
Phytotherapy as Multi-Hit Therapy to Confront the Multiple Pathophysiology in Non-Alcoholic Fatty Liver Disease: A Systematic Review of Experimental Interventions


Abstract
:1. Introduction
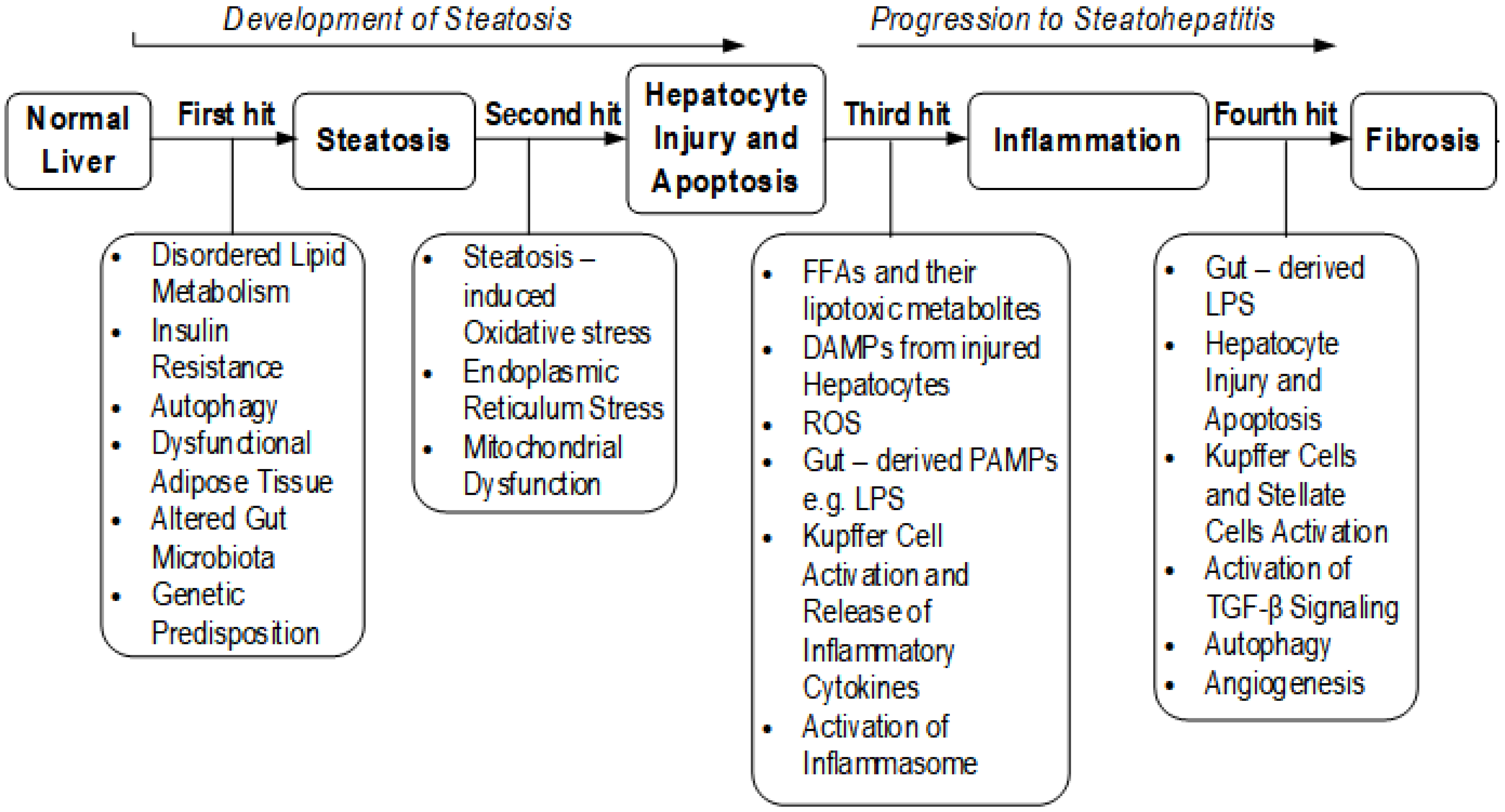
1.1. The Hits in NAFLD?
1.2. Biomarkers and Criteria Used in the Diagnosis of NAFLD
1.3. Phytotherapy
1.4. Rationale and Objectives
2. Methods
2.1. Eligibility Criteria
- (a)
- Articles that were published in English,
- (b)
- Animal studies,
- (c)
- NAFLD model induced by diet
- (d)
- Studies assessing the effectiveness of plant-derived extracts or fractions or polyherbal mixtures in the treatment of NAFLD
- (e)
- Studies evaluating at least disordered lipid metabolism, insulin resistance/T2DM, and histologically confirmed steatosis
- (f)
- Studies with one or more of the following: oxidative stress, inflammation, hepatocyte injury, obesity, fibrosis, and cardiometabolic risks (in addition to the pathological conditions in (e)).
- (a)
- Studies conducted in vitro,
- (b)
- Human studies
- (c)
- Reviews,
- (d)
- NAFLD not induced by diet
- (e)
- Studies involving the use of isolated or single phyto-compound to treat NAFLD
- (f)
- Studies not meeting the inclusion criteria stated above.
2.2. Information Sources
2.3. Search Strategy
2.4. Study Selection
- (a)
- Animal models,
- (b)
- Assessments of the effectiveness of plant extracts in NAFLD model
- (c)
- Full-text articles in English
- (d)
- Evaluation of disordered lipid metabolism, steatosis, insulin resistance (HOMA-IR), with one or more of the following: oxidative stress, inflammation, hepatocyte injury, obesity, fibrosis, and cardiometabolic risks.
2.5. Data Collection
3. Results
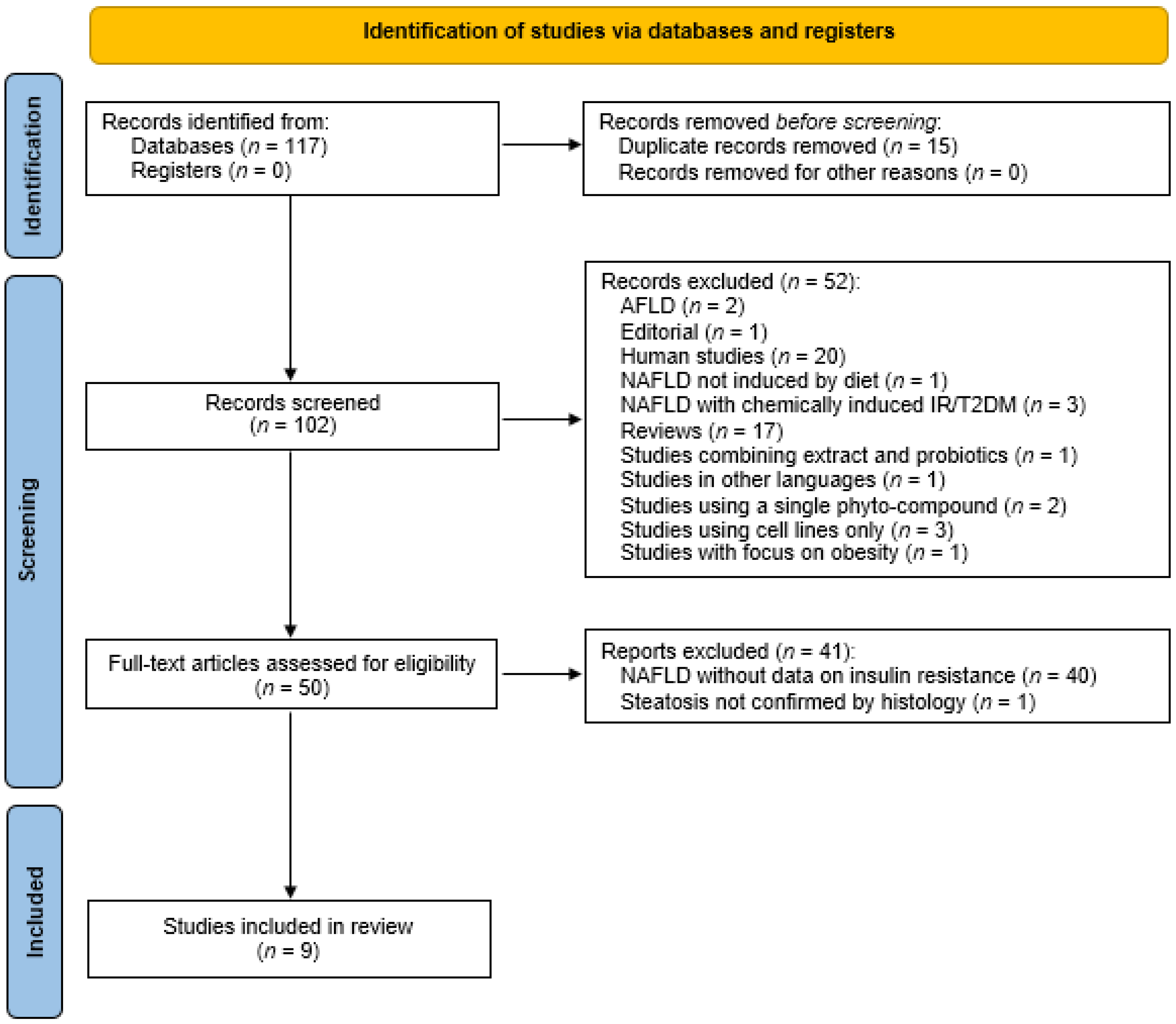
3.1. Study Selection
3.2. Study Characteristics
4. Discussion
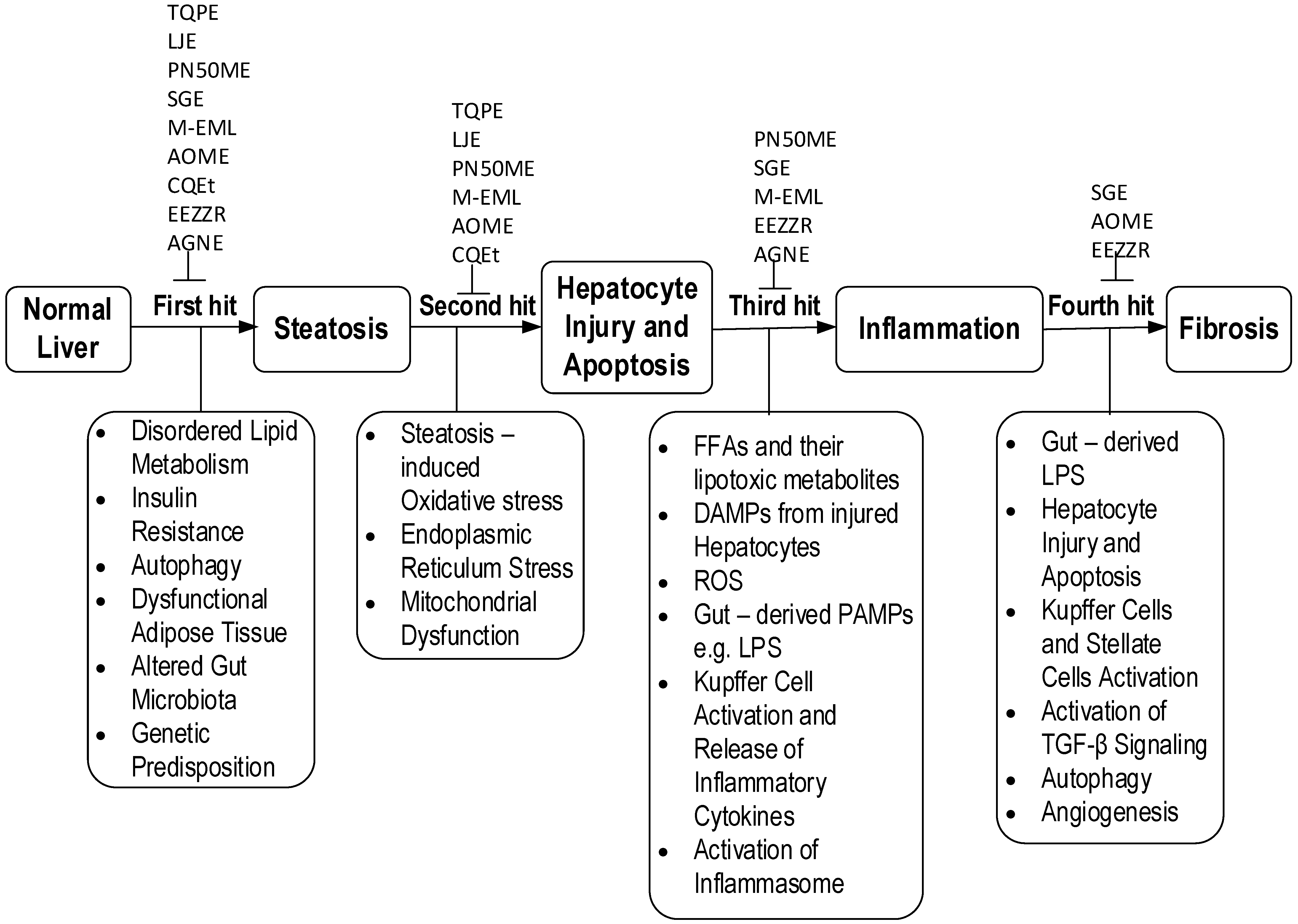
4.1. Trapa quadrispinosa Pericarp Extract (TQPE) Exerts Multiple Therapeutic Hits on NAFLD
4.2. Leonurus japonicus Ethanol Extract (LJE) and Its Multiple Hit Effects on NAFLD
4.3. Multiple Effects of Phyllanthus niruri 50% Methanol in Water Extract (PN50ME) on NAFLD
4.4. Multiple Therapeutic Actions of Combinations of Salvia miltiorrhiza Root and Fruit of Gardenia jasminoides Extracts (SGE)
4.5. Multiple Therapeutic Effects of Methanol Extract from Erica multiflora Leaf (M-EML) on NAFLD
4.6. Alisma orientalis Methanolic Extract (AOME) Alleviate Hyperlipidemia, Hepatic Steatosis, Insulin Resistance, Oxidative Stress, Hepatocyte Injury, and Obesity Associated with NAFLD
4.7. Cissus quadrangularis Stem Extract (CQEt)
4.8. Ethanol Extract of Zingiber zerumbet Rhizome (EEZZR) Attenuates NAFLD by Multiple Mechanism
4.9. Angelica gigas Nakai Extract (AGNE) Alleviate Dyslipidemia, Hepatic Steatosis, Insulin Resistance and Inflammation Related to NAFLD
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petroni, M.L.; Brodosi, L.; Bugianesi, E.; Marchesini, G. Management of non-alcoholic fatty liver disease. BMJ 2021, 372, m4747. [Google Scholar] [CrossRef]
- Basaranoglu, M.; Neuschwander-Tetri, B.A. Nonalcoholic fatty liver disease: Clinical features and pathogenesis. Gastroenterol. Hepatol. 2006, 2, 282–291. [Google Scholar]
- Ludwig, J.; Viggiano, T.R.; McGill, D.B.; Oh, B.J. Nonalcoholic steatohepatitis: Mayo clinic experiences with a hitherto unnamed disease. Mayo Clin. Proc. 1980, 55, 434–438. [Google Scholar]
- Petta, S.; Gastaldelli, A.; Rebelos, E.; Bugianesi, E.; Messa, P.; Miele, L.; Svegliati-Baroni, G.; Valenti, L.; Bonino, F. Pathophysiology of non alcoholic fatty liver disease. Int. J. Mol. Sci. 2016, 17, 2082. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J. MAFLD: A consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun, W.V.; Dufour, J.-F.; Schattenberg, J.M. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Marchesini, G.; Pinto-Cortez, H.; Petta, S. Epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: Implications for liver transplantation. Transplantation 2019, 103, 22–27. [Google Scholar] [CrossRef]
- Velázquez, K.T.; Enos, R.T.; Bader, J.E.; Sougiannis, A.T.; Carson, M.S.; Chatzistamou, I.; Carson, J.A.; Nagarkatti, P.S.; Nagarkatti, M.; Murphy, E.A. Prolonged high-fat-diet feeding promotes non-alcoholic fatty liver disease and alters gut microbiota in mice. World J. Hepatol. 2019, 11, 619–637. [Google Scholar] [CrossRef]
- Birkenfeld, A.L.; Shulman, G.I. Nonalcoholic fatty liver disease, hepatic insulin resistance, and type 2 diabetes. Hepatology 2014, 59, 713–723. [Google Scholar] [CrossRef] [Green Version]
- Dyson, J.; Day, C. Treatment of non-alcoholic fatty liver disease. Dig. Dis. 2014, 32, 597–604. [Google Scholar] [CrossRef]
- Day, C.P.; James, O.F. Steatohepatitis: A tale of two ‘‘hits’’? Gastroenterology 1998, 114, 842–845. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Evolution of inflammation in nonalcoholic fatty liver disease: The multiple parallel hits hypothesis. Hepatology 2010, 52, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Baker, R.D.; Bhatia, T.; Zhu, L.; Baker, S.S. Pathogenesis of nonalcoholic steatohepatitis. Cell Mol. Life Sci. 2016, 73, 1969–1987. [Google Scholar] [CrossRef]
- Kaufmann, B.; Reca, A.; Wang, B.; Friess, H.; Feldstein, A.E.; Hartmann, D. Mechanisms of nonalcoholic fatty liver disease and implications for surgery. Langenbeck’s Arch. Surg. 2021, 406, 1–17. [Google Scholar] [CrossRef]
- Wong, V.W.; Chan, W.K.; Chitturi, S.; Chawla, Y.; Dan, Y.Y.; Duseja, A.; Fan, J.; Goh, K.-L.; Hamaguchi, M.; Hashimoto, E. Asia-pacific working party on non-alcoholic fatty liver disease guidelines 2017—Part 1: Definition, risk factors and assessment. J. Gastroenterol. Hepatol. 2018, 33, 70–85. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. Obes. Facts 2016, 9, 65–90. [Google Scholar] [CrossRef] [Green Version]
- Obika, M.; Noguchi, H. Diagnosis and evaluation of nonalcoholic fatty liver disease. Exp. Diabetes Res. 2012, 2012, 145754. [Google Scholar] [CrossRef]
- Papatheodoridi, M.; Cholongitas, E. Diagnosis of non-alcoholic fatty liver disease (NAFLD): Current concepts. Curr. Pharm. Des. 2018, 24, 4574–4586. [Google Scholar] [CrossRef]
- Piazzolla, V.A.; Mangia, A. Noninvasive diagnosis of NAFLD and NASH. Cells 2020, 9, 1005. [Google Scholar] [CrossRef]
- Ore, A.; Akinloye, O.A. Oxidative stress and antioxidant biomarkers in clinical and experimental models of non-alcoholic fatty liver disease. Medicina 2019, 55, 26. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, D. Seed to patient in clinically proven natural medicines. In Nutraceuticals: Efficacy, Safety and Toxicity; Gupta, R.C., Ed.; Academic Press: London, UK, 2016; pp. 925–931. [Google Scholar] [CrossRef]
- Yasmin, A.R.; Chia, S.L.; Looi, Q.H.; Omar, A.R.; Noordin, M.M.; Ideris, A. Herbal Extracts as Antiviral Agents. Feed Additives, Aromatic Plants and Herbs in Animal Nutrition and Health; Florou-Paneri, P., Christaki, E., Giannenas, I., Eds.; Academic Press: London, UK, 2020; pp. 115–132. [Google Scholar] [CrossRef]
- Liu, J.; Sun, K.; Zheng, C.; Chen, X.; Zhang, W.; Wang, Z.; Shar, P.A.; Xiao, W.; Wang, Y. Pathway as a pharmacological target for herbal medicines: An investigation from reduning injection. PLoS ONE 2015, 10, e0123109. [Google Scholar] [CrossRef]
- Chen, L.; Lv, D.; Wang, D.; Chen, X.; Zhu, Z.; Cao, Y.; Chai, Y. A novel strategy of profiling the mechanism of herbal medicines by combining network pharmacology with plasma concentration determination and affinity constant measurement. J. Mol. Bisyst. 2016, 12, 3347–3356. [Google Scholar] [CrossRef]
- Tarkang, P.A.; Appiah-Opong, R.; Ofori, M.F.; Ayong, L.S.; Nyarko, A.K. Application of multi-target phytotherapeutic concept in malaria drug discovery: A systems biology approach in biomarker identification. Biomark. Res. 2016, 4, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.Y.; Lim, H.S.; Kim, Y.J.; Sohn, E.; Kim, Y.H.; Koo, I.; Jeong, S.J. Similarity of therapeutic networks induced by a multi-component herbal remedy, Ukgansan, in neurovascular unit cells. Sci. Rep. 2020, 10, 2658. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Hu, Y.; Wang, L.; Wang, Y.; Na, S.; Wang, J.; Shun, Y.; Wang, X.; Xue, P.; Zhao, P.; et al. Understanding the multitarget pharmacological mechanism of the traditional mongolian common herb pair guangzao-roudoukou acting on coronary heart disease based on a bioinformatics approach. Evid.-Based Complement. Altern. Med. 2018, 2018, 7956503. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Bai, L.; Wei, F.; Zhao, J.; Wang, D.; Xiao, Y.; Yan, W.; Wei, J. Therapeutic mechanisms of herbal medicines against insulin resistance: A review. Front. Pharmacol. 2019, 10, 661. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.L.; Lin, Y.; Bartolome, A.P.; Chen, Y.C.; Chiu, S.C.; Yang, W.C. Herbal therapies for type 2 diabetes mellitus: Chemistry, biology, and potential application of selected plants and compounds. Evid.-Based Complement. Altern. Med. 2013, 2013, 378657. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Liu, W.; Baker, S.S.; Li, H.; Chen, C.; Liu, Q.; Tang, S.; Guan, L.; Tsompana, M.; Kozielski, R.; et al. Multi-targeting therapeutic mechanisms of the Chinese herbal medicine QHD in the treatment of non-alcoholic fatty liver disease. Oncotarget 2017, 8, 27820–27838. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Jian, T.; Lü, H.; Ding, X.; Wu, Y.; Zuo, Y.; Li, J.; Chen, J.; Gu, H. Polyphenol-rich Trapa quadrispinosa pericarp extract ameliorates high-fat diet induced non-alcoholic fatty liver disease by regulating lipid metabolism and insulin resistance in mice. PeerJ 2019, 7, e8165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.R.; Park, K.I.; Ma, J.Y. Leonurus japonicus houtt attenuates nonalcoholic fatty liver disease in free fatty acid-induced HEPG2 cells and mice fed a high-fat diet. Nutrients 2017, 10, 20. [Google Scholar] [CrossRef] [Green Version]
- Al Zarzour, R.H.; Ahmad, M.; Asmawi, M.Z.; Kaur, G.; Saeed, M.A.A.; Al-Mansoub, M.A.; Saghir, S.A.M.; Usman, N.S.; Al-Dulaimi, D.W.; Yam, M.F. Phyllanthus niruri standardized extract alleviates the progression of non-alcoholic fatty liver disease and decreases atherosclerotic risk in sprague-dawley rats. Nutrients 2017, 9, 766. [Google Scholar] [CrossRef] [Green Version]
- Tan, Y.; Lao, W.; Xiao, L.; Wang, Z.; Xiao, W.; Kamal, M.A.; Seale, J.P.; Qu, X. Managing the combination of nonalcoholic Fatty liver disease and metabolic syndrome with chinese herbal extracts in high-fat-diet fed rats. Evid.-Based Complement. Altern. Med. 2013, 2013, 306738. [Google Scholar] [CrossRef]
- Khlifi, R.; Dhaouefi, Z.; Toumia, I.B.; Lahmar, A.; Sioud, F.; Bouhajeb, R.; Bellalah, A.; Chekir-Ghedira, L. Erica multiflora extract rich in quercetin-3-O-glucoside and kaempferol-3-O-glucoside alleviates high fat and fructose diet-induced fatty liver disease by modulating metabolic and inflammatory pathways in Wistar rats. J. Nutr. Biochem. 2020, 86, 108490. [Google Scholar] [CrossRef]
- Hong, X.; Tang, H.; Wu, L.; Li, L. Protective effects of the Alisma orientalis extract on the experimental nonalcoholic fatty liver disease. J. Pharm. Pharmacol. 2006, 58, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- Chidambaram, J.; Carani Venkatraman, A. Cissus quadrangularis stem alleviates insulin resistance, oxidative injury and fatty liver disease in rats fed high fat plus fructose diet. Food Chem. Toxicol. 2010, 48, 2021–2029. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.J.; Liou, S.S.; Tzeng, T.F.; Liu, I.M. The ethanol extract of Zingiber zerumbet Smith attenuates non-alcoholic fatty liver disease in hamsters fed on high-fat diet. Food Chem. Toxicol. 2014, 65, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Bae, U.; Oh, M.; Jung, T.; Chae, S.; Park, B. Decursin and decursinol angelate-rich Angelica gigas Nakai extract suppresses de novo lipogenesis and alleviates nonalcoholic fatty liver disease and dyslipidemia in mice fed a high fat diet. J. Funct. Foods 2017, 31, 208–216. [Google Scholar] [CrossRef]
- Zhang, Q.Q.; Lu, L.G. Nonalcoholic fatty liver disease: Dyslipidemia, risk for cardiovascular complications, and treatment strategy. J. Clin. Transl. Hepatol. 2015, 3, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Willows, R.; Sanders, M.J.; Xiao, B.; Patel, B.R.; Martin, S.R.; Read, J.; Wilson, J.R.; Hubbard, J.; Gamblin, S.J.; Carling, D. Phosphorylation of AMPK by upstream kinases is required for activity in mammalian cells. Biochem. J. 2017, 474, 3059–3073. [Google Scholar] [CrossRef] [Green Version]
- Shimano, H.; Sato, R. SREBP-regulated lipid metabolism: Convergent physiology—Divergent pathophysiology. Nat. Rev. Endocrinol. 2017, 13, 710–730. [Google Scholar] [CrossRef] [PubMed]
- Hunkeler, M.; Hagmann, A.; Stuttfeld, E.; Chami, M.; Guri, Y.; Stahlberg, H.; Maier, T. Structural basis for regulation of human acetyl-CoA carboxylase. Nature 2018, 558, 470–474. [Google Scholar] [CrossRef]
- Czech, M.P.; Tencerova, M.; Pedersen, D.J.; Aouadi, M. Insulin signalling mechanisms for triacylglycerol storage. Diabetologia 2013, 56, 949–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, S.; Kobayashi, M.; Kitagishi, Y. Roles for PI3K/AKT/PTEN pathway in cell signaling of nonalcoholic fatty liver disease. ISRN Endocrinol. 2013, 2013, 472432. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Pan, H.; Wang, X.; He, H.; Li, M. Leonurus japonicus Houtt.: Ethnopharmacology, phytochemistry and pharmacology of an important traditional Chinese medicine. J. Ethnopharmacol. 2014, 152, 14–32. [Google Scholar] [CrossRef]
- Shin, H.Y.; Kim, S.H.; Kang, S.M.; Chang, I.J.; Kim, S.Y.; Jeon, H.; Leem, K.H.; Park, W.H.; Lim, J.P.; Shin, T.Y. Anti-inflammatory activity of Motherwort (Leonurus sibiricus L.). Immunopharmacol. Immunotoxicol. 2009, 31, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Liss, K.H.; Finck, B.N. PPARs and nonalcoholic fatty liver disease. Biochimie 2017, 136, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Francque, S.; Verrijken, A.; Caron, S.; Prawitt, J.; Paumelle, R.; Derudas, B.; Lefebvre, P.; Taskinen, M.R.; Van Hul, W.; Mertens, I.; et al. PPARalpha gene expression correlates with severity and histological treatment response in patients with non-alcoholic steatohepatitis. J. Hepatol. 2015, 63, 164–173. [Google Scholar] [CrossRef]
- Bagalkotkar, G.; Sagineedu, S.R.; Saad, M.S.; Stanslas, J. Phytochemicals from Phyllanthus niruri Linn. And their pharmacological properties: A review. J. Pharm. Pharmacol. 2006, 58, 1559–1570. [Google Scholar] [CrossRef]
- Shanmugam, B.; Shanmugam, K.R.; Ravi, S.; Subbaiah, G.V.; Ramakrishana, C.; Mallikarjuna, K.; Reddy, K.S. Exploratory studies of (-)-Epicatechin, a bioactive compound of Phyllanthus niruri, on the antioxidant enzymes and oxidative stress markers in D-galactosamine-induced hepatitis in rats: A study with reference to clinical prospective. Pharmacogn. Mag. 2017, 13, S56. [Google Scholar] [CrossRef]
- Ji, W.; Gong, B.Q. Hypolipidemic activity and mechanism of purified herbal extract of Salvia miltiorrhiza in hyperlipidemic rats. J. Ethnopharmacol. 2008, 119, 291–298. [Google Scholar] [CrossRef]
- Wang, B.E. Treatment of chronic liver diseaseswith traditional Chinese medicine. J. Gastroenterol. Hepatol. 2000, 15, E67–E70. [Google Scholar] [CrossRef]
- Oral, E.A.; Simha, V.; Ruiz, E.; Andewelt, A.; Premkumar, A.; Snell, P.; Wagner, A.J.; DePaoli, A.M.; Reitman, M.L.; Taylor, S.I.; et al. Leptin-replacement therapy for lipodystrophy. N. Engl. J. Med. 2002, 346, 570–578. [Google Scholar] [CrossRef]
- Boutari, C.; Mantzoros, C.S. Adiponectin and leptin in the diagnosis and therapy of NAFLD. Metabolism 2019, 103, 154028. [Google Scholar] [CrossRef] [PubMed]
- Adolph, T.E.; Grander, C.; Grabherr, F.; Tilg, H. Adipokines and non-alcoholic fatty liver disease: Multiple interactions. Int. J. Mol. Sci. 2017, 18, 1649. [Google Scholar] [CrossRef] [Green Version]
- Tilg, H. The role of cytokines in non-alcoholic fatty liver disease. Dig. Dis. 2010, 28, 179–185. [Google Scholar] [CrossRef]
- Stojsavljević, S.; Gomerčić Palčić, M.; Virović Jukić, L.; Smirčić Duvnjak, L.; Duvnjak, M. Adipokines and proinflammatory cytokines, the key mediators in the pathogenesis of nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 18070–18091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khlifi, R.; Lahmar, A.; Dhaouefi, Z.; Kalboussi, Z.; Maatouk, M.; Kilani-Jaziri, S.; Ghedira, K.; Chekir-Ghedira, L. Assessment of hypolipidemic, anti-inflammatory and antioxidant properties of medicinal plant Erica multiflora in triton WR-1339-induced hyperlipidemia and liver function repair in rats: A comparison with fenofibrate. Regul. Toxicol. Pharmacol. 2019, 107, 104404. [Google Scholar] [CrossRef] [PubMed]
- Harnafi, H.; el Houda Bouanani, N.; Aziz, M.; Caid, H.S.; Ghalim, N.; Amrani, S. The hypolipidaemic activity of aqueous Erica multiflora flowers extract in triton WR-1339 induced hyperlipidaemic rats: A comparison with fenofibrate. J. Ethnopharmacol. 2007, 109, 156–160. [Google Scholar] [CrossRef]
- Tian, T.; Chen, H.; Zhao, Y.Y. Traditional uses, phytochemistry, pharmacology, toxicology and quality control of Alisma orientale (Sam.) Juzep: A review. J. Ethnopharmacol. 2014, 158, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Shu, Z.; Pu, J.; Chen, L.; Zhang, Y.; Rahman, K.; Qin, L.; Zheng, C. Alisma orientale: Ethnopharmacology, phytochemistry and pharmacology of an important traditional chinese medicine. Am. J. Chin. Med. 2016, 44, 227–251. [Google Scholar] [CrossRef]
- Sundaran, J.; Begum, R.; Vasanthi, M.; Kamalapathy, M.; Bupesh, G.; Sahoo, U. A short review on pharmacological activity of Cissus quadrangularis. Bioinformation 2020, 16, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Oben, J.E.; Ngondi, J.L.; Momo, C.N.; Agbor, G.A.; Sobgui, C.S.M. The use of a Cissus quadrangularis/Irvingia gabonensis combination in the management of weight loss: A double-blind placebo-controlled study. Lipids Health Dis. 2008, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Yob, N.J.; Jofrry, S.M.; Affandi, M.M.; The, L.K.; Salleh, M.Z.; Zakaria, Z.A. Zingiber zerumbet (L.) Smith: A review of its ethnomedicinal, chemical, and pharmacological uses. Evid.-Based Complement. Altern. Med. 2011, 2011, 543216. [Google Scholar] [CrossRef]
- Koga, A.Y.; Beltrame, F.L.; Pereira, A.V. Several aspects of Zingiber zerumbet: A review. Rev. Bras. Farmacogn. 2016, 26, 385–391. [Google Scholar] [CrossRef]
- Ahmadabadi, H.K.; Vaez-Mahdavi, M.R.; Kamalinejad, M.; Shariatpanahi, S.S.; Ghazanfari, T.; Jafari, F. Pharmacological and biochemical properties of Zingiber zerumbet (L.) Roscoe ex Sm. and its therapeutic efficacy on osteoarthritis of knee. J. Fam. Med. Prim. Care 2019, 8, 3798–3807. [Google Scholar] [CrossRef]
- Kohjima, M.; Higuchi, N.; Kato, M.; Kotoh, K.; Yoshimoto, T.; Fujino, T.; Yada, M.; Yada, R.; Harada, N.; Enjoji, M.; et al. SREBP-1c, regulated by the insulin and AMPK signaling pathways, plays a role in nonalcoholic fatty liver disease. Int. J. Mol. Med. 2008, 21, 507–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambrecht, J.; Tacke, F. Acetyl-CoA carboxylase inhibition as a therapeutic tool in the battle against NASH: Hitting more than just one mechanism? Cell. Mol. Gastroenterol. Hepatol. 2020, 10, 859–861. [Google Scholar] [CrossRef]
- Goedeke, L.; Bates, J.; Vatner, D.F.; Perry, R.J.; Wang, T.; Ramirez, R.; Li, L.; Ellis, M.W.; Zhang, D.; Wong, K.E.; et al. Acetyl-CoA carboxylase inhibition reverses NAFLD and hepatic insulin resistance but promotes hypertriglyceridemia in rodents. Hepatology 2018, 68, 2197–2211. [Google Scholar] [CrossRef] [Green Version]
- Dorn, C.; Riener, M.O.; Kirovski, G.; Saugspier, M.; Steib, K.; Weiss, T.S.; Gäbele, E.; Kristiansen, G.; Hartmann, A.; Hellerbrand, C. Expression of fatty acid synthase in nonalcoholic fatty liver disease. Int. J. Clin. Exp. Pathol. 2010, 3, 505–514. [Google Scholar]
- Kotronen, A.; Seppänen-Laakso, T.; Westerbacka, J.; Kiviluoto, T.; Arola, J.; Ruskeepää, A.L.; Oresic, M.; Yki-Järvinen, H. Hepatic stearoyl-CoA desaturase (SCD)-1 activity and diacylglycerol but not ceramide concentrations are increased in the nonalcoholic human fatty liver. Diabetes 2009, 58, 203–208. [Google Scholar] [CrossRef] [Green Version]
- He, A.; Chen, X.; Tan, M.; Chen, Y.; Lu, D.; Zhang, X.; Dean, J.M.; Razani, B.; Lodhi, I.J. Acetyl-CoA derived from hepatic peroxisomal β-oxidation inhibits autophagy and promotes steatosis via mTORC1 activation. Mol. Cell. 2020, 79, 30–42. [Google Scholar] [CrossRef]
- Chi, H.J.; Kim, H.S. Studies on the components of Umbelliferae plants in Korea: Pharmacological study of decursin, decursinol and nodakenin. Korean J. Pharmacol. 1970, 1, 25–32. [Google Scholar]
- Ok, S.; Oh, S.R.; Jung, T.S.; Jeon, S.O.; Jung, J.W.; Ryu, D.S. Effects of Angelica gigas nakai as an anti-inflammatory agent in In Vitro and In Vivo atopic dermatitis models. Evid.-Based Complement. Altern. Med. 2018, 2018, 2450712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, K.O.; Lee, I.; Paik, S.Y.; Kim, D.E.; Lim, J.D.; Kang, W.S.; Ko, S. Ultrafine angelica gigas powder normalizes ovarian hormone levels and has antiosteoporosis properties in ovariectomized rats: Particle size effect. J. Med. Food 2012, 15, 863–872. [Google Scholar] [CrossRef] [Green Version]
- Sowndhararajan, K.; Kim, S. Neuroprotective and cognitive enhancement potentials of angelica gigas Nakai root: A review. Sci. Pharm. 2017, 85, 21. [Google Scholar] [CrossRef] [Green Version]
- Reddy, C.S.; Kim, S.C.; Hur, M.; Kim, Y.B.; Park, C.G.; Lee, W.M.; Jang, J.K.; Koo, S.C. Natural Korean medicine Dang-Gui: Biosynthesis, effective extraction and formulations of major active pyranocoumarins, their molecular action mechanism in cancer, and other biological activities. Molecules 2017, 22, 2170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.; Park, P.S.; Jeong, D.H.; Sim, S.; Kim, N.; Park, H.; Jeon, K.S.; Um, Y.; Kim, M.J. The characteristics of the growth and the active compounds of angelica gigas Nakai in cultivation sites. Plants 2020, 9, 823. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Kuda, O.; Samovski, D.; Abumrad, N.A. Structure-function of CD36 and importance of fatty acid signal transduction in fat metabolism. Ann. Rev. Nutr. 2014, 34, 281–303. [Google Scholar] [CrossRef] [Green Version]
- Koonen, D.P.; Jacobs, R.L.; Febbraio, M.; Young, M.E.; Soltys, C.L.; Ong, H.; Vance, D.E.; Dyck, J.R. Increased hepatic CD36 expression contributes to dyslipidemia associated with diet-induced obesity. Diabetes 2007, 56, 2863–2871. [Google Scholar] [CrossRef] [Green Version]
- Zhan, Z.; Ren, H.; Peng, M.L. Role of CD36 in nonalcoholic fatty liver disease. Chin. J. Hepatol. 2017, 25, 953–956. [Google Scholar] [CrossRef]
- Wilson, C.G.; Tran, J.L.; Erion, D.M.; Vera, N.B.; Febbraio, M.; Weiss, E.J. Hepatocyte-specific disruption of CD36 attenuates fatty liver and improves insulin sensitivity in HFD-Fed mice. Endocrinology 2016, 157, 570–585. [Google Scholar] [CrossRef] [Green Version]
- Sampath, H.; Ntambi, J. Role of stearoyl-CoA desaturase in human metabolic disease. Future Lipidol. 2008, 3, 163–173. [Google Scholar] [CrossRef]
- Popeijus, H.E.; Saris, W.H.; Mensink, R.P. Role of stearoyl-CoA desaturases in obesity and the metabolic syndrome. Int. J. Obes. 2008, 32, 1076–1082. [Google Scholar] [CrossRef] [Green Version]
- Colak, Y.; Ozturk, O.; Senates, E.; Tuncer, I.; Yorulmaz, E.; Adali, G.; Doganay, L.; Enc, F.Y. SIRT1 as a potential therapeutic target for treatment of nonalcoholic fatty liver disease. Med. Sci. Monit. 2011, 17, HY5–HY9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, R.B.; Bao, J.; Deng, C.X. Emerging roles of SIRT1 in fatty liver diseases. Int. J. Biol. Sci. 2017, 13, 852–867. [Google Scholar] [CrossRef] [PubMed]
- Niu, B.; He, K.; Li, P.; Gong, J.; Zhu, X.; Ye, S.; Ou, Z.; Ren, G. SIRT1 upregulation protects against liver injury induced by a HFD through inhibiting CD36 and the NF-κB pathway in mouse kupffer cells. Mol. Med. Rep. 2018, 18, 1609–1615. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Metabolic Risk Abnormalities | Values |
|---|---|
| Waist circumference | ≥102/88 cm in Caucasian men and women (or ≥90/80 cm in Asian men and women) |
| Blood pressure | ≥130/85 mmHg or specific drug treatment |
| Plasma triglycerides | ≥150 mg/dL (≥1.70 mmol/L) or specific drug treatment |
| Plasma HDL-cholesterol | <40 mg/dL (<1.0 mmol/L) for men and <50 mg/dL (<1.3 mmol/L) for women or specific drug treatment |
| (a) Fasting glucose levels or (b) 2-h post-load glucose levels or (c) HbA1c | 100 to 125 mg/dL (5.6 to 6.9 mmol/L) 140 to 199 mg/dL (7.8 to 11.0 mmol) 5.7% to 6.4% (39 to 47 mmol/mol) |
| HOMA-IR score | ≥2.5 |
| Plasma hs-CRP level | >2 mg/L |
| Phytomedicine | Dosage | NAFLD Model | Study Duration | Effect on Lipometabolism | Effect on Glycometabolism/ Insulin Resistance | Effect on Hepatic Steatosis | Effect on Oxidative Stress | Effect on Hepatocyte Injury | Effect on Inflammation | Effect on Obesity | Effect on Fibrosis | Effect on Cardiometabolic Risk | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trapa quadrispinosa pericarp extract (TQPE) | 30 mg/kg/d TQPE (p.o.) | HFD/ICR mice | 12 weeks (therapy from week 5) | ↓P-TG ↓P-TC ↓P-LDL-c ↑P-HDL-c ↑p-AMPK/AMPK ↓SREBP/β-Actin ↑p-ACC/ACC | ↓S-INS ↓HOMA-IR ↑p-IRS1/IRS1 ↑p-Akt/Akt | ↓Steatosis (HE) | ↓MDA ↑SOD | ↓P-ALT ↓P-AST | n/a | ↓BW gain | n/a | n/a | [32] |
| Leonurus japonicus ethanol extract (LJE) | 100 or 200 mg/kg/d LJE p.o. | HFD/male C57BL/6 mice | 14 weeks | ↓S-TG; ↓L-TG ↓S-TC; ↓L-TC ↓S-LDL-c ↓SREBP (ns) ↑p-AMPK/AMPK ↑PPAR-α | ↓S-INS ↓S-GLU ↓HOMA-IR | ↓Steatosis (HE) | ↓MDA | ↓S-ALT ↓S-AST ↓S-LDH | n/a | ↓BW gain | n/a | n/a | [33] |
| Phyllanthus niruri 50% methanol in water extract (PN50ME) | 1000 mg/kg bw/d PN50ME p.o. | HFD/male Sprague–Dawley rats | 8 weeks (therapy from week 5) | ↓S-FFA ↓S-TC; ↓L-TC ↓L-TG ↓S-LDL | ↓S-INS ↓S-GLU ↓HOMA-IR | ↓Steatosis (HE) ↓Hepatocyte Ballooning | ↓MDA | ↓S-ALT ↓AST/ALT | ↓inflammation score (HE) | ↓BW gain | n/a | ↓CRI-I ↓CRI-II ↓AC | [34] |
| Salvia miltiorrhiza root and fruit of Gardenia jasminoides extracts (SGE) | 2 g/kg bw/d SGE p.o. | HFD/Male Sprague-Dawley | 10 weeks; therapy from week 7–10 | ↓S-FFA ↓S-TG; ↓L-TG ↓S-TC ↓S-LDL-c ↑S-HDL-c ↑AT-Leptin | ↓S-INS ↓S-GLU ↓HOMA-IR | ↓Steatosis (HE & ORO) | n/a | ↓S-ALT ↓S-AST | ↓AT-TNF-α ↓AT-IL-6 | ↓BW gain ↓Visceral fat mass | ↓Fibrosis (M3T) | n/a | [35] |
| Methanol extract from Erica multiflora leaf (M-EML) | 250 mg/kg bw/d p.o. | HFHFD/male Wistar rats | 8 weeks (therapy from week 5) | ↓P-TG ↓P-TC ↓P-LDL-c ↓P-VLDL-c ↓P-Lipase ↑P-HDL-c | ↓P-INS ↓P-GLU ↓HOMA-IR | ↓Steatosis (HE & ORO) | ↓MDA ↑SOD ↑CAT ↑GPx | ↓B-ALT ↓B-AST ↓B-ALP ↓P-TB ↓P-DB | ↓NO ↓Lysosomal activity ↓P-TNF-α ↓P-IL-6 | ↓BW gain | n/a | ↓CRI ↓AIP ↓AI | [36] |
| Alisma orientalis methanolic extract (AOME) | 150,300 and 600 mg kg−1) | HFD/Male Sprague-Dawley rats | 12 weeks, therapy from week 7 | ↓S-TG; ↓L-TG ↓S-TC; ↓L-TC | ↓FSG ↓FSI ↑ISI ↓IRI | ↓Steatosis (HE) | ↓S-MDA ↑S-SOD | ↓S-ALT ↓S-AST | n/a | BW gain (ns) | ↓Fibrosis (M3T) | n/a | [37] |
| Cissus quadrangularis stem extract (CQEt) | CQEt (10 g/100 g diet | HFFD/male Wistar albino rats | 60 days, therapy from day 16 | ↓L-FFAs ↑L-PL ↓L-TG ↓L-TC | ↓P-INS ↓P-GLU ↓HOMA-IR ↓QUICKI ↓FIRI | ↓Steatosis (HE & ORO | ↓L-TBARS ↓L-LHP ↓L-Protein carbonyls ↑SOD ↑CAT ↑GPx | ↓P-ALT ↓P-AST ↓P-GGT ↓P-ALP | n/a | ↓BW gain | n/a | n/a | [38] |
| Ethanol extract of Zingiber zerumbet rhizome (EEZZR) | 200, and 300 mg/kg | HFD/Male Golden Syrian hamsters | 10 weeks, therapy from week 3 | ↓L-TC; ↓P-TC ↓P-TG; ↓L-TG ↓P-LDL-c ↓P-FFAs ↑P-HDL-c ↓L-SREBP-1c ↓L-ACC1 ↓L-FAS ↓L-SCD-1 ↑L-PPARα ↑L-CPT-1 ↑L-ACO ↑L-ACOX1 | ↓P-INS ↓P-GLU ↓HOMA-IR | ↓Steatosis (HE | n/a | n/a | ↓L-TNF-α ↓L-IL-6 ↓L-MCP1 ↓F4/80 | ↓BW gain | ↓A-SMA | n/a | [39] |
| Angelica gigas Nakai extract (AGNE) | 40 mg/kg) | HFD/c57BL6/J mice | 16 weeks. | ↓S-Leptin ↓L-TG ↓S-TG ↓S-TC ↓S-LDL S-HDL (ns) ↓L-FAS/β-actin ↓SREBP1/LaminB ↓L-CD36/β-actin ↓L-SCD-1/β-actin ↑Sirt1/β-actin ↑p-AMPK/AMPK ↑L-p-ACC/ACC | ↓S-INS ↓S-GLU ↓HOMA-IR ↓B-GLU (GTT) ↓B-GLU (ITT) ↑S-Adiponectin ↑p-Akt/Akt | ↓Steatosis (HE, ORO) | n/a | n/a | ↓S-TNF-α ↓S-IL-6 ↓S-MCP1 ↓L-F4/80 | n/a | n/a | n/a | [40] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ore, A.; Akinloye, O.A. Phytotherapy as Multi-Hit Therapy to Confront the Multiple Pathophysiology in Non-Alcoholic Fatty Liver Disease: A Systematic Review of Experimental Interventions. Medicina 2021, 57, 822. https://doi.org/10.3390/medicina57080822
Ore A, Akinloye OA. Phytotherapy as Multi-Hit Therapy to Confront the Multiple Pathophysiology in Non-Alcoholic Fatty Liver Disease: A Systematic Review of Experimental Interventions. Medicina. 2021; 57(8):822. https://doi.org/10.3390/medicina57080822
Chicago/Turabian StyleOre, Ayokanmi, and Oluseyi Adeboye Akinloye. 2021. "Phytotherapy as Multi-Hit Therapy to Confront the Multiple Pathophysiology in Non-Alcoholic Fatty Liver Disease: A Systematic Review of Experimental Interventions" Medicina 57, no. 8: 822. https://doi.org/10.3390/medicina57080822