
Comparison of Endodontic Failures between Nonsurgical Retreatment and Endodontic Surgery: Systematic Review and Meta-Analysis with Trial Sequential Analysis

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
- I.
- Evaluation of the coronal seal: the presence of an adequate coronal restoration or a still functional prosthetic crown that seals the endodontium coronally or whose removal involves the non-restorability can lead to the choice towards surgical endodontic retreatment. On the contrary, a restoration no longer adequate, with good access to the endodontium, may lead to the choice of non-surgical endodontic retreatment [8].
- II.
- Radiographic evaluation of root canal obturation: the presence of untreated canals and a coarse filling of the canals may lead to the choice of non-surgical endodontic retreatment. On the contrary, a surgical approach could be recommended in the presence of an apparent adequate apical seal or in the presence of a root canal obturation that is far from the radiographic apex of only 1 mm (in the presence of course of symptoms of a periapical pathology), and a surgical approach should be evaluated [9,10,11].
- III.
- The presence of clinical complications such as the finding of fractured instruments (apical third of the root), the presence of zipping of internal resorptions and the presence of root perforations or ledge formations; in these cases, the surgical approach may be a suitable choice [12].
- IV.
- In the presence of recurrent infections in which a root canal retreatment has already been carried out, a surgical endodontic retreatment is absolutely to be considered as a therapeutic choice [13].
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Sources of Information, Research and Selection
2.4. Data Collection Process and Data Characteristics
2.5. Risk of Bias in Individual Studies, Summary Measures, Summary of Results, Risk of Bias between Studies and Additional Measures
3. Results
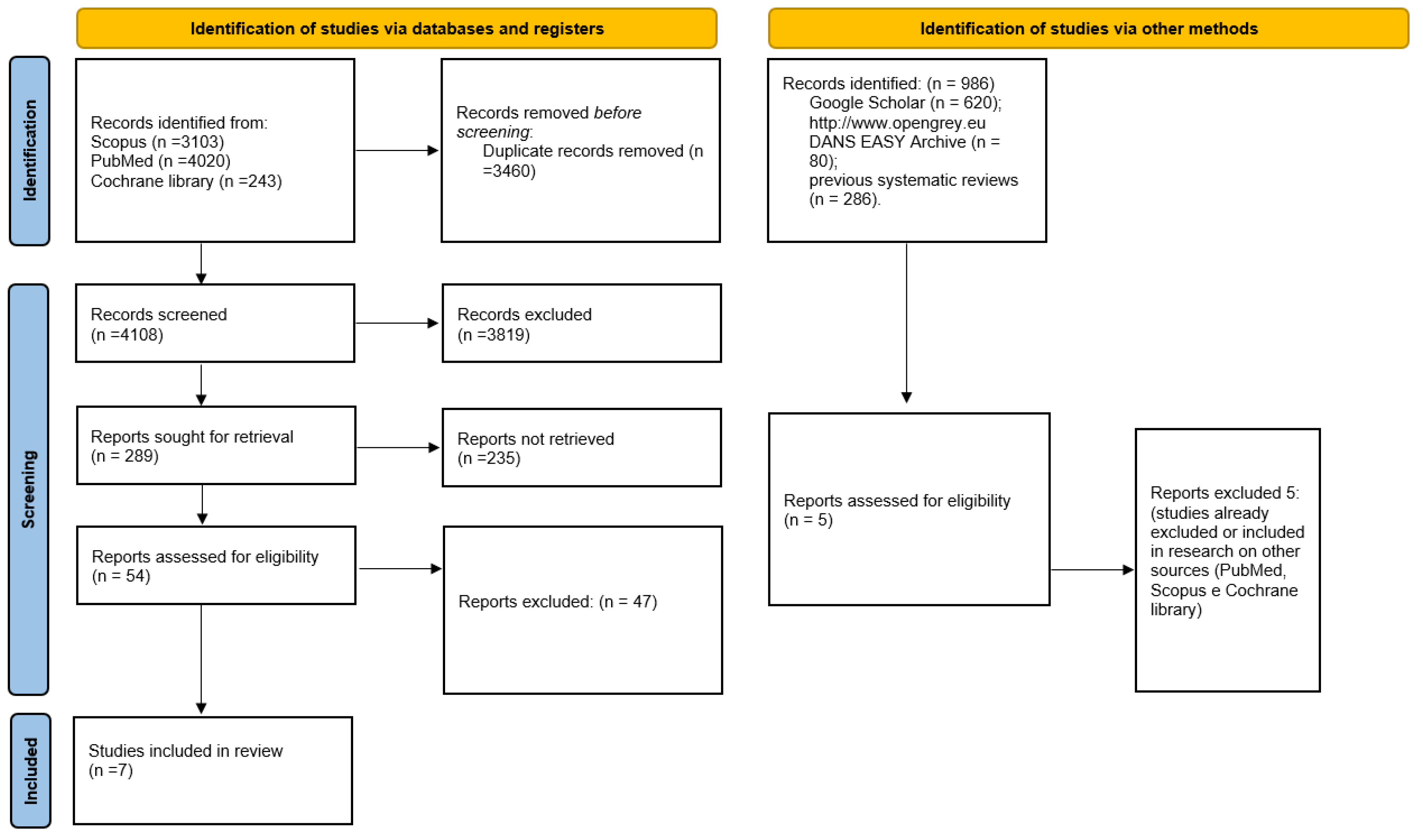
3.1. Selection of Studies
3.2. Data Characteristics
3.3. Risk of Bias
- (1)
- Non-response rate: Is the participation on/follow-up rate stated? Do the authors describe the effort to increase the participant/follow-up rate?
- (2)
- Representativeness of sample to target population: Were the subjects asked to participate in the study representative of the entire population from which they were recruited?
- (3)
- Validity and reliability of outcome measurement: Were the main outcome measures used accurate (valid and reliable)?
- (4)
- Amount of loss to follow-up: Are the non-participants/subjects lost to follow-up described? Do the authors describe the effort to increase the participation/follow-up rate?
- (5)
- Appropriate statistical tests: Are the statistical methods described?
3.4. Metanalysis
3.5. Trial Sequential Analysis, Grade
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boucher, Y.; Matossian, L.; Rilliard, F.; Machtou, P. Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. Int. Endod. J. 2002, 35, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Prada, I.; Micó-Muñoz, P.; Giner-Lluesma, T.; Micó-Martínez, P.; Collado-Castellano, N.; Manzano-Saiz, A. Influence of microbiology on endodontic failure. Literature review. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e364–e372. [Google Scholar] [CrossRef] [PubMed]
- Kayaoglu, G.; Ørstavik, D. Virulence factors of Enterococcus faecalis: Relationship to endodontic disease. Crit. Rev. Oral Biol. Med. 2004, 15, 308–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siqueira, J.F., Jr.; Rôças, I.N. Polymerase chain reaction detection of Propionibacterium propionicus and Actinomyces radicidentis in primary and persistent endodontic infections. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 215–222. [Google Scholar] [CrossRef]
- Torabinejad, M.; Corr, R.; Handysides, R.; Shabahang, S. Outcomes of nonsurgical retreatment and endodontic surgery: A systematic review. J. Endod. 2009, 35, 930–937. [Google Scholar] [CrossRef] [Green Version]
- Menini, M.; Pesce, P.; Bevilacqua, M.; Pera, F.; Tealdo, T.; Barberis, F.; Pera, P. Effect of Framework in an Implant-Supported Full-Arch Fixed Prosthesis: 3D Finite Element Analysis. Int. J. Prosthodont. 2015, 28, 627–630. [Google Scholar] [CrossRef] [Green Version]
- Karabucak, B.; Setzer, F. Criteria for the ideal treatment option for failed endodontics: Surgical or nonsurgical? Compend. Contin. Educ. Dent. 2007, 28, 304–310. [Google Scholar]
- Kalyani, P.; Patwa, N.; Gupta, N.; Bhatt, A.; Saha, S.; Kanjani, V. Clinical and radiographic assessment of post-treatment endodontic disease by primary healthcare professionals: A hospital-based 1-year follow-up. J. Fam. Med. Prim. Care 2022, 11, 1114–1118. [Google Scholar] [CrossRef]
- Javed, M.Q.; AlAttas, M.H.; Bhatti, U.A.; Dutta, S.D. Retrospective audit for quality assessment of root fillings performed by undergraduate dental students in clinics. J. Taibah Univ. Med. Sci. 2022, 17, 297–303. [Google Scholar] [CrossRef]
- Aga, N.; Thakur, M.K.; Agwan, M.A.S.; Eisa, M.; Habshi, A.Y.; Azeem, S. Evaluation of Quality of Endodontic Re-Treatment and Changes in Periapical Status. J. Pharm. BioAllied Sci. 2021, 13, S379–S382. [Google Scholar] [CrossRef]
- Al Shehadat, S.; El-Kishawi, M.; AlMudalal, A.; AlSaqer, A.; Nassar, A.; Zihlif, L.; Mahmoud, Y.; Nagendrababu, V.; Vinothkumar, T.S. An Audit of the Technical Quality and Iatrogenic Errors of Root Canal Treatment by Undergraduate Dental Students at the University of Sharjah. Eur. J. Dent. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Kalogeropoulos, K.; Xiropotamou, A.; Koletsi, D.; Tzanetakis, G.N. The Effect of Cone-Beam Computed Tomography (CBCT) Evaluation on Treatment Planning after Endodontic Instrument Fracture. Int. J. Environ. Res. Public Health 2022, 19, 4088. [Google Scholar] [CrossRef] [PubMed]
- Abusrewil, S.; Alshanta, O.A.; Albashaireh, K.; Alqahtani, S.; Nile, C.J.; Scott, J.A.; McLean, W. Detection, treatment and prevention of endodontic biofilm infections: What’s new in 2020? Crit. Rev. Microbiol. 2020, 46, 194–212. [Google Scholar] [CrossRef] [PubMed]
- Haxhia, E.; Ibrahim, M.; Bhagavatula, P. Root-end Surgery or Nonsurgical Retreatment: Are There Differences in Long-term Outcome? J. Endod. 2021, 47, 1272–1277. [Google Scholar] [CrossRef]
- Alghamdi, F.; Alhaddad, A.J.; Abuzinadah, S. Healing of Periapical Lesions After Surgical Endodontic Retreatment: A Systematic Review. Cureus 2020, 12, e6916. [Google Scholar] [CrossRef] [Green Version]
- Pinto, D.; Marques, A.; Pereira, J.F.; Palma, P.J.; Santos, J.M. Long-Term Prognosis of Endodontic Microsurgery-A Systematic Review and Meta-Analysis. Medicina 2020, 56, 447. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Taschieri, S.; Testori, T.; Francetti, L.; Weinstein, R.L. Surgical versus non-surgical endodontic re-treatment for periradicular lesions. Cochrane Database Syst. Rev. 2007, Cd005511. [Google Scholar] [CrossRef]
- Danin, J.; Strömberg, T.; Forsgren, H.; Linder, L.E.; Ramsköld, L.O. Clinical management of nonhealing periradicular pathosis. Surgery versus endodontic retreatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 213–217. [Google Scholar] [CrossRef]
- Kvist, T.; Reit, C. Results of endodontic retreatment: A randomized clinical study comparing surgical and nonsurgical procedures. J. Endod. 1999, 25, 814–817. [Google Scholar] [CrossRef]
- Kang, M.; In Jung, H.; Song, M.; Kim, S.Y.; Kim, H.C.; Kim, E. Outcome of nonsurgical retreatment and endodontic microsurgery: A meta-analysis. Clin. Oral Investig. 2015, 19, 569–582. [Google Scholar] [CrossRef]
- Dioguardi, M.; Alovisi, M.; Sovereto, D.; Troiano, G.; Malagnino, G.; di Cosola, M.; Cazzolla, A.P.; Laino, L.; Lo Muzio, L. Sealing ability and microbial leakage of root-end filling materials: MTA versus epoxy resin: A systematic review and meta-analysis. Heliyon 2021, 7, e07494. [Google Scholar] [CrossRef] [PubMed]
- Menini, M.; Pesce, P.; Pera, F.; Barberis, F.; Lagazzo, A.; Bertola, L.; Pera, P. Biological and mechanical characterization of carbon fiber frameworks for dental implant applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 70, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Grassi, F.R.; Pappalettere, C.; di Comite, M.; Corsalini, M.; Mori, G.; Ballini, A.; Crincoli, V.; Pettini, F.; Rapone, B.; Boccaccio, A. Effect of different irrigating solutions and endodontic sealers on bond strength of the dentin-post interface with and without defects. Int. J. Med. Sci. 2012, 9, 642–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Macfarlane, T.V.; Glenny, A.M.; Worthington, H.V. Systematic review of population-based epidemiological studies of oro-facial pain. J. Dent. 2001, 29, 451–467. [Google Scholar] [CrossRef]
- Pesce, P.; Menini, M.; Tommasato, G.; Patini, R.; Canullo, L. Influence of modified titanium abutment surface on peri-implant soft tissue behaviour: A systematic review of histological findings. Int. J. Oral Implantol. 2019, 12, 419–429. [Google Scholar]
- Castellini, G.; Bruschettini, M.; Gianola, S.; Gluud, C.; Moja, L. Assessing imprecision in Cochrane systematic reviews: A comparison of GRADE and Trial Sequential Analysis. Syst. Rev. 2018, 7, 110. [Google Scholar] [CrossRef] [Green Version]
- Curtis, D.M.; VanderWeele, R.A.; Ray, J.J.; Wealleans, J.A. Clinician-centered Outcomes Assessment of Retreatment and Endodontic Microsurgery Using Cone-beam Computed Tomographic Volumetric Analysis. J. Endod. 2018, 44, 1251–1256. [Google Scholar] [CrossRef]
- Calişkan, M.K. Nonsurgical retreatment of teeth with periapical lesions previously managed by either endodontic or surgical intervention. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 242–248. [Google Scholar] [CrossRef]
- Allen, R.K.; Newton, C.W.; Brown, C.E., Jr. A statistical analysis of surgical and nonsurgical endodontic retreatment cases. J. Endod. 1989, 15, 261–266. [Google Scholar] [CrossRef]
- Riis, A.; Taschieri, S.; del Fabbro, M.; Kvist, T. Tooth Survival after Surgical or Nonsurgical Endodontic Retreatment: Long-term Follow-up of a Randomized Clinical Trial. J. Endod. 2018, 44, 1480–1486. [Google Scholar] [CrossRef] [PubMed]
- Ercan, E.; Dalli, M.; Duülgergil, C.T.; Yaman, F. Effect of intracanal medication with calcium hydroxide and 1% chlorhexidine in endodontic retreatment cases with periapical lesions: An In Vivo study. J. Formos. Med. Assoc. 2007, 106, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, B.J. The Pocket Guide to Critical Appraisal: A Handbook for Health Care Professionals. CMAJ Can. Med. Assoc. J. 1997, 157, 448. [Google Scholar]
- Miladinovic, B.; Hozo, I.; Djulbegovic, B. Trial Sequential Boundaries for Cumulative Meta-Analyses. Stata J. 2013, 13, 77–91. [Google Scholar] [CrossRef] [Green Version]
- Calişkan, M.K.; Sen, B.H. Endodontic treatment of teeth with apical periodontitis using calcium hydroxide: A long-term study. Endod. Dent. Traumatol. 1996, 12, 215–221. [Google Scholar] [CrossRef]
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 39. [Google Scholar] [CrossRef] [Green Version]
- Karygianni, L.; Krengel, M.; Winter, M.; Stampf, S.; Wrbas, K.T. Comparative assessment of the incidence of vertical root fractures between conventional versus surgical endodontic retreatment. Clin. Oral Investig. 2014, 18, 2015–2021. [Google Scholar] [CrossRef]
- Komabayashi, T.; Colmenar, D.; Cvach, N.; Bhat, A.; Primus, C.; Imai, Y. Comprehensive review of current endodontic sealers. Dent. Mater. J. 2020, 39, 703–720. [Google Scholar] [CrossRef] [Green Version]
- Benetti, F.; Queiroz, Í.O.d.A.; Cosme-Silva, L.; Conti, L.C.; Oliveira, S.H.P.; Cintra, L.T.A. Cytotoxicity, Biocompatibility and Biomineralization of a New Ready-for-Use Bioceramic Repair Material. Braz. Dent. J. 2019, 30, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Joober, R.; Schmitz, N.; Annable, L.; Boksa, P. Publication bias: What are the challenges and can they be overcome? J. Psychiatry Neurosci. JPN 2012, 37, 149–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.; Harbord, R. Funnel Plots in Meta-analysis. Stata J. 2004, 4, 127–141. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.; Smith, A.F. Trial sequential analysis: Adding a new dimension to meta-analysis. Anaesthesia 2020, 75, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, M.; Garner, P.; Donegan, S. Interpretation of subgroup analyses in systematic reviews: A tutorial. Clin. Epidemiol. Glob. Health 2019, 7, 192–198. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | K Words, Search Details | Records |
|---|---|---|
| PubMed | Search: surgical endodontic retreatment Sort by: Most Recent (“surgical procedures, operative” [MeSH Terms] OR (“surgical” [All Fields] AND “procedures” [All Fields] AND “operative” [All Fields]) OR “operative surgical procedures” [All Fields] OR “surgical” [All Fields] OR “surgically” [All Fields] OR “surgicals” [All Fields]) AND (“endodontal” [All Fields] OR “endodontic” [All Fields] OR “endodontical” [All Fields] OR “endodontically” [All Fields] OR “endodontics” [MeSH Terms] OR “endodontics” [All Fields]) AND (“retreat” [All Fields] OR “retreated” [All Fields] OR “retreating” [All Fields] OR “retreatment” [MeSH Terms] OR “retreatment” [All Fields] OR “retreatments” [All Fields] OR “retreats” [All Fields]) Translations surgical: “surgical procedures, operative” [MeSH Terms] OR (“surgical” [All Fields] AND “procedures” [All Fields] AND “operative” [All Fields]) OR “operative surgical procedures” [All Fields] OR “surgical” [All Fields] OR “surgically” [All Fields] OR “surgicals” [All Fields] endodontic: “endodontal” [All Fields] OR “endodontic” [All Fields] OR “endodontical” [All Fields] OR “endodontically” [All Fields] OR “endodontics” [MeSH Terms] OR “endodontics” [All Fields] retreatment: “retreat” [All Fields] OR “retreated” [All Fields] OR “retreating” [All Fields] OR “retreatment” [MeSH Terms] OR “retreatment” [All Fields] OR “retreatments” [All Fields] OR “retreats” [All Fields] | 567 |
| Search: endodontic retreatment Sort by: Most Recent (“endodontal” [All Fields] OR “endodontic” [All Fields] OR “endodontical” [All Fields] OR “endodontically” [All Fields] OR “endodontics” [MeSH Terms] OR “endodontics” [All Fields]) AND (“retreat” [All Fields] OR “retreated” [All Fields] OR “retreating” [All Fields] OR “retreatment” [MeSH Terms] OR “retreatment” [All Fields] OR “retreatments” [All Fields] OR “retreats” [All Fields]) Translations endodontic: “endodontal” [All Fields] OR “endodontic” [All Fields] OR “endodontical” [All Fields] OR “endodontically” [All Fields] OR “endodontics” [MeSH Terms] OR “endodontics” [All Fields] retreatment: “retreat” [All Fields] OR “retreated” [All Fields] OR “retreating” [All Fields] OR “retreatment” [MeSH Terms] OR “retreatment” [All Fields] OR “retreatments” [All Fields] OR “retreats” [All Fields] | 1698 | |
| Search: apicoectomy Sort by: Most Recent “apicoectomy” [MeSH Terms] OR “apicoectomy” [All Fields] OR “apicoectomies” [All Fields] Translations apicoectomy: “apicoectomy” [MeSH Terms] OR “apicoectomy” [All Fields] OR “apicoectomies” [All Fields] | 1755 | |
| SCOPUS | TITLE-ABS-KEY (surgical AND endodontic AND retreatment) | 293 |
| TITLE-ABS-KEY ((endodontic AND retreatment) OR apicoectomy) | 3012 | |
| Cochrane library | TITLE-ABS-KEY ((endodontic AND retreatment) OR apicoectomy) | 214 |
| (Surgical AND endodontic AND retreatment) | 29 | |
| Total | 7568 | |
| Summary of Data from Studies Treating Non-Surgical Endodontic Retreatment and Surgical Endodontic Retreatment [18,19,29,30,31,32,33] | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author, Date | Type of Study, Country | Type of Evaluation | N. Teeth, (Patients) * | Filling Material ** | Failures to Follow-Up (Year) | Failure Reason *** | |||||||||||||
| GP | MTA | GC | P | O | 1y | 2y | 3y | 4y | 8y | 1y | A | B | C | D | E | ||||
| Danin et al. (1996) [18] | Randomized Clinical Trial | Clinically, radiographically | 19 R | 19 (+RC) | 8/18 | 8 | |||||||||||||
| Sweden | 19 TC | 19 | 3/19 | 3 | |||||||||||||||
| Curtis et al. (2018) [29] | retrospective | CBCT | 68 R | 68 | 12/68 | 12 | |||||||||||||
| USA | 57 TC | 57 | 3/57 | 3 | |||||||||||||||
| Calişkan (2005) [30] | retrospective | radiographically | 79 R | 79 | 13/75 1 | 16/75 | 17/75 | 17 | |||||||||||
| Turkey | 11 TC | 6 | 5 | 2/11 | 3/11 | 4/11 | 4 | ||||||||||||
| Kvist and Reit (1999) [19] | Randomized Clinical Trial | clinically and radiographically | 48 R | 48 | 25/48 | 27/48 2 | 4 | 2 | |||||||||||
| Sweden | 47 TC | 47 | 16/47 | 21/47 | 8 | 2 | |||||||||||||
| Allen et al. (1989) [31] | retrospective | radiographically | 596 R | 596 | 48/315 | ||||||||||||||
| USA | 695 TC | 51/311 | |||||||||||||||||
| Riis et al. (2018) [32] | Randomized Clinical Trial | clinically and radiographically | 60 TC | 60 | 12/47 | 7 | 2 | 3 | |||||||||||
| Sweden; | 64 R | 64 (+RC) | 11/48 | 6 | 5 | ||||||||||||||
| Ercan et al. (2007) [33] | Prospective | clinically and radiographically | 59 R | 59 | 5/55 | 10/55 | 13/55 | 13 | |||||||||||
| Turkey | 11 TC | 11 | 0/9 | 1/9 | 1/9 | 1 | |||||||||||||
| Selection | Outcome | Loss to Follow-Up | Analysis | Score | ||
|---|---|---|---|---|---|---|
| Reference | Non-Response Rate | Representativeness of Sample to Target Population | Validity and Reliability of Outcome Measurement | Amount of Loss to Follow-Up | Appropriate Statistical Tests | |
| Danin et al. (1996) [18] | 3 | 4 | 5 | 3 | 3 | 18 |
| Curtis et al. (2018) [29] | 3 | 4 | 4 | 4 | 4 | 19 |
| Calişkan (2005) [30] | 4 | 4 | 4 | 3 | 4 | 19 |
| Kvist and Reit (1999) [19] | 3 | 4 | 5 | 4 | 4 | 20 |
| Allen et al. (1989) [31] | 3 | 5 | 4 | 3 | 3 | 18 |
| Riis et al. (2018) [32] | 5 | 5 | 5 | 5 | 5 | 25 |
| Ercan et al. (2007) [33] | 4 | 4 | 4 | 4 | 4 | 20 |
| Certainty Assessment | No of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Endodontic Retreatment | Apicoectomy | Relative (95% CI) | Absolute (95% CI) | |
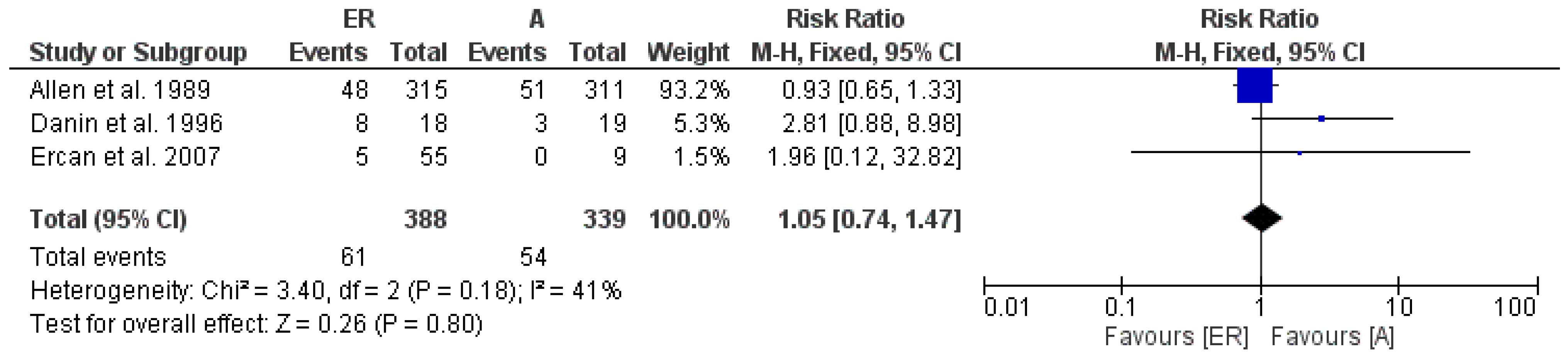
| ER vs. A 1-year follow-up | |||||||||||
| 3 | observational studies | not serious | not serious | not serious | not serious | none | 61/388 (15.7%) | 54/339 (15.9%) | RR 1.05 (0.74 to 1.47) | 8 more per 1.000 (from 41 fewer to 75 more) | ⨁⨁◯◯ Low |
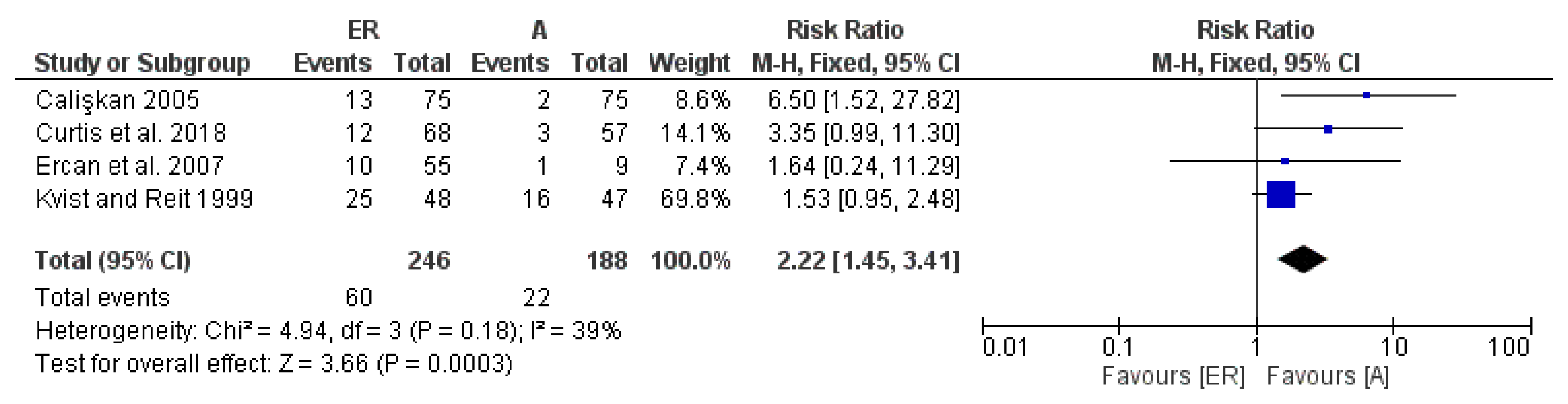
| ER vs. A 2-years follow-up | |||||||||||
| 4 | observational studies | not serious | not serious | not serious | not serious | strong association | 60/246 (24.4%) | 22/188 (11.7%) | RR 2.22 (1.45 to 3.41) | 143 more per 1.000 (from 53 more to 282 more) | ⨁⨁⨁◯ Moderate |
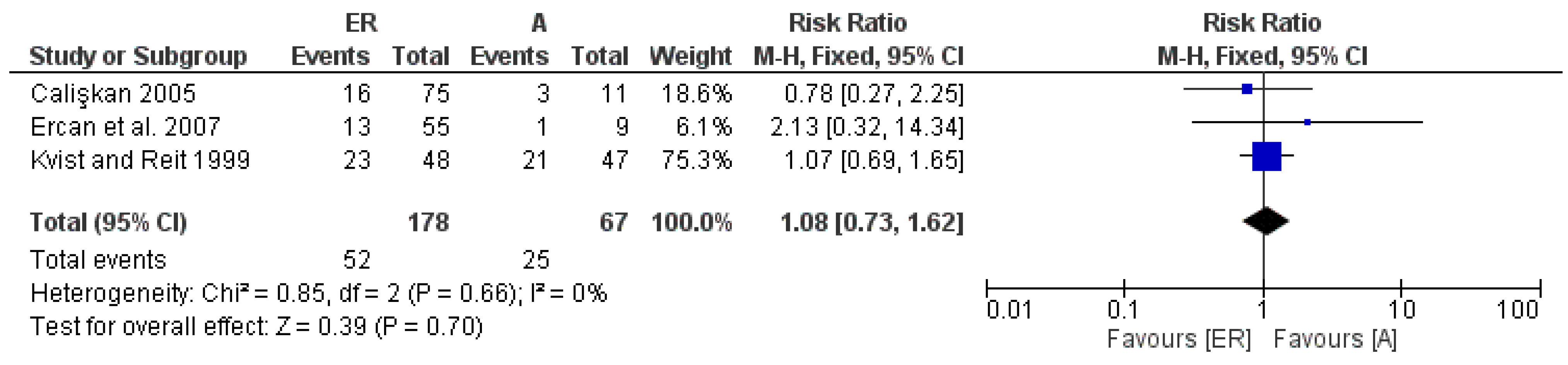
| ER vs. A 3–4-years follow-up | |||||||||||
| 3 | observational studies | not serious | not serious | not serious | not serious | none | 52/178 (29.2%) | 25/67 (37.3%) | RR 1.08 (0.73 to 1.62) | 30 more per 1.000 (from 101 fewer to 231 more) | ⨁⨁◯◯ Low |
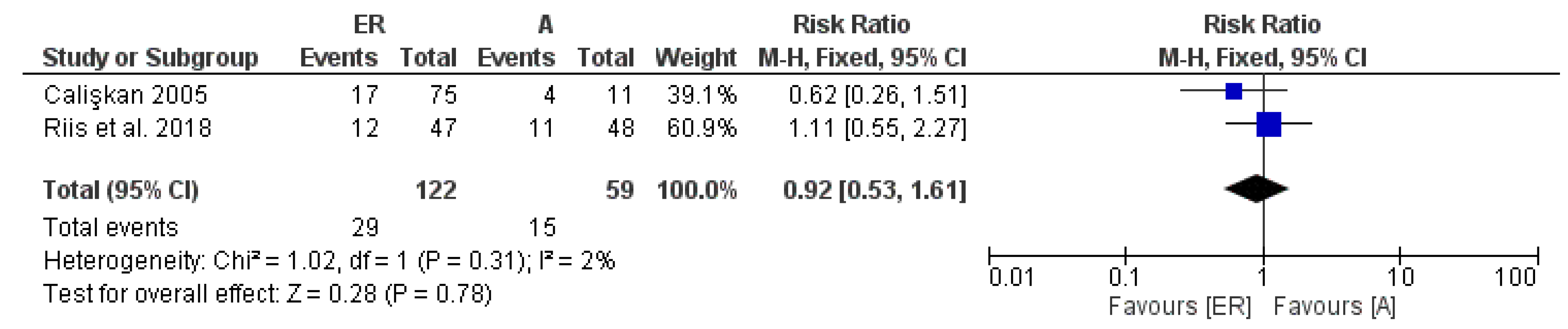
| ER vs. A 8–10-years follow-up | |||||||||||
| 2 | observational studies | not serious | not serious | not serious | not serious | none | 29/122 (23.8%) | 15/59 (25.4%) | RR 0.92 (0.53 to 1.61) | 20 fewer per 1.000 (from 119 fewer to 155 more) | ⨁⨁◯◯ Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dioguardi, M.; Stellacci, C.; La Femina, L.; Spirito, F.; Sovereto, D.; Laneve, E.; Manfredonia, M.F.; D’Alessandro, A.; Ballini, A.; Cantore, S.; et al. Comparison of Endodontic Failures between Nonsurgical Retreatment and Endodontic Surgery: Systematic Review and Meta-Analysis with Trial Sequential Analysis. Medicina 2022, 58, 894. https://doi.org/10.3390/medicina58070894
Dioguardi M, Stellacci C, La Femina L, Spirito F, Sovereto D, Laneve E, Manfredonia MF, D’Alessandro A, Ballini A, Cantore S, et al. Comparison of Endodontic Failures between Nonsurgical Retreatment and Endodontic Surgery: Systematic Review and Meta-Analysis with Trial Sequential Analysis. Medicina. 2022; 58(7):894. https://doi.org/10.3390/medicina58070894
Chicago/Turabian StyleDioguardi, Mario, Camilla Stellacci, Lucia La Femina, Francesca Spirito, Diego Sovereto, Enrica Laneve, Massimo Francesco Manfredonia, Alfonso D’Alessandro, Andrea Ballini, Stefania Cantore, and et al. 2022. "Comparison of Endodontic Failures between Nonsurgical Retreatment and Endodontic Surgery: Systematic Review and Meta-Analysis with Trial Sequential Analysis" Medicina 58, no. 7: 894. https://doi.org/10.3390/medicina58070894