
Considering the Effects and Maternofoetal Implications of Vascular Disorders and the Umbilical Cord
 , , , , ,
, , , , ,  , , and
, , and
Abstract
:1. Introduction
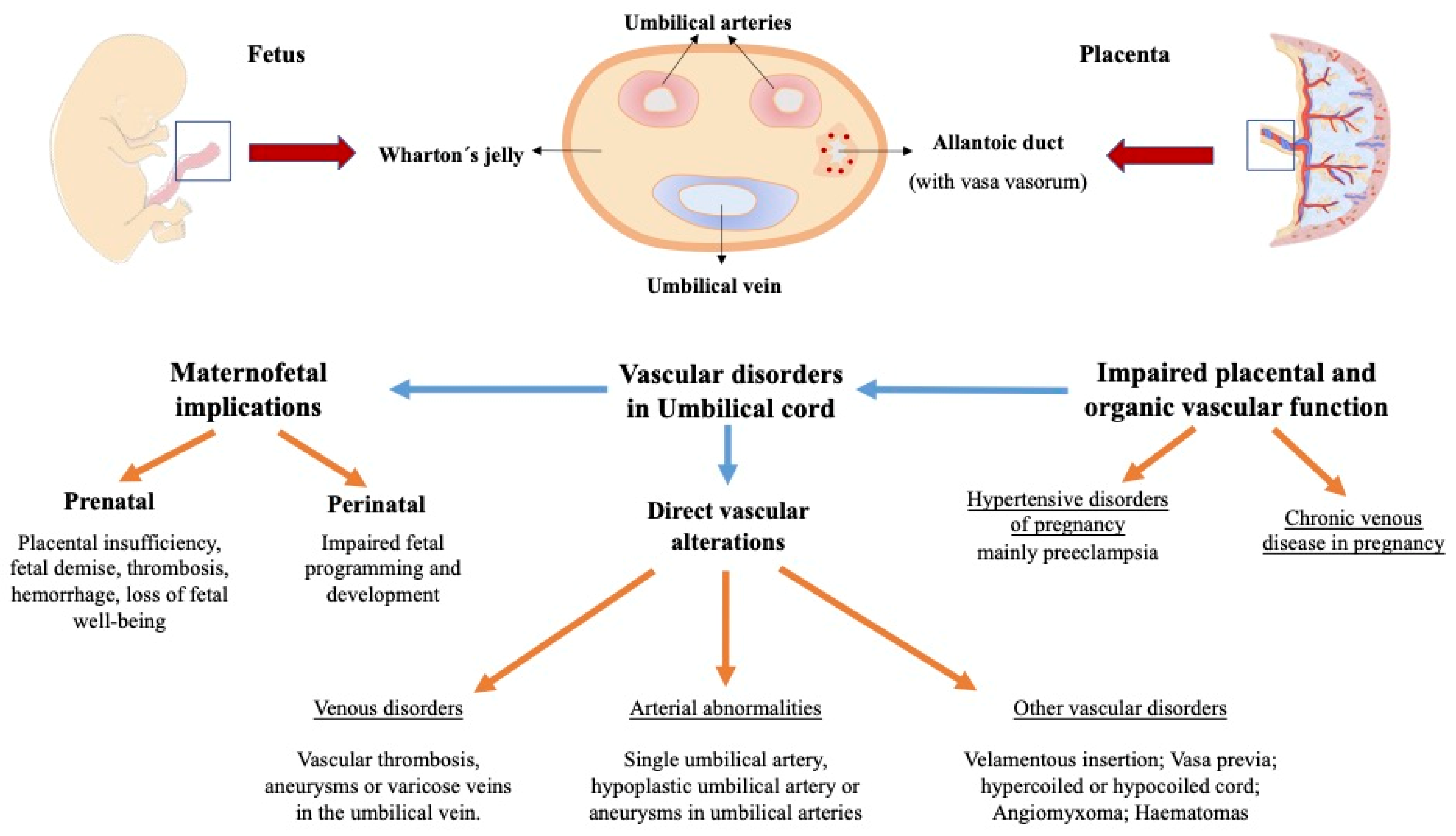
2. Vascular Alterations of the Umbilical Cord and Its Impact on the Foetus and Newborn
2.1. Arterial Vascular Alterations of the Umbilical Cord
2.2. Venous Vascular Disorders of the Umbilical Cord and Their Impact on the Foetus and Newborn
2.3. Other Vascular Disorders
2.4. Foetal Programming: How Vascular Alterations in the Umbilical Cord Can Impact on the Foetus and Newborn
3. Umbilical Cord Alterations Related to Non-Hypertensive Maternal Diseases
4. Hypertensive Disorders and Chronic Venous Disease during Pregnancy: Placental and Umbilical Cord Alterations
4.1. Hypertensive Disorders during Pregnancy
4.2. Chronic Venous Disease during Pregnancy: Placental and Umbilical Cord Alterations and Their Impact on the Foetus and the Newborn
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benirschke, K.; Kaufmann, P.; Baergen, R. Pathology of the Human Placenta, 6th ed.; Springer: New York, NY, USA, 2012. [Google Scholar]
- Hammad, I.A.; Blue, N.R.; Allshouse, A.A.; Silver, R.M.; Gibbins, K.J.; Page, J.M.; Goldenberg, R.L.; Reddy, U.M.; Saade, G.R.; Dudley, D.J.; et al. Umbilical Cord Abnormalities and Stillbirth. Obs. Gynecol. 2020, 135, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Bohîlțea, R.E.; Dima, V.; Ducu, I.; Iordache, A.M.; Mihai, B.M.; Munteanu, O.; Grigoriu, C.; Veduță, A.; Pelinescu-Onciul, D.; Vlădăreanu, R. Clinically Relevant Prenatal Ultrasound Diagnosis of Umbilical Cord Pathology. Diagnostics 2022, 12, 236. [Google Scholar] [CrossRef] [PubMed]
- AIUM-ACR-ACOG-SMFM-SRU Practice Parameter for the Performance of Standard Diagnostic Obstetric Ultrasound Examinations. J. Ultrasound Med. 2018, 37, E13–E24. [CrossRef] [PubMed] [Green Version]
- Salomon, L.J.; Alfirevic, Z.; Berghella, V.; Bilardo, C.M.; Chalouhi, G.E.; Da Silva Costa, F.; Hernandez-Andrade, E.; Malinger, G.; Munoz, H.; Paladini, D.; et al. ISUOG Practice Guidelines (updated): Performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obs. Gynecol. 2022, 59, 840–856. [Google Scholar] [CrossRef] [PubMed]
- Krzyżanowski, A.; Kwiatek, M.; Gęca, T.; Stupak, A.; Kwaśniewska, A. Modern Ultrasonography of the Umbilical Cord: Prenatal Diagnosis of Umbilical Cord Abnormalities and Assessement of Fetal Wellbeing. Med. Sci. Monit. 2019, 25, 3170. [Google Scholar] [CrossRef]
- James, J.L.; Boss, A.L.; Sun, C.; Allerkamp, H.H.; Clark, A.R. From stem cells to spiral arteries: A journey through early placental development. Placenta 2022, 125, 68–77. [Google Scholar] [CrossRef]
- Stanek, J. Umbilical cord compromise versus other clinical conditions predisposing to placental fetal vascular malperfusion. Placenta 2022, 127, 8–11. [Google Scholar] [CrossRef]
- Li, T.; Wang, G.; Xie, F.; Yao, J.; Yang, L.; Wang, M.; Wang, J.; Xing, L.; Nie, F. Prenatal diagnosis of single umbilical artery and postpartum outcome. Eur. J. Obs. Gynecol. Reprod. Biol. 2020, 254, 6–10. [Google Scholar] [CrossRef]
- Dagklis, T.; Siargkas, A.; Apostolopoulou, A.; Tsakiridis, I.; Mamopoulos, A.; Athanasiadis, A.; Sotiriadis, A. Adverse perinatal outcomes following the prenatal diagnosis of isolated single umbilical artery in singleton pregnancies: A systematic review and meta-analysis. J. Perinat. Med. 2021, 50, 244–252. [Google Scholar] [CrossRef]
- Prucka, S.; Clemens, M.; Craven, C.; McPherson, E. Single umbilical artery: What does it mean for the fetus? A case-control analysis of pathologically ascertained cases. Genet. Med. 2004, 6, 54–57. [Google Scholar] [CrossRef]
- Petrikovsky, B.; Schneider, E. Prenatal diagnosis and clinical significance of hypoplastic umibilical artery. Prenat. Diagn. 1996, 16, 938–940. [Google Scholar] [CrossRef]
- Vyas, N.M.; Manjeera, L.; Rai, S.; Devdas, S. Prenatal Diagnosis of Umbilical Artery Aneurysm with Good Fetal Outcome and Review of Literature. J. Clin. Diagn. Res. 2016, 10, QD01. [Google Scholar] [CrossRef]
- Zhu, Y.; Beejadhursing, R.; Liu, Y. 10 cases of umbilical cord thrombosis in the third trimester. Arch. Gynecol. Obs. 2021, 304, 59–64. [Google Scholar] [CrossRef]
- Wei, J.; Li, Q.; Zhai, H. Umbilical artery thrombosis diagnosed at different gestational ages and fetal outcomes: A case series. BMC Pregnancy Childbirth 2021, 21, 788. [Google Scholar] [CrossRef]
- Sepulveda, W.; Sebire, N.J.; Harris, R.M.; Nyberg, D.A. The Placenta, Umbilical Cord and Membranes. In Diagnostic Imaging of Fetal Anomalies, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2003; pp. 114–115. [Google Scholar]
- Lallar, M.; Phadke, S.R. Fetal intra abdominal umbilical vein varix: Case series and review of literature. Indian J. Radiol. Imaging 2017, 27, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Navarro-González, T.; Bravo-Arribas, C.; Pérez-Fernández-Pacheco, R.; Gámez-Alderete, F.; de León-Luis, J. Resultados perinatales luego del diagnóstico ecográfico prenatal de variz de la vena umbilical intraabdominal. Ginecol. Obs. Mex. 2013, 81, 504–509. [Google Scholar]
- Fung, T.Y.; Leung, T.N.; Leung, T.Y.; Lau, T.K. Fetal intra-abdominal umbilical vein varix: What is the clinical significance? Ultrasound Obstet. Gynecol. 2005, 25, 149–154. [Google Scholar] [CrossRef]
- Buchanan-Hughes, A.; Bobrowska, A.; Visintin, C.; Attilakos, G.; Marshall, J. Velamentous cord insertion: Results from a rapid review of incidence, risk factors, adverse outcomes and screening. Syst. Rev. 2020, 9, 147. [Google Scholar] [CrossRef]
- Turnpenny, P.D.; Stahl, S.; Bowers, D.; Bingham, P. Peripheral ischaemia and gangrene presenting at birth. Eur. J. Pediatr. 1992, 151, 550–554. [Google Scholar] [CrossRef]
- Thuring, A.; Maršál, K.; Laurini, R. Placental ischemia and changes in umbilical and uteroplacental arterial and venous hemodynamics. J. Matern. Fetal Neonatal Med. 2012, 25, 750–755. [Google Scholar] [CrossRef] [Green Version]
- McDermott, M.; Gillan, J.E. Chronic reduction in fetal blood flow is associated with placental infarction. Placenta 1995, 16, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Laurini, R.; Laurin, J.; Marsål, K. Placental histology and fetal blood flow in intrauterine growth retardation. Acta Obs. Gynecol. Scand. 1994, 73, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Beken, S.; Sarıyılmaz, K.; Albayrak, E.; Akçay, A.; Korkmaz, A. Extremity Necrosis Due to Intrauterine Arterial Ischemia. Turk. J. Haematol. Off. J. Turk. Soc. Haematol. 2021, 38, 222–223. [Google Scholar] [CrossRef]
- Vahanian, S.A.; Lavery, J.A.; Ananth, C.V.; Vintzileos, A. Placental implantation abnormalities and risk of preterm delivery: A systematic review and metaanalysis. Am. J. Obs. Gynecol. 2015, 213, S78–S90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Laat, M.W.M.; Franx, A.; Bots, M.L.; Visser, G.H.A.; Nikkels, P.G.J. Umbilical coiling index in normal and complicated pregnancies. Obs. Gynecol. 2006, 107, 1049–1055. [Google Scholar] [CrossRef]
- Pergialiotis, V.; Kotrogianni, P.; Koutaki, D.; Christopoulos-Timogiannakis, E.; Papantoniou, N.; Daskalakis, G. Umbilical cord coiling index for the prediction of adverse pregnancy outcomes: A meta-analysis and sequential analysis. J. Matern. Fetal Neonatal Med. 2019, 33, 4022–4029. [Google Scholar] [CrossRef]
- Ernst, L.M.; Minturn, L.; Huang, M.H.; Curry, E.; Su, E.J. Gross patterns of umbilical cord coiling: Correlations with placental histology and stillbirth. Placenta 2013, 34, 583–588. [Google Scholar] [CrossRef]
- Brunelli, R.; de Spirito, M.; Giancotti, A.; Palmieri, V.; Parasassi, T.; di Mascio, D.; Flammini, G.; D’Ambrosio, V.; Monti, M.; Boccaccio, A.; et al. The biomechanics of the umbilical cord Wharton Jelly: Roles in hemodynamic proficiency and resistance to compression. J. Mech. Behav. Biomed. Mater. 2019, 100, 103377. [Google Scholar] [CrossRef]
- Proctor, L.K.; Fitzgerald, B.; Whittle, W.L.; Mokhtari, N.; Lee, E.; MacHin, G.; Kingdom, J.C.P.; Keating, S.J. Umbilical cord diameter percentile curves and their correlation to birth weight and placental pathology. Placenta 2013, 34, 62–66. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Aoki, S.; Oba, M.S.; Seki, K.; Hirahara, F. Relationship Between Short Umbilical Cord Length and Adverse Pregnancy Outcomes. Fetal Pediatr. Pathol. 2016, 35, 81–87. [Google Scholar] [CrossRef]
- Debebe, S.K.; Cahill, L.S.; Kingdom, J.C.; Whitehead, C.L.; Chandran, A.R.; Parks, W.T.; Serghides, L.; Baschat, A.; Macgowan, C.K.; Sled, J.G. Wharton’s jelly area and its association with placental morphometry and pathology. Placenta 2020, 94, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Aoki, S.; Oba, M.S.; Seki, K.; Hirahara, F. Short umbilical cord length: Reflective of adverse pregnancy outcomes. Clin. Exp. Obs. Gynecol. 2017, 44, 216–219. [Google Scholar] [CrossRef]
- Suzuki, S. Excessively long umbilical cord: A preventive factor of miserable outcomes of pregnancies with true umbilical cord knots. J. Matern. Fetal Neonatal Med. 2020, 33, 3757–3760. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Heerema-McKenney, A.; Kollikonda, S.; Karnati, S. Changing Course of an Umbilical Cord Mass—Chasing the Diagnosis of Angiomyxoma. Pediatr. Dev. Pathol. 2022, 25, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Göksever, H.; Celiloğlu, M.; Küpelioğlu, A. Angiomyxoma: A rare tumor of the umbilical cord. J. Turk. Ger. Gynecol. Assoc. 2010, 11, 58. [Google Scholar] [PubMed]
- Vougiouklakis, T.; Mitselou, A.; Zikopoulos, K.; Dallas, P.; Charalabopoulos, K. Ruptured hemangioma of the umbilical cord and intrauterine fetal death, with review data. Pathol. Res. Pract. 2006, 202, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Khatiwada, P.; Alsabri, M.; Wiredu, S.; Kusum, V.; Kiran, V. Spontaneous Umbilical Cord Hematoma. Cureus 2021, 13, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Gualandri, G.; Rivasi, F.; Santunione, A.L.; Silingardi, E. Spontaneous umbilical cord hematoma: An unusual cause of fetal mortality: A report of 3 cases and review of the literature. Am. J. Forensic Med. Pathol. 2008, 29, 185–190. [Google Scholar] [CrossRef]
- Clermont-Hama, Y.; Thibouw, K.; Devisme, L.; Franquet-Ansart, H.; Stichelbout, M.; Subtil, D. Risk factors for spontaneous hematoma of the umbilical cord: A case-control study. Placenta 2020, 99, 152–156. [Google Scholar] [CrossRef]
- Wright, R.G.; Macindoe, C.; Green, P. Placental Abnormalities Associated with Childbirth. Acad. Forensic Pathol. 2019, 9, 2–14. [Google Scholar] [CrossRef]
- Herzog, E.M.; Eggink, A.J.; Reijnierse, A.; Kerkhof, M.A.M.; de Krijger, R.R.; Roks, A.J.M.; Reiss, I.K.M.; Nigg, A.L.; Eilers, P.H.C.; Steegers, E.A.P.; et al. Impact of early-and late-onset preeclampsia on features of placental and newborn vascular health. Placenta 2017, 49, 72–79. [Google Scholar] [CrossRef]
- Koech, A.; Ndungu, B.; Gichangi, P. Structural Changes in Umbilical Vessels in Pregnancy Induced Hypertension. Placenta 2008, 29, 210–214. [Google Scholar] [CrossRef]
- Green, B.B.; Marsit, C.J. Select Prenatal Environmental Exposures and Subsequent Alterations of Gene-Specific and Repetitive Element DNA Methylation in Fetal Tissues. Curr. Environ. Health Rep. 2015, 2, 126–136. [Google Scholar] [CrossRef] [Green Version]
- Fajersztajn, L.; Veras, M.M. Hypoxia: From Placental Development to Fetal Programming. Birth Defects Res. 2017, 109, 1377–1385. [Google Scholar] [CrossRef]
- Konkel, L. Lasting Impact of an Ephemeral Organ: The Role of the Placenta in Fetal Programming. Environ. Health Perspect. 2016, 124, A124. [Google Scholar] [CrossRef] [Green Version]
- Gilstrap, L.C.; Leveno, K.J.; Burris, J.; Williams, M.L.; Little, B.B. Diagnosis of birth asphyxia on the basis of fetal pH, Apgar score, and newborn cerebral dysfunction. Am. J. Obs. Gynecol. 1989, 161, 825–830. [Google Scholar] [CrossRef]
- Malin, G.L.; Morris, R.K.; Khan, K.S. Strength of association between umbilical cord pH and perinatal and long term outcomes: Systematic review and meta-analysis. BMJ 2010, 340, 1121. [Google Scholar] [CrossRef] [Green Version]
- Andres, R.L.; Saade, G.; Gilstrap, L.C.; Wilkins, I.; Witlin, A.; Zlatnik, F.; Hankins, G.V. Association between umbilical blood gas parameters and neonatal morbidity and death in neonates with pathologic fetal acidemia. Am. J. Obs. Gynecol. 1999, 181, 867–871. [Google Scholar] [CrossRef]
- Knutzen, L.; Svirko, E.; Impey, L. The significance of base deficit in acidemic term neonates. Am. J. Obs. Gynecol. 2015, 213, e1–e373. [Google Scholar] [CrossRef]
- Dain, C.; Roze J christophe Olivier, M.; Bossard, M.; Praud, M.; Flamant, C. Neurodevelopmental outcome at 24 months of healthy infants at birth with an umbilical artery blood pH ≤ 7 and/or hyperlactacidemia ≥ 7 mmol/L. Birth 2021, 48, 178–185. [Google Scholar] [CrossRef]
- Tuuli, M.G.; Stout, M.J.; Shanks, A.; Odibo, A.O.; Macones, G.A.; Cahill, A.G. Umbilical cord arterial lactate compared with pH for predicting neonatal morbidity at term. Obs. Gynecol. 2014, 124, 756–761. [Google Scholar] [CrossRef] [PubMed]
- White, C.R.H.; Doherty, D.A.; Henderson, J.J.; Kohan, R.; Newnham, J.P.; Pennell, C.E. Accurate prediction of hypoxic-ischaemic encephalopathy at delivery: A cohort study. J. Matern. Fetal Neonatal Med. 2012, 25, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Watterberg, K.L.; Aucott, S.; Benitz, W.E.; Cummings, J.J.; Eichenwald, E.C.; Goldsmith, J.; Poindexter, B.B.; Puopolo, K.; Stewart, D.L.; Wang, K.S.; et al. The Apgar Score. Pediatrics 2015, 136, 819–822. [Google Scholar] [CrossRef] [Green Version]
- Ahmadpour-Kacho, M.; Asnafi, N.; Javadian, M.; Hajiahmadi, M.; Taleghani, N.H. Correlation between Umbilical Cord pH and Apgar Score in High-Risk Pregnancy. Iran. J. Pediatr. 2010, 20, 401. [Google Scholar] [PubMed]
- Cnattingius, S.; Norman, M.; Granath, F.; Petersson, G.; Stephansson, O.; Frisell, T. Apgar Score Components at 5 Minutes: Risks and Prediction of Neonatal Mortality. Paediatr. Perinat. Epidemiol. 2017, 31, 328–337. [Google Scholar] [CrossRef]
- Mu, Y.; Li, M.; Zhu, J.; Wang, Y.; Xing, A.; Liu, Z.; Xie, Y.; Wang, X.; Liang, J. Apgar score and neonatal mortality in China: An observational study from a national surveillance system. BMC Pregnancy Childbirth 2021, 21, 47. [Google Scholar] [CrossRef]
- Yılmaz, A.; Kaya, N.; Ülkersoy, İ.; Taner, H.E.; Acar, H.C.; Kaymak, D.; Perk, Y.; Vural, M. The Correlation of Cord Arterial Blood Gas Analysis Results and Apgar Scores in Term Infants Without Fetal Distress. Turk. Arch. Pediatr. 2022, 57, 538–543. [Google Scholar] [CrossRef]
- Mlodawska, M.; Mlodawski, J.; Gladys-Jakubczyk, A.; Pazera, G. Relationship between Apgar score and umbilical cord blood acid-base balance in full-term and late preterm newborns born in medium and severe conditions. Ginekol. Pol. 2021, 93, 57–62. [Google Scholar] [CrossRef]
- Omo-Aghoja, L. Maternal and fetal Acid-base chemistry: A major determinant of perinatal outcome. Ann. Med. Health Sci. Res. 2014, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Kostro, M.; Jacyna, N.; Głuszczak-Idziakowska, E.; Sułek-Kamas, K.; Jakiel, G.; Wilińska, M. Factors affecting the differentiation of the apgar score and the biochemical correlation of fetal well-being—A prospective observational clinical study. J. Mother Child 2021, 22, 238–246. [Google Scholar] [CrossRef]
- Monari, F.; Menichini, D.; Salerno, C.; Donno, V.; Po’, G.; Melis, B.; Facchinetti, F. Impact of endocrine disorders on stillbirth: A prospective cohort study. Gynecol. Endocrinol. 2022, 38, 483–487. [Google Scholar] [CrossRef]
- Campbell, I.W.; Duncan, C.; Urquhart, R.; Evans, M. Placental dysfunction and stillbirth in gestational diabetes mellitus. Br. J. Diabetes Vasc. Dis. 2009, 9, 38–40. [Google Scholar] [CrossRef]
- Leach, L.; Taylor, A.; Sciota, F. Vascular dysfunction in the diabetic placenta: Causes and consequences. J. Anat. 2009, 215, 69. [Google Scholar] [CrossRef]
- Pietryga, M.; Bra̧zert, J.; Wender-Ozegowska, E.; Dubiel, M.; Gudmundsson, S. Placental Doppler velocimetry in gestational diabetes mellitus. J. Perinat. Med. 2006, 34, 108–110. [Google Scholar] [CrossRef]
- Najafi, L.; Honardoost, M.; Khajavi, A.; Cheraghi, S.; Kadivar, M.; Khamseh, M.E. The association of umbilical coiling and angiogenesis markers: Impact assessment of gestational diabetes. Placenta 2022, 129, 70–76. [Google Scholar] [CrossRef]
- Tenaw Goshu, B. Histopathologic Impacts of Diabetes Mellitus on Umbilical Cord During Pregnancy. Pediatr. Health Med. 2022, 13, 37–41. [Google Scholar] [CrossRef]
- Najafi, L.; Khamseh, M.E.; Kashanian, M.; Younesi, L.; Abedini, A.; Valojerdi, A.E.; Amoei, Z.; Heiran, E.N.K.; Keshtkar, A.A.; Malek, M. Antenatal umbilical coiling index in gestational diabetes mellitus and non-gestational diabetes pregnancy. Taiwan J. Obs. Gynecol. 2018, 57, 487–492. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Parks, W.T.; Perkins, K.; Pugh, S.J.; Platt, R.W.; Feghali, M.; Florio, K.; Young, O.; Bernstein, S.; Simhan, H.N. Maternal prepregnancy obesity and cause-specific stillbirth. Am. J. Clin. Nutr. 2015, 102, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Åmark, H.; Westgren, M.; Sirotkina, M.; Varli, I.H.; Persson, M.; Papadogiannakis, N. Maternal obesity and stillbirth at term; placental pathology—A case control study. PLoS ONE 2021, 16, e0250983. [Google Scholar] [CrossRef]
- Cardona-Benavides, I.; Mora-González, P.; Pineda, A.; Puertas, A.; Manzanares Galán, S. Maternal obesity and the risk of fetal acidosis at birth. J. Matern. Fetal Neonatal Med. 2022, 35, 765–769. [Google Scholar] [CrossRef]
- Olaya, C.M.; Salcedo-Betancourt, J.; Galvis, S.H.; Ortiz, A.M.; Gutierrezb, S.; Bernal, J.E. Umbilical cord and preeclampsia. J. Neonatal Perinat. Med. 2016, 9, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Naftali, S.; Ashkenazi, Y.N.; Ratnovsky, A. A novel approach based on machine learning analysis of flow velocity waveforms to identify unseen abnormalities of the umbilical cord. Placenta 2022, 127, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Shahid, N.; Masood, M.; Bano, Z.; Naz, U.; Hussain, S.F.; Anwar, A.; Hashmi, A.A. Role of Uterine Artery Doppler Ultrasound in Predicting Pre-Eclampsia in High-Risk Women. Cureus 2021, 13, e16276. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Gómez-Lahoz, A.M.; Sánchez-Trujillo, L.; Fraile-Martinez, O.; García-Montero, C.; Guijarro, L.G.; Bravo, C.; De Leon-Luis, J.A.; Saz, J.V.; Bujan, J.; et al. Chronic Venous Disease during Pregnancy Causes a Systematic Increase in Maternal and Fetal Proinflammatory Markers. Int. J. Mol. Sci. 2022, 23, 8976. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.; Hicks, C.W.; Heller, J.A. The hemodynamic effects of pregnancy on the lower extremity venous system. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 246–255. [Google Scholar] [CrossRef]
- Troiano, N.H. Physiologic and hemodynamic changes during pregnancy. AACN Adv. Crit. Care 2018, 29, 273–283. [Google Scholar] [CrossRef]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Álvarez-Mon, M.A.; Chaowen, C.; Ruiz-Grande, F.; Pekarek, L.; Monserrat, J.; Asúnsolo, A.; García-Honduvilla, N.; et al. Understanding Chronic Venous Disease: A Critical Overview of Its Pathophysiology and Medical Management. J. Clin. Med. 2021, 10, 3239. [Google Scholar] [CrossRef]
- Ortega, M.A.; Saez, M.A.; Fraile-Martínez, O.; Asúnsolo, Á.; Pekarek, L.; Bravo, C.; Coca, S.; Sainz, F.; Mon, M.Á.-; Buján, J.; et al. Increased angiogenesis and lymphangiogenesis in the placental villi of women with chronic venous disease during pregnancy. Int. J. Mol. Sci. 2020, 21, 2487. [Google Scholar] [CrossRef] [Green Version]
- Ortega, M.A.; Saez, M.Á.; Asúnsolo, Á.; Romero, B.; Bravo, C.; Coca, S.; Sainz, F.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Upregulation of VEGF and PEDF in Placentas of Women with Lower Extremity Venous Insufficiency during Pregnancy and Its Implication in Villous Calcification. BioMed Res. Int. 2019, 2019, 5320902. [Google Scholar] [CrossRef]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Sáez, M.A.; Álvarez-Mon, M.A.; Torres-Carranza, D.; Álvarez-Mon, M.; Bujan, J.; García-Honduvilla, N.; Bravo, C.; et al. The Pivotal Role of the Placenta in Normal and Pathological Pregnancies: A Focus on Preeclampsia, Fetal Growth Restriction, and Maternal Chronic Venous Disease. Cells 2022, 11, 568. [Google Scholar] [CrossRef]
- Schoots, M.H.; Gordijn, S.J.; Scherjon, S.A.; van Goor, H.; Hillebrands, J.L. Oxidative stress in placental pathology. Placenta 2018, 69, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Bedard, K.; Krause, K.H. The NOX family of ROS-generating NADPH oxidases: Physiology and pathophysiology. Physiol. Rev. 2007, 87, 245–313. [Google Scholar] [CrossRef] [PubMed]
- Perrone, S.; Laschi, E.; Buonocore, G. Biomarkers of oxidative stress in the fetus and in the newborn. Free Radic. Biol. Med. 2019, 142, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Romero, B.; Asúnsolo, Á.; Martínez-Vivero, C.; Sainz, F.; Bravo, C.; de León-Luis, J.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Pregnancy-associated venous insufficiency course with placental and systemic oxidative stress. J. Cell. Mol. Med. 2020, 24, 4157–4170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrone, S.; Laschi, E.; Buonocore, G. Oxidative stress biomarkers in the perinatal period: Diagnostic and prognostic value. Semin. Fetal Neonatal Med. 2020, 25, 101087. [Google Scholar] [CrossRef] [PubMed]
- Draganovic, D.; Lucic, N.; Jojic, D.; Milicevic, S. Correlation of oxidative stress markers with ultrasound and cardiotocography parameters with hypertension induced pregnancy. Acta Inf. Med. 2017, 25, 19–23. [Google Scholar] [CrossRef] [Green Version]
- Ortega, M.A.; Chaowen, C.; Fraile-Martinez, O.; García-Montero, C.; Saez, M.A.; Cruza, I.; Pereda-Cerquella, C.; Alvarez-Mon, M.A.; Guijarro, L.G.; Fatych, Y.; et al. Chronic Venous Disease in Pregnant Women Causes an Increase in ILK in the Placental Villi Associated with a Decrease in E-Cadherin. J. Pers. Med. 2022, 12, 277. [Google Scholar] [CrossRef]
- Incebiyik, A.; Kocarslan, S.; Camuzcuoglu, A.; Hilali, N.G.; Incebiyik, H.; Camuzcuoglu, H. Trophoblastic E-cadherin and TGF-beta expression in placenta percreta and normal pregnancies. J. Matern. Fetal Neonatal Med. 2016, 29, 126–129. [Google Scholar] [CrossRef]
- Duzyj, C.M.; Buhimschi, I.A.; Motawea, H.; Laky, C.A.; Cozzini, G.; Zhao, G.; Funai, E.F.; Buhimschi, C.S. The invasive phenotype of placenta accreta extravillous trophoblasts associates with loss of E-cadherin. Placenta 2015, 36, 645–651. [Google Scholar] [CrossRef]
- Li, H.W.; Cheung, A.N.Y.; Tsao, S.W.; Cheung, A.L.M.; Wai-Sum, O. Expression of e-cadherin and beta-catenin in trophoblastic tissue in normal and pathological pregnancies. Int. J. Gynecol. Pathol. 2003, 22, 63–70. [Google Scholar] [CrossRef]
- Raghupathy, R.; Kalinka, J. Cytokine imbalance in pregnancy complications and its modulation. Front. Biosci. 2008, 13, 985–994. [Google Scholar] [CrossRef]
- Velez, D.R.; Fortunato, S.J.; Morgan, N.; Edwards, T.L.; Lombardi, S.J.; Williams, S.M.; Menon, R. Patterns of cytokine profiles differ with pregnancy outcome and ethnicity. Hum. Reprod. 2008, 23, 1902–1909. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.; Karmaus, W.; Davis, S.; Gangur, V. Immune markers in breast milk and fetal and maternal body fluids: A systematic review of perinatal concentrations. J. Hum. Lact. 2011, 27, 171–186. [Google Scholar] [CrossRef]


{kind=link}
| Pathology | Cause and Risk Factors | Vascular Alteration | Impact | References |
|---|---|---|---|---|
| Single umbilical artery (SUA) | Primary agenesis, atresia, or secondary atrophy. Chromosomal abnormalities. | Variation of the anatomy of the cord in which only a single umbilical artery is present. Absence of the left umbilical artery is more frequent. Occurs in 0.5–5% of spontaneous pregnancies. | There is no clear relationship of this isolated variant with a certain foetal or neonatal pathology, although studies suggest that there could be increased risks of preterm delivery, caesarean section, low birth weight, small for gestational age newborn and admission to the NICU. The association of SUA with other chromosomal or anatomical abnormalities (malformation of the urinary system, cardiovascular system and digestive system) may also imply changes in foetal and neonatal development. | [9,10,11] |
| Umbilical artery aneurysm | SUA. Trisomy 18. | Turbulent pulsatile flow at the ultrasound level. Found in areas close to the placental insertion site that are less protected by Wharton’s jelly, usually during the second or third trimester of gestation. | They are associated with delayed intrauterine growth, aneuploidy and foetal demise. | [13] |
| Pregnancy-induced hypertension | Risk factors: primary hypertension, renal disease, diabetes, multiple gestations. | Decrease in the lumen of the umbilical vein, thickening of the tunica media, increase in elastic fibres and a decrease in collagen fibres. | Influences foetal blood flow and potentially the foetus | [44,74] |
| Preeclampsia | Unknown cause. | Decreased venous area and wall thickness in the umbilical cords. Other studies show an increased wall thickness, with increases in the thickness of the tunica media and wall-luminal ratio. Some studies also show relationships of preeclampsia with hypercoiling, marginal and paramarginal insertion and SUA. | Associated with FGR (foetal growth restriction) and preterm delivery. Some studies suggest relationship with hyoercoiling, marginal and paramarginal insertion and SUA. | [43,73,75] |
| Vascular thrombosis: umbilical cord thrombi. | Maternal coagulation disorders, vascular endothelial damage, elevated blood glucose. Risk factors: hypercoiling, long cord, narrowed cord. | They mainly affect the umbilical vein and are related to vellum insertion of the cord and an excess of cord coiling, with long cords and little Wharton jelly. | They are related to FGR and foetal demise. | [14,15] |
| Varicose veins or umbilical vein aneurysms | No specific causes and risk factors known. | They are more frequent than umbilical artery aneurysms. Turbulent nonpulsatile flows occur in dilation zones. They are diagnosed by visualizing dilations greater than 9 mm in diameter or with a diameter greater than 50% of the unaffected vessel. They can be intra- or extra-abdominal. | They do not usually have foetal repercussions. Some studies have found an increased risk of intra-amniotic haemorrhage, low birth weight or foetal demise. | [17,18,19] |
| Velamentous cord insertion and vasa praevia. | No specific causes and risk factors known. | Velamentous insertion of the umbilical cord consists of the divergence of umbilical vessels, unsupported by the umbilical cord or placental tissue, as they traverse amnion and chorion before reaching the placenta with little Wharton jelly and susceptibility to compression. Vasa praevia consists in an anomaly of the umbilical vessels that cross the membranes of the low uterine segment, unsupported by umbilical cord or placental tissue, with a hight risk of rupture of the vessels | The rupture of membranes can cause the rupture of vessels with risk of exsanguination and foetal demise. Flow compression can translate into placental infarcts and limb amputations. In addition, there are increased risks of low birth weight and perinatal death. | [20,21,22,23,24,25,26] |
| Hypercoiled umbilical cord | No specific causes and risk factors known. | Modifies fetoplacental flow. | Increased risk of adverse perinatal events and foetal demise, increased risk of preterm delivery, loss of foetal well-being, meconium amniotic fluid, Apgar > 7, small for gestational age, foetal and cardiac abnormalities, foetal demise and admission to the NICU. | [28,29] |
| Hypocoiled umbilical cord | No specific causes and risk factors known. | Modifies fetoplacental flow. | Increased risk of adverse perinatal events and foetal demise, chronic foetal vascular obstruction, stillbirth, increased risk of preterm delivery, loss of foetal well-being, meconium amniotic fluid, Apgar > 7, small for gestational age, foetal and cardiac abnormalities, foetal demise and admission to the NICU. | [28,29] |
| Thin umbilical cord | No specific causes and risk factors known. | Favours vascular compression with repercussions for foetal flow and uterine growth. | Small placental size, low birth weight, placental insufficiency, intrauterine growth restriction and low birth weight. | [30,31,33,34] |
| Long umbilical cord | No specific causes and risk factors known. | Greater than 70 cm. | They allow wide foetal movements with greater risk of crossed and circular entanglement and true cord knots, which increases the risk of foetal demise. | [35] |
| Short umbilical cord | No specific causes and risk factors known. | Less than 35 cm. | Higher incidence of adverse events such as urgent caesarean section or low birth weight. | [32,34] |
| Umbilical angiomyxoma or haemangioma | Mostly incidental. Risk factors: Hydrops, cord torsion, foetal demise, rupture, haematomas. | Infrequent tumour that arises from the proliferation of mesenchymal angiogenic cells in a close relationship with the umbilical vessels. Solid cystic mass, echogenic and vascularized lesions, usually located in the area of foetal insertion. | Foetal demise due to the risk of compression of vessels, their rupture and formation of haematomas that compromise the umbilical flow to the foetus. | [36,37,38] |
| Umbilical haematoma | Mostly spontaneous. Risk factors: Invasive procedures (amniocentesis), infections, oligoamnios and morphological abnormalities. | Extravasation of blood from the umbilical vein to Wharton’s jelly. | Loss of foetal well-being, intrapartum asphyxia and hypoxic-ischaemic encephalopathy in the newborn. Oligoamnios in the third trimester. Increased risks of prenatal and perinatal death. | [39,40,41] |
| Chronic venous disease | Vsodilation, compression of iliac veins and venous stasis during pregnancy, favour its development. | Increases in the gene and protein expression of NOX-1, NOX-2, iNOS, HIF-1alpha and MDA. This oxidative stress has been linked to ultrasound and cardiotocographic alterations [87,88] such as intrauterine growth retardation, foetal growth restriction, or preterm delivery. Some studies have shown that gestational CVD favours this proinflammatory state, as indicated by increases in the levels of proinflammatory cytokines (IL-6, IL-12, TNF-α, IL-10, IL-13, IL-2, IL-7, IFN-γ, IL-4, IL-5, IL-21, IL-23, GM-CSF, chemokines (fractalkine), MIP-3α and MIP-1β). This proinflammatory profile has been related to multiple pathologies, such as preeclampsia, preterm delivery, and the development of bronchial hyperresponsiveness or overweight during the first years of life and therefore forms part of the so-called “foetal programming | [46,47,76,85,87,88] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Trujillo, L.; García-Montero, C.; Fraile-Martinez, O.; Guijarro, L.G.; Bravo, C.; De Leon-Luis, J.A.; Saez, J.V.; Bujan, J.; Alvarez-Mon, M.; García-Honduvilla, N.; et al. Considering the Effects and Maternofoetal Implications of Vascular Disorders and the Umbilical Cord. Medicina 2022, 58, 1754. https://doi.org/10.3390/medicina58121754
Sánchez-Trujillo L, García-Montero C, Fraile-Martinez O, Guijarro LG, Bravo C, De Leon-Luis JA, Saez JV, Bujan J, Alvarez-Mon M, García-Honduvilla N, et al. Considering the Effects and Maternofoetal Implications of Vascular Disorders and the Umbilical Cord. Medicina. 2022; 58(12):1754. https://doi.org/10.3390/medicina58121754
Chicago/Turabian StyleSánchez-Trujillo, Lara, Cielo García-Montero, Oscar Fraile-Martinez, Luis G. Guijarro, Coral Bravo, Juan A. De Leon-Luis, Jose V. Saez, Julia Bujan, Melchor Alvarez-Mon, Natalio García-Honduvilla, and et al. 2022. "Considering the Effects and Maternofoetal Implications of Vascular Disorders and the Umbilical Cord" Medicina 58, no. 12: 1754. https://doi.org/10.3390/medicina58121754