Physical Activity and Body Composition in Children and Their Mothers According to Mother’s Gestational Diabetes Risk: A Seven-Year Follow-Up Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
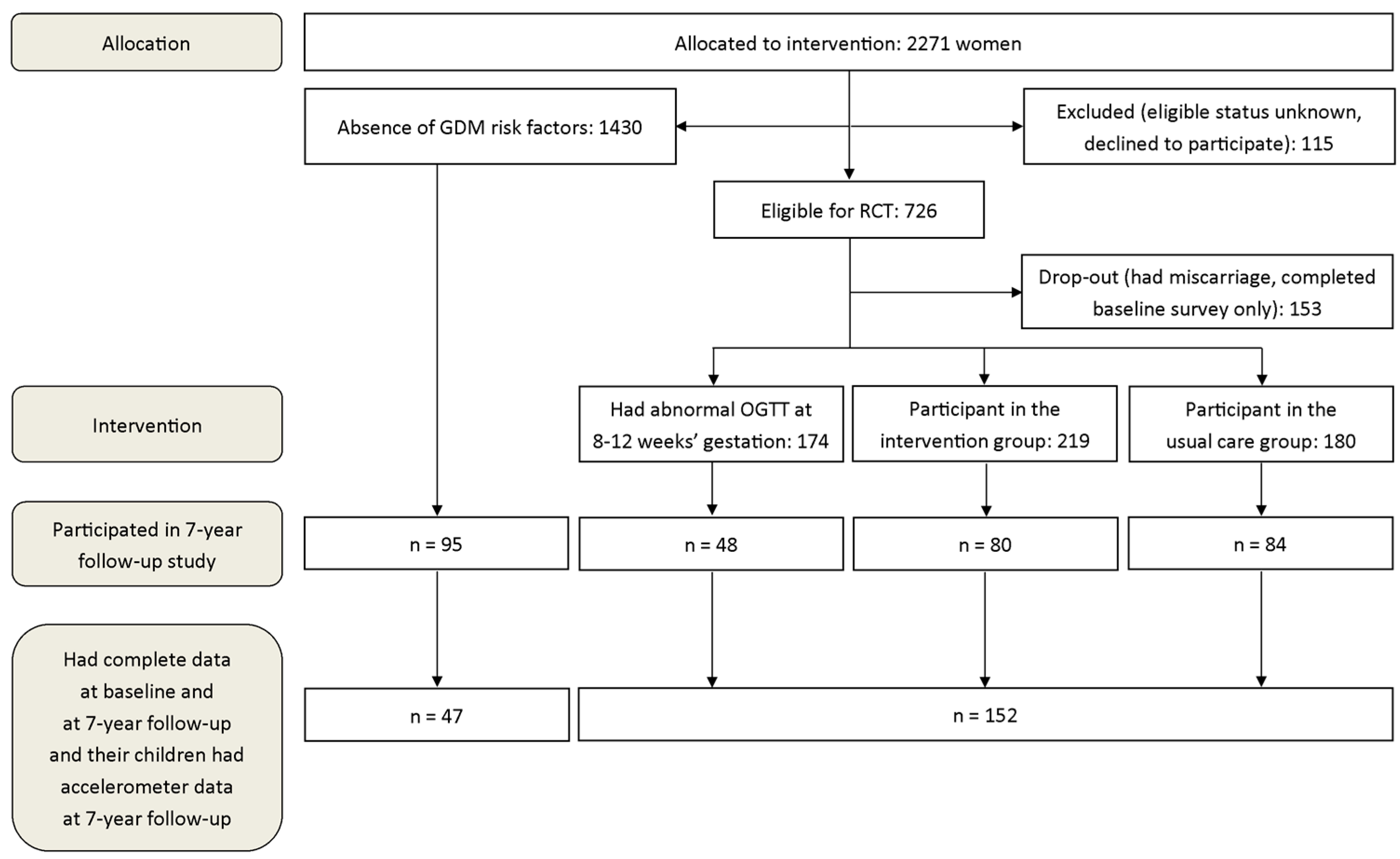
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Methods
3. Results
3.1. Change in Self-Reported PA between Baseline and Seven-Year Follow-Up
3.2. Mothers’ Measured PA at the Seven-Year Follow-Up
3.3. Children’s Measured PA and Body Composition
4. Discussion
4.1. Change in Self-Reported PA between Baseline and Seven-Year Follow-Up
4.2. Mothers’ Measured PA at the Seven-Year Follow-Up
4.3. Children’s Measured PA and Body Composition
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Gestational diabetes mellitus. Diabetes Care 2004, 27, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Bardenheier, B.H.; Imperatore, G.; Gilboa, S.M.; Geiss, L.S.; Saydah, S.H.; Devlin, H.M.; Kim, S.Y.; Gregg, E.W. Trends in gestational diabetes among hospital deliveries in 19 U.S. states, 2000–2010. Am. J. Prev. Med. 2015, 49, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Vuori, E.; Gissler, M. Perinataalitilasto—Synnyttäjät, Synnytykset ja Vastasyntyneet 2016. Available online: https://www.thl.fi/fi/tilastot/ (accessed on 15 December 2018).
- Zhang, C.; Rawal, S.; Chong, Y. Risk factors for gestational diabetes: Is prevention possible? Diabetologia 2016, 59, 1385–1390. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report 2008. Available online: https://health.gov/paguidelines/report/ (accessed on 17 September 2017).
- American College of Obstetricians and Gynecologists. Physical activity and exercise during pregnancy and the postpartum period. Obstet. Gynecol. 2015, 126, e135–e142. [Google Scholar] [CrossRef] [PubMed]
- Juhl, M.; Madsen, M.; Andersen, A.-N.; Andersen, P.K.; Olsen, J. Distribution and predictors of exercise habits among pregnant women in the danish national birth cohort. Scand. J. Med. Sci Sports 2012, 22, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Herring, A.H.; Wen, F. Self-reported and objectively measured physical activity among a cohort of postpartum women: The PIN postpartum study. J. Phys. Act. Health 2012, 9, 5–20. [Google Scholar] [CrossRef] [PubMed]
- van der Pligt, P.; Olander, E.K.; Ball, K.; Crawford, D.; Hesketh, K.D.; Teychenne, M.; Campbell, K. Maternal dietary intake and physical activity habits during the postpartum period: Associations with clinician advice in a sample of Australian first time mothers. BMC Pregnancy Childbirth 2016, 16, 27. [Google Scholar] [CrossRef]
- Gaston, A.; Cramp, A. Exercise during pregnancy: A review of patterns and determinants. J. Sci. Med. Sport 2011, 14, 299–305. [Google Scholar] [CrossRef]
- Pereira, M.A.; Rifas-Shiman, S.L.; Kleinman, K.P.; Rich-Edwards, J.W.; Peterson, K.E.; Gillman, M.W. Predictors of change in physical activity during and after pregnancy: Project viva. Am. J. Prev. Med. 2007, 32, 312. [Google Scholar] [CrossRef]
- Butte, N.F.; Puyau, M.R.; Wilson, T.A.; Liu, Y.; Wong, W.W.; Adolph, A.L.; Zakeri, I.F. Role of physical activity and sleep duration in growth and body composition of preschool-aged children. Obesity 2016, 24, 1328–1335. [Google Scholar] [CrossRef] [Green Version]
- Leppänen, M.H.; Nyström, C.D.; Henriksson, P.; Pomeroy, J.; Ruiz, J.R.; Ortega, F.B.; Cadenas-Sánchez, C.; Löf, M. Physical activity intensity, sedentary behavior, body composition and physical fitness in 4-year-old children: Results from the ministop trial. Int. J. Obes. 2016, 40, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Farrell, K.; Thomas, A.; Huston-Presley, L.; Mencin, P.; de Mouzon, S.H.; Amini, S.B. Perinatal risk factors for childhood obesity and metabolic dysregulation. Am. J. Clin. Nutr. 2009, 90, 1303–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luoto, R.M.; Kinnunen, T.I.; Aittasalo, M.; Ojala, K.; Mansikkamäki, K.; Toropainen, E.; Kolu, P.; Vasankari, T. Prevention of gestational diabetes: Design of a cluster-randomized controlled trial and one-year follow-up. BMC Pregnancy Childbirth 2010, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Luoto, R.; Kinnunen, T.I.; Aittasalo, M.; Kolu, P.; Raitanen, J.; Ojala, K.; Mansikkamäki, K.; Lamberg, S.; Vasankari, T.; Komulainen, T.; et al. Primary prevention of gestational diabetes mellitus and large-for-gestational-age newborns by lifestyle counseling: A cluster-randomized controlled trial. PLoS Med. 2011, 8, e1001036. [Google Scholar] [CrossRef] [PubMed]
- Aittasalo, M.; Raitanen, J.; Kinnunen, T.I.; Ojala, K.; Kolu, P.; Luoto, R. Is intensive counseling in maternity care feasible and effective in promoting physical activity among women at risk for gestational diabetes? secondary analysis of a cluster randomized NELLI study in Finland. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 104. [Google Scholar] [CrossRef] [PubMed]
- Aittasalo, M.; Pasanen, M.; Fogelholm, M.; Ojala, K. Validity and repeatability of a short pregnancy leisure time physical activity questionnaire. J. Phys. Act. Health 2010, 7, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Leppänen, M.; Aittasalo, M.; Raitanen, J.; Kinnunen, T.; Kujala, U.; Luoto, R. Physical activity during pregnancy: Predictors of change, perceived support and barriers among women at increased risk of gestational diabetes. Matern Child Health J. 2014, 18, 2158–2166. [Google Scholar] [CrossRef] [PubMed]
- Vähä-Ypyä, H.; Vasankari, T.; Husu, P.; Mänttäri, A.; Vuorimaa, T.; Suni, J.; Sievänen, H. Validation of cut-points for evaluating the intensity of physical activity with accelerometry-based mean amplitude deviation (MAD). PLoS ONE 2015, 10, e0134813. [Google Scholar] [CrossRef]
- Aittasalo, M.; Vaha-Ypya, H.; Vasankari, T.; Husu, P.; Jussila, A.M.; Sievanen, H. Mean amplitude deviation calculated from raw acceleration data: A novel method for classifying the intensity of adolescents physical activity irrespective of accelerometer brand. BMC Sports Sci. Med. Rehabil. 2015, 7, 18. [Google Scholar] [CrossRef]
- Tuominen, P.; Husu, P.; Raitanen, J.; Luoto, R. Differences in sedentary time and physical activity among mothers and children using a movement-to-music video program in the home environment: A pilot study. SpringerPlus 2016, 5, 1–10. [Google Scholar] [CrossRef]
- Saari, A.; Sankilampi, U.; Hannila, M.; Kiviniemi, V.; Kesseli, K.; Dunkel, L. New finnish growth references for children and adolescents aged 0 to 20 years: Length/height-for-age, weight-for-length/height, and body mass index-for-age. Ann. Med. 2011, 43, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Retnakaran, R.; Qi, Y.; Sermer, M.; Connelly, P.W.; Zinman, B.; Hanley, A.J. Gestational diabetes and postpartum physical activity: Evidence of lifestyle change one year after delivery. Obesity 2009, 18, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Ruchat, S.M.; Mottola, M.F.; Skow, R.J.; Nagpal, T.S.; Meah, V.L.; James, M.; Riske, L.; Sobierajski, F.; Kathol, A.J.; Marchand, A.A.; et al. Effectiveness of exercise interventions in the prevention of excessive gestational weight gain and postpartum weight retention: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Kujala, U.; Pietilä, J.; Myllymäki, T.; Mutikainen, S.; Föhr, T.; Korhonen, I.; Helander, E. Physical activity: Absolute intensity versus relative-to-fitness-level volumes. Med. Sci. Sports Exerc. 2017, 49, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Liu, E.; Qiao, Y.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Maternal gestational diabetes and childhood obesity at age 9–11: Results of a multinational study. Diabetologia 2016, 59, 2339–2348. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, A.D.; Fraser, A.; Lindsay, R.; Ness, A.; Dabelea, D.; Catalano, P.; Davey Smith, G.; Sattar, N.; Nelson, S.M. Association of existing diabetes, gestational diabetes and glycosuria in pregnancy with macrosomia and offspring body mass index, waist and fat mass in later childhood: Findings from a prospective pregnancy cohort. Diabetologia 2010, 53, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Castillo, H.; Santos, I.S.; Matijasevich, A. Relationship between maternal pre-pregnancy body mass index, gestational weight gain and childhood fatness at 6–7 years by air displacement plethysmography. Matern. Child Nutr. 2015, 11, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Kujala, U. Physical activity, genes, and lifetime predisposition to chronic disease. Eur. Rev. Aging Phys. Act. 2011, 8, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wen, L.M.; Rissel, C. Associations of parental influences with physical activity and screen time among young children: A systematic review. J. Obes. 2015, 2015, 546925. [Google Scholar] [CrossRef]
- Muthuri, S.K.; Onywera, V.O.; Tremblay, M.S.; Broyles, S.T.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Relationships between parental education and overweight with childhood overweight and physical activity in 9–11 year old children: Results from a 12-country study. PLoS ONE 2016, 11, e0147746. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Gregorich, S.E.; Tschann, J.M.; Penilla, C.; Pasch, L.A.; De Groat, C.L.; Flores, E.; Deardorff, J.; Greenspan, L.C.; Martinez, S.M. Longitudinal effects of parental, child and neighborhood factors on moderate-vigorous physical activity and sedentary time in latino children. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 108. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| GDMRno a (N = 47) | GDMRyes a (N = 152) | p-Value for Difference | |
|---|---|---|---|
| Characteristics at baseline | |||
| Age (years) | 29.3 (5.5) | 30.2 (4.6) | 0.26 b |
| Height (cm) | 166.6 (6.0) | 166.5 (6.6) | 0.92 b |
| Weight (kg) | 61.8 (6.6) | 74.2 (14.5) | <0.001 b |
| Body mass index, BMI (kg/m2) | 22.3 (2.0) | 26.8 (4.9) | <0.001 b |
| Education, N (%) | |||
| Academic | 13 (28.9) | 44 (28.9) | 0.96 c |
| Polytechnic | 19 (42.2) | 61 (40.1) | |
| Basic or secondary school | 13 (28.9) | 47 (30.9) | |
| Working status, N (%) | |||
| Fulltime | 30 (63.8) | 94 (61.8) | 0.81 c |
| Part-time, unemployed, student, maternity leave | 17 (36.2) | 58 (38.2) | |
| Marital status, N (%) | |||
| Married | 46 (97.9) | 148 (97.4) | 0.85 c |
| Not married | 1 (2.1) | 4 (2.6) | |
| Number of children in the home, N (%) | |||
| 0 | 22 (46.8) | 69 (45.7) | 0.89 c |
| 1+ | 25 (53.2) | 82 (54.3) | |
| GDM risk factors, N (%) | |||
| Age ≥ 40 years | - | 3 (2.0) | |
| Pre-pregnancy BMI ≥25 kg/m² | - | 95 (62.5) | |
| Newborn’s macrosomia e | - | 4 (2.6) | |
| GDM or signs of glucose intolerance | - | 22 (14.5) | |
| Family history of diabetes | - | 88 (57.9) | |
| Number of GDM risk factors, N (%) | |||
| 1 | - | 97 (63.8) | |
| 2 | - | 50 (32.9) | |
| 3+ | - | 5 (3.3) | |
| Self-reported PA (min/week) | |||
| LPA | 197.1 (216) | 182.8 (235) | 0.56 d |
| MVPA | 179.2 (133) | 195.2 (201) | 0.88 d |
| Total PA | 376.3 (288) | 378.0 (330) | 0.96 d |
| Characteristics at the seven-year follow-up | |||
| Age (years) | 37.0 (5.5) | 37.8 (4.6) | 0.34 b |
| Weight (kg) | 63.6 (7.2) | 77.7 (15.8) | <0.001 b |
| Body mass index, BMI (kg/m2) | 22.9 (2.6) | 28.1 (5.7) | <0.001 b |
| Working status, N (%) | |||
| Fulltime | 21 (44.7) | 101 (66.4) | 0.007 c |
| Part-time, unemployed, student, maternity leave | 26 (55.3) | 51 (33.6) | |
| Marital status, N (%) | |||
| Married | 38 (80.9) | 120 (78.9) | 0.78 c |
| Not married | 9 (19.1) | 32 (21.1) | |
| Number of children in the home, N (%) | |||
| 1 | 5 (10.6) | 15 (10.0) | 0.90 c |
| 2+ | 42 (89.4) | 135 (90.0) | |
| Self-reported PA (min/week) | |||
| LPA | 295.5 (207) | 212.1 (193) | 0.005 d |
| MVPA | 206.3 (179) | 161.9 (120) | 0.33 d |
| Total PA | 501.7 (319) | 373.9 (234) | 0.012 d |
| Accelerometer-based PA (% of awake wear time/day) | |||
| SB | 71.2 (7.9) | 73.9 (6.1) | 0.042 d |
| LPA | 18.6 (5.0) | 16.8 (4.1) | 0.029 d |
| MVPA | 10.1 (3.9) | 9.2 (2.9) | 0.25 d |
| Children’s characteristics, N (boys %) | 47 (55.3) | 152 (53.3) | |
| Age (years) | 6.6 (0.5) | 6.5 (0.6) | 0.33 b |
| Height (cm) | 122.7 (5.5) | 123.0 (6.0) | 0.82 b |
| Height for age z-score f | 0.11 (0.9) | 0.37 (1.1) | 0.18 b |
| Weight (kg) | 24.2 (3.6) | 24.7 (4.8) | 0.82 d |
| Weight for age z-score f | 0.05 (0.9) | 0.23 (1.0) | 0.31 b |
| BMI (kg/m2) | 16.0 (0.2) | 16.2 (0.2) | 0.56 b |
| Overweight or obese f | 6 (14.6) | 31 (21.8) | 0.31 c |
| Accelerometer-based PA (% of awake wear time/day) | |||
| SB | 59.0 (5.4) | 58.3 (5.9) | 0.50 d |
| LPA | 23.1 (3.5) | 22.9 (3.2) | 0.61 d |
| MVPA | 17.8 (3.3) | 18.8 (4.1) | 0.19 d |
| Light-Intensity PA c | MVPA c | Total PA c | |
|---|---|---|---|
| B (95% CI) | B (95% CI) | B (95% CI) | |
| GDMRno a, unadjusted, N = 199 | 69.0 (−19.4, 157) | 60.5 (−2.15, 123) | 130 (18.6, 240) * |
| GDMRno, adjusted b, N = 195 | 88.2 (20.0, 156) * | 41.0 (−6.46, 88.4) | 130 (41.9, 217) ** |
| Age | −8.93 (−14.9, −2.92) ** | −3.20 (−7.37, 0.98) | −11.8 (−19.6, −4.08) ** |
| Pre-pregnancy BMI | 4.02 (−1.97, 10.0) | −1.81 (−6.02, 2.39) | 2.48 (−5.28, 10.2) |
| Education (Reference basic or secondary school) | |||
| Polytechnic | 25.3 (−40.0, 90.7) | 39.9 (−6.58, 84.6) | 60.9 (−23.7, 146) |
| Academic | 13.2 (−59.0, 85.4) | 28.8 (−21.3, 78.8) | 41.9 (−51.0, 135) |
| Working status (Reference full day) | |||
| Part-time, student, unemployed, maternity leave | 12.4 (−47.8, 72.5) | 6.22 (−34.7, 47.1) | 13.3 (−63.6, 90.3) |
| Children in the home (Reference at least one) | |||
| Not at all | −75.1 (−135, −14.9) * | 16.8 (−23.6, 57.3) | −63.9 (−140, 12.4) |
| Sedentary Behavior | Light-Intensity PA c | MVPA c | |
|---|---|---|---|
| B (95% CI) | B (95% CI) | B (95% CI) | |
| GDMRno a, unadjusted, N = 199 | −2.68 (−4.84, −0.53) * | 1.78 (0.36, 3.21) * | 0.90 (−0.14, 1.94) |
| GDMRno, adjusted b, N = 195 | −0.57 (−2.90, 1.76) | 0.40 (−1.12, 1.91) | 0.17 (−1.02, 1.36) |
| Age | 0.03 (−0.17, 0.23) | −0.03 (−0.15, 0.10) | −0.001 (−0.10, 0.10) |
| Current BMI | 0.20 (0.03, 0.37) * | −0.11 (−0.22, 0.00) | −0.09 (−0.18, −0.01) * |
| Education (Reference basic or secondary school) | |||
| Polytechnic | 1.62 (−0.55, 3.80) | −0.90 (−2.31, 0.51) | −0.72 (−1.83, 0.38) |
| Academic | 4.25 (1.83, 6.66) *** | −2.99 (−4.56, −1.42) *** | −1.26 (−2.48, −0.30) * |
| Working status (Reference full day) | |||
| Part-time, student, unemployed, maternity leave | −2.03 (−3.97, −0.10) * | 1.74 (0.49, 3.00) ** | 0.29 (−0.69, 1.27) |
| Children in the home (Reference at least two) | |||
| One | −1.24 (−4.18, 1.71) | 0.77 (−1.15, 2.69) | 0.47 (−1.04, 1.96) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leppänen, M.H.; Raitanen, J.; Husu, P.; Kujala, U.M.; Tuominen, P.P.; Vähä-Ypyä, H.; Luoto, R. Physical Activity and Body Composition in Children and Their Mothers According to Mother’s Gestational Diabetes Risk: A Seven-Year Follow-Up Study. Medicina 2019, 55, 635. https://doi.org/10.3390/medicina55100635
Leppänen MH, Raitanen J, Husu P, Kujala UM, Tuominen PP, Vähä-Ypyä H, Luoto R. Physical Activity and Body Composition in Children and Their Mothers According to Mother’s Gestational Diabetes Risk: A Seven-Year Follow-Up Study. Medicina. 2019; 55(10):635. https://doi.org/10.3390/medicina55100635
Chicago/Turabian StyleLeppänen, Marja H, Jani Raitanen, Pauliina Husu, Urho M Kujala, Pipsa PA Tuominen, Henri Vähä-Ypyä, and Riitta Luoto. 2019. "Physical Activity and Body Composition in Children and Their Mothers According to Mother’s Gestational Diabetes Risk: A Seven-Year Follow-Up Study" Medicina 55, no. 10: 635. https://doi.org/10.3390/medicina55100635