
First Clinical Experience with a Novel 3D C-Arm-Based System for Navigated Percutaneous Thoracolumbar Pedicle Screw Placement



Abstract
:1. Introduction
2. Materials and Methods
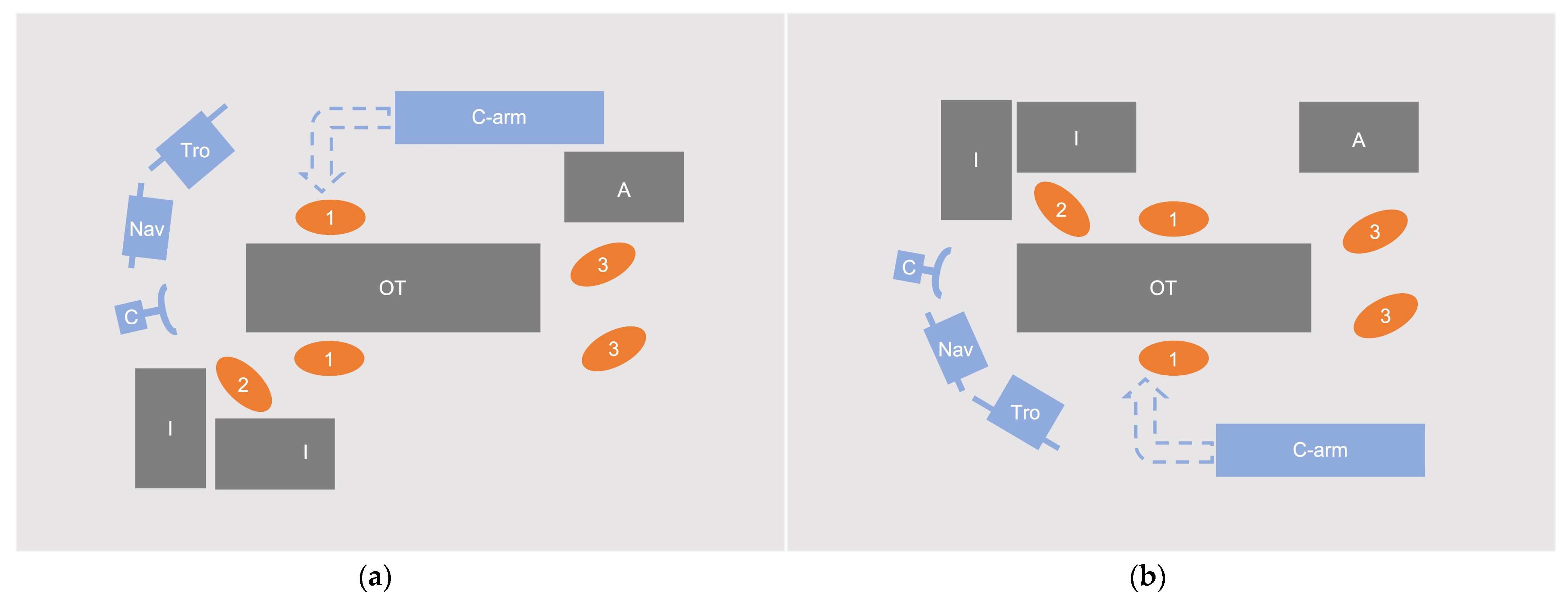
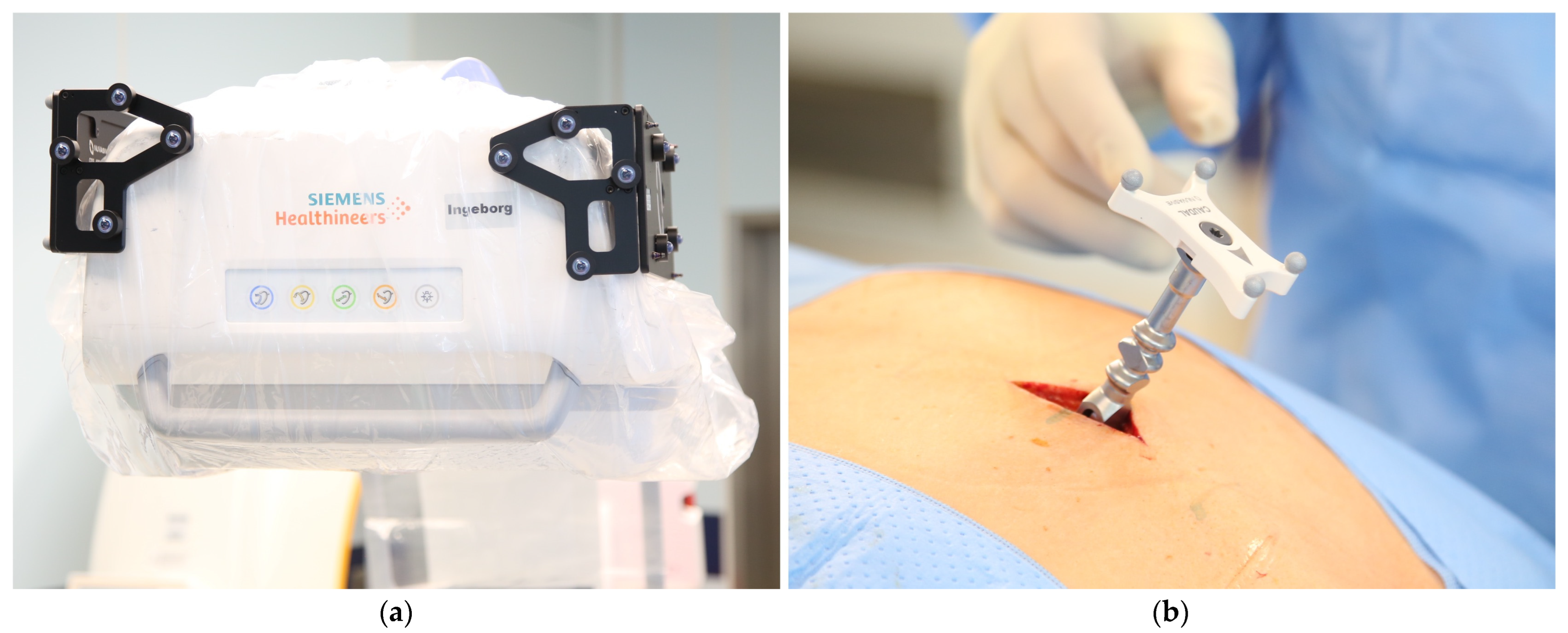
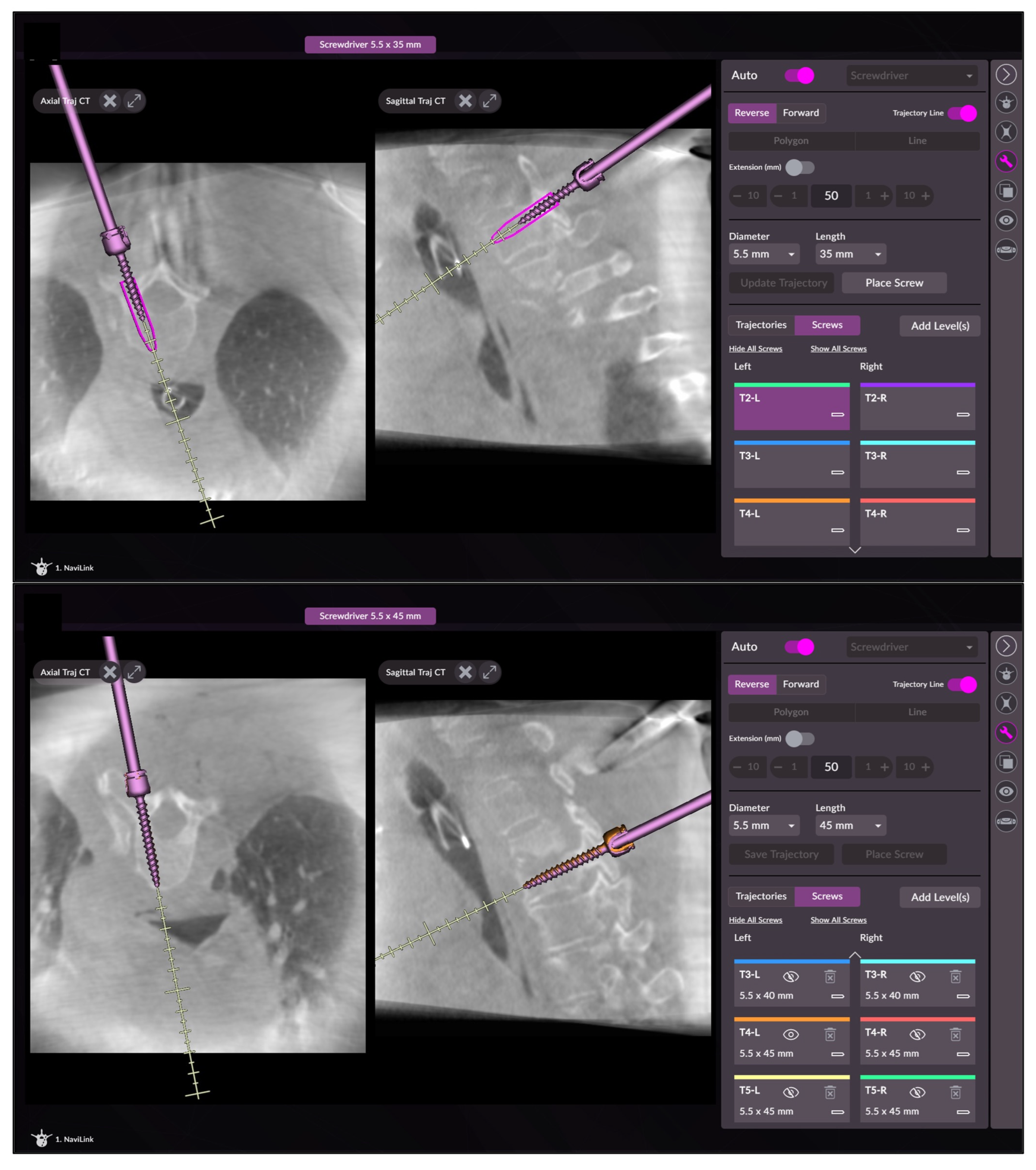
2.1. Intraoperative Workflow
2.2. Data Collection
- Patient data including diagnosis, spinal levels to be instrumented, as well as the number of segments instrumented, and screws placed.
- Procedural times during the procedures:
- Operating time (OT, from first incision to suture);
- Navigation time (NT, first insertion of the navigated pointer until after placement of the last screw);
- Screw placement time (SPT) for every single screw (insertion of the drill guide until the removal of the screwdriver after screw placement).
- Intraoperative patient radiation exposure as dose area product (DAP) and fluoroscopy time (FT) as documented in the imaging system dose report; for calculation of the effective dose (ED) in mSv, ED/DAP conversion factors of 0.29 (Body mass index, BMI < 25), 0.26 (BMI 25–30) and 0.23 (BMI > 30) were used [20].
- Intraoperative revision of guide wires or screws.
- Intraoperative complications or technical problems.
- Postoperative complications (changes in neurovascular status, infection, wound healing disorder, revision surgery)
- Pedicle screw accuracy was assessed in postoperative CT by an independent investigator with extensive experience according to Gertzbein–Robbins grading system with grades A (no pedicle breach) and B (pedicle breach < 2 mm) considered clinically acceptable and Grades C (pedicle breach < 4 mm), D (pedicle breach < 6 mm), and E (pedicle breach ≥ 6 mm) deemed unacceptable because of potential neurovascular injury [21].
2.3. Statistical Analysis
3. Results
3.1. Patient Data
3.2. Procedural Times
3.3. Patient Radiation Exposure
3.4. Intraoperative Revisions and Intra-/Postoperative Complications
3.5. Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosinski, A.A.; Mittal, A.; Odeh, K.; Ungurean, V.; Leasure, J.; Telles, C.; Kondrashov, D. Alternatives to Traditional Pedicle Screws for Posterior Fixation of the Degenerative Lumbar Spine. JBJS Rev. 2021, 9, e20. [Google Scholar] [CrossRef]
- Roy-Camille, R.; Saillant, G.; Berteaux, D.; Salgado, V. Osteosynthesis of thoraco-lumbar spine fractures with metal plates screwed through the vertebral pedicles. Reconstr. Surg. Traumatol. 1976, 15, 2–16. [Google Scholar]
- Verma, K.; Boniello, A.; Rihn, J. Emerging Techniques for Posterior Fixation of the Lumbar Spine. J. Am. Acad. Orthop. Surg. 2016, 24, 357–364. [Google Scholar] [CrossRef]
- Boucher, H.H. A method of spinal fusion. J. Bone Jt. Surgery. Br. Vol. 1959, 41, 248–259. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Sivabalan, P.; Li, J. Technique, challenges and indications for percutaneous pedicle screw fixation. J. Clin. Neurosci. 2011, 18, 741–749. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Rizzolo, S.J.; Balderston, R.A.; Allardyce, T.J.; Garfin, S.R.; Dolinskas, C.; An, H.S. Placement of pedicle screws in the thoracic spine. Part II: An anatomical and radiographic assessment. JBJS 1995, 77, 1200–1206. [Google Scholar] [CrossRef]
- Qureshi, S.; Lu, Y.; McAnany, S.; Baird, E. Three-dimensional intraoperative imaging modalities in orthopaedic surgery: A narrative review. JAAOS-J. Am. Acad. Orthop. Surg. 2014, 22, 800–809. [Google Scholar] [CrossRef]
- Mason, A.; Paulsen, R.; Babuska, J.M.; Rajpal, S.; Burneikiene, S.; Nelson, E.L.; Villavicencio, A.T. The accuracy of pedicle screw placement using intraoperative image guidance systems. J. Neurosurg. Spine 2014, 20, 196–203. [Google Scholar] [CrossRef]
- Meng, X.T.; Guan, X.F.; Zhang, H.L.; He, S.S. Computer navigation versus fluoroscopy-guided navigation for thoracic pedicle screw placement: A meta-analysis. Neurosurg. Rev. 2016, 39, 385–391. [Google Scholar] [CrossRef]
- Perdomo-Pantoja, A.; Ishida, W.; Zygourakis, C.; Holmes, C.; Iyer, R.R.; Cottrill, E.; Theodore, N.; Witham, T.F.; Lo, S.-F.L. Accuracy of Current Techniques for Placement of Pedicle Screws in the Spine: A Comprehensive Systematic Review and Meta-Analysis of 51,161 Screws. World Neurosurg. 2019, 126, 664–678. [Google Scholar] [CrossRef]
- Shin, B.J.; James, A.R.; Njoku, I.U.; Härtl, R. Pedicle screw navigation: A systematic review and meta-analysis of perforation risk for computer-navigated versus freehand insertion: A review. J. Neurosurg. Spine 2012, 17, 113–122. [Google Scholar] [CrossRef]
- Tian, N.-F.; Huang, Q.-S.; Zhou, P.; Zhou, Y.; Wu, R.-K.; Lou, Y.; Xu, H.-Z. Pedicle screw insertion accuracy with different assisted methods: A systematic review and meta-analysis of comparative studies. Eur. Spine J. 2011, 20, 846–859. [Google Scholar] [CrossRef]
- Tian, N.-F.; Xu, H.-Z. Image-guided pedicle screw insertion accuracy: A meta-analysis. Int. Orthop. 2009, 33, 895–903. [Google Scholar] [CrossRef]
- Noriega, D.C.; Hernández-Ramajo, R.; Milano, F.R.-M.; Sanchez-Lite, I.; Toribio, B.; Ardura, F.; Torres, R.; Corredera, R.; Kruger, A. Risk-benefit analysis of navigation techniques for vertebral transpedicular instrumentation: A prospective study. Spine J. 2017, 17, 70–75. [Google Scholar] [CrossRef]
- Verma, S.K.; Singh, P.K.; Agrawal, D.; Sinha, S.; Gupta, D.; Satyarthee, G.D.; Sharma, B.S. O-arm with navigation versus C-arm: A review of screw placement over 3 years at a major trauma center. Br. J. Neurosurg. 2016, 30, 658–661. [Google Scholar] [CrossRef]
- Hecht, N.; Kamphuis, M.; Czabanka, M.; Hamm, B.; König, S.; Woitzik, J.; Synowitz, M.; Vajkoczy, P. Accuracy and workflow of navigated spinal instrumentation with the mobile AIRO® CT scanner. Eur. Spine J. 2016, 25, 716–723. [Google Scholar] [CrossRef]
- Hecht, N.; Yassin, H.; Czabanka, M.; Föhre, B.; Arden, K.; Liebig, T.; Vajkoczy, P. Intraoperative Computed Tomography Versus 3D C-Arm Imaging for Navigated Spinal Instrumentation. Spine 2018, 43, 370–377. [Google Scholar] [CrossRef]
- Farah, K.; Coudert, P.; Graillon, T.; Blondel, B.; Dufour, H.; Gille, O.; Fuentes, S. Prospective Comparative Study in Spine Surgery Between O-Arm and Airo Systems: Efficacy and Radiation Exposure. World Neurosurg. 2018, 118, e175–e184. [Google Scholar] [CrossRef]
- Scarone, P.; Vincenzo, G.; Distefano, D.; Del Grande, F.; Cianfoni, A.; Presilla, S.; Reinert, M. Use of the Airo mobile intraoperative CT system versus the O-arm for transpedicular screw fixation in the thoracic and lumbar spine: A retrospective cohort study of 263 patients. J. Neurosurg. Spine 2018, 29, 397–406. [Google Scholar] [CrossRef]
- Hwang, Y.-S.; Tsai, H.-Y.; Lin, Y.-Y.; Lui, K.-W. Investigations of organ and effective doses of abdominal cone-beam computed tomography during transarterial chemoembolization using Monte Carlo simulation. BMC Med. Imaging 2018, 18, 2. [Google Scholar] [CrossRef]
- Gertzbein, S.D.; Robbins, S.E. Accuracy of pedicular screw placement in vivo. Spine 1990, 15, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Terander, A.; Burström, G.; Nachabe, R.; Skulason, H.; Pedersen, K.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Söderman, M.; Holmin, S.; et al. Pedicle Screw Placement Using Augmented Reality Surgical Navigation with Intraoperative 3D Imaging: A First In-Human Prospective Cohort Study. Spine 2018, 44, 517. [Google Scholar] [CrossRef]
- Ryang, Y.M.; Villard, J.; Obermüller, T.; Friedrich, B.; Wolf, P.; Gempt, J.; Ringel, F.; Meyer, B. Learning curve of 3D fluoroscopy image-guided pedicle screw placement in the thoracolumbar spine. Spine J. 2015, 15, 467–476. [Google Scholar] [CrossRef]
- Tabaraee, E.; Gibson, A.G.; Karahalios, D.G.; Potts, E.A.; Mobasser, J.-P.; Burch, S. Intraoperative cone beam-computed tomography with navigation (O-ARM) versus conventional fluoroscopy (C-ARM): A cadaveric study comparing accuracy, efficiency, and safety for spinal instrumentation. Spine 2013, 38, 1953–1958. [Google Scholar] [CrossRef]
- Sun, J.; Wu, D.; Wang, Q.; Wei, Y.; Yuan, F. Pedicle Screw Insertion: Is O-Arm-Based Navigation Superior to the Conventional Freehand Technique? A Systematic Review and Meta-Analysis. World Neurosurg. 2020, 144, e87–e99. [Google Scholar] [CrossRef]
- Tajsic, T.; Patel, K.; Farmer, R.; Mannion, R.J.; Trivedi, R.A. Spinal navigation for minimally invasive thoracic and lumbosacral spine fixation: Implications for radiation exposure, operative time, and accuracy of pedicle screw placement. Eur. Spine J. 2018, 27, 1918–1924. [Google Scholar] [CrossRef]
- Tkatschenko, D.; Kendlbacher, P.; Czabanka, M.; Bohner, G.; Vajkoczy, P.; Hecht, N. Navigated percutaneous versus open pedicle screw implantation using intraoperative CT and robotic cone-beam CT imaging. Eur. Spine J. 2020, 29, 803–812. [Google Scholar] [CrossRef]
- Rampersaud, Y.R.; Foley, K.T.; Shen, A.C.; Williams, S.; Solomito, M. Radiation exposure to the spine surgeon during fluoroscopically assisted pedicle screw insertion. Spine 2020, 25, 2637–2645. [Google Scholar] [CrossRef]
- Puvanesarajah, V.; Liauw, J.A.; Lo, S.F.; Lina, I.A.; Witham, T.F. Techniques and accuracy of thoracolumbar pedicle screw placement. World J. Orthop. 2014, 5, 112–123. [Google Scholar] [CrossRef]
- Villard, J.; Ryang, Y.-M.; Demetriades, A.K.; Reinke, A.; Behr, M.; Preuss, A.; Meyer, B.; Ringel, F. Radiation exposure to the surgeon and the patient during posterior lumbar spinal instrumentation: A prospective randomized comparison of navigated versus non-navigated freehand techniques. Spine 2014, 39, 1004–1009. [Google Scholar] [CrossRef]
- Pennington, Z.; Cottrill, E.; Westbroek, E.M.; Goodwin, M.L.; Lubelski, D.; Ahmed, A.K.; Sciubba, D.M. Evaluation of surgeon and patient radiation exposure by imaging technology in patients undergoing thoracolumbar fusion: Systematic review of the literature. Spine J. 2019, 19, 1397–1411. [Google Scholar] [CrossRef]
- Mendelsohn, D.; Strelzow, J.; Dea, N.; Ford, N.L.; Batke, J.; Pennington, A.; Yang, K.; Ailon, T.; Boyd, M.; Dvorak, M.; et al. Patient and surgeon radiation exposure during spinal instrumentation using intraoperative computed tomography-based navigation. Spine J. 2016, 16, 343–354. [Google Scholar] [CrossRef]
- Foster, N.; Shaffrey, C.; Buchholz, A.; Turner, R.; Yang, L.Z.; Niedzwiecki, D.; Goode, A. Image Quality and Dose Comparison of 3 Mobile Intraoperative Three-Dimensional Imaging Systems in Spine Surgery. World Neurosurg. 2022, 160, e142–e151. [Google Scholar] [CrossRef]
- Keil, H.; Luxenhofer, M.; Vetter, S.Y.; Beisemann, N.; Grützner, P.A.; Franke, J. Evaluation of image quality and assessability of a new flat-panel 3D C-arm compared to mobile and fixed computed tomography in posterior spinal fixation. Int. J. Med. Robot. Comput. Assist. Surg. 2020, 17, e2181. [Google Scholar] [CrossRef]
- Sarwahi, V.; Payares, M.; Wendolowski, S.; Maguire, K.; Thornhill, B.; Lo, Y.; Amaral, T.D. Low-Dose Radiation 3D Intraoperative Imaging: How Low Can We Go? An O-Arm, CT Scan, Cadaveric Study. Spine 2017, 42, E1311–E1317. [Google Scholar] [CrossRef]
- Rajasekaran, S.; Bhushan, M.; Aiyer, S.; Kanna, R.; Shetty, A.P. Accuracy of pedicle screw insertion by AIRO® intraoperative CT in complex spinal deformity assessed by a new classification based on technical complexity of screw insertion. Eur. Spine J. 2018, 27, 2339–2347. [Google Scholar] [CrossRef]
- Burström, G.; Nachabe, R.; Persson, O.; Edström, E.; Elmi Terander, A. Augmented and Virtual Reality Instrument Tracking for Minimally Invasive Spine Surgery: A Feasibility and Accuracy Study. Spine 2019, 44, 1097–1104. [Google Scholar] [CrossRef]
- Beisemann, N.; Gierse, J.; Mandelka, E.; Hassel, F.; Grützner, P.A.; Franke, J.; Vetter, S.Y. Comparison of three imaging and navigation systems regarding accuracy of pedicle screw placement in a sawbone model. Sci. Rep. 2022, 12, 12344. [Google Scholar] [CrossRef]
- Laudato, P.A.; Pierzchala, K.; Schizas, C. Pedicle Screw Insertion Accuracy Using O-Arm, Robotic Guidance, or Freehand Technique: A Comparative Study. Spine 2018, 43, E373–E378. [Google Scholar] [CrossRef]
- Pojskić, M.; Bopp, M.; Nimsky, C.; Carl, B.; Saβ, B. Initial Intraoperative Experience with Robotic-Assisted Pedicle Screw Placement with Cirq® Robotic Alignment: An Evaluation of the First 70 Screws. J. Clin. Med. 2021, 10, 5725. [Google Scholar] [CrossRef]
- Gonzalvo, A.; Fitt, G.; Liew, S.; de la Harpe, D.; Turner, P.; Ton, L.; Rogers, M.A.; Wilde, P.H. The learning curve of pedicle screw placement: How many screws are enough? Spine 2009, 34, E761–E765. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Diagnosis | No. of Screws Placed | No. of Levels Fused | Levels Fused | Further Interventions | OT 1 [min] | NT 2 [min] | mSPT 3 [mm:ss] |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 78 | Spondylodiscitis | 8 | 3 | L3-S1 | None | 86 | 54 | 3:18 |
| 2 | 73 | Fracture T12/L1 | 8 | 3 | T11-L2 | None | 94 | 43 | 3:27 |
| 3 | 65 | Fracture L2 | 6 | 2 | T12-L2 | None | 74 | 31 | 2:02 |
| 4 | 82 | Fracture L2/3 | 8 | 3 | L1-L4 | None | 116 | 66 | 5:22 |
| 5 | 57 | Fracture T8/9 | 8 | 3 | T7-T10 | None | 90 | 41 | 2:45 |
| 6 | 78 | Fracture T3 | 10 | 4 | T1-T5 | None | 107 | 58 | 3:17 |
| 7 | 54 | Fracture T4 | 8 | 3 | T2-T5 | None | 89 | 34 | 2:21 |
| 8 | 78 | Spondylodiscitis | 8 | 3 | L2-L5 | None | 77 | 46 | 1:39 |
| 9 | 69 | Fracture L2 | 4 | 2 | L1 onto L3 | BSC * L2 | 58 | 18 | 2:57 |
| 10 | 80 | Fracture T7 | 8 | 3 | T5-T8 | None | 93 | 63 | 4:07 |
| 11 | 82 | Spondylodiscitis | 8 | 3 | T7-T10 | None | 95 | 54 | 2:34 |
| 12 | 78 | Fracture L1 | 8 | 4 | T11/12 onto L2/3 | CA# | 130 | 32 | 1:56 |
| 13 | 85 | Fracture L4 | 8 | 3 | L2-L5 | None | 132 | 43 | 3:16 |
| 14 | 71 | Fracture T12 | 8 | 4 | T10/11 onto L1/2 | CA# | 82 | 26 | 1:31 |
| 15 | 58 | Fracture L2 | 6 | 2 | L1-L3 | None | 62 | 24 | 2:08 |
| 16 | 59 | Spondylodiscitis | 8 | 3 | T2-T5 | None | 100 | 47 | 3:09 |
| 17 | 61 | Fracture T6 | 8 | 4 | T4/5 onto T7/8 | BSC * T6, CA # | 106 | 42 | 1:53 |
| 18 | 56 | Spondylodiscitis | 12 | 5 | L1/2/3 onto L4/5/S1 | None | 112 | 52 | 2:11 |
| 19 | 58 | Fracture L2 | 6 | 3 | L1-L3 | None | 69 | 28 | 2:45 |
| 20 | 50 | Spondylodiscitis | 8 | 3 | T6-T9 | None | 73 | 33 | 1:48 |
| Mean | 95% CI 1 | |
|---|---|---|
| Dose area product (Gycm2) | 29.78 | 22.43–37.12 |
| Fluoroscopy time (s) | 93.7 | 80.6–106.8 |
| Effective dose (mSv) | 7.46 | 5.77–9.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandelka, E.; Gierse, J.; Gruetzner, P.A.; Franke, J.; Vetter, S.Y. First Clinical Experience with a Novel 3D C-Arm-Based System for Navigated Percutaneous Thoracolumbar Pedicle Screw Placement. Medicina 2022, 58, 1111. https://doi.org/10.3390/medicina58081111
Mandelka E, Gierse J, Gruetzner PA, Franke J, Vetter SY. First Clinical Experience with a Novel 3D C-Arm-Based System for Navigated Percutaneous Thoracolumbar Pedicle Screw Placement. Medicina. 2022; 58(8):1111. https://doi.org/10.3390/medicina58081111
Chicago/Turabian StyleMandelka, Eric, Jula Gierse, Paul A. Gruetzner, Jochen Franke, and Sven Y. Vetter. 2022. "First Clinical Experience with a Novel 3D C-Arm-Based System for Navigated Percutaneous Thoracolumbar Pedicle Screw Placement" Medicina 58, no. 8: 1111. https://doi.org/10.3390/medicina58081111