
The Attitude of Patients from a Romanian Tertiary Cardiology Center Regarding Participation in Biomarker-Based Clinical Trials

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
3.1. Respondent Characteristics
3.2. Attitudes and Expectations
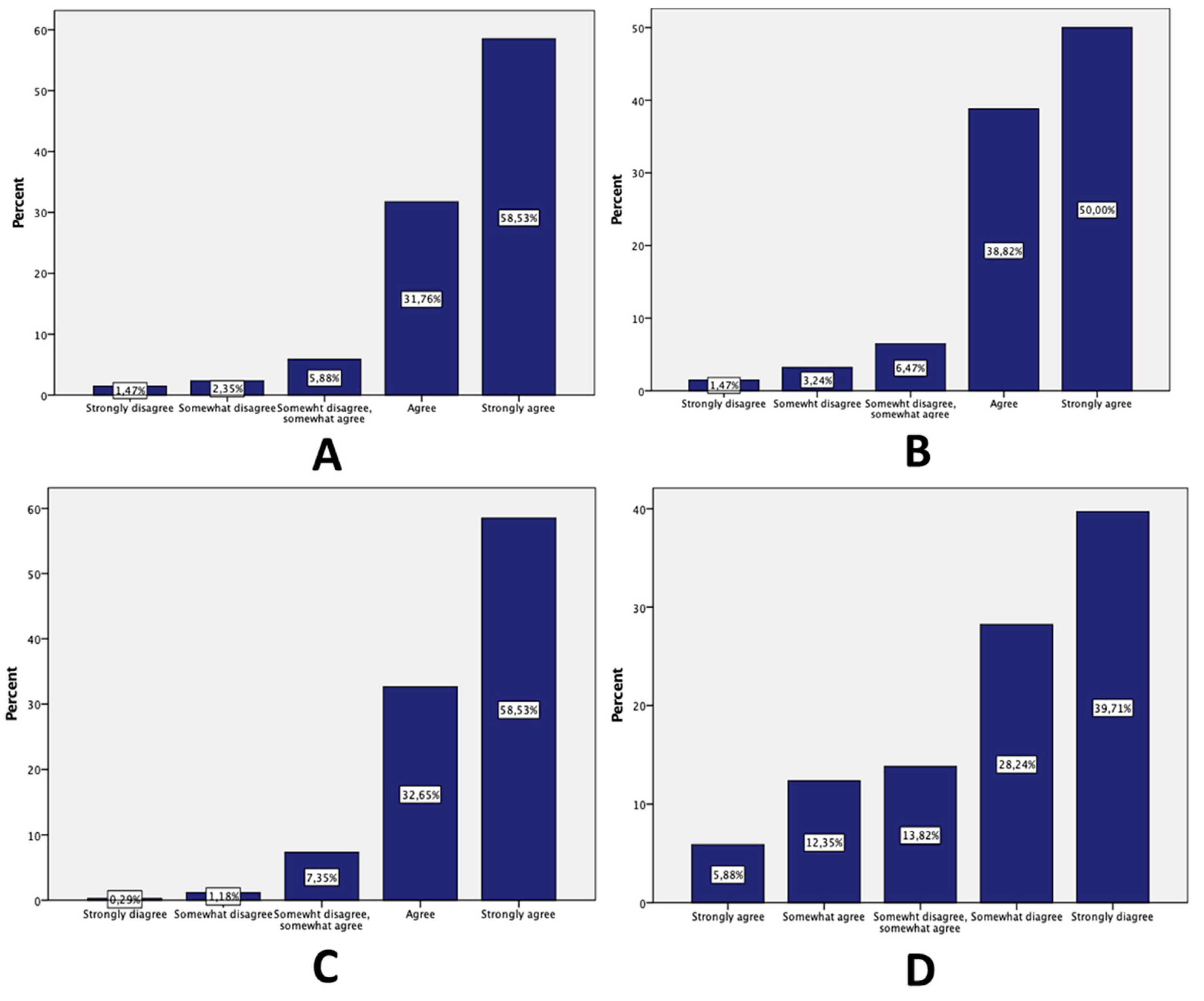
3.3. Trust in Physicians
3.4. Respondent Characteristics, Questionnaire Resolutions and Significant Associations
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sand, K.; Kaasa, S.; Loge, J.H. The understanding of informed consent information-definitions and measurements in empirical studies. AJOB Prim. Res. 2010, 30, 4–24. [Google Scholar] [CrossRef]
- Whiddett, R.; Hunter, I.; Engelbrecht, J.; Handy, J. Patients’ attitudes towards sharing their health information. Int. J. Med. Inform. 2006, 75, 530–541. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J.; Pritts, J.L.; Neblo, M.A.; Kalarickal, R.J.; Creswell, J.W.; Hayward, R.A. Patients, privacy and trust: Patients’ willingness to allow researchers to access their medical records. Soc. Sci. Med. 2007, 64, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Warner, T.D.; Weil, C.J.; Andry, C.; Degenholtz, H.B.; Parker, L.; Carithers, L.J.; Feige, M.; Wendler, D.; Pentz, R.D. Broad consent for research on biospecimens: The views of actual donors at four U.S. medical centers. J. Empir. Res. Hum. Res. Ethics 2018, 13, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, E.; Loomes, M.; Butow, P.; Boyle, F.M. A systematic literature review of attitudes towards secondary use and sharing of health administrative and clinical trial data: A focus on consent. Syst. Rev. 2021, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Mihaela Micheu, M.; Udrea, O.-M.; Octavia Popa, M.; Rusu, I.; Gheorghe-Fronea, O.; Scafa-Udriste, A.; Dorobantu, M. The attitude of patients from a Romanian tertiary cardiology center as regards participation in biomarker-based clinical trials—Survey methodology. J. Med. Life 2018, 11, 320. [Google Scholar] [CrossRef] [PubMed]
- Blanchette, P.S.; Spreafico, A.; Miller, F.A.; Chan, K.; Bytautas, J.; Kang, S.; Bedard, P.L.; Eisen, A.; Potanina, L.; Holland, J.; et al. Genomic testing in cancer: Patient knowledge, attitudes, and expectations. Cancer 2014, 120, 3066–3073. [Google Scholar] [CrossRef] [PubMed]
- Bossert, S.; Kahrass, H.; Heinemeyer, U.; Prokein, J.; Strech, D. Participatory improvement of a template for informed consent documents in biobank research—Study results and methodological reflections. BMC Med. Ethics 2017, 18, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossert, S.; Kahrass, H.; Strech, D. The public’s awareness of and attitude toward research biobanks—A regional German survey. Front. Genet. 2018, 9, 190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lhousni, S.; Daoudi, F.; Belmokhtar, I.; Belmokhtar, K.Y.; Abda, N.; Boulouiz, R.; Tajir, M.; Bellaoui, M.; Ouarzane, M. Patients’ knowledge and attitude toward biobanks in eastern Morocco. Biopreserv. Biobank. 2020, 18, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Mezinska, S.; Kaleja, J.; Mileiko, I.; Santare, D.; Rovite, V.; Tzivian, L. Public awareness of and attitudes towards research biobanks in Latvia. BMC Med. Ethics 2020, 21, 65. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, K.D.; Boenink, M. Subtle voices, distant futures: A critical look at conditions for patient involvement in Alzheimer’s biomarker research and beyond. J. Responsible Innov. 2020, 7, 170–192. [Google Scholar] [CrossRef] [Green Version]
- Buck, D.; Gamble, C.; Dudley, L.; Preston, J.; Hanley, B.; Williamson, P.R.; Young, B.; Allam, A.; Bell, P.; Formstone, N.; et al. From plans to actions in patient and public involvement: Qualitative study of documented plans and the accounts of researchers and patients sampled from a cohort of clinical trials. BMJ Open 2014, 4, e006400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belfrage, S.; Lynöe, N.; Helgesson, G. Willingness to share yet maintain influence: A cross-sectional study on attitudes in Sweden to the use of electronic health data. Public Health Ethics 2021, 14, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Spencer, K.; Sanders, C.; Whitley, E.A.; Lund, D.; Kaye, J.; Dixon, W.G. Patient perspectives on sharing anonymized personal health data using a digital system for dynamic consent and research feedback: A qualitative study. J. Med. Internet Res. 2016, 18, e5011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopper, K.D.; TenHave, T.R.; Hartzel, J. Informed consent forms for clinical and research imaging procedures: How much do patients understand? Am. J. Roentgenol. 1995, 164, 493–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, M.V.; Parker, R.M.; Baker, D.W.; Parikh, N.S.; Pitkin, K.; Coates, W.C.; Nurss, J.R. Inadequate functional health literacy among patients at two public hospitals. JAMA J. Am. Med. Assoc. 1995, 274, 1677–1682. [Google Scholar] [CrossRef]
- Davis, T.C.; Holcombe, R.F.; Berkel, H.J.; Pramanik, S.; Divers, S.G. Informed consent for clinical trials: A comparative study of standard versus simplified forms. J. Natl. Cancer Inst. 1998, 90, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.C.H.; Pu, C.; Chou, Y.J.; Huang, N. Public trust in physicians—Health care commodification as a possible deteriorating factor: Cross-sectional analysis of 23 countries. INQUIRY: J. Health Care Organ. Provis. Financing 2018, 55, 0046958018759174. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Number (Percentage) of Patients |
|---|---|
| Age (years) | 59.68 ± 13.15 (19–92) |
| Sex, female, n (%) | 101 (29.6%) |
| Community size | |
| Urban area | 248 (72.7%) |
| Rural area | 90 (26.4%) |
| Education | |
| Graduate degree | 94 (27.6%) |
| High school graduate | 85 (24.95) |
| Some college | 108 (31.7%) |
| 4-year degree | 52 (15.2%) |
| Ethnicity | |
| European | 314 (92.1%) |
| Indo-European | 10 (2.9%) |
| Indian | 1 (0.3%) |
| Mongol | 1 (0.3%) |
| Married/partner | 250 (73.3%) |
| Religion | |
| Orthodox | 308 (90.3%) |
| Catholic | 3 (0.9%) |
| Hindus | 1 (0.3%) |
| Pentecostal | 3 (0.9%) |
| Baptist | 1 (0.3%) |
| Muslim | 1 (0.3%) |
| Atheist | 5 (1.5%) |
| Chronic disease | |
| Yes, cardiovascular | 127 (37.35) |
| Yes, other | 8 (2.35%) |
| No | 205 (60.29%) |
| Compliance to treatment | |
| Yes | 61 (17.9%) |
| No | 219 (64.4%) |
| Not the case | 60 (17.65%) |
| Reasons | Number (Percentage) of Patients |
|---|---|
| To help other patients with the same disease as me | 72 (21.1%) |
| To help other members of my family that could have the same disease | 29 (8.5%) |
| For myself-maybe the information obtained would be helpful | 56 (16.4%) |
| For contributing to the enrichment of the disease’s knowledge, even if would not be direct beneficiary | 32 (9.4%) |
| For contributing to science in general | 8 (26.1%) |
| I would not participate | 52 (15.2%) |
| 1&2 | 4 (1.2) |
| 1&5 | 3 (0.9%) |
| 3&4 | 1 (0.3%) |
| 3&5 | 1 (0.3%) |
| 4&5 | 1 (0.3%) |
| Information | Number (Percentage) of Patients |
|---|---|
| The possibility to find out the results of the study and their impact on my health | 173 (35.16%) |
| The non-invasive nature of sampling | 23 (4.67%) |
| Material compensations | 28(5.69%) |
| The knowing of the biological sample usage | 18 (3.66%) |
| The exposure of the advantages if enrolling | 17 (3.45%) |
| The certainty that participation in the study would ameliorate my health status | 75 (15.24%) |
| The certainty that samples will not be used for purposes other than those mentioned | 31 (6.3%) |
| The certainty that my rights would be respected throughout the study | 52 (10.57%) |
| The possibility to retire from the study at any time without affecting the quality of the medical treatment | 42 (8.54%) |
| Others | 3(0.61%) |
| Nothing | 30 (6.1%) |
| Aspects | Number (Percentage) of Patients |
|---|---|
| Clear exposure of the possible risks | 170 (37.78%) |
| Explanation of study purpose in accessible terms | 89 (19.78%) |
| Drawings, schemas, tables with relevant data | 11 (2.44%) |
| Statistics on biomarkers’ importance | 39 (8.67%) |
| Direct communication with the research team | 107 (23.78%) |
| Others | 1 (0.22%) |
| Nothing | 33 (7.33%) |
| Aspects | Number (Percentage) of Patients |
|---|---|
| Long and complicated phrases/the lack of accessible terms | 214 (46.22%) |
| Insufficient medical data | 78 (16.85%) |
| Too detailed medical information | 60 (12.96%) |
| Insufficient data about personal rights | 110 (23.76%) |
| Others | 1 (0.21%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusu, I.; Popa-Fotea, N.-M.; Stanculescu, M.O.; Rusu, D.; Dumitru, A.; Scafa-Udriste, A.; Udrea, O.-M.; Micheu, M.M. The Attitude of Patients from a Romanian Tertiary Cardiology Center Regarding Participation in Biomarker-Based Clinical Trials. Medicina 2021, 57, 1180. https://doi.org/10.3390/medicina57111180
Rusu I, Popa-Fotea N-M, Stanculescu MO, Rusu D, Dumitru A, Scafa-Udriste A, Udrea O-M, Micheu MM. The Attitude of Patients from a Romanian Tertiary Cardiology Center Regarding Participation in Biomarker-Based Clinical Trials. Medicina. 2021; 57(11):1180. https://doi.org/10.3390/medicina57111180
Chicago/Turabian StyleRusu, Iulia, Nicoleta-Monica Popa-Fotea, Mihaela Octavia Stanculescu, Diana Rusu, Alexandra Dumitru, Alexandru Scafa-Udriste, Oana-Maria Udrea, and Miruna Mihaela Micheu. 2021. "The Attitude of Patients from a Romanian Tertiary Cardiology Center Regarding Participation in Biomarker-Based Clinical Trials" Medicina 57, no. 11: 1180. https://doi.org/10.3390/medicina57111180