
Continuous Rod Load Monitoring to Assess Spinal Fusion Status–Pilot In Vivo Data in Sheep

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
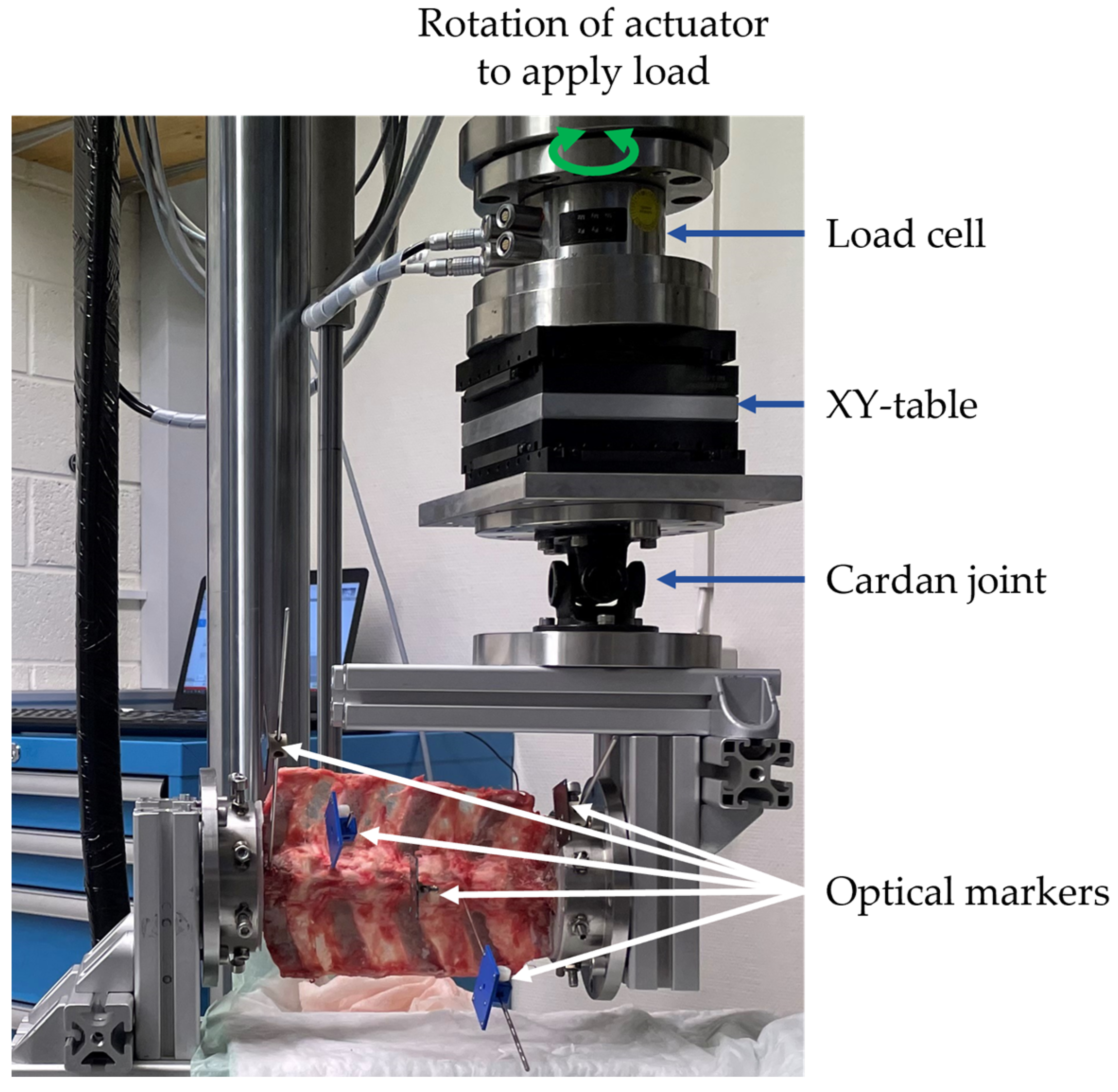
2. Materials and Methods
2.1. Implantable Sensor System
2.2. Animal Study
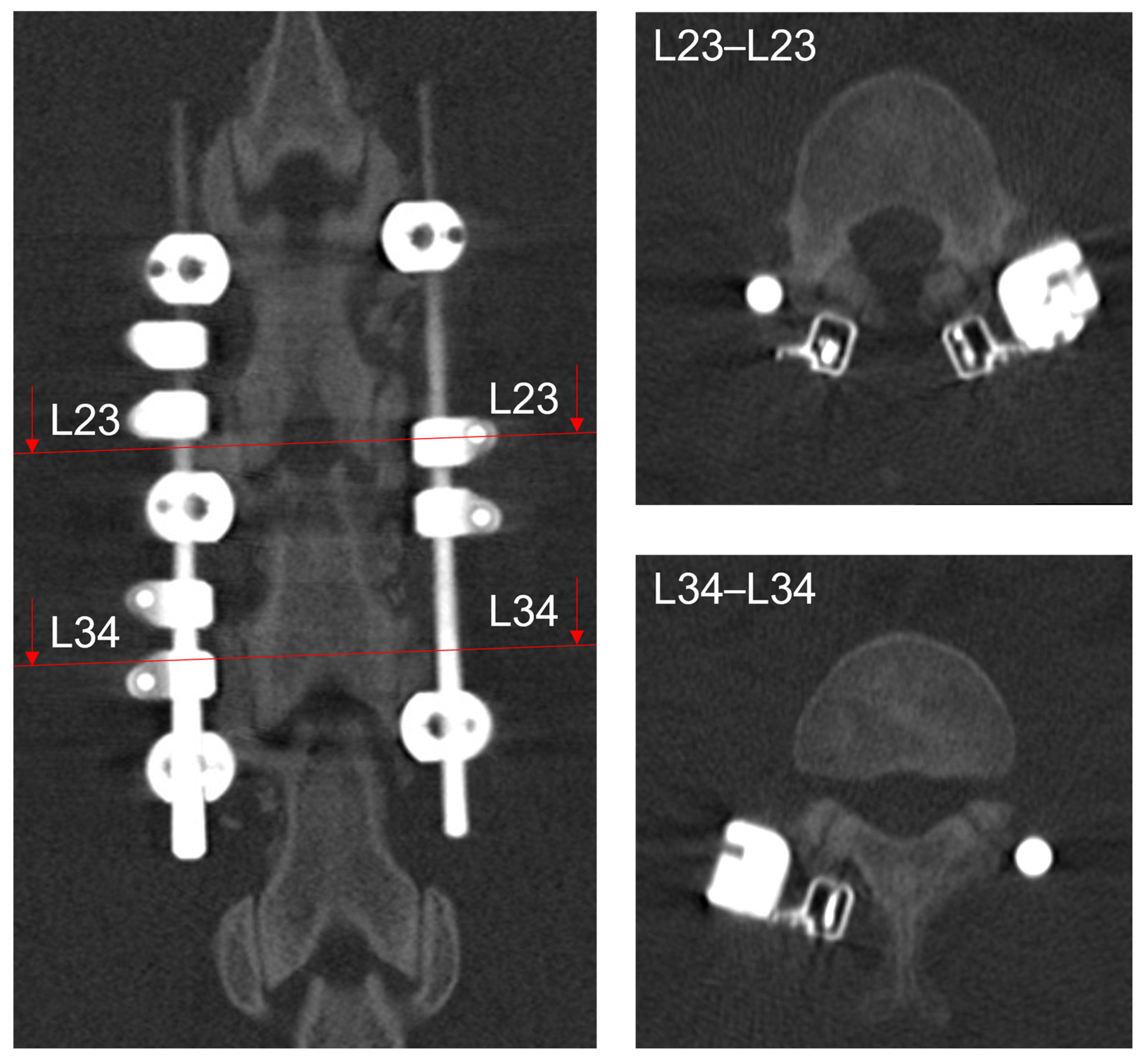
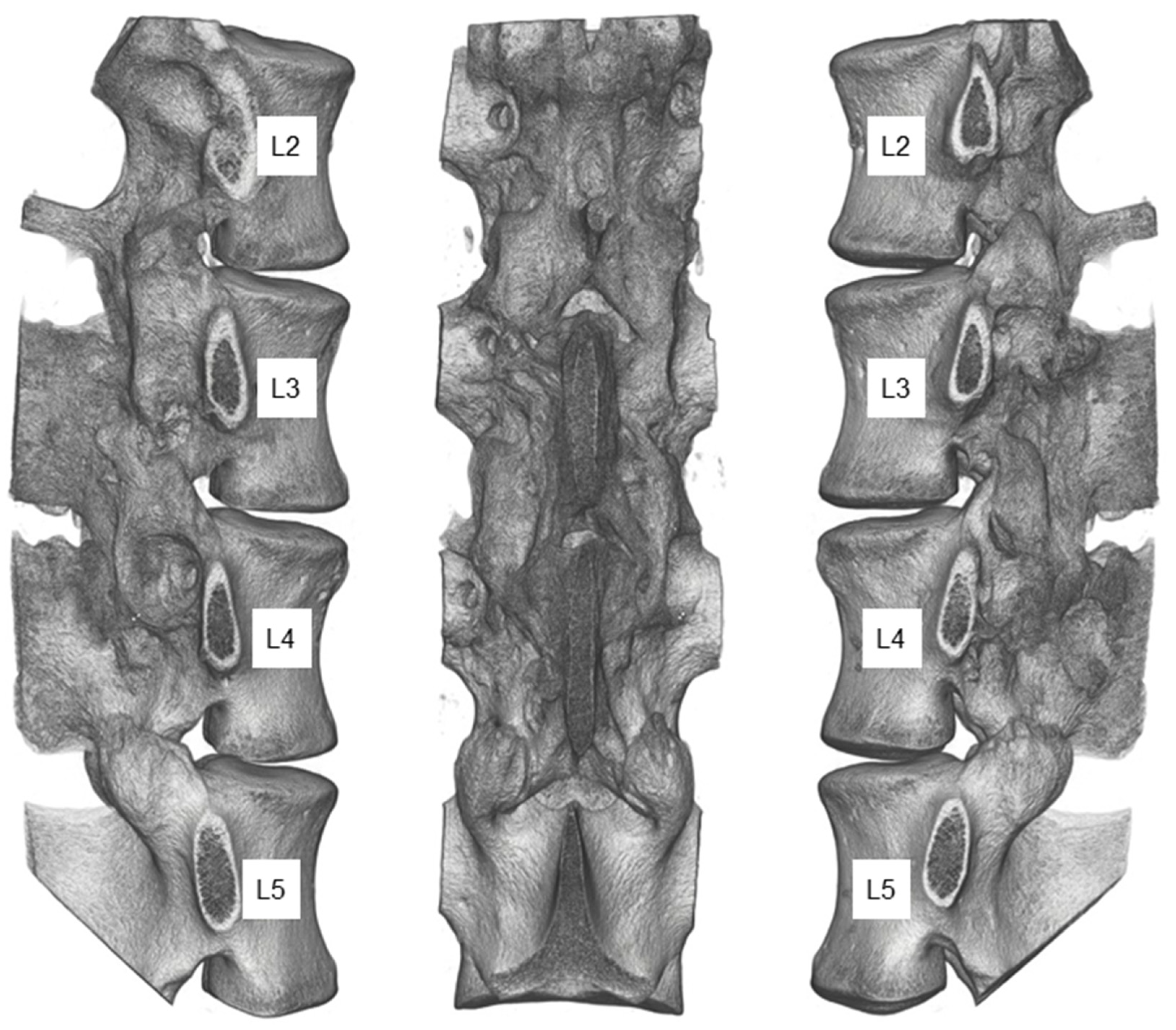
2.3. Postmortem Evaluation
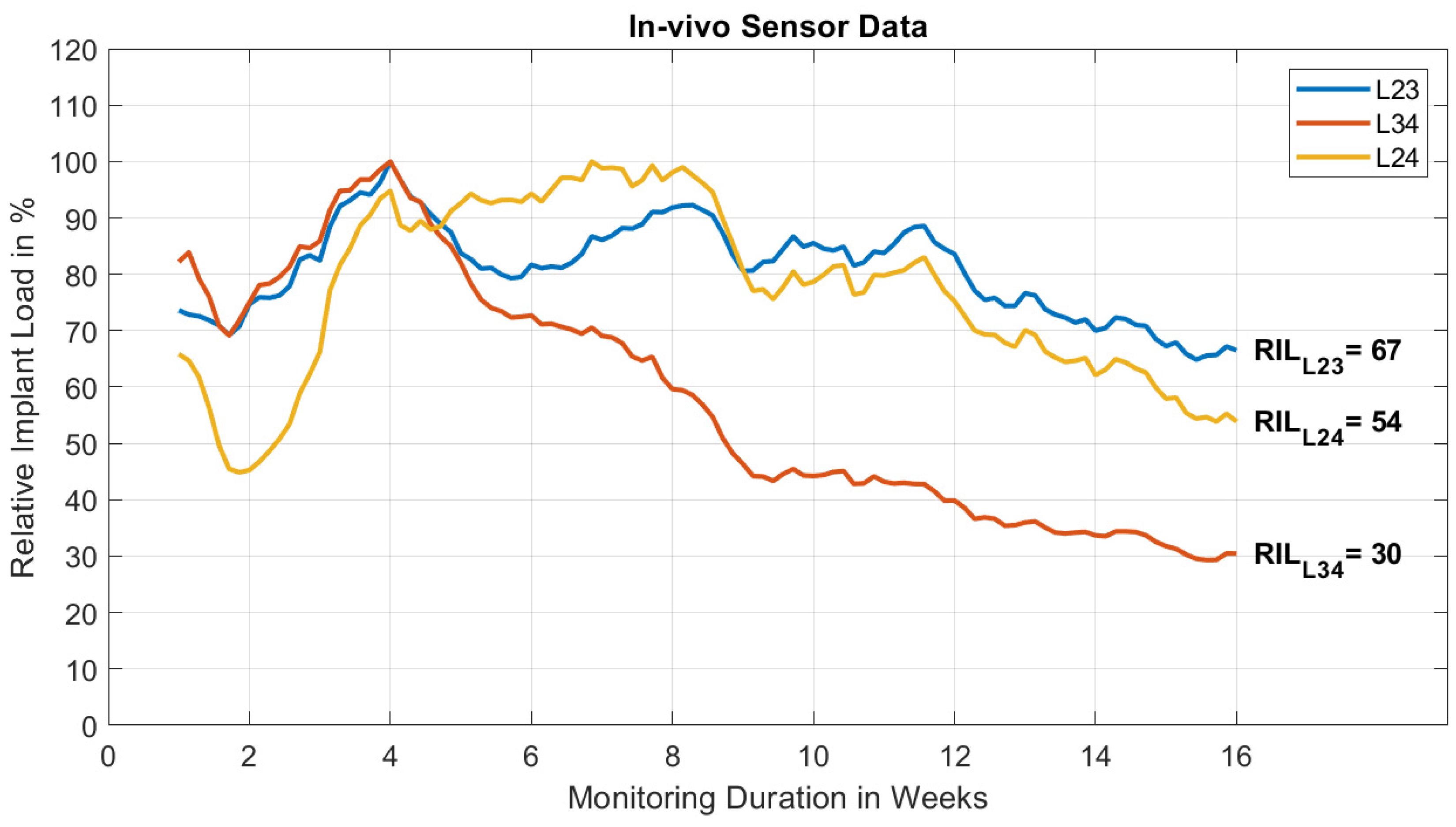
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yang, J.H.; Glaeser, J.D.; Kanim, L.E.A.; Battles, C.Y.; Bondre, S.; Bae, H.W. Bone Grafts and Bone Graft Substitutes. In Handbook of Spine Technology; Cheng, B.C., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 197–273. [Google Scholar] [CrossRef]
- Chun, D.S.; Baker, K.C.; Hsu, W.K. Lumbar pseudarthrosis: A review of current diagnosis and treatment. Neurosurg. Focus 2015, 39, E10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.; Dorcil, J.; Radomisli, T.E. Nonunion of the Spine: A Review. Clin. Orthop. Relat. Res. 2004, 419, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Carreon, L.Y.; Djurasovic, M.; Glassman, S.D.; Sailer, P. Diagnostic Accuracy and Reliability of Fine-Cut CT Scans With Reconstructions to Determine the Status of an Instrumented Posterolateral Fusion With Surgical Exploration as Reference Standard. Spine 2007, 32, 892–895. [Google Scholar] [CrossRef] [PubMed]
- Swink, I.R.; Jaffee, S.; Diehl, D.; Xu, C.; Carbone, J.; Yu, A.K.; Cheng, B.C. Cyclical Loading to Evaluate the Bone Implant Interface. In Handbook of Spine Technology; Cheng, B.C., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 377–400. [Google Scholar] [CrossRef]
- Umali, J.; Ghahreman, A.; Diwan, A.D. Spinal Fusion Evaluation in Various Settings: A Summary of Human-Only Studies. In Handbook of Spine Technology; Cheng, B.C., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 1131–1147. [Google Scholar] [CrossRef]
- Blumenthal, S.L.; Gill, K. Can lumbar spine radiographs accurately determine fusion in postoperative patients? Correlation of routine radiographs with a second surgical look at lumbar fusions. Spine (Phila Pa 1976) 1993, 18, 1186–1189. [Google Scholar] [CrossRef]
- Ramakrishna, V.A.S.; Chamoli, U.; Rajan, G.; Mukhopadhyay, S.C.; Prusty, B.G.; Diwan, A.D. Smart orthopaedic implants: A targeted approach for continuous postoperative evaluation in the spine. J. Biomech. 2020, 104, 109690. [Google Scholar] [CrossRef]
- Ernst, M.; Richards, R.G.; Windolf, M. Smart implants in fracture care–only buzzword or real opportunity? Injury 2021, 52, S101–S105. [Google Scholar] [CrossRef]
- Rohlmann, A.; Eick, O.; Bergmann, G.; Graichen, F. In-vitro measurement of loading using an instrumented vertebral internal fixator. Z. Orthop. Ihre Grenzgeb. 1995, 133, 136–140. [Google Scholar] [CrossRef]
- Aebersold, J.W.; Hnat, W.P.; Voor, M.J.; Puno, R.M.; Jackson, D.J.; Lin, J.T.; Walsh, K.M.; Naber, J.F. Development of a Strain Transferring Sensor Housing for a Lumbar Spinal Fusion Detection System. J. Med. Devices 2006, 1, 159–164. [Google Scholar] [CrossRef]
- Lin, J.-T.; Walsh, K.W.; Jackson, D.; Aebersold, J.; Crain, M.; Naber, J.F.; Hnat, W.P. Development of capacitive pure bending strain sensor for wireless spinal fusion monitoring. Sens. Actuators A Phys. 2007, 138, 276–287. [Google Scholar] [CrossRef]
- Daniels, A.U.; Gemperline, P.; Grahn, A.R.; Dunn, H.K. A new method for continuous intraoperative measurement of Harrington rod loading patterns. Ann. Biomed. Eng. 1984, 12, 233–246. [Google Scholar] [CrossRef]
- Kanayama, M.; Cunningham, B.W.; Weis, J.C.; Parker, L.M.; Kaneda, K.; McAFEE, P.C. Maturation of the Posterolateral Spinal Fusion and Its Effect on Load-Sharing of Spinal Instrumentation. An In Vivo Sheep Model. JBJS 1997, 79, 1710–1720. [Google Scholar] [CrossRef] [PubMed]
- Waugh, T.R. Intravital Measurements During Instrumental Correction of Idiopathic Scoliosis. Acta Orthop. Scand. 1966, 37, 1–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szivek, J.A.; Roberto, R.F.; Margolis, D.S. In vivo strain measurements from hardware and lamina during spine fusion. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 75, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Rohlmann, A.; Graichen, F.; Weber, U.; Bergmann, G. 2000 Volvo Award winner in biomechanical studies: Monitoring in vivo implant loads with a telemeterized internal spinal fixation device. Spine (Phila Pa 1976) 2000, 25, 2981–2986. [Google Scholar] [CrossRef]
- Ernst, M.; Baumgartner, H.; Döbele, S.; Höntzsch, D.; Pohlemann, T.; Windolf, M. Clinical feasibility of fracture healing assessment through continuous monitoring of implant load. J. Biomech. 2021, 116, 110188. [Google Scholar] [CrossRef]
- Windolf, M.; Ernst, M.; Schwyn, R.; Perren, S.; Mathis, H.; Wilke, M.; Richards, R. A Biofeedback System for Continuous Monitoring of Bone Healing. In Proceedings of the Biodevices-2014, Angers, France, 3–6 March 2014; pp. 243–248. [Google Scholar]
- Windolf, M.; Varjas, V.; Gehweiler, D.; Schwyn, R.; Arens, D.; Constant, C.; Zeiter, S.; Richards, R.G.; Ernst, M. Continuous Implant Load Monitoring to Assess Bone Healing Status—Evidence from Animal Testing. Medicina 2022, 58, 858. [Google Scholar] [CrossRef]
- Wilke, H.-J.; Claes, L.; Schmitt, H.; Wolf, S. A universal spine tester for in vitro experiments with muscle force simulation. Eur. Spine J. 1994, 3, 91–97. [Google Scholar] [CrossRef]
- Wilke, H.-J.; Wenger, K.; Claes, L. Testing criteria for spinal implants: Recommendations for the standardization of in vitro stability testing of spinal implants. Eur. Spine J. 1998, 7, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Wilke, H.-J.; Jungkunz, B.; Wenger, K.; Claes, L.E. Spinal segment range of motion as a function of in vitro test conditions: Effects of exposure period, accumulated cycles, angular-deformation rate, and moisture condition. Anat. Rec. 1998, 251, 15–19. [Google Scholar] [CrossRef]
- Kanayama, M.; Cunningham, B.W.; Weis, J.C.; Parker, L.M.; Kaneda, K.; McAfee, P.C. The effects of rigid spinal instrumentation and solid bony fusion on spinal kinematics. A posterolateral spinal arthrodesis model. Spine (Phila Pa 1976) 1998, 23, 767–773. [Google Scholar] [CrossRef]
- Panjabi, M.M. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J. Spinal Disord. 1992, 5, 390–396, discussion 397. [Google Scholar] [CrossRef] [PubMed]
- Rohlmann, A.; Bergmann, G.; Graichen, F.; Mayer, H.-M. Influence of Muscle Forces on Loads in Internal Spinal Fixation Devices. Spine 1998, 23, 537–542. [Google Scholar] [CrossRef] [PubMed]
- White, A.A.; Panjabi, M.M. Clinical Biomechanics of the Spine; Lippincott: Philadelphia, PA, USA, 1990. [Google Scholar]
- Zeng, Z.-L.; Zhu, R.; Wu, Y.-C.; Zuo, W.; Yu, Y.; Wang, J.-J.; Cheng, L.-M. Effect of Graded Facetectomy on Lumbar Biomechanics. J. Healthc. Eng. 2017, 2017, 7981513. [Google Scholar] [CrossRef] [PubMed]
- Wilke, H.-J.; Kettler, A.; Claes, L.E. Are sheep spines a valid biomechanical model for human spines? Spine (Phila Pa 1976) 1997, 22, 2365–2374. [Google Scholar] [CrossRef]
- Wilke, H.-J.; Kettler, A.; Wenger, K.H.; Claes, L.E. Anatomy of the sheep spine and its comparison to the human spine. Anat. Rec. 1997, 247, 542–555. [Google Scholar] [CrossRef]
- Kavlock, K.; Nagaraja, S.; Peck, J. FDA Premarket Review of Orthopedic Spinal Devices. In Handbook of Spine Technology; Cheng, B.C., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 401–422. [Google Scholar] [CrossRef]
- Martini, L.; Fini, M.; Giavaresi, G.; Giardino, R. Sheep Model in Orthopedic Research: A Literature Review. Comp. Med. 2001, 51, 292–299. [Google Scholar]
- Smit, T.H. The use of a quadruped as an in vivo model for the study of the spine–biomechanical considerations. Eur. Spine J. 2002, 11, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Grgurevic, L.; Erjavec, I.; Gupta, M.; Pecin, M.; Bordukalo-Niksic, T.; Stokovic, N.; Vnuk, D.; Farkas, V.; Capak, H.; Milosevic, M.; et al. Autologous blood coagulum containing rhBMP6 induces new bone formation to promote anterior lumbar interbody fusion (ALIF) and posterolateral lumbar fusion (PLF) of spine in sheep. Bone 2020, 138, 115448. [Google Scholar] [CrossRef]
- Makanji, H.; Schoenfeld, A.J.; Bhalla, A.; Bono, C.M. Critical analysis of trends in lumbar fusion for degenerative disorders revisited: Influence of technique on fusion rate and clinical outcomes. Eur. Spine J. 2018, 27, 1868–1876. [Google Scholar] [CrossRef]
- Mohi Eldin, M.M.; Ali, A.M.A. Lumbar transpedicular implant failure: A clinical and surgical challenge and its radiological assessment. Asian Spine J. 2014, 8, 281–297. [Google Scholar] [CrossRef]
- La Barbera, L.; Galbusera, F.; Wilke, H.J.; Villa, T. Preclinical evaluation of posterior spine stabilization devices: Can we compare in vitro and in vivo loads on the instrumentation? Eur. Spine J. 2017, 26, 200–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilke, H.-J.; Rohlmann, A.; Neller, S.; Schulthei, M.; Bergmann, G.; Graichen, F.; Claes, L.E. Is It Possible to Simulate Physiologic Loading Conditions by Applying Pure Moments?: A Comparison of In Vivo and In Vitro: Load Components in an Internal Fixator. Spine 2001, 26, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Rohlmann, A.; Bergmann, G.; Graichen, F.; Weber, U. Comparison of loads on internal spinal fixation devices measured in vitro and in vivo. Med. Eng. Phys. 1997, 19, 539–546. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Windolf, M.; Heumann, M.; Varjas, V.; Constant, C.; Ernst, M.; Richards, R.G.; Wilke, H.-J.; Benneker, L.M. Continuous Rod Load Monitoring to Assess Spinal Fusion Status–Pilot In Vivo Data in Sheep. Medicina 2022, 58, 899. https://doi.org/10.3390/medicina58070899
Windolf M, Heumann M, Varjas V, Constant C, Ernst M, Richards RG, Wilke H-J, Benneker LM. Continuous Rod Load Monitoring to Assess Spinal Fusion Status–Pilot In Vivo Data in Sheep. Medicina. 2022; 58(7):899. https://doi.org/10.3390/medicina58070899
Chicago/Turabian StyleWindolf, Markus, Maximilian Heumann, Viktor Varjas, Caroline Constant, Manuela Ernst, Robert Geoff Richards, Hans-Joachim Wilke, and Lorin Michael Benneker. 2022. "Continuous Rod Load Monitoring to Assess Spinal Fusion Status–Pilot In Vivo Data in Sheep" Medicina 58, no. 7: 899. https://doi.org/10.3390/medicina58070899