Factors Associated with the Delayed Termination of Viral Shedding in COVID-19 Patients with Mild Severity in South Korea

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
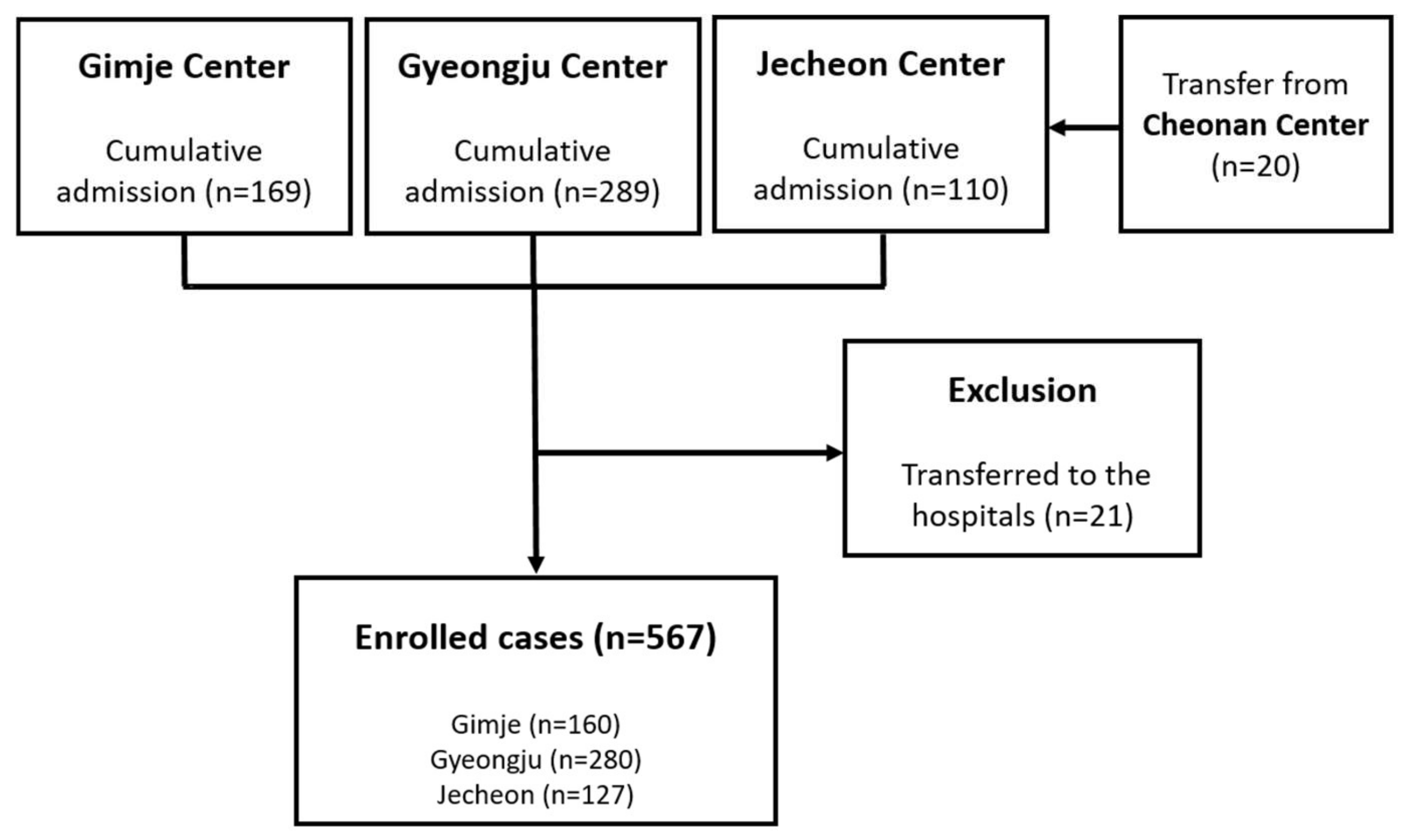
2.1. Study Setting and Study Population
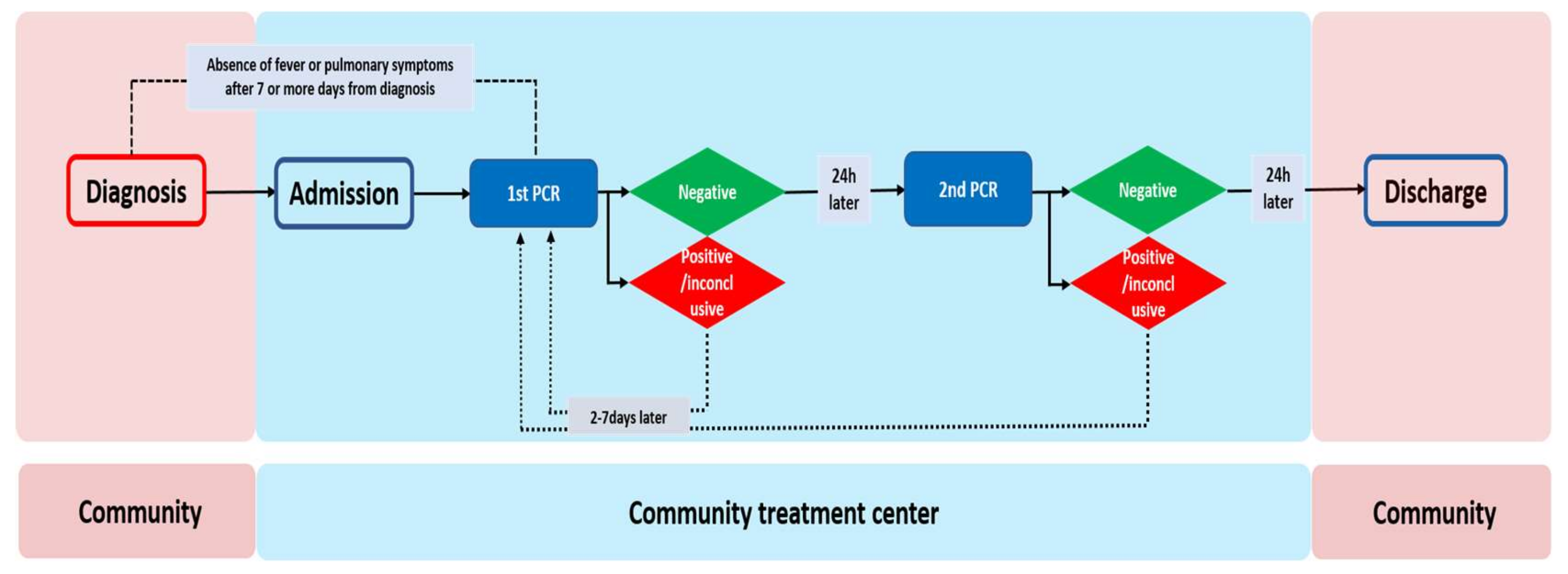
2.2. RT-PCR Test and Discharge Process for Patients
2.3. Data Collection
2.4. Definitions
2.5. Statistical Analysis
2.6. Ethics Statements
3. Results
3.1. Clinical Characteristics of Patients
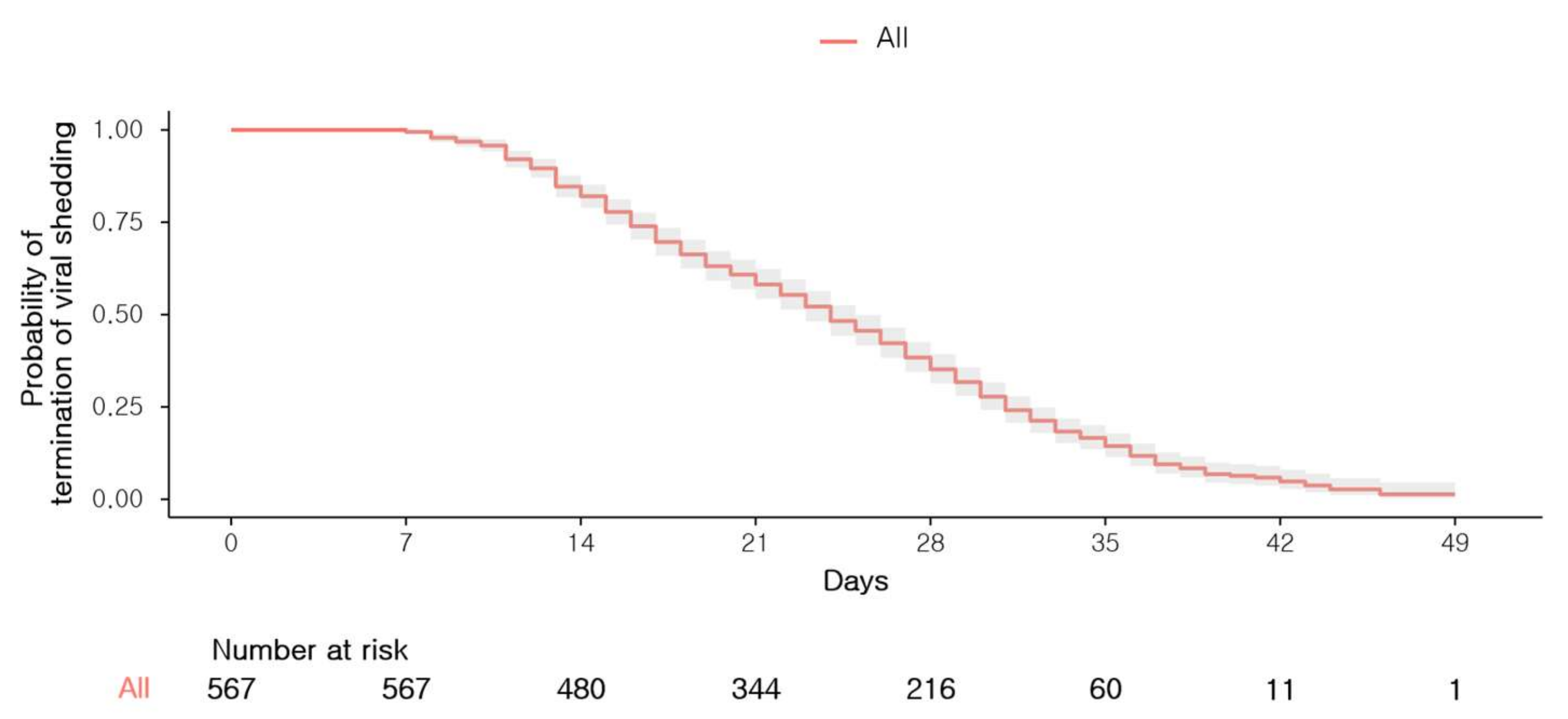
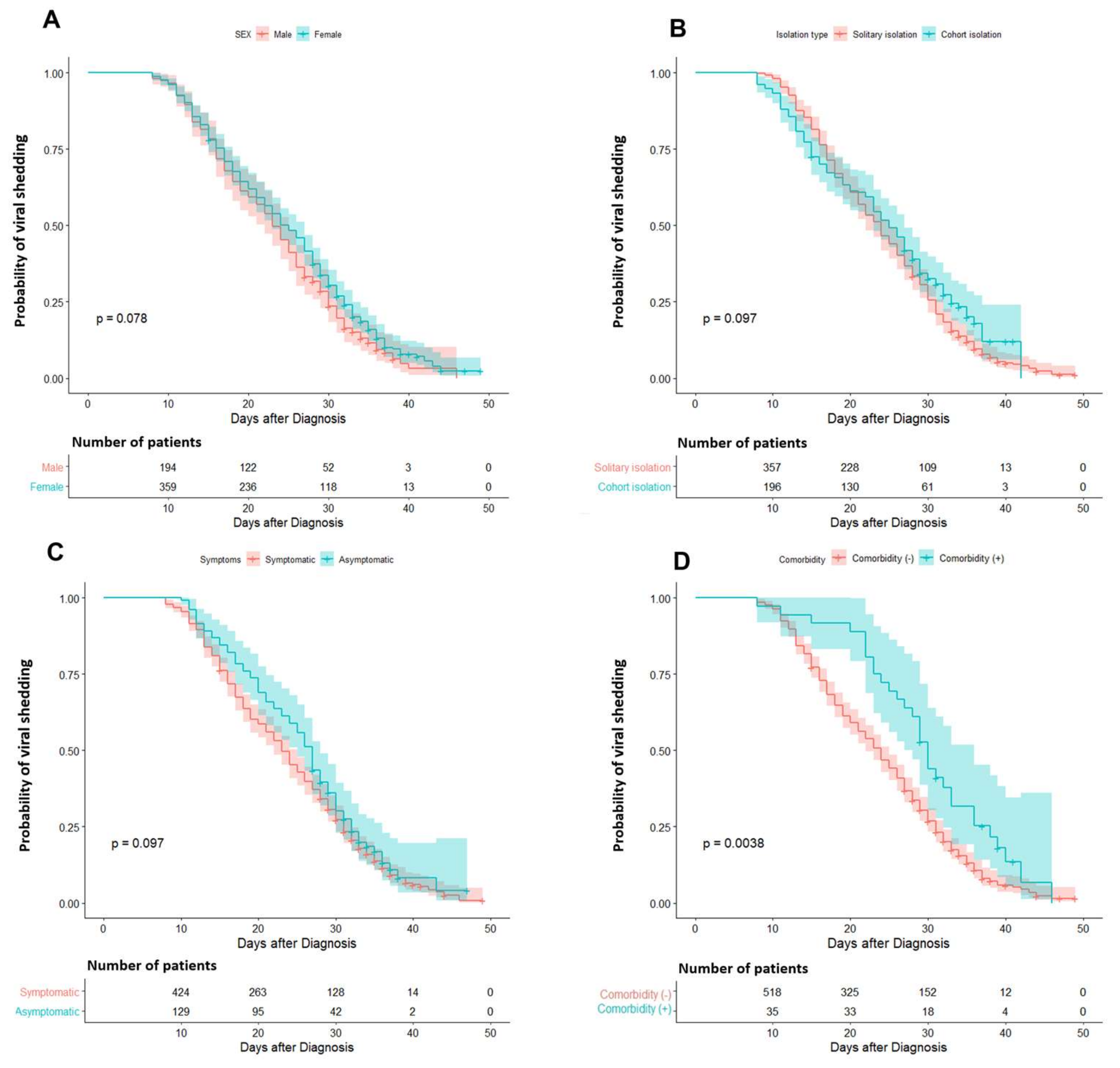
3.2. Factors Associated with the Probability of Early Termination of Viral Shedding
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Eng. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Choe, P.G.; Oh, Y.; Oh, K.J.; Kim, J.; Park, S.J.; Park, J.H.; Na, H.K.; Oh, M.D. The first case of 2019 novel coronavirus pneumonia imported into Korea from Wuhan, China: Implication for infection prevention and control measures. J. Korean Med. Sci. 2020, 35, e61. [Google Scholar] [CrossRef] [PubMed]
- Korean Society of Infectious Diseases; Korean Society of Pediatric Infectious Diseases; Korean Society of Epidemiology; Korean Society for Antimicrobial Therapy; Korean Society for Healthcare-Associated Infection Control and Prevention; Korea Centers for Disease Control and Prevention. Report on the epidemiological features of coronavirus disease 2019 (COVID-19) outbreak in the Republic of Korea from 19 January to 2 March 2020. J. Korean Med. Sci. 2020, 35, e112. [Google Scholar] [CrossRef] [PubMed]
- Center Accident Investigation Headquarters; Center Discharge Countermeasures Headquarters. Guideline for Countermeasures for COVID-19 Version 7-3; Suppl. 7, Ministry of Health and Welfare: Sejong, Korea, 2020. (In Korean)
- Park, S.Y.; Yun, S.G.; Shin, J.W.; Lee, B.Y.; Son, H.-J.; Lee, S.; Lee, E.; Kim, T.H. Persistent severe acute respiratory syndrome coronavirus 2 detection after resolution of coronavirus disease 2019-associated symptoms/signs. Korean J. Intern. Med. 2020, 35, 793–796. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro. Surveill. 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Centers for Disease Control and Prevention. COVID-19 Patient Treatment & Mangement. Available online: http://ncov.mohw.go.kr/en/baroView.do?brdId=11&brdGubun=112&dataGubun=&ncvContSeq=&contSeq=&board_id= (accessed on 24 March 2020).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Eng. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–24 February 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---24-february-2020 (accessed on 4 April 2020).
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Eng. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January–March 2020: Retrospective cohort study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Tong, Y.X.; Xiao, A.T. Profile of RT-PCR for SARS-CoV-2: A preliminary study from 56 COVID-19 patients. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention. Symptom-Based Strategy to Discontinue Isolation for Persons with COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/strategy-discontinue-isolation.html (accessed on 15 May 2020).
- Center Accident Investigation Headquarters; Center Discharge Countermeasures Headquarters. Guideline for Countermeasures for COVID-19 Version 9-1; Suppl. 37, Ministry of Health and Welfare: Sejong, Korea, 2020. (In Korean)
- Fu, Y.; Han, P.; Zhu, R.; Bai, T.; Yi, J.; Zhao, X.; Tao, M.; Quan, R.; Chen, C.; Zhang, Y.; et al. Risk factors for viral RNA shedding in COVID-19 patients. Eur. Respir. J. 2020, 56, 2001190. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Sheng, J.; Liu, Y.; Xu, Y.; Wang, Z.; Liu, L.; Shi, D.; Yu, L.; Cao, Q.; Ruan, B.; et al. Factors associated with prolonged viral RNA shedding in patients with coronavirus disease 2019 (COVID-19). Clin. Infect. Dis. 2020, 71, 799–806. [Google Scholar]
- Hu, X.; Xing, Y.; Jia, J.; Ni, W.; Liang, J.; Zhao, D.; Song, X.; Gao, R.; Jiang, F. Factors associated with negative conversion of viral RNA in patients hospitalized with COVID-19. Sci. Total Environ. 2020, 728, 138812. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Jeong, H.S.; Yu, Y.; Shin, S.U.; Kim, S.; Oh, T.H.; Kim, U.J.; Kang, S.J.; Jang, H.C.; Jung, S.I.; et al. Viral kinetics of SARS-CoV-2 in asymptomatic carriers and presymptomatic patients. Int. J. Infect. Dis. 2020, 95, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yan, L.M.; Wan, L.; Xiang, T.X.; Le, A.; Liu, J.M.; Peiris, M.; Poon, L.L.M.; Zhang, W. Viral dynamics in mild and severe cases of COVID-19. Lancet Infect Dis. 2020, 20, 656–657. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maugeri, A.; Barchitta, M.; Battiato, S.; Agodi, A. Estimation of unreported novel coronavirus (SARS-CoV-2) infections from reported deaths: A susceptible–exposed–infectious–recovered–dead model. J. Clin. Med. 2020, 9, 1350. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Isolation Type | COVID-19-Associated Symptoms | ||||||
|---|---|---|---|---|---|---|---|
| Total (n = 567) | Solitary (n = 360) | Cohort (n = 207) | p-Value | Asymptomatic (n = 438) | Symptomatic (n = 129) | p-Value | |
| Centers | |||||||
| Gimje | 160 (28.2) | 121 (29.1) | 39 (25.8) | <0.001 | 111 (25.3) | 49 (38.0) | 0.001 |
| Gyeongju | 280 (49.4) | 226 (54.3) | 54 (35.8) | - | 235 (53.7) | 45 (34.9) | - |
| Jecheon | 127 (22.4) | 13 (3.6) | 114 (55.1) | 92 (21.0) | 35 (27.1) | - | |
| Age, mean ± SD | 35.5 ± 14.9 | 36.3 ± 14.1 | 34.2 ± 16.2 | 0.119 | 35.4 ± 14.9 | 36.0 ± 15.0 | 0.654 |
| Female sex (%) | 368 (64.9) | 236 (65.6) | 132 (63.8) | 0.668 | 280 (63.9) | 88 (68.2) | 0.370 |
| Isolated at the cohort room (%) | 207 (36.5) | - | - | - | 154 (35.2) | 53 (41.1) | 0.219 |
| Existence of underlying comorbidities a (%) | 36 (6.3) | 23 (6.4) | 13 (6.3) | 0.959 | 28 (6.4) | 8 (6.2) | 0.938 |
| COVID-19-associated symptoms over the course of the disease (%) | |||||||
| Absence | 438 (77.2) | 284 (78.9) | 154 (74.4) | 0.219 | - | - | - |
| Presence | 129 (22.8) | 76 (21.1) | 53 (25.6) | - | - | - | |
| Fever | 3 (0.5) | 3 (0.8) | 0 (0) | 0.557 | - | - | - |
| Dyspnea | 1 (0.2) | 0 (0) | 1 (0.5) | 0.365 | - | - | - |
| Cough | 64 (11.3) | 39 (10.8) | 25 (12.1) | 0.652 | - | - | - |
| Nasal congestion | 54 (9.5) | 35 (9.7) | 19 (9.2) | 0.832 | - | - | - |
| Decreased sense of smell or taste | 4 (0.7) | 2 (0.6) | 2 (1.0) | 0.625 | - | - | - |
| Others b | 52 (9.2) | 33 (9.2) | 19 (9.2) | 0.996 | - | - | - |
| Number of RT-PCR tests, median (IQR) | 3.0 (2.0–4.0) | 2.5 (2.0–4.0) | 3.0 (2.0–4.0) | 0.084 | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 0.178 |
| Period of viral shedding, mean ± SD | 23.8 ± 8.7 | 24.1 ± 8.7 | 23.3 ± 8.7 | 0.302 | 23.4 ± 8.9 | 25.0 ± 7.8 | 0.051 |
| Existence of viral shedding after 24 days | 273 (48.1) | 168 (46.7) | 105 (50.7) | 0.352 | 197 (45.0) | 76 (58.9) | 0.005 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value | Hazard Ratio | 95% Confidence Interval | p-Value |
| Age | 1.000 | 0.994–1.006 | 0.965 | 1.001 | 0.994–1.007 | 0.829 |
| Female sex | 0.848 | 0.707–1.018 | 0.078 | 0.835 | 0.693–1.005 | 0.057 |
| Cohort isolation | 0.848 | 0.701–1.026 | 0.090 | 0.868 | 0.717–1.050 | 0.146 |
| Presence of COVID-19-associated symptoms a | 0.836 | 0.674–1.036 | 0.102 | 0.810 | 0.652–1.007 | 0.058 |
| Existence of underlying comorbidities b | 0.590 | 0.410–0.851 | 0.005 | 0.561 | 0.388–0.812 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.; Sohn, J.W.; Nam, S.; Sohn, J.W.; Choi, W.S.; Kim, H.S. Factors Associated with the Delayed Termination of Viral Shedding in COVID-19 Patients with Mild Severity in South Korea. Medicina 2020, 56, 659. https://doi.org/10.3390/medicina56120659
Kim B, Sohn JW, Nam S, Sohn JW, Choi WS, Kim HS. Factors Associated with the Delayed Termination of Viral Shedding in COVID-19 Patients with Mild Severity in South Korea. Medicina. 2020; 56(12):659. https://doi.org/10.3390/medicina56120659
Chicago/Turabian StyleKim, Bongyoung, Jang Wook Sohn, Soomin Nam, Jang Won Sohn, Won Suk Choi, and Hyoung Seop Kim. 2020. "Factors Associated with the Delayed Termination of Viral Shedding in COVID-19 Patients with Mild Severity in South Korea" Medicina 56, no. 12: 659. https://doi.org/10.3390/medicina56120659