
Computational Models Used to Predict Cardiovascular Complications in Chronic Kidney Disease Patients: A Systematic Review

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
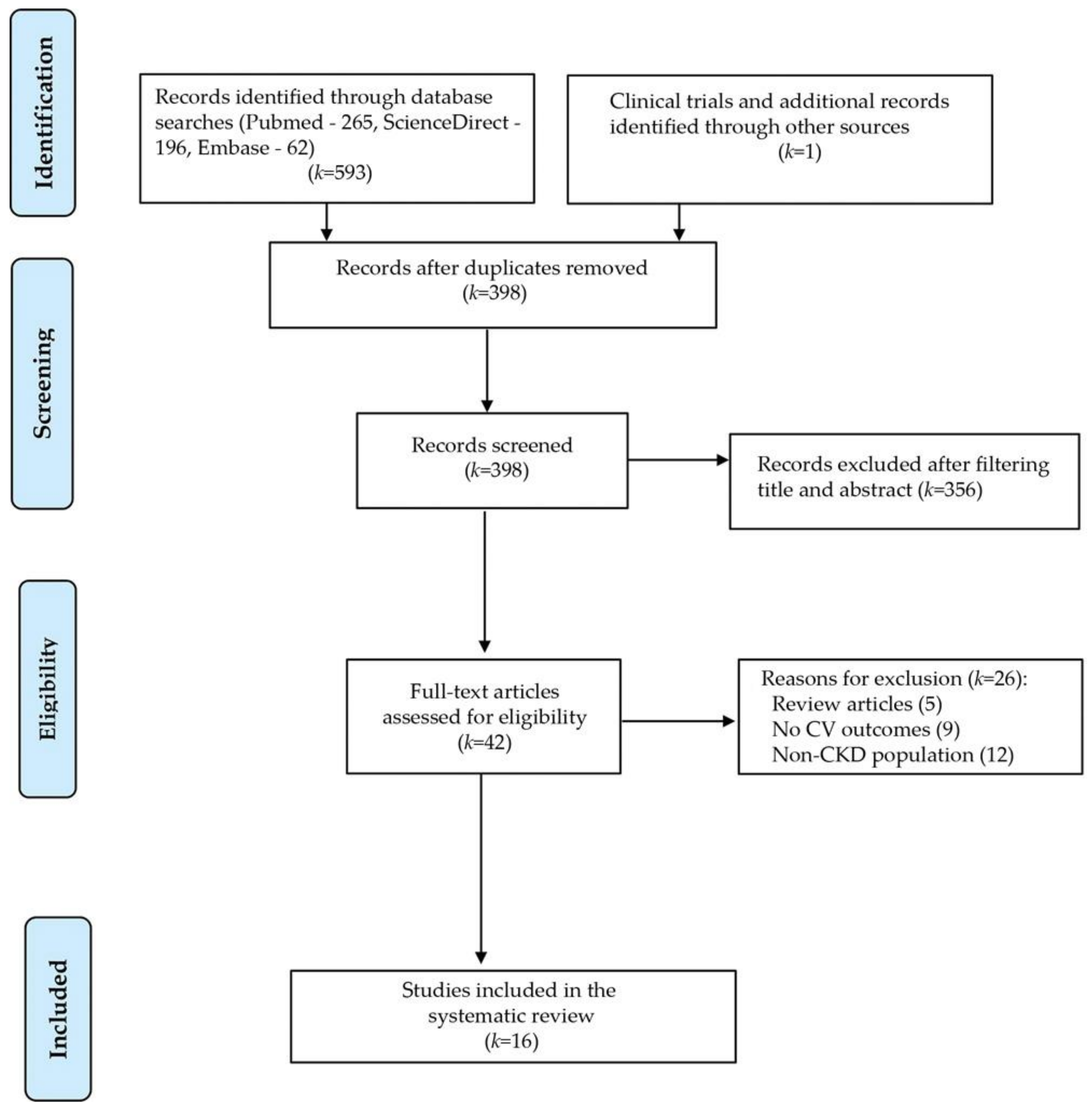
2. Materials and Methods
2.1. Data Sources
2.2. Study Selection
2.3. Data Extraction
2.4. Outcomes
2.5. Quality Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Streja, E.; Norris, K.C.; Budoff, M.J.; Hashemi, L.; Akbilgic, O.; Kalantar-Zadeh, K. The quest for cardiovascular disease risk prediction models in patients with nondialysis chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2021, 30, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Roy, G.C.; Sutradhar, S.R.; Barua, U.K.; Datta, N.C.; Debnath, C.R.; Hoque, M.M.; Hossain, A.S.; Haider, M.S.; Das, M. Cardiovascular complications of chronic renal failure—An updated review. Mymensingh Med. J. 2012, 21, 573–579. [Google Scholar] [PubMed]
- Sarnak, M.J. Cardiovascular complications in chronic kidney disease. Am. J. Kidney Dis. 2003, 41, 11–17. [Google Scholar] [CrossRef]
- Schiffrin, E.L.; Lipman, M.L.; Mann, J.F. Chronic kidney disease: Effects on the cardiovascular system. Circulation 2007, 116, 85–97. [Google Scholar] [CrossRef] [Green Version]
- Alloghani, M.; Al-Jumeily, D.; Hussain, A.; Liatsis, P.; Aljaaf, A.J. Performance-Based Prediction of Chronic Kidney Disease Using Machine Learning for High-Risk Cardiovascular Disease Patients, in Nature-Inspired Computation in Data Mining and Machine Learning; Yang, X.-S., He, X.-S., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 187–206. [Google Scholar]
- Tonelli, M.; Wiebe, N.; Culleton, B.; House, A.; Rabbat, C.; Fok, M.; McAlister, F.; Garg, A.X. Chronic Kidney Disease and Mortality Risk: A Systematic Review. J. Am. Soc. Nephrol. 2006, 17, 2034–2047. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; Dave, N.; Virani, S.S.; Navaneethan, S.D. Primary and Secondary Prevention of Cardiovascular Disease in Patients with Chronic Kidney Disease. Curr. Atheroscler. Rep. 2019, 21, 32. [Google Scholar] [CrossRef]
- Mark, P.B. Strategies to manage cardiovascular risk in chronic kidney disease. Nephrol. Dial. Transplant. 2017, 33, 23–25. [Google Scholar] [CrossRef]
- Burlacu, A.; Iftene, A.; Busoiu, E.; Cogean, D.; Covic, A. Challenging the supremacy of evidence-based medicine through artificial intelligence: The time has come for a change of paradigms. Nephrol. Dial. Transplant. 2020, 35, 191–194. [Google Scholar] [CrossRef]
- Burlacu, A.; Iftene, A.; Jugrin, D.; Popa, I.V.; Lupu, P.M.; Vlad, C.; Covic, A. Using Artificial Intelligence Resources in Dialysis and Kidney Transplant Patients: A Literature Review. BioMed Res. Int. 2020, 2020, 1–14. [Google Scholar] [CrossRef]
- Krittanawong, C.; Virk, H.U.H.; Bangalore, S.; Wang, Z.; Johnson, K.W.; Pinotti, R.; Zhang, H.; Kaplin, S.; Narasimhan, B.; Kitai, T.; et al. Machine learning prediction in cardiovascular diseases: A meta-analysis. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Cuocolo, R.; Perillo, T.; De Rosa, E.; Ugga, L.; Petretta, M. Current applications of big data and machine learning in cardiology. J. Geriatr. Cardiol. 2019, 16, 601–607. [Google Scholar]
- Banerjee, A.; Chen, S.; Fatemifar, G.; Zeina, M.; Lumbers, R.T.; Mielke, J.; Gill, S.; Kotecha, D.; Freitag, D.F.; Denaxas, S.; et al. Machine learning for subtype definition and risk prediction in heart failure, acute coronary syndromes and atrial fibrillation: Systematic review of validity and clinical utility. BMC Med. 2021, 19, 85. [Google Scholar] [CrossRef]
- Lorenzoni, G.; Sabato, S.S.; Lanera, C.; Bottigliengo, D.; Minto, C.; Ocagli, H.; De Paolis, P.; Gregori, D.; Iliceto, S.; Pisanò, F. Comparison of Machine Learning Techniques for Prediction of Hospitalization in Heart Failure Patients. J. Clin. Med. 2019, 8, 1298. [Google Scholar] [CrossRef] [Green Version]
- He, W.; Xie, Y.; Lu, H.; Wang, M.; Chen, H. Predicting Coronary Atherosclerotic Heart Disease: An Extreme Learning Machine with Improved Salp Swarm Algorithm. Symmetry 2020, 12, 1651. [Google Scholar] [CrossRef]
- Ardhanari, S.; Alpert, M.A.; Aggarwal, K. Cardiovascular disease in chronic kidney disease: Risk factors, pathogenesis, and prevention. Adv. Perit. Dial. Conf. Perit. Dial. 2014, 30, 40–53. [Google Scholar]
- Lekawanvijit, S. Cardiotoxicity of Uremic Toxins: A Driver of Cardiorenal Syndrome. Toxins 2018, 10, 352. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BMJ 2015, 350, g7594. [Google Scholar] [CrossRef] [Green Version]
- Wolff, R.F.; Moons, K.G.; Riley, R.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; PROBAST Group. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Dubin, R.F.; Whooley, M.; Pico, A.; Ganz, P.; Schiller, N.B.; Meyer, C. Proteomic analysis of heart failure hospitalization among patients with chronic kidney disease: The Heart and Soul Study. PLoS ONE 2018, 13, e0208042. [Google Scholar] [CrossRef] [Green Version]
- Akbilgic, O.; Obi, Y.; Potukuchi, P.K.; Karabayir, I.; Nguyen, D.V.; SooHoo, M.; Streja, E.; Molnar, M.Z.; Rhee, C.M.; Kalantar-Zadeh, K.; et al. Machine Learning to Identify Dialysis Patients at High Death Risk. Kidney Int. Rep. 2019, 4, 1219–1229. [Google Scholar] [CrossRef] [Green Version]
- Gowda, S.N.; Bhatnagar, U.; Blue, M.; Orvarsson, J.; Pham, R.; Abdullah, H.; Stys, A.T.; Stys, T.; Petrasko, M.; Rajpurohit, N.; et al. Efficacy of remote pulmonary artery hemodynamic monitoring system in reducing hospital encounters in heart failure patients with chronic kidney disease. J. Am. Coll. Cardiol. 2020, 75, 783. [Google Scholar] [CrossRef]
- Ahmed, A. Improving Outcomes in Veterans with Heart Failure and Chronic Kidney Disease. 2019. Available online: https://projectreporter.nih.gov/project_info_description.cfm?aid=9722004&icde=0 (accessed on 5 February 2021).
- Zelnick, L.R.; Shlipak, M.; Soliman, E.Z.; Anderson, A.H.; Christenson, R.; Lash, J.P.; Deo, R.; Rao, P.S.; Afshinnia, F.; Chen, J. et al. Prediction of Atrial Fibrillation Using Clinical and Cardiac Biomarker Data: The CRIC Study. In ASN Kidney Week; American Society of Nephrology: Washington, DC, USA, 2020. [Google Scholar]
- Galloway, C.D.; Valys, A.V.; Shreibati, J.B.; Treiman, D.L.; Petterson, F.L.; Gundotra, V.P.; Albert, D.E.; Attia, Z.I.; Carter, R.E.; Asirvatham, S.J.; et al. Development and Validation of a Deep-Learning Model to Screen for Hyperkalemia From the Electrocardiogram. JAMA Cardiol. 2019, 4, 428–436. [Google Scholar] [CrossRef]
- Fernandez-Lozano, C.; Valente, R.A.; Díaz, M.F.; Pazos, A. A generalized linear model for cardiovascular complications prediction in PD patients. In Proceedings of the First International Conference on Data Science, E-learning and Information Systems; Association for Computing Machinery (ACM), Madrid, Spain, 1–2 October 2018; p. 43. [Google Scholar]
- Forné, C.; Cambray, S.; Bermúdez-López, M.; Fernandez, E.; Bozic, M.; Valdivielso, J.M.; Regidor, J.A.; Almirall, J.; Ponz, E.; Coloma, J.A.; et al. Machine learning analysis of serum biomarkers for cardiovascular risk assessment in chronic kidney disease. Clin. Kidney J. 2019, 13, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Bermúdez-López, M.; Forne, C.; Amigo, N.; Bozic, M.; Arroyo, D.; Bretones, T.; Alonso, N.; Cambray, S.; Del Pino, M.D.; Mauricio, D.; et al. An in-depth analysis shows a hidden atherogenic lipoprotein profile in non-diabetic chronic kidney disease patients. Expert Opin. Ther. Targets 2019, 23, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.-S.; Kim, J.; Kim, D.; Woo, J.; Kim, M.; Choi, H.; Kang, A.; Park, S. Prediction of Postoperative Complications for Patients of End Stage Renal Disease. Sensors 2021, 21, 544. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; Peixoto, H.; Esteves, M.; Machado Abelha, J. Understanding Stroke in Dialysis and Chronic Kidney Disease. Procedia Comput. Sci. 2017, 113, 591–596. [Google Scholar] [CrossRef]
- Lash, J.P.; Go, A.S.; Appel, L.J.; He, J.; Ojo, A.; Rahman, M.; Townsend, R.R.; Xie, D.; Cifelli, D.; Cohan, J.; et al. Chronic Renal Insufficiency Cohort (CRIC) Study: Baseline Characteristics and Associations with Kidney Function. Clin. J. Am. Soc. Nephrol. 2009, 4, 1302–1311. [Google Scholar] [CrossRef]
- Junyent, M.; Martínez, M.; Borràs, M.; Coll, B.; Valdivielso, J.M.; Vidal, T.; Sarró, F.; Roig, J.; Craver, L.; Fernández, E. Predicting cardiovascular disease morbidity and mortality in chronic kidney disease in Spain. The rationale and design of NEFRONA: A prospective, multicenter, observational cohort study. BMC Nephrol. 2010, 11, 14. [Google Scholar] [CrossRef] [Green Version]
- de Gonzalo-Calvo, D.; Martínez-Camblor, P.; Bär, C.; Duarte, K.; Girerd, N.; Fellström, B.; Schmieder, R.E.; Jardine, A.G.; Massy, Z.A.; Holdaas, H.; et al. Improved cardiovascular risk prediction in patients with end-stage renal disease on hemodialysis using machine learning modeling and circulating microribonucleic acids. Theranostics 2020, 10, 8665–8676. [Google Scholar] [CrossRef]
- Matsushita, K.; Jassal, S.K.; Sang, Y.; Ballew, S.H.; Grams, M.E.; Surapaneni, A.; Arnlov, J.; Bansal, N.; Bozic, M.; Brenner, H.; et al. Incorporating kidney disease measures into cardiovascular risk prediction: Development and validation in 9 million adults from 72 datasets. EClinicalMedicine 2020, 27, 100552. [Google Scholar] [CrossRef]
- Titze, S.; Schmid, M.; Köttgen, A.; Busch, M.; Floege, J.; Wanner, C.; Kronenberg, F.; Eckardt, K.-U.; GCKD Study Investigators; Eckardt, K.U.; et al. Disease burden and risk profile in referred patients with moderate chronic kidney disease: Composition of the German Chronic Kidney Disease (GCKD) cohort. Nephrol. Dial. Transplant. 2015, 30, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Cai, Q.-Z.; Lu, X.-Z.; Lu, Y.; Wang, A.Y.-M. Longitudinal Changes of Cardiac Structure and Function in CKD (CASCADE Study). J. Am. Soc. Nephrol. 2014, 25, 1599–1608. [Google Scholar] [CrossRef] [Green Version]
- Titapiccolo, J.I.; Ferrario, M.; Cerutti, S.; Barbieri, C.; Mari, F.; Gatti, E.; Signorini, M.G. Artificial intelligence models to stratify cardiovascular risk in incident hemodialysis patients. Expert Syst. Appl. 2013, 40, 4679–4686. [Google Scholar] [CrossRef]
- Goldstein, B.A.; Chang, T.I.; Mitani, A.A.; Assimes, T.L.; Winkelmayer, W.C. Near-Term Prediction of Sudden Cardiac Death in Older Hemodialysis Patients Using Electronic Health Records. Clin. J. Am. Soc. Nephrol. 2014, 9, 82–91. [Google Scholar] [CrossRef] [Green Version]
- Mezzatesta, S.; Torino, C.; De Meo, P.; Fiumara, G.; Vilasi, A. A machine learning-based approach for predicting the outbreak of cardiovascular diseases in patients on dialysis. Comput. Methods Programs Biomed. 2019, 177, 9–15. [Google Scholar] [CrossRef]
- Di Lullo, L.; House, A.; Gorini, A.; Santoboni, A.; Russo, D.; Ronco, C. Chronic kidney disease and cardiovascular complications. Heart Fail. Rev. 2015, 20, 259–272. [Google Scholar] [CrossRef]
- Tamulėnaitė, E.; Žvirblytė, R.; Ereminienė, R.; Žiginskienė, E.; Ereminienė, E. Changes of Left and Right Ventricle Mechanics and Function in Patients with End-Stage Renal Disease Undergoing Haemodialysis. Medicina 2018, 54, 87. [Google Scholar] [CrossRef] [Green Version]
- Pun, P.H. The Interplay Between CKD, Sudden Cardiac Death, and Ventricular Arrhythmias. Adv. Chronic Kidney Dis. 2014, 21, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Heywood, J.T.; Fonarow, G.; Costanzo, M.R.; Mathur, V.S.; Wigneswaran, J.R.; Wynne, J. High Prevalence of Renal Dysfunction and Its Impact on Outcome in 118,465 Patients Hospitalized With Acute Decompensated Heart Failure: A Report From the ADHERE Database. J. Card. Fail. 2007, 13, 422–430. [Google Scholar] [CrossRef]
- Kaya, B.; Paydaş, S.; Aikimbaev, K.; Altun, E.; Balal, M.; Deniz, A.; Kaypakli, O.; Demirtaş, M.; Kaypaklı, O. Prevalence of cardiac arrhythmia and risk factors in chronic kidney disease patients. Saudi J. Kidney Dis. Transplant. 2018, 29, 567. [Google Scholar] [CrossRef]
- Winkelmayer, W.C.; Patrick, A.R.; Liu, J.; Brookhart, M.A.; Setoguchi, S. The Increasing Prevalence of Atrial Fibrillation among Hemodialysis Patients. J. Am. Soc. Nephrol. 2011, 22, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Cheung, A.K.; Sarnak, M.J.; Yan, G.; Berkoben, M.; Heyka, R.; Kaufman, A.; Lewis, J.; Rocco, M.; Toto, R.; Windus, D.; et al. Cardiac diseases in maintenance hemodialysis patients: Results of the HEMO Study. Kidney Int. 2004, 65, 2380–2389. [Google Scholar] [CrossRef] [Green Version]
- Bansal, N.; Keane, M.; Delafontaine, P.; Dries, D.; Foster, E.; Gadegbeku, C.A.; Go, A.S.; Hamm, L.L.; Kusek, J.W.; Ojo, A.O.; et al. A Longitudinal Study of Left Ventricular Function and Structure from CKD to ESRD: The CRIC Study. Clin. J. Am. Soc. Nephrol. 2013, 8, 355–362. [Google Scholar] [CrossRef] [Green Version]
- Kottgen, A.; Russell, S.D.; Loehr, L.R.; Crainiceanu, C.M.; Rosamond, W.D.; Chang, P.P.; Chambless, L.E.; Coresh, J. Reduced Kidney Function as a Risk Factor for Incident Heart Failure: The Atherosclerosis Risk in Communities (ARIC) Study. J. Am. Soc. Nephrol. 2007, 18, 1307–1315. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Population | Outcomes | Sample Size/Predictors No. | Algorithm | Performance |
|---|---|---|---|---|---|
| Composite CV outcomes | |||||
| de Gonzalo-Calvo et al. 2020 [34] | Hemodialysis | Time to CV death, nonfatal MI, or nonfatal stroke (24 months follow-up) | 778/8 | DT using the CART algorithm | AUC: 0.71 |
| Matsushita et al. 2020 [35] | Moderate CKD (GCKD cohort): 5-year follow-up | MI or fatal CHD or stroke | 5217 (validation set) | CKD Patch (Linear regression + Statistical methods) | AUC: 0.698 |
| Stage 3–5 CKD (Hong Kong CKD): 10-year follow-up | 300 (validation set) | AUC: 0.73 | |||
| Titapiccolo et al. 2013 [38] | Incident hemodialysis | CV events (CV mortality, insurgence of new CV co-morbidity, or CV hospitalization) in the next six months | 4246/39 | RF | AUC: 0.737 ± 1.2; ACC: 67.3 ± 2.8%; SE: 69.2 ± 3.3%; SP: 67.3 ± 2.8% |
| Jeong et al. 2021 [30] | Postoperative ESRD patients | MACE (1 month postoperatively) | 3220/40 | RF | F1 score: 0.797 |
| Fernandez-Lozano et al. 2018 [27] | Peritoneal dialysis | CVC prediction | 114 | Generalized Linear Model | AUC: 0.96 |
| Sudden cardiac death (SCD) | |||||
| Goldstein et al. 2014 [39] | Hemodialysis | Sudden cardiac death the day of or day after a dialysis session | 1796/72 | RF | AUC: 0.799 |
| Mezzatesta et al., 2019 [40] | Hemodialysis | CV death (2.5-year follow-up) | 861/23 | SVM + RBF kernel | ACC: 80% |
| Ischemic heart disease (IHD) | |||||
| Mezzatesta et al. 2019 [40] | Hemodialysis | IHD (2.5-year follow-up) | 522/29 | SVM + RBF kernel | ACC: 95.25% |
| 2677/23 | ACC: 92.15% | ||||
| Heart failure (HF) | |||||
| Dubin et al. 2018 [21] | CKD | Prognostic proteins associated with HF in CKD | 364 | RSF regression + Cox survival analysis | Angiopoietin-2: HR 1.45 [1.33, 1.59] Spondin-1: HR 1.13 [1.06, 1.20] |
| Mezzatesta et al. 2019 [40] | Hemodialysis | HF (2.5-year follow-up) | 522/29 | SVM + RBF kernel | ACC: 93% |
| 2677/23 | ACC: 64% | ||||
| Akbilgic et al. 2019 [22] | ESRD patients with congestive HF | 30-, 90-, 180-, and 365-day all-cause mortality | 14800/49 | RF | AUC: 0.683, 0.716, 0.725, and 0.725 (risk of death within the 4 different time windows) |
| Gowda et al. 2020 [23] | CKD | HF admissions in patients with CKD (1-year follow-up) | 117 | Remote IoT sensors | Significant decrease in HF admissions after implantation |
| Ahmed et al. [24] | CKD patients with HF and reduced ejection fraction | Safety and efficiency prediction of low-dose ACEIs and ARBs | Not available | ML algorithm (unspecified) | Not available (study ongoing) |
| Arrhythmias | |||||
| Zelnick et al. 2020 [25] | CKD patients without prior AF | Incident AF | 2690/32 | Lasso regression | AUC: 0.76 |
| Mezzatesta et al. 2019 [40] | Hemodialysis | Arrhythmia (2.5-year follow-up) | 522/29 | SVM + RBF kernel | ACC: 95% |
| 2677/23 | ACC: 67% | ||||
| Other CV-related predictions | |||||
| Forné et al. 2020 [28] | Stage 3–5 CKD | Atheromatous CVC (4-year follow-up) | 1366/38 | RSF | AUC: 0.744 |
| Bermudez-Lopez et al. 2019 [29] | Stage 3–5 CKD + Controls | Discriminate between proatherogenic lipid profile in CKD vs. controls | 395/10 | RF | AUC: 0.789 |
| Rodrigues et al. 2017 [31] | CAPD | Stroke risk | 850/7 | K-nearest neighbor | ACC: 99.65%; SE: 95.35%; SP: 99.88% |
| Galloway et al. 2019 [26] | Stage 3–5 CKD | Hyperkalemia detection from the ECG | 61,965 ECG-potassium pairs (validation set) | DCNN | AUC: 0.853–0.883 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burlacu, A.; Iftene, A.; Popa, I.V.; Crisan-Dabija, R.; Brinza, C.; Covic, A. Computational Models Used to Predict Cardiovascular Complications in Chronic Kidney Disease Patients: A Systematic Review. Medicina 2021, 57, 538. https://doi.org/10.3390/medicina57060538
Burlacu A, Iftene A, Popa IV, Crisan-Dabija R, Brinza C, Covic A. Computational Models Used to Predict Cardiovascular Complications in Chronic Kidney Disease Patients: A Systematic Review. Medicina. 2021; 57(6):538. https://doi.org/10.3390/medicina57060538
Chicago/Turabian StyleBurlacu, Alexandru, Adrian Iftene, Iolanda Valentina Popa, Radu Crisan-Dabija, Crischentian Brinza, and Adrian Covic. 2021. "Computational Models Used to Predict Cardiovascular Complications in Chronic Kidney Disease Patients: A Systematic Review" Medicina 57, no. 6: 538. https://doi.org/10.3390/medicina57060538