
Level of Anxiety Caused by the Coronavirus (COVID-19) Pandemic among Dentists in Poland

 , and
, and
Abstract
:1. Introduction
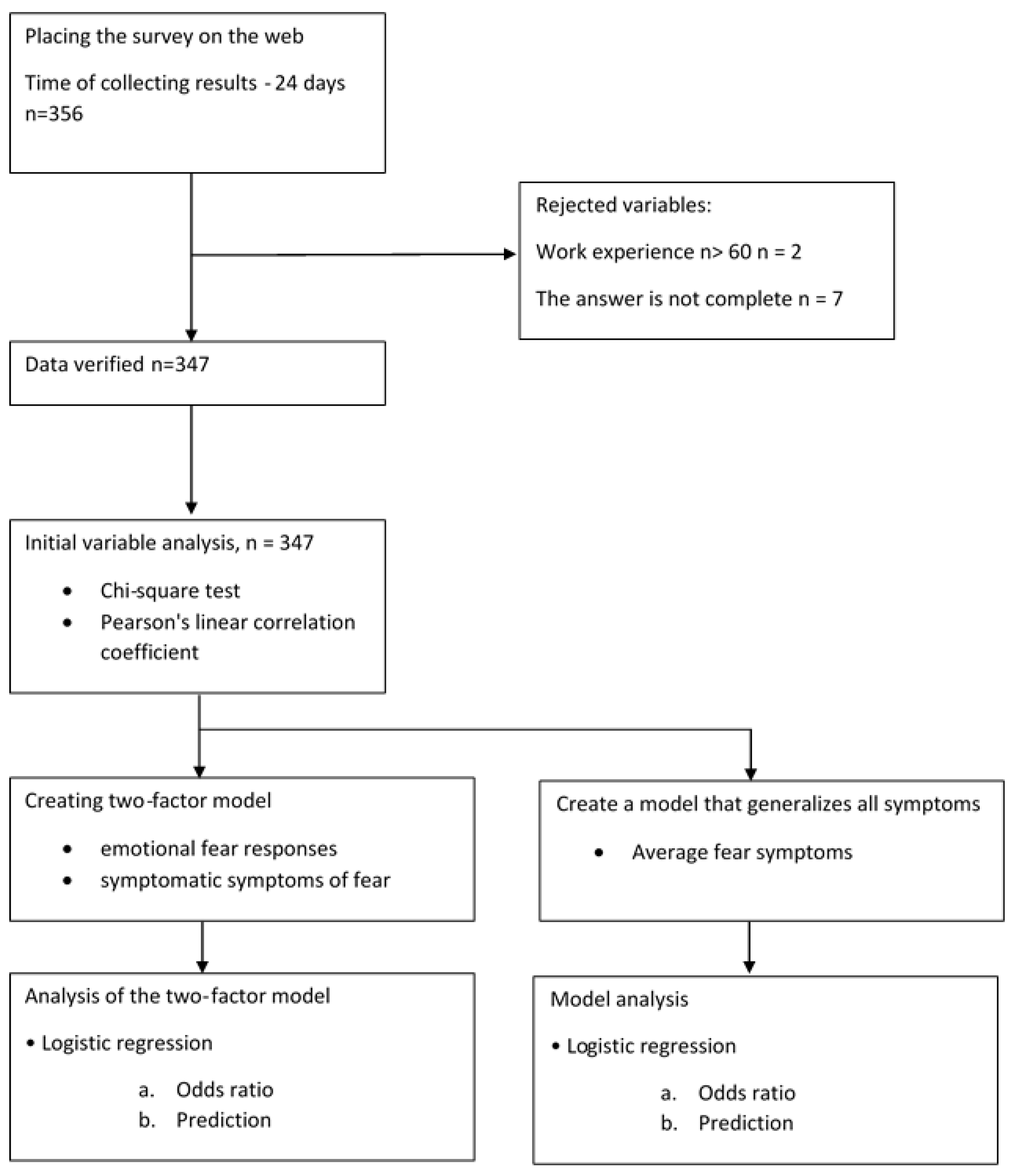
2. Materials and Methods
2.1. Study Design, Setting, Participants
2.2. Variables
- I am afraid of coronavirus (COVID-19) more than anything else.
- Thinking about coronavirus (COVID-19) makes me uncomfortable.
- My palms sweat when I think about coronavirus.
- I am worried that I will die from the coronavirus infection.
- When I hear about coronavirus (COVID-19) in the media and on the Internet, I get nervous and worried.
- I cannot sleep because of coronavirus.
- My heart starts to beat faster when I think about coronavirus.
2.3. Study Size
- Confidence level (α) 95%
- Sample size (n) 1000
- Proportion percentage (p) 50
- Population size (N) 37,773
2.4. Statistical Methods
2.5. Quantitative Variables
2.6. Bias
3. Results
Participants
4. Discussion
The Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lancet, T. COVID-19: Fighting panic with information. Lancet 2020, 395, 537. [Google Scholar] [CrossRef] [Green Version]
- Gamio, L. The Workers Who Face the Greatest Coronavirus Risk—The New York Times. Available online: https://www.nytimes.com/interactive/2020/03/15/business/economy/coronavirus-worker-risk.html (accessed on 16 December 2021).
- Karwowska, A. Coronavirus Has Restricted Our Access to Medical Care. Here Is the Breakdown of How Hospitals, Clinics and Private Practice Now Operate. Available online: https://wyborcza.pl/7,173236,25964988,coronavirus-has-restricted-our-access-to-medical-care-here.html (accessed on 16 December 2021).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 16 December 2021).
- Lin, C.-Y. Social reaction toward the 2019 novel coronavirus (COVID-19). Soc. Health Behav. 2020, 3, 1. [Google Scholar] [CrossRef]
- Bhuiyan, A.K.M.I.; Sakib, N.; Pakpour, A.H.; Griffiths, M.D.; Mamun, M.A. COVID-19-Related Suicides in Bangladesh Due to Lockdown and Economic Factors: Case Study Evidence from Media Reports. Int. J. Ment. Health Addict. 2020, 19, 2110–2115. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Pappas, G.; Kiriaze, I.; Giannakis, P.; Falagas, M. Psychosocial consequences of infectious diseases. Clin. Microbiol. Infect. 2009, 15, 743–747. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2019; pp. 23–39. [Google Scholar]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakib, N.; Bhuiyan, A.K.M.I.; Hossain, S.; Al Mamun, F.; Hosen, I.; Abdullah, A.H.; Sarker, A.; Mohiuddin, M.S.; Rayhan, I.; Hossain, M.; et al. Psychometric Validation of the Bangla Fear of COVID-19 Scale: Confirmatory Factor Analysis and Rasch Analysis. Int. J. Ment. Health Addict. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the Fear of COVID-19 Scale: Its Association with Psychological Distress and Life Satisfaction in Turkey. Int. J. Ment. Health Addict. 2020, 19, 1980–1988. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 4, 1–10. [Google Scholar] [CrossRef]
- Polish Supreme Medical Council. Statistical Information of the Polish Supreme Medical Council, on 3 July 2020. Available online: https://nil.org.pl/rejestry/centralny-rejestr-lekarzy/informacje-statystyczne (accessed on 16 December 2021).
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical Dental Care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef]
- Ferrara, M.; Langiano, E.; Falese, L.; De Marco, A.; De Vito, E. Quality of Life and Psychosocial Impacts of the Different Restrictive Measures during One Year into the COVID-19 Pandemic on Patients with Cancer in Italy: An Ecological Study. Int. J. Environ. Res. Public Health 2021, 18, 7161. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, Q.K.; Jafree, S.R.; Mukhtar, S.; Fischer, F. Social Media Use, Self-Efficacy, Perceived Threat, and Preventive Behavior in Times of COVID-19: Results of a Cross-Sectional Study in Pakistan. Front. Psychol. 2021, 12, 2354. [Google Scholar] [CrossRef] [PubMed]
- De Kock, J.H.; Latham, H.A.; Leslie, S.J.; Grindle, M.; Munoz, S.A.; Ellis, L.; Polson, R.; O’Malley, C.M. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: Implications for supporting psychological well-being. BMC Public Health 2021, 21, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Jerusalem, M.; Schwarzer, R. Self-efficacy as a resource factor in stress appraisal processes. In Self-Efficacy: Thought Control of Action; Hemisphere Publishing Corp.: Washington, DC, USA, 1992; pp. 195–213. [Google Scholar]



{kind=link}
{kind=link}
| Demographics | Group | n (%) |
|---|---|---|
| Gender | Female | 245 (70.6%) |
| Male | 102 (29.4%) | |
| Relationship status | Single | 15 (4.3%) |
| Divorced or widowed | 52 (15.0%) | |
| In a relationship, living apart together | 15 (4.3%) | |
| In a relationship, living together | 38 (11.0%) | |
| Having children | No | 145 (41.8%) |
| Yes | 202 (58.2%) | |
| Elderly care | No | 297 (85.6%) |
| Yes | 50 (14.4%) |
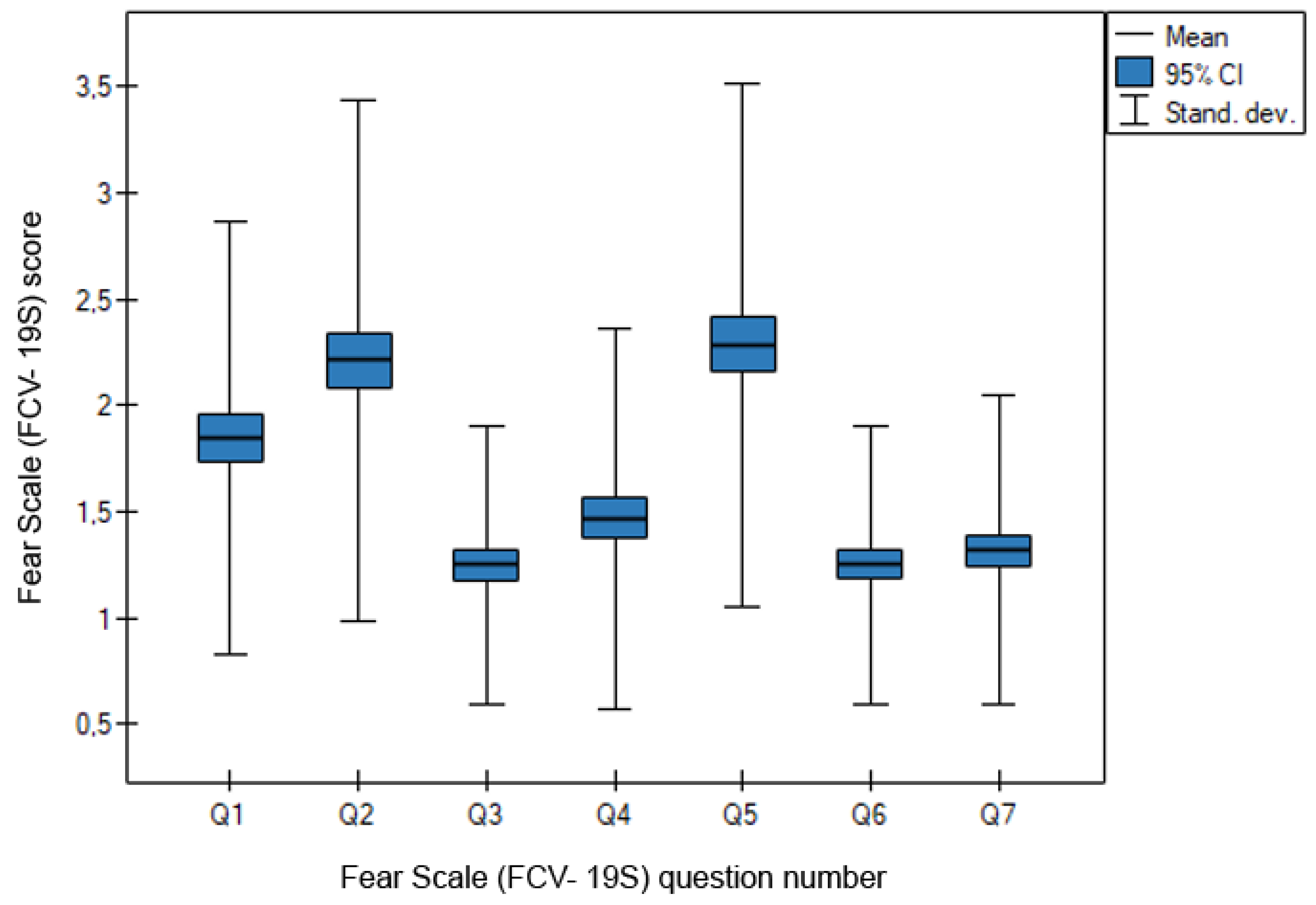
| Questionnaire Item | Group | Frequency | Percent | Mean | Std. Dev. |
|---|---|---|---|---|---|
| I am most afraid of COVID-19. | 1 | 173 | 49.9 | 1.85 | 1.016 |
| 2 | 85 | 24.5 | |||
| 3 | 63 | 18.2 | |||
| 4 | 21 | 6.1 | |||
| 5 | 5 | 1.4 | |||
| It makes me uncomfortable to think about COVID-19. | 1 | 133 | 38.3 | 2.22 | 1.224 |
| 2 | 85 | 24.5 | |||
| 3 | 68 | 19.6 | |||
| 4 | 43 | 12.4 | |||
| 5 | 18 | 5.2 | |||
| My hands become clammy when I think about COVID-19. | 1 | 290 | 83.6 | 1.25 | 0.652 |
| 2 | 36 | 10.4 | |||
| 3 | 14 | 4.0 | |||
| 4 | 5 | 1.4 | |||
| 5 | 2 | 0.6 | |||
| I am afraid of losing my life because of COVID-19. | 1 | 250 | 72.0 | 1.47 | 0.897 |
| 2 | 55 | 15.9 | |||
| 3 | 24 | 6.9 | |||
| 4 | 12 | 3.5 | |||
| 5 | 6 | 1.7 | |||
| When watching news and stories about COVID-19 on social media, I become nervous or anxious. | 1 | 124 | 35.7 | 2.29 | 1.229 |
| 2 | 87 | 25.1 | |||
| 3 | 64 | 18.4 | |||
| 4 | 57 | 16.4 | |||
| 5 | 15 | 4.3 | |||
| I cannot sleep because I’m worrying about getting COVID-19. | 1 | 289 | 83.3 | 1.25 | 0.653 |
| 2 | 37 | 10.7 | |||
| 3 | 14 | 4.0 | |||
| 4 | 5 | 1.4 | |||
| 5 | 2 | 0.6 | |||
| My heart races or palpitates when I think about getting COVID-19. | 1 | 276 | 79.5 | 1.32 | 0.728 |
| 2 | 44 | 12.7 | |||
| 3 | 18 | 5.2 | |||
| 4 | 6 | 1.7 | |||
| 5 | 3 | 0.9 |
| Level of Fear | Percent | Mean |
|---|---|---|
| 1—Fear low | 63.2 | 1.66 |
| 2 | 17.7 | |
| 3 | 10.9 | |
| 4 | 6.1 | |
| 5—Fear extremely high | 2.1 |
| Questionnaire Item | Gender | Work Experience | Relationship Status | Having Children | Eldery Care |
|---|---|---|---|---|---|
| I am most afraid of COVID-19. | 0.28 | Pearson Correlation R = 0.12 Sig. = 0.03 | 0.42 | 0.00 | 0.01 |
| It makes me uncomfortable to think about COVID-19. | 0.08 | Pearson Correlation R = 0.05 Sig. = 0.31 | 0.21 | 0.00 | 0.16 |
| My hands become clammy when I think about COVID-19. | 0.46 | Pearson Correlation R = 0.01 Sig. = 0.83 | 0.58 | 0.41 | 0.00 |
| I am afraid of losing my life because of COVID-19. | 0.18 | Pearson Correlation R = 0.12 Sig. = 0.03 | 0.38 | 0.02 | 0.26 |
| When watching news and stories about COVID-19 on social media, I become nervous or anxious. | 0.69 | Pearson Correlation R = 0.10 Sig. = 0.08 | 0.36 | 0.00 | 0.00 |
| I cannot sleep because I’m worrying about getting COVID-19. | 0.28 | Pearson Correlation R = 0.12 Sig. = 0.03 | 0.42 | 0.00 | 0.01 |
| My heart races or palpitates when I think about getting COVID-19. | 0.08 | Pearson Correlation R = 0.05 Sig. = 0.31 | 0.21 | 0.00 | 0.16 |
| b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI | |
|---|---|---|---|---|---|---|---|---|---|
| Intercept | −2.36 | 0.45 | −3.24 | −1.47 | 27.32 | <0.001 | 0.09 | 0.04 | 0.23 |
| Having children | 0.88 | 0.26 | 0.38 | 1.39 | 11.65 | <0.001 | 2.42 | 1.46 | 4.02 |
| b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI | |
|---|---|---|---|---|---|---|---|---|---|
| Intercept | −2.20 | 0.39 | −2.97 | −1.44 | 32.02 | <0.001 | 0.11 | 0.05 | 0.24 |
| Person lives with the elderly | 1.10 | 0.31 | 0.49 | 1.72 | 12.42 | <0.001 | 3.01 | 1.63 | 5.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusyan, E.; Mielczarek, A.; Bogusławska-Kapała, A.; Adamczyk, K.; Piec, R.; Szykuła-Piec, B. Level of Anxiety Caused by the Coronavirus (COVID-19) Pandemic among Dentists in Poland. Medicina 2022, 58, 415. https://doi.org/10.3390/medicina58030415
Rusyan E, Mielczarek A, Bogusławska-Kapała A, Adamczyk K, Piec R, Szykuła-Piec B. Level of Anxiety Caused by the Coronavirus (COVID-19) Pandemic among Dentists in Poland. Medicina. 2022; 58(3):415. https://doi.org/10.3390/medicina58030415
Chicago/Turabian StyleRusyan, Ewa, Agnieszka Mielczarek, Agnieszka Bogusławska-Kapała, Kamil Adamczyk, Robert Piec, and Barbara Szykuła-Piec. 2022. "Level of Anxiety Caused by the Coronavirus (COVID-19) Pandemic among Dentists in Poland" Medicina 58, no. 3: 415. https://doi.org/10.3390/medicina58030415