4.14 | 4.36 | 4.62 | 5.04 | 3.77 |
| 8000–8999 | 1.45 | 1.69 | 1.91 | 2.31 | 2.27 | 2.46 | 2.61 | 2.65 | 2.83 | 2.91 | 2.31 |
| 9000–9999 | 1.05 | 1.19 | 1.37 | 1.67 | 1.61 | 1.73 | 1.91 | 1.86 | 1.99 | 2.03 | 1.64 |
| ≥10000 | 4.18 | 5.30 | 6.34 | 7.15 | 8.43 | 8.82 | 10.81 | 11.03 | 9.22 | 10.06 | 8.14 |
| 2000–3999 | 31.8 | 37.2 | 40.3 | 44.0 | 46.6 | 48.9 | 52.2 | 56.0 | 62.0 | 70.6 | 49.0 |
| ≥4000 | 24.3 | 30.0 | 34.4 | 39.1 | 41.7 | 45.3 | 48.9 | 52.1 | 52.7 | 61.8 | 43.0 |
| Girls | |||||||||||
| 0–99 | 653 | 630 | 615 | 616 | 598 | 585 | 600 | 576 | 584 | 555 | 601 |
| 100–999 | 62.2 | 65.0 | 65.8 | 72.8 | 65.1 | 67.7 | 71.9 | 73.9 | 74.0 | 75.7 | 69.4 |
| 1000–1999 | 33.6 | 35.6 | 38.6 | 42.0 | 39.7 | 42.1 | 43.3 | 46.0 | 46.1 | 48.3 | 41.5 |
| 2000–2999 | 17.9 | 20.2 | 22.4 | 24.6 | 24.8 | 27.2 | 27.9 | 29.6 | 31.2 | 34.1 | 26.0 |
| 3000–3999 | 10.9 | 12.8 | 14.1 | 16.2 | 16.6 | 18.2 | 19.8 | 21.6 | 23.2 | 26.3 | 17.9 |
| 4000–4999 | 6.5 | 7.9 | 8.5 | 9.8 | 10.2 | 11.0 | 11.9 | 13.0 | 14.1 | 16.2 | 10.9 |
| 5000–5999 | 3.9 | 5.0 | 5.3 | 6.0 | 6.2 | 6.7 | 7.0 | 7.7 | 8.1 | 9.3 | 6.5 |
| 6000–6999 | 2.8 | 3.7 | 3.8 | 4.4 | 4.4 | 4.7 | 5.0 | 5.4 | 5.5 | 6.3 | 4.6 |
| 7000–7999 | 1.81 | 2.41 | 2.59 | 2.99 | 2.87 | 3.05 | 3.29 | 3.47 | 3.61 | 3.94 | 3.00 |
| 8000–8999 | 1.12 | 1.51 | 1.61 | 1.90 | 1.78 | 1.87 | 2.03 | 2.13 | 2.25 | 2.43 | 1.86 |
| 9000–9999 | 0.82 | 1.09 | 1.17 | 1.35 | 1.28 | 1.34 | 1.48 | 1.54 | 1.61 | 1.72 | 1.34 |
| ≥10000 | 3.79 | 6.16 | 5.39 | 6.95 | 7.20 | 6.79 | 8.22 | 9.13 | 9.07 | 8.80 | 7.15 |
| 2000–3999 | 28.8 | 33.0 | 36.5 | 40.8 | 41.4 | 45.4 | 47.7 | 51.2 | 54.4 | 60.4 | 43.9 |
| ≥4000 | 20.7 | 27.8 | 28.4 | 33.4 | 33.9 | 35.5 | 38.9 | 42.4 | 44.2 | 48.7 | 35.4 |
| Physical Activity Intensity (cpm) | Decentiles of 7000–7999 cpm | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean | |
| Boys | |||||||||||
| 0–99 | 647 | 624 | 605 | 602 | 586 | 586 | 573 | 583 | 569 | 554 | 593 |
| 100–999 | 61.1 | 68.2 | 71.6 | 69.7 | 72.2 | 68.6 | 70.0 | 73.4 | 73.5 | 73.5 | 70.2 |
| 1000–1999 | 36.5 | 41.5 | 42.9 | 43.6 | 45.3 | 42.7 | 44.6 | 46.2 | 47.3 | 48.1 | 43.9 |
| 2000–2999 | 22.9 | 26.0 | 27.5 | 27.6 | 29.1 | 27.8 | 30.0 | 30.0 | 31.3 | 33.0 | 28.5 |
| 3000–3999 | 15.1 | 17.2 | 18.5 | 19.5 | 20.9 | 20.1 | 22.1 | 22.2 | 23.5 | 25.8 | 20.5 |
| 4000–4999 | 8.2 | 10.0 | 10.8 | 12.4 | 13.3 | 12.9 | 14.4 | 14.9 | 16.1 | 18.4 | 13.1 |
| 5000–5999 | 4.4 | 5.7 | 6.2 | 7.3 | 8.0 | 8.0 | 9.1 | 9.7 | 10.7 | 12.5 | 8.2 |
| 6000–6999 | 2.8 | 3.7 | 4.2 | 4.8 | 5.4 | 5.8 | 6.5 | 7.2 | 8.2 | 9.8 | 5.8 |
| 7000–7999 | 1.55 | 2.23 | 2.59 | 3.02 | 3.41 | 3.77 | 4.20 | 4.72 | 5.45 | 6.81 | 3.77 |
| 8000–8999 | 0.91 | 1.33 | 1.55 | 1.83 | 2.07 | 2.32 | 2.57 | 2.87 | 3.36 | 4.28 | 2.31 |
| 9000–9999 | 0.64 | 0.94 | 1.09 | 1.31 | 1.50 | 1.66 | 1.79 | 2.02 | 2.38 | 3.07 | 1.64 |
| ≥10000 | 2.83 | 4.21 | 5.80 | 6.57 | 8.33 | 8.59 | 8.29 | 9.72 | 12.16 | 14.97 | 8.14 |
| 2000–3999 | 38.0 | 43.2 | 46.0 | 47.1 | 50.0 | 47.9 | 52.1 | 52.2 | 54.8 | 58.8 | 49.0 |
| ≥4000 | 21.3 | 28.1 | 32.2 | 37.2 | 42.0 | 43.0 | 46.9 | 51.1 | 58.4 | 69.8 | 43.0 |
| Girls | |||||||||||
| 0–99 | 646 | 624 | 620 | 607 | 597 | 587 | 604 | 590 | 567 | 567 | 601 |
| 100–999 | 61.6 | 66.7 | 69.8 | 66.3 | 71.0 | 66.4 | 71.4 | 72.2 | 72.1 | 76.1 | 69.4 |
| 1000–1999 | 34.9 | 38.9 | 40.4 | 38.6 | 42.6 | 40.8 | 42.2 | 43.8 | 48.2 | 20.7 | 41.5 |
| 2000–2999 | 20.7 | 23.2 | 24.4 | 23.7 | 26.6 | 26.4 | 27.0 | 28.7 | 27.4 | 31.8 | 26.0 |
| 3000–3999 | 13.2 | 15.2 | 16.4 | 16.5 | 18.0 | 18.2 | 19.2 | 19.9 | 19.5 | 23.1 | 17.9 |
| 4000–4999 | 7.2 | 8.7 | 9.6 | 10.0 | 10.7 | 11.1 | 11.8 | 12.3 | 12.6 | 15.1 | 10.9 |
| 5000–5999 | 3.8 | 4.9 | 5.6 | 5.8 | 6.5 | 6.8 | 7.1 | 7.6 | 7.8 | 9.7 | 6.5 |
| 6000–6999 | 2.4 | 3.2 | 3.7 | 3.9 | 4.5 | 4.7 | 5.1 | 5.5 | 5.8 | 7.2 | 4.6 |
| 7000–7999 | 1.38 | 1.93 | 2.27 | 2.48 | 2.82 | 3.05 | 3.34 | 3.70 | 4.01 | 5.05 | 3.00 |
| 8000–8999 | 0.82 | 1.20 | 1.33 | 1.50 | 1.72 | 1.89 | 2.05 | 2.32 | 2.58 | 3.24 | 1.86 |
| 9000–9999 | 0.58 | 0.87 | 0.96 | 1.07 | 1.22 | 1.36 | 1.45 | 1.71 | 1.87 | 2.30 | 1.34 |
| ≥10000 | 2.50 | 5.01 | 5.06 | 4.84 | 7.16 | 6.47 | 7.15 | 9.49 | 11.50 | 12.22 | 7.15 |
| 2000–3999 | 33.9 | 38.4 | 40.8 | 40.2 | 44.6 | 44.6 | 46.2 | 48.6 | 46.9 | 54.9 | 43.9 |
| ≥4000 | 16.2 | 20.8 | 23.5 | 24.8 | 27.5 | 28.9 | 30.8 | 33.1 | 34.7 | 42.6 | 28.2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aadland, E.; Andersen, L.B.; Resaland, G.K.; Kvalheim, O.M. Interpretation of Multivariate Association Patterns between Multicollinear Physical Activity Accelerometry Data and Cardiometabolic Health in Children—A Tutorial. Metabolites 2019, 9, 129. https://doi.org/10.3390/metabo9070129
Aadland E, Andersen LB, Resaland GK, Kvalheim OM. Interpretation of Multivariate Association Patterns between Multicollinear Physical Activity Accelerometry Data and Cardiometabolic Health in Children—A Tutorial. Metabolites. 2019; 9(7):129. https://doi.org/10.3390/metabo9070129
Chicago/Turabian StyleAadland, Eivind, Lars Bo Andersen, Geir Kåre Resaland, and Olav Martin Kvalheim. 2019. "Interpretation of Multivariate Association Patterns between Multicollinear Physical Activity Accelerometry Data and Cardiometabolic Health in Children—A Tutorial" Metabolites 9, no. 7: 129. https://doi.org/10.3390/metabo9070129