
Omega-3 Fatty Acids Reduce Remnant-like Lipoprotein Cholesterol and Improve the Ankle–Brachial Index of Hemodialysis Patients with Dyslipidemia: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
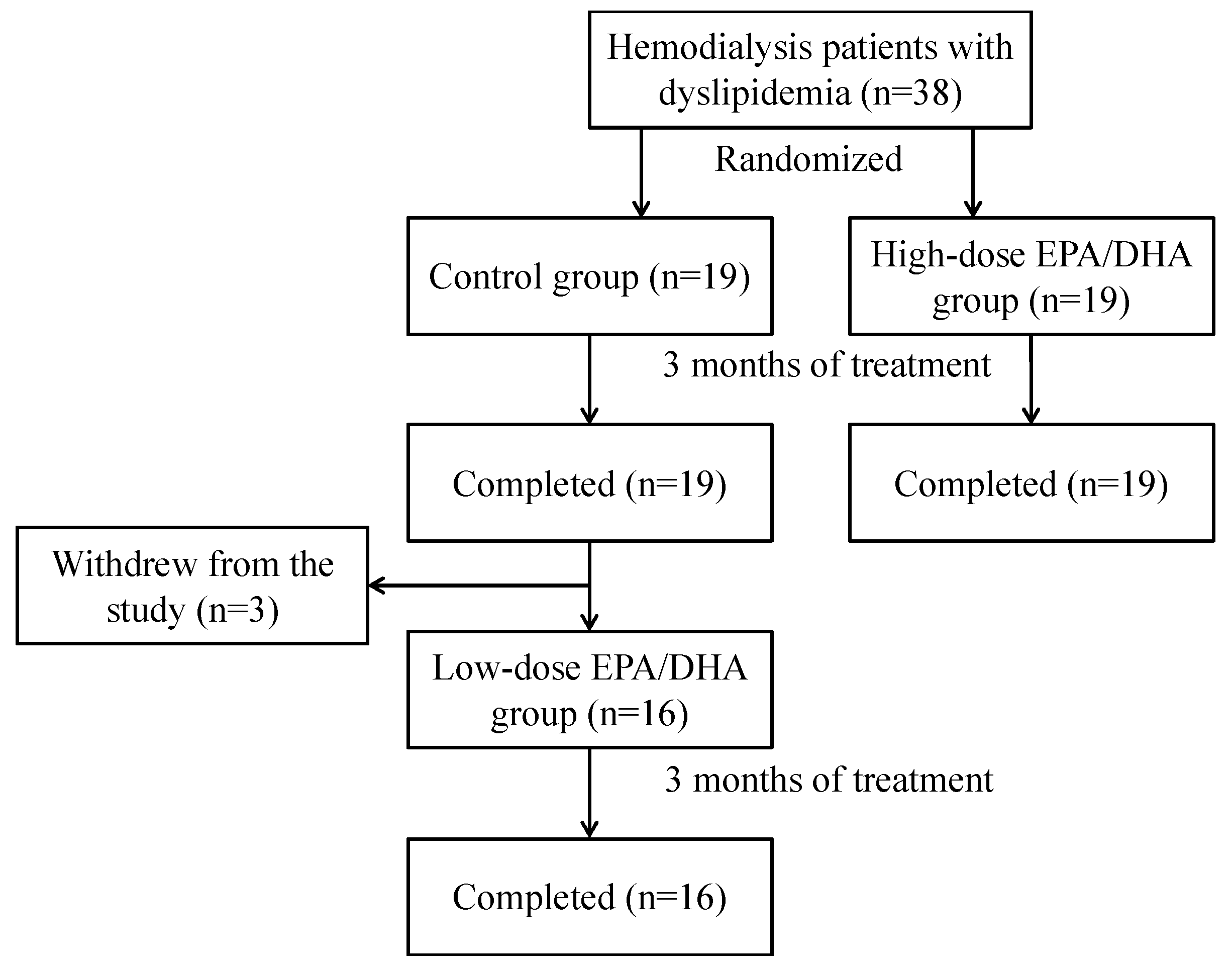
2.1. Study Design
2.2. Participants
2.3. Sample Size Calculation
2.4. Demographic and Clinical Assessments
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitation
6. Future Research Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arici, M.; Walls, J. End-stage renal disease, atherosclerosis, and cardiovascular mortality: Is C-reactive protein the missing link? Kidney Int. 2001, 59, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Foley, R.N.; Murray, A.M.; Li, S.; Herzog, C.A.; McBean, A.M.; Eggers, P.W.; Collins, A.J. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J. Am. Soc. Nephrol. 2005, 16, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Dellegrottaglie, S.; Furniss, A.L.; Gillespie, B.W.; Satayathum, S.; Lameire, N.; Saito, A.; Akiba, T.; Jadoul, M.; Ginsberg, N.; et al. Peripheral arterial disease in patients with end-stage renal disease: Observations from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Circulation 2006, 114, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, K.; Nakanishi, K.; Shimada, K.; Nakamura, H.; Inanami, H.; Nishioka, H.; Fujimoto, K.; Kasayuki, N.; Yoshiyama, M. Ankle-brachial index, arterial stiffness, and biomarkers in the prediction of mortality and outcomes in patients with end-stage kidney disease. Clin. Cardiol. 2019, 42, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, M.; Takeuchi, H.; Uchida, H.A.; Kakio, Y.; Okuyama, Y.; Umebayashi, R.; Wada, K.; Sugiyama, H.; Sugimoto, K.; Rakugi, H.; et al. Peripheral artery disease is associated with frailty in chronic hemodialysis patients. Vascular 2018, 26, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Mays, R.J.; Casserly, I.P.; Kohrt, W.M.; Ho, P.M.; Hiatt, W.R.; Nehler, M.R.; Regensteiner, J.G. Assessment of functional status and quality of life in claudication. J. Vasc. Surg. 2011, 53, 1410–1421. [Google Scholar] [CrossRef] [PubMed]
- Barnes, J.A.; Eid, M.A.; Creager, M.A.; Goodney, P.P. Epidemiology and Risk of Amputation in Patients with Diabetes Mellitus. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1808–1817. [Google Scholar] [CrossRef]
- Wu, A.; Coresh, J.; Selvin, E.; Tanaka, H.; Heiss, G.; Hirsch, A.T.; Jaar, B.G.; Matsushita, K.J. Lower Extremity Peripheral Artery Disease and Quality of Life Among Older Individuals in the Community. Am. Heart Assoc. 2017, 6, e004519. [Google Scholar] [CrossRef]
- Bello, A.K.; Okpechi, I.G.; Osman, M.A.; Cho, Y.; Htay, H.; Jha, V.; Wainstein, M.; Johnson, D.W. Epidemiology of haemodialysis outcomes. Nat. Rev. Nephrol. 2022, 18, 378–395. [Google Scholar] [CrossRef]
- Keane, W.F.; Tomassini, J.E.; Neff, D.R. Lipid abnormalities in patients with chronic kidney disease: Implications for the pathophysiology of atherosclerosis. J. Atheroscler. Thromb. 2013, 20, 123–133. [Google Scholar] [CrossRef]
- Nestel, P.J.; Fidge, N.H.; Tan, M.H. Increased lipoprotein-remnant formation in chronic renal failure. N. Engl. J. Med. 1982, 307, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, M.; Burstein, A.; Rassin, T.; Liron, M.; Ringel, Y.; Cabili, S.; Blum, M.; Peer, G.; Iaina, A. Severe defect in clearing postprandial chylomicron remnants in dialysis patients. Kidney Int. 1992, 42, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Takano, H.; Umetani, K.; Kawabata, K.; Obata, J.E.; Kitta, Y.; Kodama, Y.; Mende, A.; Ichigi, Y.; Fujioka, D.; et al. Remnant lipoproteinemia is a risk factor for endothelial vasomotor dysfunction and coronary artery disease in metabolic syndrome. Atherosclerosis 2005, 181, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Saeed, A.; Feofanova, E.V.; Yu, B.; Sun, W.; Virani, S.S.; Nambi, V.; Coresh, J.; Guild, C.S.; Boerwinkle, E.; Ballantyne, C.M.; et al. Remnant-like particle cholesterol, low-density lipoprotein triglycerides, and incident cardiovascular disease. J. Am. Coll. Cardiol. 2018, 72, 156–169. [Google Scholar] [CrossRef]
- Nakamura, T.; Obata, J.E.; Hirano, M.; Kitta, Y.; Fujioka, D.; Saito, Y.; Kawabata, K.; Watanabe, K.; Watanabe, Y.; Mishina, H.; et al. Predictive value of remnant lipoprotein for cardiovascular events in patients with coronary artery disease after achievement of LDL-cholesterol goals. Atherosclerosis 2011, 218, 163–167. [Google Scholar] [CrossRef]
- Homma, K.; Yoshizawa, J.; Shiina, Y.; Ozawa, H.; Igarashi, M.; Matsuoka, T.; Sasaki, J.; Yoshizawa, M.; Homma, Y. A dipeptidyl peptidase-4 inhibitor, teneligliptin, decreases plasma triglyceride-rich lipoprotein remnants in diabetic patients with chronic kidney disease undergoing hemodialysis. Drugs R D 2017, 17, 397–402. [Google Scholar] [CrossRef]
- Ikejiri, A.; Hirano, T.; Murayama, S.; Yoshino, G.; Gushiken, N.; Hyodo, T.; Taira, T.; Adachi, M. Effects of atorvastatin on triglyceride-rich lipoproteins, low-density lipoprotein subclass, and C-reactive protein in hemodialysis patients. Metabolism 2004, 53, 1113–1137. [Google Scholar] [CrossRef]
- Fujihara, Y.; Nakamura, T.; Horikoshi, T.; Obata, J.E.; Fujioka, D.; Watanabe, Y.; Watanabe, K.; Kugiyama, K. Remnant lipoproteins are residual risk factor for future cardiovascular events in patients with stable coronary artery disease and on-statin low-density lipoprotein cholesterol levels <70 mg/dL. Circ. J. 2019, 83, 1302–1308. [Google Scholar] [CrossRef]
- Ando, M.; Sanaka, T.; Nihei, H. Eicosapentanoic acid reduces plasma levels of remnant lipoproteins and prevents in vivo peroxidation of LDL in dialysis patients. J. Am. Soc. Nephrol. 1999, 10, 2177–2184. [Google Scholar] [CrossRef]
- Bell, S.; Cooney, J.; Packard, C.J.; Caslake, M.J.; Deighan, C.J. The effect of omega-3 fatty acids on the atherogenic lipoprotein phenotype in patients with nephrotic range proteinuria. Clin. Nephrol. 2012, 77, 445–453. [Google Scholar] [CrossRef]
- Ras, R.T.; Demonty, I.; Zebregs, Y.E.; Quadt, J.F.; Olsson, J.; Trautwein, E.A. Low doses of eicosapentaenoic acid and docosahexaenoic acid from fish oil dose-dependently decrease serum triglyceride concentrations in the presence of plant sterols in hypercholesterolemic men and women. J. Nutr. 2014, 144, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.N.; Packard, C.J.; Chapman, M.J.; Borén, J.; Aguilar-Salinas, C.A.; Averna, M.; Ference, B.A.; Gaudet, D.; Hegele, R.A.; Kersten, S.; et al. Triglyceride-rich lipoproteins and their remnants: Metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies-a consensus statement from the European Atherosclerosis Society. Eur. Heart J. 2021, 42, 4791–4806. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, T.; Sasaki, J.; Ueshima, H.; Egusa, G.; Kinoshita, M.; Shimamoto, K.; Daida, H.; Biro, S.; Hirobe, K.; Funahashi, T.; et al. Executive summary of Japan Atherosclerosis Society (JAS) guideline for diagnosis and prevention of atherosclerotic cardiovascular diseases for Japanese. J. Atheroscler. Thromb. 2007, 14, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Fujikawa, T.; Kobayashi, H.; Sumida, K.; Suzuki, S.; Kagimoto, M.; Okuyama, Y.; Ehara, Y.; Katsumata, M.; Fujita, M.; et al. Relationship between arterial stiffness and blood pressure drop during the sit-to-stand test in patients with diabetes mellitus. J. Atheroscler. Thromb. 2017, 24, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef] [PubMed]
- ASCEND Study Collaborative Group; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of n-3 fatty acid supplements in diabetes mellitus. N. Engl. J. Med. 2018, 379, 1540–1550. [Google Scholar] [CrossRef]
- Shoji, T.; Nishizawa, Y.; Kawagishi, T.; Kawasaki, K.; Taniwaki, H.; Tabata, T.; Inoue, T.; Morii, H. Intermediate-density lipoprotein as an independent risk factor for aortic atherosclerosis in hemodialysis patients. J. Am. Soc. Nephrol. 1998, 9, 1277–1284. [Google Scholar] [CrossRef]
- Nakano, T.; Hiyamuta, H.; Yotsueda, R.; Tanaka, S.; Taniguchi, M.; Tsuruya, K.; Kitazono, T. Higher cholesterol level predicts cardiovascular event and inversely associates with mortality in hemodialysis patients: 10-year outcomes of the q-cohort study. Ther. Apher. Dial. 2020, 24, 431–438. [Google Scholar] [CrossRef]
- Wang, T.; Elam, M.B.; Forbes, W.P.; Zhong, J.; Nakajima, K. Reduction of remnant lipoprotein cholesterol concentrations by cilostazol in patients with intermittent claudication. Atherosclerosis 2003, 171, 337–342. [Google Scholar] [CrossRef]
- González, A.; Schreier, L.; Elbert, A.; Berg, G.; Beresan, H.; López, G.; Wikinski, R. Lipoprotein alterations in hemodialysis: Differences between diabetic and nondiabetic patients. Metabolism 2003, 52, 116–121. [Google Scholar] [CrossRef]
- Chait, A.; Ginsberg, H.N.; Vaisar, T.; Heinecke, J.W.; Goldberg, I.J.; Bornfeldt, K.E. Remnants of the Triglyceride-Rich Lipoproteins, Diabetes, and Cardiovascular Disease. Diabetes 2020, 69, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Tam, K.W.; Wu, M.Y.; Siddiqui, F.J.; Chan, E.S.; Zhu, Y.; Jafar, T.H. Omega-3 fatty acids for dialysis vascular access outcomes in patients with chronic kidney disease. Cochrane Database Syst. Rev. 2018, 11, CD011353. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, T.; Nishibe, T.; Ohya, Y.; Inoue, S.; Ogino, H. Infrainguinal lesion of peripheral artery disease and levels of ω-3 polyunsaturated fatty acids in peripheral artery disease. Ann. Vasc. Dis. 2018, 11, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.Y.; Lin, Y.S.; Lin, D.S.; Lee, J.K.; Chen, W.J. Association of statin therapy with major adverse cardiovascular and limb outcomes in patients with end-stage kidney disease and peripheral artery disease receiving maintenance dialysis. JAMA Netw. Open 2022, 5, e2229706. [Google Scholar] [CrossRef] [PubMed]
- Bernasconi, A.A.; Wiest, M.M.; Lavie, C.J.; Milani, R.V.; Laukkanen, J.A. Effect of omega-3 dosage on cardiovascular outcomes: An updated meta-Analysis and meta-regression of interventional trials. Mayo Clin. Proc. 2021, 96, 304–313. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Wung, C.H.; Wang, Y.H.; Lee, Y.C.; Chang, C.W.; Wu, P.Y.; Huang, J.C.; Tsai, Y.C.; Chen, S.C.; Chang, J.M.; Hwang, S.J. Association between flow-mediated dilation and skin perfusion pressure with peripheral artery disease in hemodialysis patients. J. Pers. Med. 2021, 11, 1251. [Google Scholar] [CrossRef]
- Tram, L.; Bork, C.S.; Venø, S.K.; Lasota, A.N.; Lundbye-Christensen, S.; Schmidt, E.B.; Overvad, K. Intake of marine n-3 polyunsaturated fatty acids and the risk of incident peripheral artery disease. Eur. J. Clin. Nutr. 2021, 75, 1483–1490. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control Group n = 19 | High-Dose EPA/DHA Group n = 19 | p-Value | |
|---|---|---|---|
| Age, years | 73.6 ± 12.7 | 66.3 ± 11.2 | 0.068 |
| Female sex, n (%) | 7 (36.8) | 4 (21.1) | 0.476 |
| Systolic blood pressure, mmHg | 147.6 ± 16.4 | 157.4 ± 22.9 | 0.139 |
| Diastolic blood pressure, mmHg | 78.7 ± 10.5 | 80.2 ± 11.6 | 0.685 |
| LDL cholesterol level, mg/dL | 60.0 (51.0) | 73.5 (37.5) | 0.760 |
| HDL cholesterol level, mg/dL | 48.5 (18.8) | 47.0 (27.5) | 0.963 |
| Triglyceride level, mg/dL | 101.5 (43.8) | 113.5 (119.8) | 0.785 |
| RLP cholesterol level, mg/dL | 4.65 (3.27) | 5.65 (8.73) | 0.208 |
| Non-HDL cholesterol level, mg/dL | 78.5 (42.5) | 91.5 (44.0) | 0.640 |
| Apolipoprotein B level, mg/dL | 59.5 (18.5) | 67.0 (18.5) | 0.330 |
| CRP level, mg/dL | 0.10 (0.23) | 0.07 (0.14) | 0.453 |
| Ankle–brachial index | 1.09 ± 0.21 | 1.11 ± 0.14 | 0.727 |
| Duration of hemodialysis, months | 49.0 (43.8) | 57.0 (116.0) | 0.865 |
| History of diabetes, n (%) | 10 (52.6) | 11 (57.9) | 1.000 |
| History of CVD, n (%) | 6 (31.6) | 2 (10.5) | 0.741 |
| History of PAD, n (%) | 4 (21.1) | 2 (10.5) | 0.660 |
| Use of statins, n (%) | 9 (47.4) | 8 (42.1) | 1.000 |
| Use of statins before initiation of hemodialysis, n (%) | 12 (63.2) | 11 (57.9) | 1.000 |
| Use of ezetimibe, n (%) | 4 (21.1) | 3 (15.8) | 1.000 |
| Control Group n = 19 | High-Dose EPA/DHA Group n = 19 | p-Value | |
|---|---|---|---|
| LDL cholesterol level, mg/dL | −3.7 ± 12.2 | −4.3 ± 13.5 | 0.880 |
| HDL cholesterol level, mg/dL | 3.8 ± 14.6 | 2.5 ± 6.9 | 0.725 |
| Triglyceride level, mg/dL | 5.8 ± 34.6 | −41.0 ± 45.2 | <0.001 |
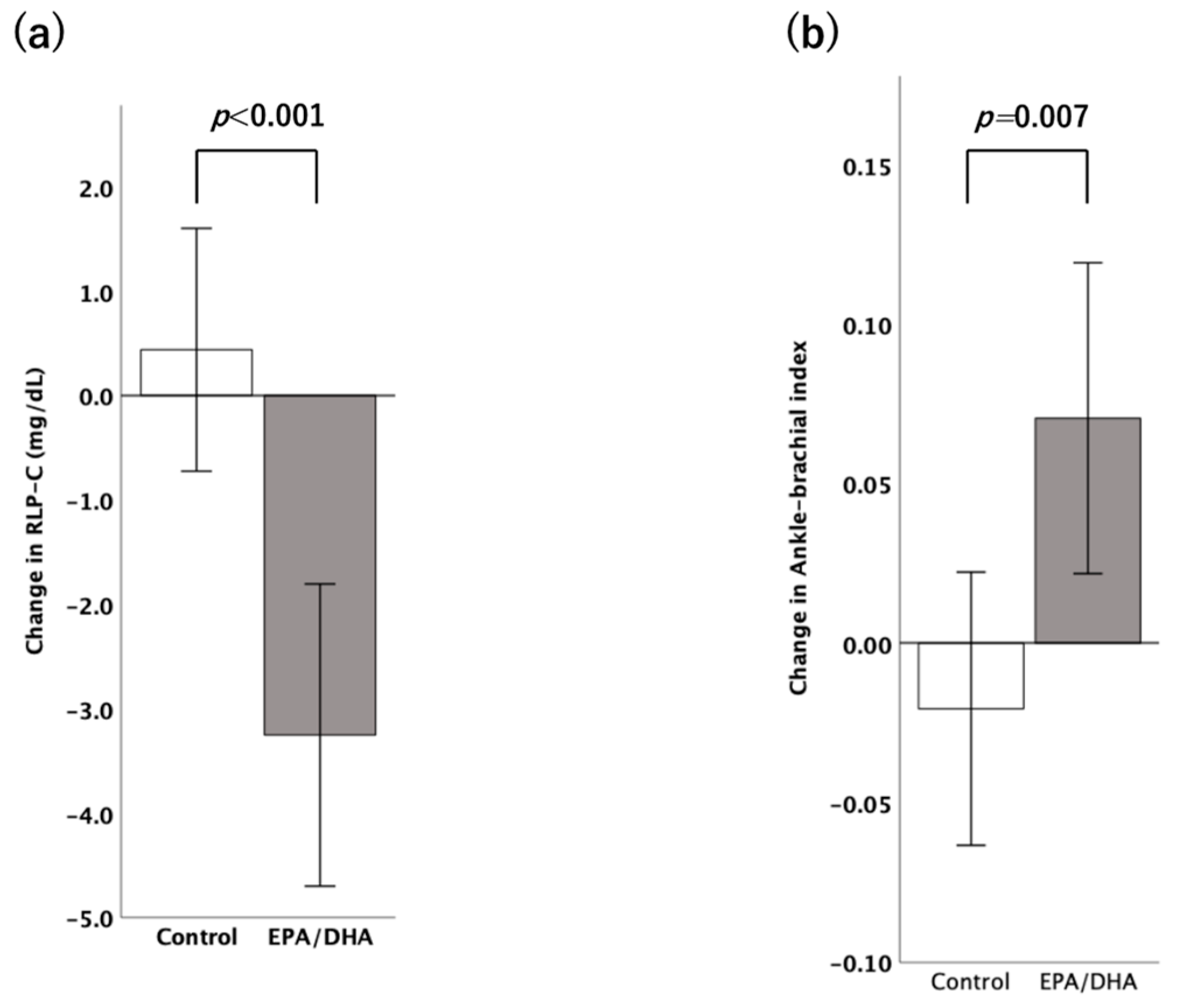
| RLP-cholesterol level, mg/dL | 0.44 ± 2.53 | −3.25 ± 3.15 | <0.001 |
| Non-HDL cholesterol level, mg/dL | −4.5 ± 20.1 | −14.8 ± 33.6 | 0.260 |
| Apolipoprotein B level, mg/dL | −1.95 ± 9.26 | −1.68 ± 9.39 | 0.931 |
| CRP level, mg/dL | 0.22 ± 0.67 | −0.02 ± 0.09 | 0.143 |
| Β | p-Value | |
|---|---|---|
| Model 1 | −0.555 | 0.001 |
| Model 2 | −0.617 | <0.001 |
| Model 3 | −0.653 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, Y.; Fujikawa, T.; Haruna, A.; Kawano, R.; Ozawa, M.; Haze, T.; Komiya, S.; Suzuki, S.; Ohki, Y.; Fujiwara, A.; et al. Omega-3 Fatty Acids Reduce Remnant-like Lipoprotein Cholesterol and Improve the Ankle–Brachial Index of Hemodialysis Patients with Dyslipidemia: A Pilot Study. Medicina 2024, 60, 75. https://doi.org/10.3390/medicina60010075
Kobayashi Y, Fujikawa T, Haruna A, Kawano R, Ozawa M, Haze T, Komiya S, Suzuki S, Ohki Y, Fujiwara A, et al. Omega-3 Fatty Acids Reduce Remnant-like Lipoprotein Cholesterol and Improve the Ankle–Brachial Index of Hemodialysis Patients with Dyslipidemia: A Pilot Study. Medicina. 2024; 60(1):75. https://doi.org/10.3390/medicina60010075
Chicago/Turabian StyleKobayashi, Yusuke, Tetsuya Fujikawa, Aiko Haruna, Rina Kawano, Moe Ozawa, Tatsuya Haze, Shiro Komiya, Shota Suzuki, Yuki Ohki, Akira Fujiwara, and et al. 2024. "Omega-3 Fatty Acids Reduce Remnant-like Lipoprotein Cholesterol and Improve the Ankle–Brachial Index of Hemodialysis Patients with Dyslipidemia: A Pilot Study" Medicina 60, no. 1: 75. https://doi.org/10.3390/medicina60010075