Effects of Fish n-3 PUFAs on Intestinal Microbiota and Immune System


Department of Pharmacological and Biomolecular Sciences, Università degli Studi di Milano, 20122 Milano, Italy
Mar. Drugs 2019, 17(6), 374; https://doi.org/10.3390/md17060374
Submission received: 7 May 2019
/
Revised: 13 June 2019
/
Accepted: 20 June 2019
/
Published: 22 June 2019
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Studies over several decades have documented the beneficial actions of n-3 polyunsaturated fatty acids (PUFAs), which are plentiful in fish oil, in different disease states. Mechanisms responsible for the efficacy of n-3 PUFAs include: (1) Reduction of triglyceride levels; (2) anti-arrhythmic and antithrombotic effects, and (3) resolution of inflammatory processes. The human microbiota project and subsequent studies using next-generation sequencing technology have highlighted that thousands of different microbial species are present in the human gut, and that there has been a significant variability of taxa in the microbiota composition among people. Several factors (gestational age, mode of delivery, diet, sanitation and antibiotic treatment) influence the bacterial community in the human gastrointestinal tract, and among these diet habits play a crucial role. The disturbances in the gut microbiota composition, i.e., gut dysbiosis, have been associated with diseases ranging from localized gastrointestinal disorders to neurologic, respiratory, metabolic, ocular, and cardiovascular illnesses. Many studies have been published about the effects of probiotics and prebiotics on the gut microbiota/microbioma. On the contrary, PUFAs in the gut microbiota have been less well defined. However, experimental studies suggested that gut microbiota, n-3 PUFAs, and host immune cells work together to ensure the intestinal wall integrity. This review discussed current evidence concerning the links among gut microbiota, n-3 PUFAs intake, and human inflammatory disease.
1. Introduction
Polyunsaturated fatty acids (PUFAs) are important constituents of the phospholipids of all cell membranes, where they play roles assuring the correct environment for membrane protein function, maintaining membrane fluidity, regulating cell signaling, gene expression and cellular function, and serving as substrates for the synthesis of lipid mediators. The fatty acid composition of inflammatory cells can be modified by increasing intake of marine n-3 PUFAs, which leads to a higher content of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) [1]. These changes in membrane phospholipid fatty acid composition might be expected to influence the function of cells involved in inflammation through: (1) Alterations of the membrane fluidity and raft structure; (2) effects on cell signalling pathways; and (3) alterations in the pattern of the lipid mediators produced [2].
Chronic inflammatory disease, such as atherosclerosis, nonalcoholic fatty liver disease (NAFLD) [3], chronic obstructive pulmonary disease (COPD) [4], inflammatory bowel disease (IBD) [5], and retinal illnesses [6], are responsible of pain, impaired function, and diminished quality of life, as well as, the associated high health-care costs and loss of productivity [7].
The human gut microbiota has become a widely discussed topic over the past decade. The intestinal microbial community lives in a mutualistic relationship with its host and is a key contributor to host metabolism. There is mounting evidence from the literature that brought to the forefront the impact of mutualistic bacterial communities of the gut microbiota on human health. Each person’s microbiome is unique, rapidly developing throughout early childhood and with differing rates of variability in adulthood. Microbial colonization runs in parallel with immune system maturation and plays a role in intestinal physiology and regulation [8]. Moreover, the network of mucosal immune cells and intestinal epithelium acts in concert to enforce barrier function, prevent mucosal infections and maintain a symbiotic relationship with the commensal flora. The disruption of this balance, whether due to genetic or environmental insults, is now recognized for having important and far-reaching impacts on immune tolerance and hypersensitivity in intestinal and extra-intestinal tissues, including the liver, the lung, the eyes, and the central nervous system [9].
Both genetic and environmental factors, including diet, geographical location, toxin/carcinogen exposure, and hormones, can influence variations in gut microbial composition [10]. The western lifestyle, including over-feeding of highly refined diets and sedentary behavior, is associated with systemic low-grade inflammation, responsible for chronic degenerative disease.
This review describes the connections among gut microbiota, n-3 PUFAs intake, and IBD or retinal disease.
2. Fish n-3 PUFAs
In recent years, much focus has been placed on the beneficial effects of fish consumption strengthened by the concept that the ocean offers a wonderful resource for novel compounds. Many of the positive effects of fish, including those on dyslipidemia and heart disease, have been attributed to n-3 PUFAs, i.e., EPA and DHA. However, in addition to n-3 PUFAs, other nutrients, such as minerals, vitamins and proteins, [11] have been associated to the prevention/treatment of cardiovascular (CV) disease and associated health complications [1,12,13,14]. Indeed, in a recent experimental study, krill oil (a sustainable source of EPA and DHA) and krill proteins proved to be effective in lowering atherosclerosis development in apoE deficient mice [15]. Krill oil seems to exert this effect mainly by interfering with cholesterol synthesis, whereas krill protein may affect atherosclerosis development by supplying nitric oxide (NO) through arginine [16], thus preserving endothelial function, and, possibly, through the release of atheroprotective peptides [17].
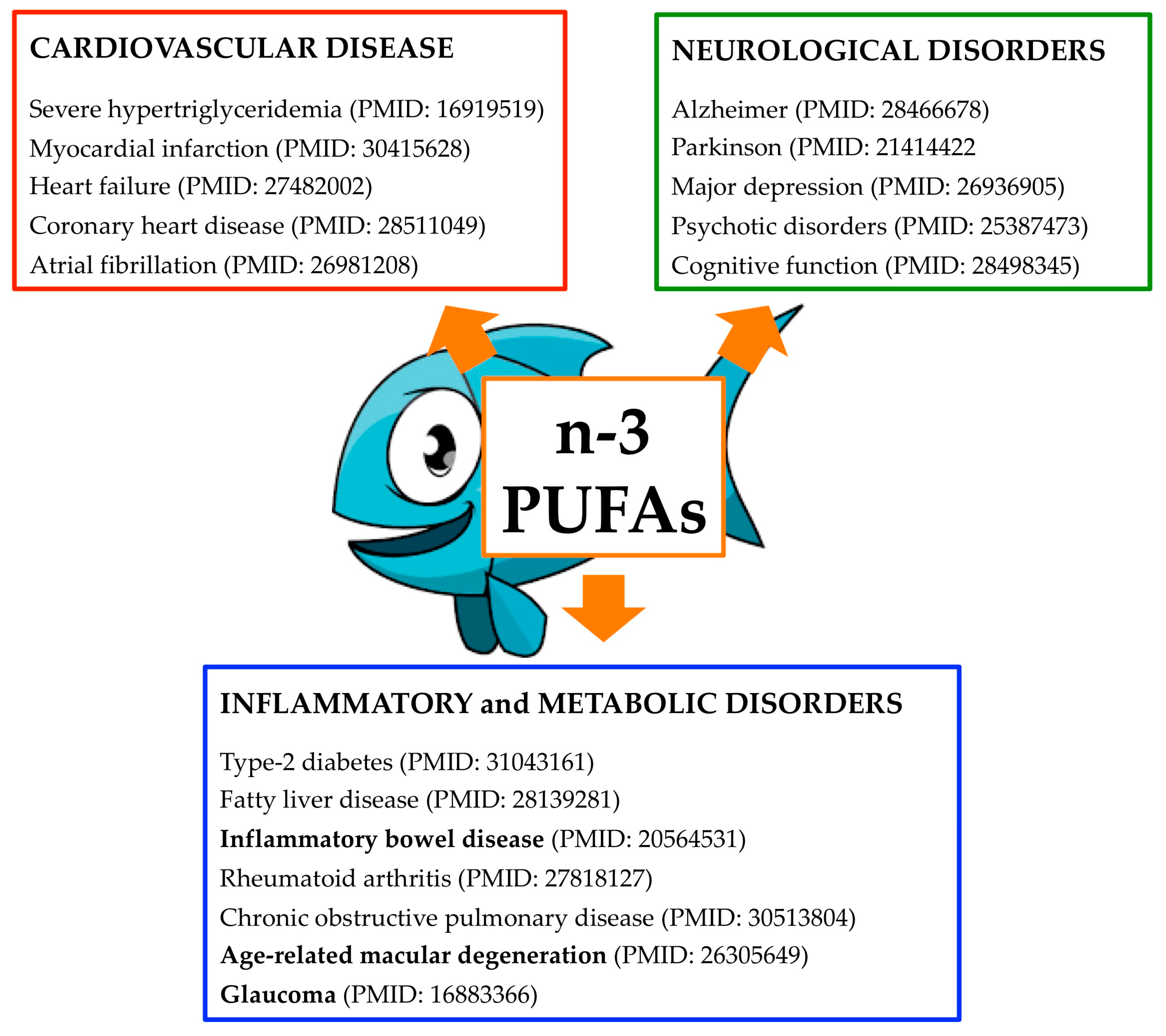
EPA and DHA are concentrated in fatty fish and marine mammals and these are the main source in the eastern diet. n-3 PUFAs are also commercially available as dietary supplements in the form of oil and capsules. In 2008, the US Food and Drug Administration (FDA) have formally stated that consumption of up to 3 g/d of marine-based n-3 PUFAs is generally regarded as safe. In line with this health claim, fish consumption is recommended in the 2015–2020 Dietary Guidelines for Americans and by the American Heart Association (Figure 1) [18].
Clinical complications of atherosclerosis like myocardial infarction, stroke and peripheral arterial disease still represent the leading cause of mortality and morbidity in the world [9,19]. Among patients who are receiving appropriate treatment with statins, the rates of CV events remain high [20,21]. In addition, recent genetic [22,23,24] and Mendelian randomization studies [25,26] have highlighted triglyceride levels as an independent risk factor for the incidence of ischemic events. Therefore, there is renewed interest in targeting triglycerides aiming at reducing the residual cardiovascular risk [21]. Lifestyle modification remains the starting point of therapy for the hypertriglyceridemia, followed by fibrates and n-3 PUFAs administration [27].
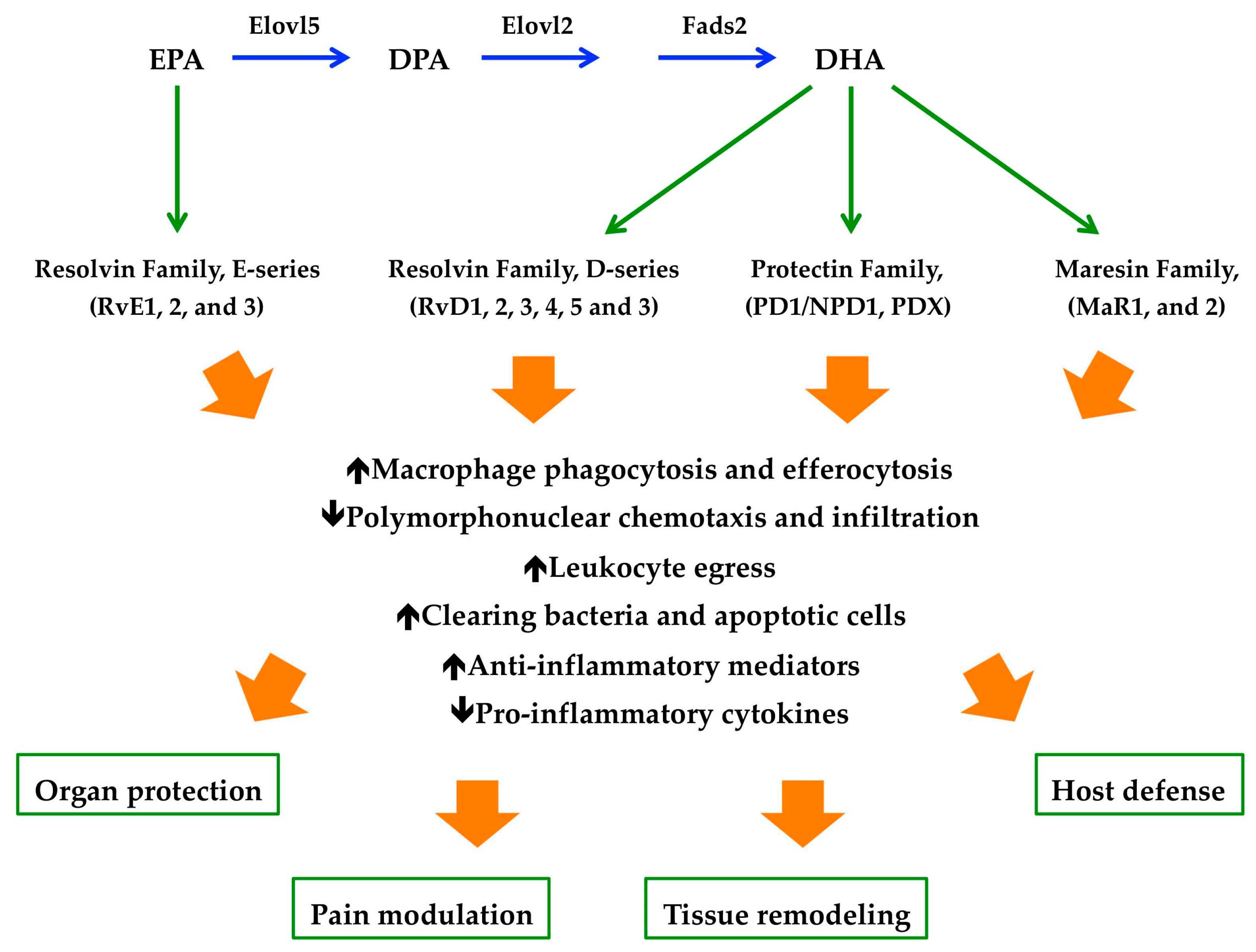
While earlier studies on CV outcomes demonstrated favorable effects of n-3 PUFAs [28,29], subsequent clinical trials evaluating the impact of EPA (20:5n-3) and DHA (22:6n-3) administration, alone or in combination, failed to confirm the previous results [30,31,32]. These considerations led to the design of the prospective, randomized, double-blind Reduction in Cardiovascular Events with EPA-Intervention Trial (REDUCE-IT) assessing the ability of icosapent ethyl to reduce CV outcomes in high-risk statin-treated patients with triglyceride levels of at least 500 mg/dL [33,34]. In this study, the risk of both primary (25%) and secondary (26%) composite end points was significantly lower among patients treated with 2 g of icosapent ethyl than among those in the placebo group [35]. The overall rates of adverse events leading to discontinuation of trial were similar in both the clinical groups. However, serious adverse events, i.e., bleeding and the rate of hospitalization for atrial fibrillation or flutter, were observed with higher frequency among patients in the icosapent ethyl group. The authors suggested that the observed reduction in the risk of ischemic events caused by icosapent ethyl administration may be explained by metabolic effects other than a reduction of triglyceride levels, i.e., antithrombotic, membrane-stabilizing, plaque stabilizing and anti-inflammatory mechanisms [36,37,38,39]. It is known that, n-3 PUFAs, being natural agonists of GPR120 (also called free fatty acid receptor 4) [40], attenuate NF-κB activation and stimulate PPARs, resulting in the reduced production of prostaglandin E2 (PGE2), TNF-α, interleukin 6 (IL-6), IL-1β, soluble E selectin, and high-sensitivity C-reactive protein [41,42]. In addition, n3-PUFAs also act as substrates for the synthesis of specialized pro-resolving mediators (SPMs), i.e., resolvins (short for resolution phase interaction products), protectins, and maresins (short for macrophage mediators in resolving inflammation) [43], reducing the inflammatory circuits of atherosclerosis [44]. These SPMs, upon activation of specific receptors, actively terminate the inflammatory reactions by increasing efferocytosis, phagocytosis and leukocytes egress (Figure 2) [45].
In line with these data, a recent study provided a link among EPA supplementation, the generation of SPM’s precursors, and their signaling pathways in the context of cardiovascular disease [46]. Specifically, the authors identified 18-HEPE as a plasma biosynthetic pathway marker of EPA supplementation, and characterized the receptor for the 18-HEPE–derived lipid mediator RvE1, i.e., ERV1/ChemR23, as a key player in atherosclerosis. The targeted deletion of Erv1/Chemr23 in 2 independent hyperlipidemic murine models was instead associated with proatherogenic signaling in macrophages, increased oxLDL uptake, reduced phagocytosis, and increased atherosclerotic plaque size and necrotic core formation. Moreover, a specific ERV1/ChemR23–expressing macrophage subtype was detected near the necrotic core into the human atherosclerotic lesions and its gene expression was increased in the plaques harvested from patients receiving statins [46,47].
The ongoing (VITAL, NCT01169259) placebo-controlled trial, designed to examine major CV events, might clarify the utility of Lovaza, a drug formulation containing ethyl ester of EPA (465 mg) and DHA (375 mg), in primary prevention of CV disease [48]. The randomized trial for evaluation in secondary prevention efficacy of combination therapy–statin and EPA (RESPECT-EPA, UMIN000012069), a study involving statin-treated patients in Japan, and the effect of Vascepa (a preparation of EPA as ethyl ester) on improving coronary atherosclerosis in people with high triglyceride levels taking statin therapy trial (EVAPORATE, NCT02926027), which is examining changes in coronary plaque over 9 to 18 months, will provide further information on the effects of these agents. In addition, the statin residual risk reduction with Epanova in hiGh cardiovascular risk patients with hypertriglyceridemia (STRENGTH NCT02104817) is an ongoing trial that will be exploring residual cardiovascular risk reduction with 4 g daily of EPA/DHA (Epanova) versus corn oil in patients on statin therapy.
Finally, it is should be noted that n-3 PUFAs have dramatically modified the biochemical composition of the lipid rafts, i.e., the dynamic sphingolipid-cholesterol enriched regions of the membrane that concentrate specific signaling proteins [49]. These lipid microdomanins play a crucial role in the CD4+ T cell activation and differentiation, and downstream in the B cell activity [50]. Several in vitro and in vivo data have shown that n-3 PUFAs displaced many of the signaling proteins necessary for CD4+ T cell activation [51]. In addition, n-3 PUFAs suppressed CD4+T cell polarization into Th1 and Th17 cells, probably by altering the IL-6/gp130/STAT3 pathway [52]. On the other hand, n-3 PUFAs or SPMs boosted humoral immunity by influencing B cell development in the bone marrow, B cell activation and antibody production in response to antigen [53]. Although these data need to be confirmed and the underlying mechanisms better clarified, it can be speculated that n-3 PUFAs may contribute in the attenuation of autoimmune and chronic inflammatory disease [51].
3. The Gut Microbiota
The gastrointestinal (GI) tract is a passage formed by mucosa, submucosa, and smooth muscle containing a huge network of nerves and blood vessels. The mucosa is responsible for: Digestion and absorption of nutrients from the diet; protection of the body against physical and chemical damage from luminal contents; and supply of immunity [54,55]. The small intestinal epithelium, the single cell layer that forms the luminal surface, is folded to form villi and crypts. Both these structures serve to increase the total absorption surface of the intestine. Moreover, in the mucosa different types of cells are present, such as enterocytes (the main cellular component accounting for about 80%), Paneth, goblet, and enteroendocrine (comprise just 1% of the epithelium) [56]. Enteroendocrine cells, distributed throughout the GI tract, form a large endocrine organ that control: (1) GI secretion and motility; (2) regulation of food intake; (3) postprandial glucose levels; and (4) direct communication with neurons innervating the GI tract (these cells are part of the gut brain axis) [57].
The mammalian intestine is colonized by a complex community of microorganisms, called microbiota, constituted by bacteria (approximately 4 × 1013), archaea, viruses (especially bacteriophages), protozoans and fungi [58]. Shotgun metagenomic sequencing through random sequencing of all genes established that the human gut possesses a bacterial microbiome that is predominated by phyla, such as Firmicutes, Bacteroidetes, Actinobacteria, Proteobacteria, Verrucomicrobia. Firmicutes and Bacteroidetes represent 90% of the gut microbiota [9]. It is important to remember that the colonization of the human gut starts prenatally and continues after birth, reaching the adult microbiota state between the ages of 2 and 5 years [59]. Following birth, diverse microbes colonize the human intestine, and several factors are known to affect this process, i.e., gestational age, mode of delivery, diet (breast milk vs formula), sanitation and antibiotic treatment [60]. Several studies showed a positive correlation between human milk oligosaccharides and the number of Bifidobacterium demonstrating that milk oligosaccharides have a probiotic effect by stimulating the development of Bifidobacterium-rich microbiota [61]. Furthermore, in addition to proteins, fats, carbohydrates and endocannabinoids, human breast milk contains immunoglobulins (IgA and IgG), antimicrobial compounds (lysozyme and lactoferrin), immune-regulatory cytokines (e.g. TGF-β and IL-10), and lymphocytes that express gut homing markers [62,63]. Altogether these data indicate that intestinal bacterial colonization dramatically influence the development of the host immune system in early life and affects health and disease in later life, as indicated by the loss of immune function in germ-free (GF) mice [63,64,65].
A significant change in the gut microbiota composition accompanies the weaning from the mother and the introduction of solid foods, with enhanced colonization of butyrate producers, including Bacteroides and certain Clostridium species [66]. Once established, the composition of the gut microbiota is relatively stable throughout adult life in the absence of perturbations such as long-term dietary changes, disease-associated dysbiosis, or the use of antibiotics. However, centenarian’s microbiota showed decreased levels of Bacteroides, Bifidobacterium and Enterobacteriaceae, while Clostridium species levels were increased compared with younger adults. For these reasons, dietary-intervention studies are warranted to investigate whether changing the dietary pattern of elderly individuals can alter their gut microbiota in a way that is beneficial to their general health [67].
The Gut Microbiota and the Immune System
A noticeable example of the symbiotic effects of the microbiome is the immune system, whose normal development and behavior are strongly influenced by microbial metabolites that are produced by: (i) Bacteria from dietary components; (ii) the host and biochemically modified by gut bacteria; and (iii) by gut microbes. In this context, a complex interplay between the local microbiota, the intestinal epithelium and the resident immune cells has begun to emerge, in which all participants actively foster GI homeostasis [9]. Segmented filamentous bacteria are best known for their ability to induce the differentiation of naïve T cells to form antigen-specific Th17 cells in the ileum of mice [68] and humans [69]. Th17 cells play a critical role in host defense against extracellular pathogens (i.e., fungi and extracellular bacteria [70]) and tissue homeostasis (i.e., promoting epithelial barrier functions [71]) but can induce autoimmunity [72]. The mechanisms implicated in the balance between ‘pathogenic’ and ‘non-pathogenic’ Th17 cell states are still unknown. However, treatment of non-pathogenic Th17 cells with IL-23 converts them into a pathogenic phenotype, suggesting that IL-23 is a cytokine that drives the functional phenotype of Th17 cells [73]. Furthermore, the metabolic relationship between diets and immune cells in the gut has been strengthened by the finding that short chain fatty acids (SCFAs) promoted B cell metabolism [74] and the development and function of colonic regulatory T (Treg) cells [75]. Treg cells have played a role of gatekeeper of commensal tolerance by the immune system, through suppression of aberrant T cell responses. A balance between Th17 and Treg cell differentiation has been demonstrated [76]. Beyond SCFAs, gut microbiota have produced several additional immunologically important metabolites from food components. Dietary tryptophan, for instance, is processed to different indole derivatives, which can act as ligands for the aryl hydrocarbon receptor (AhR) [77], a ligand-activated transcription factor which plays a crucial role in the development of multiple tissues. In the intestinal mucosa, AhR is required for postnatal maintenance of Group 3 innate lymphoid cells (ILC3s) producing IL-22, as well as for the formation of isolated lymphoid follicles [9]. IL-22 is a cytokine that supports the integrity of the intestinal mucosa by inducing the secretion of antimicrobial peptides from epithelial cells, the production of mucins and the proliferation of intestinal goblet cells [78]. Highly reactive polyamines, i.e., putrescine, spermidine and spermine, derive from arginine by the action of gut microbiota, are involved in the development and maintenance of the intestinal mucosa and resident immune cells [79]. In addition, arginine itself is an important modulator of the immunometabolism of macrophages and T cells, and thus affects their effector functions [80]. Moreover, free taurine generated by deconjugation of primary bile acids [81] can promote the activation of the NLRP6 inflammasome and the production IL-18, supporting epithelial barrier function and maintenance [82]. In addition, bile acids are able to downregulate the expression of pro-inflammatory cytokines from monocytes, macrophages, dendritic cells and Kupffer cells [9].
On the other hand, a deficit of vitamin B1 is responsible for the reduction in the number of naïve B cells in Peyer’s patches, due to their dependence on this Krebs cycle cofactor, but has a neutral effect on IgA+ plasma cells present in the lamina propria [83].
4. Human Disease, n-3 PUFAs and Gut Microbiota
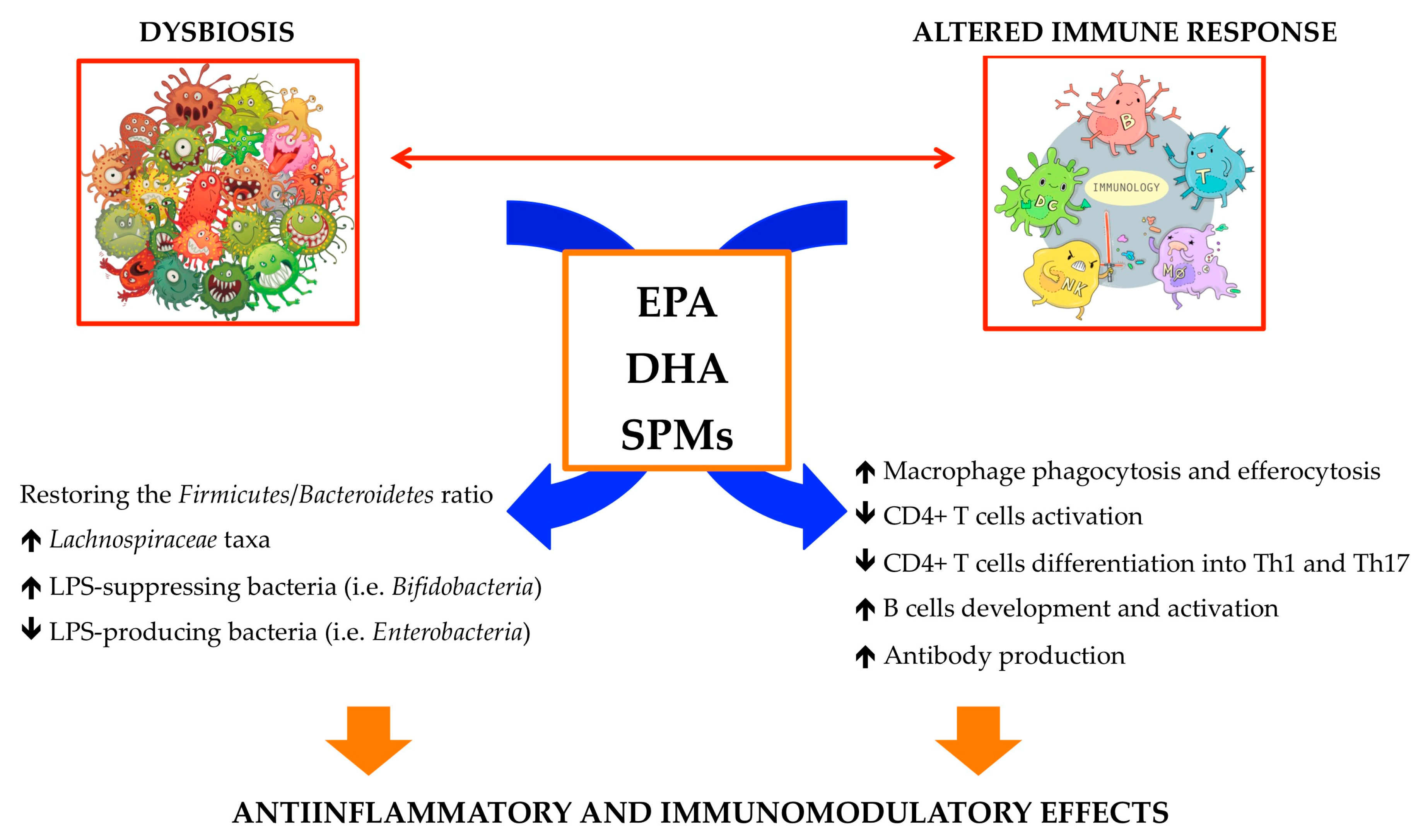
Inflammation seems to be the common denominator among the above described seemingly unrelated biological entities, i.e., the gut microbiome, the immune system, and n-3 PUFAs. Inflammation is currently accepted to play a key role in the progression of several chronic diseases, such as atherosclerosis, inflammatory bowel disease, cancer, diabetes, neurodegenerative syndromes, etc. [9]. In addition, as above described several evidences support the role of both the microbiota and the n-3 PUFAs in regulating inflammation and the immune system [45,52,74]. Moreover, dietary n-3 PUFAs, affecting gut integrity, have been shown to reduce clinical colitis and colonic immunopathology by improving epithelial barrier function in animal models [84]. Indeed, in clinical studies n-3 PUFAs have demonstrated the ability of: (i) Decreasing the Firmicutes/Bacteroidetes ratio; (ii) decreasing the levels of Coprococcus and Facecalibacterium; (iii) increasing the abundance of butyrate-producing bacterial genera, i.e., Bifidobacterium, Lachnospira, Roseburia and Lactobacillus [85,86,87]. These data were in line with those obtained in a subsequent study where the authors also found a significant correlation between n-3 PUFAs plasma levels and SCFA-producing bacteria, i.e., Lachnospiraceae family [85]. In addition, a diet supplemented with n-3 PUFAs was able to prevent neuropsychiatric disorders and dysbiosis induced by social instability stress during adolescence, and these effects were maintained through adulthood [88,89] supporting the concept that a healthy diet may have long-lasting beneficial effects and help fight off neurodegenerative diseases. Altogether these data allow hypothesizing a link among n-3 PUFAs intake, gut microbiome shaping and immune system modulation with the final common aim of hampering inflammatory-based disease (Figure 3). Accordingly, this review will particularly focus on the recent studies regarding the therapeutic potential of the combination between fish n-3 PUFAs and probiotic/prebiotic in the IBD and retinal disease.
4.1. Inflammatory Bowel Disease
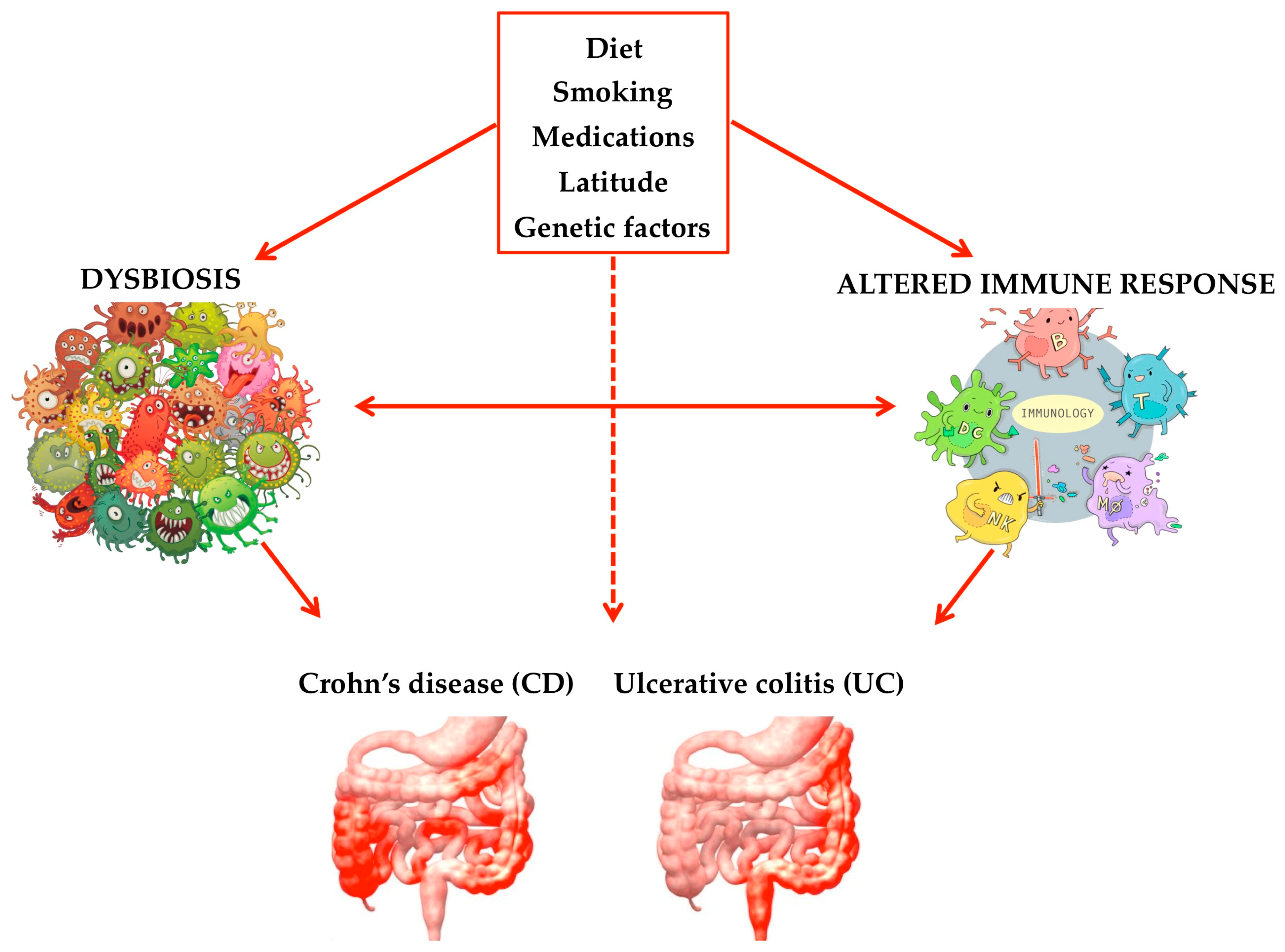
IBD, specifically Crohn’s disease (CD) and ulcerative colitis (UC), are relapsing and remitting inflammatory diseases of the GI tract without a clear etiology. The symptoms include abdominal pain, diarrhea, weight loss, ulceration, perforation, and bowel obstruction. Although the all picture of the pathogenesis of IBD remains unclear, aberrations in genetics, imbalances in the gut microbiome, dietary and lifestyle factors such as cigarette smoking, medications, and environmental triggers (i.e., geographical location and social status) are all believed to play a role in the disease’s development (Figure 4).
Genome-wide association studies (GWAS) have identified 242 loci associated to the presence of IBD [5,90]. For example, variants at the NOD2 and CDH1 loci confer the largest increase in relative risk of IBD and have been associated to UC, respectively [91,92,93]. The NOD2 gene encodes a protein that is activated within the cytoplasm of macrophages and dendritic cells by bacterial ligands [94], whereas CDH1 gene has a critical role in cell-cell adhesion and is also required for epithelial cell tight junction formation [95]. Moreover, a meta-analysis revealed that genetic variations in TLR4 gene, the receptor for LPS, conferred a statistically significant risk of developing CD and UC [96,97]. In addition, polymorphisms in TLR2, the main receptor for gram-positive bacteria, have been associated with IBD in humans and there is an inflammation-dependent induction of TLR2 expression in intestinal macrophages [98].
The hyper-responsiveness of T cells toward non-pathogenic antigens could represent one of the possible etiologies for IBD. The presence of antibodies against commensal microbial antigens and autoantigens, such as anti-Saccharomyces cerevisiae, and anti-Pseudomonas fluorescens-associated sequence 12 [99,100,101], has been associated to dysbiosis and loss of microbiota responsible for the gut mucus barrier integrity. Since it has been shown that colitis-prone genetically predisposed GF mice colonized by IBD-associated-microbiota developed severe colitis compared to those that were colonized by healthy human microbiota, it can be hypothesized that gut dysbiosis contributes to IBD pathogenesis [102]. Together, these findings strongly indicate a bidirectional relationship between such diseases and gut dysbiosis, in which dysbiosis potentially contributes to the onset of IBD and also serves as a secondary consequence of gut inflammation [103,104].
It is well known that the microbiota and the gut have a symbiotic relationship: The human host supplies the nutrients needed for the survival of the microbes, and these latter protect the host against pathogens, and act as regulatory factors of the immune responses [56]. An aberrant mucosal immune system and irregular mucosal epithelium with increased intestinal permeability (IP) may permit the translocation of bacterial-derived toxins causing gut inflammation. The communication between the gut microbiota system and all the organs of the human body is regulated by the IP [105,106]. Indeed, IP degree is very changeable and results from the interconnection between several factors: Type of diet; gene expression; intestinal/liver pathology; surface mucus; integrity of tight junctions; and production of immunoglobulins [107]. Several investigators detected a decrease of several protective bacteria (i.e., Fecalibacterium prausnitzii, Clostridium clusters IV and XIVa, some Bacteroides species, Bifidobacterium) and an increase of harmful bacteria (i.e., adherent-invasive Escherichia coli, Fusobacterium, Campylobacter concisus, Enterohepatic Helicobacter, Clostridium difficile, Veillonella) in IBD patients [108,109].
Several mechanisms are responsible for the intestinal inflammation caused by the consumption of high-fat diets (HFDs), including both changes in the intestinal barrier and composition of the intestinal microbiota. Experimental and clinical data indicated a direct correlation between plasma endotoxin levels and dietary fat intake, which suggested an increase of the IP [110,111] due to the decrease of epithelial tight junction proteins, such as occludin. Indeed, several experimental studies showed a dramatic decrease of intestinal occludin expression associated to the administration of a HFD [112,113,114]. On the other hand, high consumption of carbohydrates, such as glucose, sucrose, lactose, or fructose, overwhelms absorptive mechanisms of the intestine, resulting in high luminal sugar concentrations used by the microbiota as an energy source [115]. In support of this hypothesis, consumption of a high sugar diet was demonstrated to promote intestinal dysbiosis, the expansion of harmful bacteria (such as, Ruminococcus torques, Bacteroides, Prevotella), increased IP and inflammation [116,117]. In contrast, a fish-oil based diet has been associated with Lactobacillus and Akkermansia muciniphila blooming, and reduced gut inflammation [118,119]. The observed increase in the abundance of Akkermansia muciniphila could be a paradox because this is a mucin-user bacterium and at the same time, it is crucial for the maintenance of the mucus layer integrity [120]. However, this latest effect appeared to be more significant as proved by the fact that increased intestinal levels of Akkermansia muciniphila has been associated to a mucus layer thickening and a reduction of IP [121].
Recently, the treatment for IBD has made progress from simply controlling symptoms to modifying the course of the disease by achieving and maintaining remission which is defined as complete mucosal healing and normalization of blood markers, as well as disappearance of symptoms [122]. However, the development of a safer and more effective novel treatment for IBD is in great need.
The role of gut microbiota in colitis development was confirmed by using animal models. GF mice displayed minimal inflammation or delayed onset of chemically and genetically induced colitis compared to the conventionally raised (CONV-R) animals [123,124,125]. However, higher mortality was seen in GF than CONV-R mice after giving dextran sulfate sodium (DSS), due to massive gut epithelial injury [126]. The seemingly paradoxical phenomenon could be explained by the lack of immune maturation and/or tolerance as well as the impairment of epithelial turnover (which is dependent on commensal colonization) in GF mouse intestine [127,128]. Gut microbiota metabolites act as important signals for the monitoring of the correct function of the epithelial barrier and the immune cells. Similarly, immune-driven signals central to gut homeostasis can also modulate the metabolism of immune cells [129]. It is well known that several hematopoietic cells produce IL-10 and its importance for maintaining tolerance within the intestinal microbiota come from experimental observations using IL-10- or IL-10R-deficient mice (both these mouse models develop spontaneous colitis) (see below, [130]), and clinical data (IBD patients are characterized by decreased levels of the anti-inflammatory cytokine IL-10). In line with these results, administration of genetically modified probiotic, i.e., Lactococcus lactis expressing IL-10, had demonstrated a significant remission of disease activity in CD patients. Furthermore, oligofructose-enriched inulin (OF-IN) administration was able to induce an improvement in CD associated to a reduction of the Ruminococcus gnavus. In addition, it has been recorded that the intake of this prebiotic is able to increase the abundance of the Bifidobacterium longum. This bacteria neutralizes reactive oxygen species and exerts anti-inflammatory effects at the site of inflammation, reducing gastrointestinal discomfort and tissue injury [131]. Previous studies also showed that different probiotic combinations, especially Bifidobacterium longum or a multistrain mix of Bifidobacterium longum, Lactobacillus acidophilus, and Streptococcus faecalis, increased expression of tight junction proteins in IBD [132]. Furthermore, VSL#3®, a mixture of 4 species of Lactobacillus, 3 species of Bifidobacterium, and 1 species of Streptococcus, has been shown to: (i) Improve epithelial barrier damage; (ii) induce remission in active UC; and (iii) decrease pro-inflammatory mucosal cytokine expression [133].
Meta-analyses revealed a low incidence of IBD in eskimos, whose diet is particularly rich in n-3 PUFAs [134]. Starting from these clinical evidences, the impact of dietary n-3 PUFAs has been evaluated in different models of colitis. All the results obtained in these experiments are coherent and indicate that n-3 PUFAs decrease chemically-induced intestinal tissue damage and inflammation [135]. Similarly, in fat-1 transgenic mice, characterized by high levels of endogenous n-3 PUFAs, the intestinal tissue damage was significantly reduced compared to wild type mice, together with decreased expression of TNF-α, IL-1β, and increased synthesis of SPMs [136,137]. In addition, the fat-1 mice displayed higher gut microbiota diversity and more abundance of Verrucomicrobiota plylum (Akkermansia genus) compared to wild-type [138].
Moreover, a diet high in fibers and n-3 PUFAs is protective for the development of IBD, whereas a diet high in refined sugars, complex carbohydrates, and n-6 PUFAs (i.e., red meat), increases the risk of acquiring IBD. A number of studies indicated that homeostasis is crucial to have a good n-3 to n-6 PUFAs ratio, the former being anti-inflammatory and the latter pro-inflammatory molecules [1,139]. Therefore, dietary n-3 PUFAs supplementation is encouraged as anti-inflammatory adjuvants for IBD [140,141]. On the contrary, a low-fiber diet may increase the risk of CD, and, if associated to high consumption of sugar and soft drinks, it may also increase UC risk [142]. However, thus far, the effects of dietary interventions on CD and UC are uncertain [143]. The cornerstone is that dietary fiber is a plant-based carbohydrate that resists digestion by intestinal and pancreatic enzymes in the human GI tract. Soluble and insoluble dietary fibers are essential for gastrointestinal mucosa health because they serve as important substrates for the gut microbiota. The fermentation products selectively promote the growth of beneficial Bifidobacteria and Lactobacilli and exert anti-inflammatory (such as, inhibition of NFκB transcription) and anti-carcinogenic functions [144].
Two large clinical trials designed at evaluating the effects of n-3 PUFA supplementation on CD provided conflicting results and concluded that supplementation was not effective in preventing CD relapse [145,146]. Intriguingly, another study suggested that IBD patients that achieved a n-3/n-6 ratio of 1 maintained disease remission at a significantly higher rate compared to those did not reach this goal [147]. A double-blind, randomized study was carried out in 38 pediatric CD patients, who received, for 12 months, 5-aminosalicylic acid (50 mg/kg/d) + n-3 PUFAs (3 capsule/d, each capsule contained 400 mg/g EPA and 200 mg/g DHA) or 5-5-aminosalicylic acid (50 mg/kg/d) + olive oil placebo capsules [148]. The results indicated that the addition of enteric-coated capsules to a conventional therapy with 5-aminosalicylic acid delayed the relapse of the disease even though it could not prevent it. Another study used enteric-coated n-3 PUFAs capsules for remission maintenance in adult CD patients at high risk of relapse, and found n-3 PUFAs to be more effective than placebo [149]. However, two multicentre, randomized, double-blind, placebo-controlled studies, called Epanova Program in Crohn’s 1 and 2, (EPIC1 and EPIC2), found that relapse occurred in 32% with n-3 PUFAs and 36% with placebo in EPIC1, and 48% with n-3 PUFAs and 49% with placebo in EPIC2, indicating that n-3 PUFAs did not reduce the rate of relapse in patients with quiescent CD [146]. Of interest, two random double-blind placebo crossover studies reported significant improvement of the disease [150] and of the oxidative stress status in active UC patients receiving sulfasalazine, respectively [151]. Thus, the efficacy of n-3 PUFA or fish oil against CD or UC is, at best, marginal. However, none of the studies reported any adverse effects associated with n-3 PUFA supplementation. A recent meta-analysis of observational studies showed that fish consumption was inversely associated with the risk of CD. Moreover, there was a strong inverse association between dietary n-3 PUFAs intake and the risk of UC [152]. Previously published studies revealed that fish consumption and dietary n-3 PUFAs intake might play a role in the etiology of IBD [153,154]. In line with these findings, one study revealed that the Mediterranean diet, rich in fish and seafood, reduced inflammation [151] and normalized the gut microbiome in CD patients, i.e., an increase in Bacteroidetes and Clostridium clusters, and a reduction of Protebacteria and Bacillaceae [155]. In a pilot study, short-term EPA-supplementation reduced mucosal inflammation favoring an improvement of both endoscopic and histological inflammation in almost all patients, together with a significant up-regulation of IL-10 expression, and a reduction of STAT3 activation [156]. Moreover, microbiota analysis showed that EPA treatment increased the family Porphyromonadaceae and the genus Parabacteroides, and reduced the genus Bacteroides that include mucolytic species [157].
In addition to fats and fibers, bioactive amino acids and oligopeptides are derived from food proteins through chemical and enzymatic hydrolysis, or bacterial metabolism [158,159]. In vitro and in vivo models of IBD have been used to test the antioxidant properties of amino acids. Cysteine, methionine, taurine, tryptophan, tyrosine, phenylalanine are able to reduce the oxidative stress, because of the presence of a thiol group and of an aromatic ring [142,160]. In addition, dietary cysteine was effective at reducing the intestinal inflammatory responses and at enhancing mucin synthesis in DSS-induced colitis animal models [161,162,163]. The anti-inflammatory activity of these bioactive molecules involves the activation of the calcium-sensing receptor (CaSR), a protein controlling different cellular activities (i.e., proliferation, differentiation, and apoptosis) [164,165]. On the other hand, mucins are cysteine-rich glycoproteins, secreted by goblet cells, and very important for intestinal epithelial integrity.
4.2. Retinal Disease
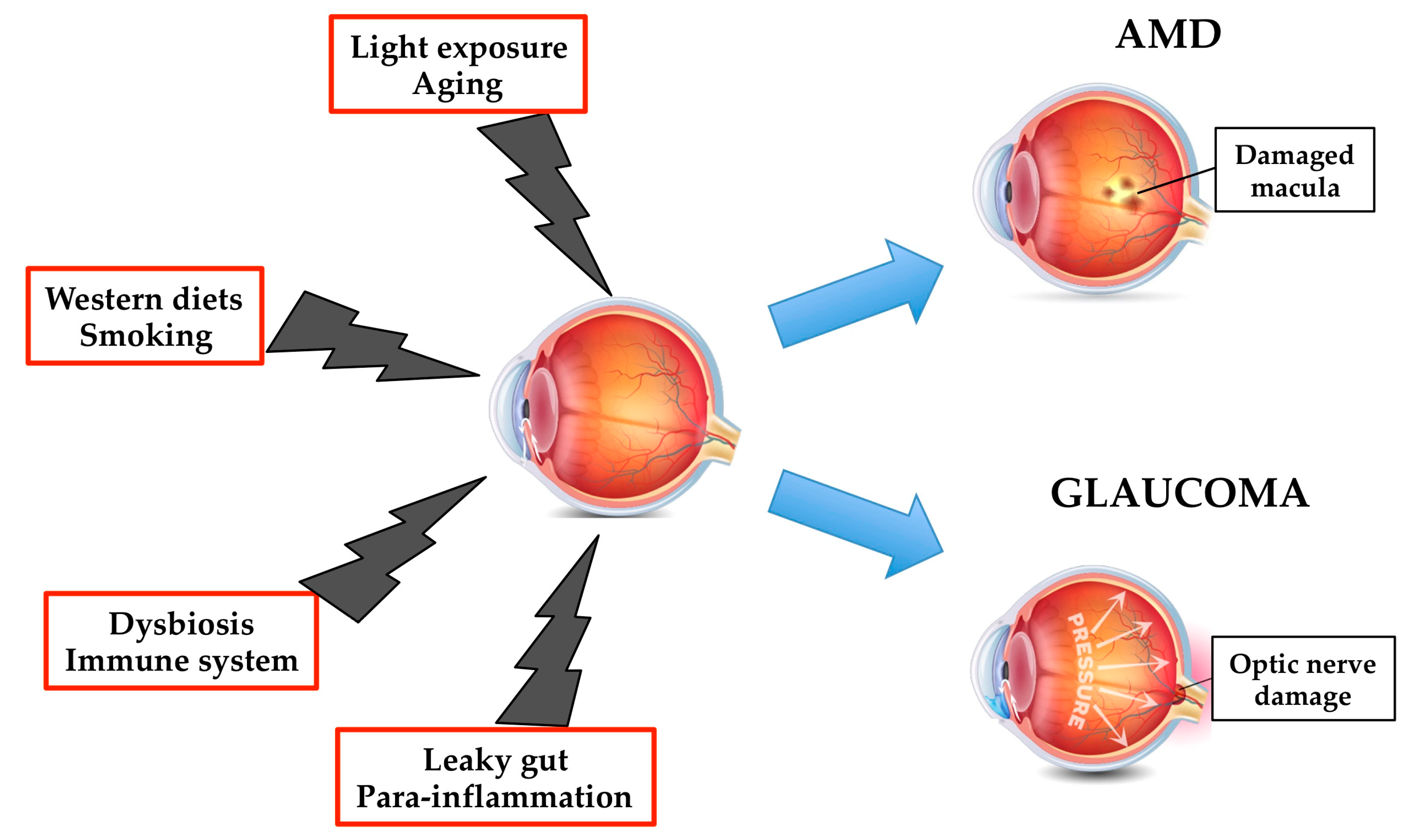
Despite major advances in treatment and management, retinal disease cause over three-quarters of all cases of irreversible vision loss in the western world. Recent estimates indicated that the leading causes of irreversible severe visual impairment in those >50 years of age were diabetic retinopathy, age-related macular degeneration (AMD) and glaucoma, affecting~5.4 million people globally [166]. Retinal disease manifest abnormal angiogenesis, proliferative neovascularization, excessive vascular permeability, immunoregulatory dysfunction, alterations in physiologic reduction-oxidation (redox) balance, or retinal pigment epithelial (RPE) cell degeneration.
Pathological factors affecting the retina health include ischemia, light exposure, oxidative stress, apoptosis, inflammation, neuroactive cell signaling molecules, and aging. Moreover, plasma levels of high-sensitivity C-reactive protein and pro-inflammatory cytokines, such as TNF-α and IL-6, have been elevated in subjects with essential hypertension, coronary heart disease, type 2 diabetes, retinal disease, and inflammatory bowel disease [167,168,169,170]. Anti-inflammatory therapy with canakinumab, targeting the IL-1β innate immunity pathway, markedly reduced the plasma levels of IL-6 and high-sensitivity C-reactive protein [171], and led to a significantly lower rate of recurrent cardiovascular events than placebo, independent of lipid-level lowering [172]. These studies provide the proof of concept that the removal of pro-inflammatory markers reduces the inflammatory-based disease risk.
Within the neural retina, phosphatidylcholine (PC) and phosphatidylethanolamine (PEA) represent the predominant PUFA-rich lipid class, followed by phosphatidylserine (PS) and phosphatidylinositol (PI). Arachidonic acid (AA) is the major PUFA in the neural and vascular tissue of the retina [173,174]. PUFA-containing phospholipids enter the RPE or photoreceptor inner segment via a receptor mediated transport process. Tracer studies have indicated that DHA-containing phospholipids are then integrated as structural constituents of photoreceptor disk membranes and are retained in proximity to rhodopsin molecules across the life span of these organelles [175]. Several bioactive molecules play a crucial role in the retinal disease, i.e., eicosanoids, angiogenic factors, matrix metalloproteinases (MMPs), reactive oxygen species, cyclic nucleotides, neurotransmitters and neuromodulators, proinflammatory and immunoregulatory cytokines, and inflammatory phospholipids. It has been shown that n-3 PUFAs are able to modulate the production, activation, and potency of these molecules. DHA and its substrate, EPA, influence eicosanoid metabolism by reducing n-6 PUFAs levels (mainly arachidonic acid, AA, 20:4n-6) and compete for enzymes (cyclooxygenase, COX and lipoxygenase, LOX) producing AA-based angiogenic and proinflammatory eicosanoids [176].
As above mentioned, intestinal bacteria are often considered a hidden metabolic organ, since they play a significant role in human nutrition and metabolism. It has been demonstrated that CONV-R mice had reduced levels of multiple PC species in lens and retina compared to GF animals, which suggested that the gut microbiota influenced the lens and retinal lipid composition [177]. Antibiotics depletion of gut microbiota in a spontaneous mouse model of uveitis resulted in significant attenuation of the retinal disease, associated with a reduced population of Th17 cells in the intestinal lamina propria (LP). Co-housing GF with CON-R mice restored disease development [178]. Recently, an experimental study demonstrated subclinical intestinal dysfunction in retinal disease leading to enhanced migration of leukocytes between the intestine and the eye. These alterations were improved by 3-week pre-treatment of SCFA sthrough induction of Treg in several tissues and inhibition of T cell differentiation into Th1 and Th17 [179]. Altogether, these data suggest that commensal microbiota may serve as triggers of immune responses and offer clues to the environmental origin of ocular inflammation [180].
4.2.1. Age-Related Macular Degeneration
In patients older than 55 years, age-related macular degeneration (AMD) is considered the leading cause of serious visual loss in the developed world [97,181], and the third leading cause of blindness in the world [182]. AMD is a degenerative disease caused by the concomitant presence of non-modifiable (genetics, sex, age) and modifiable factors (nutritional status, smoking status) (Figure 5) [183]. Several genetic associations have been found, the most studied are those related to inflammatory genes such as complement factor H and certain complement components (i.e., C3 and C2) [184]. Recently, a tissue-adaptive response, called para-inflammation, where the innate immune system engages a low-grade inflammatory response to restore tissue homeostasis, has been associated to the pathogenesis of ADM [185].
The development of treatments targeting vascular endothelial growth factor (VEGF) over the past 10 years has seen a dramatic reduction in vision loss from advanced AMD. However, with long-term treatment, many patients with AMD continue to lose vision [186]
Experimental and epidemiologic studies have indicated a link between the dietary consumption of xanthophyll carotenoids, i.e., lutein (L) and zeaxanthin (Z), or n-3 PUFAs and the reduced risk of advanced AMD [187,188,189,190,191]. Specifically, they found a direct correlation between the daily intake of these xanthophyll carotenoids and their concentrations in both plasma and macula, the latter being the district were they used to synthetize the macular pigment [192,193,194,195]. This is an important event, because the macular pigments exhibit protective functions against oxidative stress and inflammation, both factors implicated in the pathogenesis of AMD [196].
On the other hand, the neuroprotective role of n-3 PUFAs has been proved by several epidemiological studies that observed a decreased risk of ADM in subjects with high intake of n-3 PUFAs [173,197]. In a large prospective study, with 24–28 years of follow-up, n-3 PUFAs and fatty fish intakes were associated to a lower risk of visually intermediate AMD, but no relationship was found with the risk of advanced AMD [198]. Moreover, in healthy volunteers, macular pigment density was associated not only with L and Z plasma concentrations, but also with plasma levels of phospholipids containing n-3 PUFAs, particularly EPA and docosapentaenoic acid (DPA) [199]. The latter being the second most abundant n-3 PUFAs found within the retina and a metabolic intermediary between EPA and DHA [200]. In a mouse model of AMD, the administration of L, Z and n-3 PUFAs caused retinal lesion regression associated with a reduced expression of pathologic genes, and preservation of photoreceptors [201]. Moreover, in another experimental model of AMD, the supplementation with n-3 PUFAs reduced the photoreceptor damage, and the mRNA and protein expression of inflammatory mediators [202,203,204]. Altogether these data indicated that the efficacy of n-3 PUFAs could be explained by a combination between the resolution of inflammation and the induction of a regenerative process. Coherent with this hypothesis is the discovery of elovanoids, bioactive lipid mediators derived from very long chain (VLC) n-3 PUFAs by the action of the elongase ELOVL4. Indeed, the contemporary presence of free VLC n-3 PUFAs and oxidative stress seems to generate a pro-homeostatic and cytoprotective milieu [205]. In line with these results, it has been observed that mutant EVOVL4 caused juvenile macular degeneration due to protein mislocalization and photoreceptor cell death [205]. Recently, a linear association between the dose of fish consumption and the risk of AMD was found, strengthening the role of n-3 PUFAs in AMD pathogenesis [206]. Taken together, these results suggested that the metabolic pathway responsible for the synthesis of the elovanoids should be the object of future studies because it could open a new therapeutic approach for AMD.
As discussed earlier, gut microbiota affect all aspects of immune development and homeostasis in health and disease [9]. For this reason, the intestinal microbiota represent candidates for the interplay between the genetic and environmental factors that cause AMD. Using mouse models of neovascular AMD, it has been demonstrated that HFDs exacerbated choroidal neovascularization by altering gut microbiota [207]. Gut dysbiosis instead leads to heightened IP and chronic low-grade inflammation, characteristic of inflammaging, with elevated production of IL-6, IL-1β, TNF-α, and VEGF-A. Both antibiotic treatment and microbiotal transplants (T) from chow diet (CD)-fed mice restored microbial proportions, i.e., Bacteroidetes to Firmicutes ratio of 3 to 1. In addition, improved glucose tolerance, lower systemic and choroidal inflammation, and IP in HFDxCDT mice compared to HFDxHFDT mice were observed [207]. Furthermore, mice fed high-glucose diet (HGD) developed a dysbiosis associated with AMD-like features, such as RPE and photoreceptor atrophy, and lipofuscin accumulation [208]. In addition, HGD-fed mice showed lower microbial diversity than CD-fed animals, with a reduced abundance of Bacteroidetes and an increased level of Proteobacteria at the phylus levels (one of the best source of LPS), as well as higher levels of the Desulfovibrio vulgaris species. A significant increase of IP, demonstrated by a reduced expression of tight junction proteins, such as ZO-1 and occludin, was also observed [209].
In a clinical study, AMD patients displayed significant gut microbial alterations compared with healthy controls. Moreover, AMD associated gut bacteria were immunologically relevant, enriched in the IgA-bound fraction, and contained altered microbes relating to fatty acid metabolism and carotenoid pathway biosynthesis, compared to controls [210]. A cross-sectional study reported that the western diet, rich in dairy products, red meats, and eggs, was significantly associated to a higher incidence of advanced AMD compared with the oriental diet, rich in vegetable, legumes, rice, fruits, low-fat dairy products and fish [211].
4.2.2. Glaucoma
Glaucoma is a term defining a group of optic degenerative diseases characterized by the progressive death of retinal ganglion cells (RGCs) and excavation of the optic nerve head (ONH) [212]. Glaucoma is the leading cause of global irreversible blindness. The number of people with glaucoma worldwide (aged 40 e 80 years) will increase from 64.3 million in 2013 to 111.8 million in 2040, disproportionately affecting people residing in Asia and Africa [213]. Primary open-angle glaucoma is characterized by a particular abnormal appearance of the optic- nerve disk, whereas pigmentary glaucoma is a secondary glaucoma showing: (1) Disruption of the posterior iris-pigment epithelium; (2) dispersion of the pigment throughout the anterior segment and the trabecular mesh work; and (3) increase in intraocular pressure (IOP) [214]. Age, elevated IOP, race, family history, myopia, diabetes, and para-inflammation are involved in the pathogenesis, development and progression of glaucoma (Figure 5) [215] [216,217,218]. Moreover, several data have suggested that the immune system is involved even before the normal signs of glaucoma begin [217,219]. The up to date treatments for the early management of the glaucoma have involved the reduction of IOP, via topical instillation of anti-glaucoma eye drops, laser therapy or invasive surgery [220]. Preclinical and clinical studies have demonstrated the protective effects of n-3 PUFAs in different retinal disease [221,222,223], including glaucoma [224]. Interestingly, EPA and DHA plasma levels found in patients affected by primary open-angle glaucoma were lower than those measured in healthy subjects [225]. In addition, in an experimental model of hereditary glaucoma [226], the administration of n-3 PUFAs, alone or in combination with timolol, displayed neuroprotective effects only when the ratio of AA to Epa was kept between 1 and 1.5 [227]. This result was associated with the downregulation of IL-18 and TNF-α expression only when n-3 PUFAs were administrated alone, which indicated that the neuroprotection in the retina might be mediated by other mechanisms, i.e., the synthesis of SPMs were able, not only to resolve inflammation, but also protected organs and stimulate tissue regeneration (Figure 2) [228]. It has been demonstrated that RGCs are the most susceptible retinal neurons to high IOP [229]. Ocular hypertension also lead to an alteration of visual function [230], since both a and b-wave amplitudes of the electroretinogram (ERG) were decreased after a marked elevation of IOP caused by an ischemia-reperfusion sequence [231,232]. In an in vivo rat model of IOP elevation, it has been demonstrated that dietary supplementation of n-3 and n-6 PUFAs was able to reduce retinal stress and preserve retinal structure [233]. In line with these data, Bazan and co-workers demonstrated that the oxygenated metabolite of DHA, neuroprotectin D1 (NPD1), was responsible of these neuroprotective effects (Figure 2) [234,235]. NPD1 was shown to decrease: (i) The production of inflammatory molecules (such as COX-2, IL-1β); (ii) to up-regulate anti-apoptotic Bcl-2 proteins; and (iii) to down-regulate pro-apoptotic proteins (Bax, Bad, Caspase-3) [233,236].
Recently, in a mouse model, it was shown that a transient elevation of IOP was sufficient to induce T-cell infiltration into the retina and this step was essential for the development of glaucoma. In addition, the authors demonstrated that T-cell activations and glaucomatous neurodegeneration were abolished in GF mice, strengthening the hypothesis that a bacteria-sensitized T-cell responses underly the pathogenesis of glaucoma [237]. In line with these data, long-term intake of Lactobacillus paracasei KW3110 has been associated with a more abundance of beneficial gut bacteria and a reduction of the age-related immune dysfunctions, i.e., lowered expansion of pro-inflammatory T cells and serum cytokines [238]. Instead, this probiotic treatment determined a reduction of the Firmicutes to Bacteroidetes ratio, demonstrated by increased Bifidobacteriaceae and decreased Streptococcaceae families. It is important to highlight that Bifidobacterium is known as one of the most beneficial bacterial family [67], and Streptococcaceae bacteria are able to stimulate the intestinal cells to secrete pro-inflammatory cytokines [239].
5. Conclusions
Many observational studies have shown the potential role of nutraceuticals and functional foods, such as n3-PUFAs, probiotics and prebiotics, in preventing chronic inflammatory disease or to aid in their treatment. Since IBD, AMD and glaucoma are illnesses increasing at alarming rates, more basic and clinical studies are needed to definitely determine if dietary factors (alone or in combination) are able to prevent the development of these disabling pathologies. The discovery of n-3 PUFAs-derived anti-inflammatory molecules, i.e., SPMs, may offer a fascinating new complementary option for the treatment of these inflammatory-based diseases. Indeed, a new area of research is focusing on the development of synthetic analogs of the natural SPMs as well as on the combination between n-3 PUFAs with drugs acting as regulators of endogenous enzyme activities [240]. The former strategy has been pursued by the OMEICOS Therapeutics and the compound OMT-28 entered clinical phase I in February 2017 (NTC 03906799).
On the other hand, n-3 PUFAs can also be considered prebiotics due to the fact that they are able to increase the production of anti-inflammatory molecules, such as SCFAs. Coherent with this data, recent reports suggested that the combination between prebiotics and probiotics, called symbiotic, bear great potential for correcting the gut dysbiosis and selectively stimulated the growth and/or activated the metabolism of one or a limited number of health-promoting bacteria, aimed at restoring the mutualism of holobiont [241]. Moreover, a better understanding of the mechanisms that underlie microbial resilience towards external perturbations will be a key requirement for microbiome-directed precision medicine [242].
In summary, modulation of the microbiota remains a promising therapeutic option for the prevention and treatment of complex diseases, but much more must be learned to maximize treatment success.
Funding
This work was supported by from MIUR Progetto Eccellenza.
Acknowledgments
We thank Elda Desiderio Pinto for administrative assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chiesa, G.; Busnelli, M.; Manzini, S.; Parolini, C. Nutraceuticals and Bioactive Components from Fish for Dyslipidemia and Cardiovascular Risk Reduction. Mar. Drugs 2016, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Fatty acids and inflammation: the cutting edge between food and pharma. Eur J. Pharmacol. 2011, 668 (Suppl. 1), S50–S58. [Google Scholar] [CrossRef]
- Arrese, M.; Cabrera, D.; Kalergis, A.M.; Feldstein, A.E. Innate Immunity and Inflammation in NAFLD/NASH. Dig. Dis. Sci. 2016, 61, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Pizzini, A.; Lunger, L.; Sonnweber, T.; Weiss, G.; Tancevski, I. The Role of Omega-3 Fatty Acids in the Setting of Coronary Artery Disease and COPD: A Review. Nutrients 2018, 10, 1864. [Google Scholar] [CrossRef] [PubMed]
- Mirkov, M.U.; Verstockt, B.; Cleynen, I. Genetics of inflammatory bowel disease: beyond NOD2. Lancet. Gastroenterol. Hepatol. 2017, 2, 224–234. [Google Scholar] [CrossRef]
- Arjamaa, O.; Aaltonen, V.; Piippo, N.; Csont, T.; Petrovski, G.; Kaarniranta, K.; Kauppinen, A. Hypoxia and inflammation in the release of VEGF and interleukins from human retinal pigment epithelial cells. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Busnelli, M.; Manzini, S.; Sirtori, C.R.; Chiesa, G.; Parolini, C. Effects of Vegetable Proteins on Hypercholesterolemia and Gut Microbiota Modulation. Nutrients 2018, 10, 1249. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, A.J.; Harris, N.L. Interactions between commensal intestinal bacteria and the immune system. Nat. Rev. Immunol. 2004, 4, 478–485. [Google Scholar] [CrossRef]
- Illiano, P.; Brambilla, R.; Parolini, C. The mutual interplay of gut microbiota, diet and human disease. Med. Res. Rev. 2019. under review. [Google Scholar]
- Lloyd-Price, J.; Mahurkar, A.; Rahnavard, G.; Crabtree, J.; Orvis, J.; Hall, A.B.; Brady, A.; Creasy, H.H.; McCracken, C.; Giglio, M.G.; et al. Strains, functions and dynamics in the expanded Human Microbiome Project. Nature 2017, 550, 61–66. [Google Scholar] [CrossRef]
- Vazquez, C.; Botella-Carretero, J.I.; Corella, D.; Fiol, M.; Lage, M.; Lurbe, E.; Richart, C.; Fernandez-Real, J.M.; Fuentes, F.; Ordonez, A.; et al. White fish reduces cardiovascular risk factors in patients with metabolic syndrome: the WISH-CARE study, a multicenter randomized clinical trial. Nutr. Met. Cardiovasc. Dis. 2014, 24, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Howard, A.; Udenigwe, C.C. Mechanisms and prospects of food protein hydrolysates and peptide-induced hypolipidaemia. Food Funct. 2013, 4, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Parolini, C.; Vik, R.; Busnelli, M.; Bjorndal, B.; Holm, S.; Brattelid, T.; Manzini, S.; Ganzetti, G.S.; Dellera, F.; Halvorsen, B.; et al. A salmon protein hydrolysate exerts lipid-independent anti-atherosclerotic activity in ApoE-deficient mice. PLoS ONE 2014, 9, e97598. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Colletti, A. Potential role of bioactive peptides in prevention and treatment of chronic diseases: a narrative review. Br. J. Pharmacol. 2017, 174, 1378–1394. [Google Scholar] [CrossRef] [PubMed]
- Busnelli, M.; Manzini, S.; Hilvo, M.; Parolini, C.; Ganzetti, G.S.; Dellera, F.; Ekroos, K.; Janis, M.; Escalante-Alcalde, D.; Sirtori, C.R.; et al. Liver-specific deletion of the Plpp3 gene alters plasma lipid composition and worsens atherosclerosis in apoE(-/-) mice. Sci. Rep. 2017, 7, 44503. [Google Scholar] [CrossRef] [PubMed]
- Dellera, F.; Ganzetti, G.S.; Froio, A.; Manzini, S.; Busnelli, M.; Meinitzer, A.; Sirtori, C.R.; Chiesa, G.; Parolini, C. L-homoarginine administration reduces neointimal hyperplasia in balloon-injured rat carotids. Thromb. Haemost. 2016, 116, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Parolini, C.; Bjorndal, B.; Busnelli, M.; Manzini, S.; Ganzetti, G.S.; Dellera, F.; Ramsvik, M.; Bruheim, I.; Berge, R.K.; Chiesa, G. Effect of Dietary Components from Antarctic Krill on Atherosclerosis in apoE-Deficient Mice. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Rimm, E.B.; Appel, L.J.; Chiuve, S.E.; Djousse, L.; Engler, M.B.; Kris-Etherton, P.M.; Mozaffarian, D.; Siscovick, D.S.; Lichtenstein, A.H.; On behalf of the American Heart Association Nutrition Committee of the Council on Lifestyle and Cardiometabolic Health; et al. Seafood Long-Chain n-3 Polyunsaturated Fatty Acids and Cardiovascular Disease: A Science Advisory From the American Heart Association. Circulation 2018, 138, e35–e47. [Google Scholar] [CrossRef]
- Busnelli, M.; Manzini, S.; Parolini, C.; Escalante-Alcalde, D.; Chiesa, G. Lipid phosphate phosphatase 3 in vascular pathophysiology. Atherosclerosis 2018, 271, 156–165. [Google Scholar] [CrossRef]
- Superko, H.R.; King, S., 3rd. Lipid management to reduce cardiovascular risk: A new strategy is required. Circulation 2008, 117, 560–568. [Google Scholar] [CrossRef]
- Parolini, C.; Adorni, M.P.; Busnelli, M.; Manzini, S.; Cipollari, E.; Favari, E.; Lorenzon, P.; Ganzetti, G.S.; Fingerle, J.; Bernini, F.; et al. Infusions of large synthetic HDL containing trimeric apoA-I stabilize atherosclerotic plaques in hypercholesterolemic rabbits. Can. J. Cardiol. 2019. accepted for publication. [Google Scholar] [CrossRef]
- Chiesa, G.; Parolini, C.; Sirtori, C.R. Acute effects of high-density lipoproteins: biochemical basis and clinical findings. Curr. Opin. Cardiol. 2008, 23, 379–385. [Google Scholar] [CrossRef]
- Do, R.; Stitziel, N.O.; Won, H.H.; Jorgensen, A.B.; Duga, S.; Angelica Merlini, P.; Kiezun, A.; Farrall, M.; Goel, A.; Zuk, O.; et al. Exome sequencing identifies rare LDLR and APOA5 alleles conferring risk for myocardial infarction. Nature 2015, 518, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Myocardial Infarction, G.; Investigators, C.A.E.C.; Stitziel, N.O.; Stirrups, K.E.; Masca, N.G.; Erdmann, J.; Ferrario, P.G.; Konig, I.R.; Weeke, P.E.; Webb, T.R.; et al. Coding Variation in ANGPTL4, LPL, and SVEP1 and the Risk of Coronary Disease. N. Engl. J. Med. 2016, 374, 1134–1144. [Google Scholar] [CrossRef]
- Klempfner, R.; Erez, A.; Sagit, B.Z.; Goldenberg, I.; Fisman, E.; Kopel, E.; Shlomo, N.; Israel, A.; Tenenbaum, A. Elevated Triglyceride Level Is Independently Associated With Increased All-Cause Mortality in Patients With Established Coronary Heart Disease: Twenty-Two-Year Follow-Up of the Bezafibrate Infarction Prevention Study and Registry. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Nichols, G.A.; Philip, S.; Reynolds, K.; Granowitz, C.B.; Fazio, S. Increased Cardiovascular Risk in Hypertriglyceridemic Patients With Statin-Controlled LDL Cholesterol. J. Clin. Endocrinol. Metab. 2018, 103, 3019–3027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watts, G.F.; Ooi, E.M.; Chan, D.C. Demystifying the management of hypertriglyceridaemia. Nat. Rev. Cardiol. 2013, 10, 648–661. [Google Scholar] [CrossRef]
- Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet 1999, 354, 447–455. [CrossRef] [PubMed]
- Saito, Y.; Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; et al. Effects of EPA on coronary artery disease in hypercholesterolemic patients with multiple risk factors: sub-analysis of primary prevention cases from the Japan EPA Lipid Intervention Study (JELIS). Atherosclerosis 2008, 200, 135–140. [Google Scholar] [CrossRef]
- Kromhout, D.; Giltay, E.J.; Geleijnse, J.M.; Alpha Omega Trial, G. n-3 fatty acids and cardiovascular events after myocardial infarction. N. Engl. J. Med. 2010, 363, 2015–2026. [Google Scholar] [CrossRef]
- Investigators, O.T.; Bosch, J.; Gerstein, H.C.; Dagenais, G.R.; Diaz, R.; Dyal, L.; Jung, H.; Maggiono, A.P.; Probstfield, J.; Ramachandran, A.; et al. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N. Engl. J. Med. 2012, 367, 309–318. [Google Scholar] [CrossRef]
- Aung, T.; Halsey, J.; Kromhout, D.; Gerstein, H.C.; Marchioli, R.; Tavazzi, L.; Geleijnse, J.M.; Rauch, B.; Ness, A.; Galan, P.; et al. Associations of Omega-3 Fatty Acid Supplement Use With Cardiovascular Disease Risks: Meta-analysis of 10 Trials Involving 77917 Individuals. JAMA Cardiol. 2018, 3, 225–234. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Brinton, E.A.; Jacobson, T.A.; Miller, M.; Tardif, J.C.; Ketchum, S.B.; Doyle, R.T., Jr.; Murphy, S.A.; Soni, P.N.; et al. Rationale and design of REDUCE-IT: Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial. Clin. Cardiol. 2017, 40, 138–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzini, S.; Busnelli, M.; Parolini, C.; Minoli, L.; Ossoli, A.; Brambilla, E.; Simonelli, S.; Lekka, E.; Persidis, A.; Scanziani, E.; et al. Topiramate protects apoE-deficient mice from kidney damage without affecting plasma lipids. Pharmacol. Res. 2018, 141, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, G.; Rigamonti, E.; Monteggia, E.; Parolini, C.; Marchesi, M.; Miragoli, L.; Grotti, A.; Maggioni, F.; Lorusso, V.; Sirtori, C.R. Evaluation of a soft atherosclerotic lesion in the rabbit aorta by an invasive IVUS method versus a non-invasive MRI technology. Atherosclerosis 2004, 174, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Mason, R.P.; Jacob, R.F.; Shrivastava, S.; Sherratt, S.C.R.; Chattopadhyay, A. Eicosapentaenoic acid reduces membrane fluidity, inhibits cholesterol domain formation, and normalizes bilayer width in atherosclerotic-like model membranes. Biochim. Biophys. Acta 2016, 1858, 3131–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, J.R.; Wani, O.; May, H.T.; Budoff, M. Potential benefits of eicosapentaenoic acid on atherosclerotic plaques. Vasc. Pharmacol. 2017, 91, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bays, H.E.; Ballantyne, C.M.; Braeckman, R.A.; Stirtan, W.G.; Soni, P.N. Icosapent ethyl, a pure ethyl ester of eicosapentaenoic acid: Effects on circulating markers of inflammation from the MARINE and ANCHOR studies. Am. J. Cardiovasc. Drugs. 2013, 13, 37–46. [Google Scholar] [CrossRef]
- Im, D.S. Functions of omega-3 fatty acids and FFA4 (GPR120) in macrophages. Eur. J. Pharmacol. 2016, 785, 36–43. [Google Scholar] [CrossRef]
- Kromhout, D.; Yasuda, S.; Geleijnse, J.M.; Shimokawa, H. Fish oil and omega-3 fatty acids in cardiovascular disease: do they really work? Eur. Heart J. 2012, 33, 436–443. [Google Scholar] [CrossRef]
- Darwesh, A.M.; Sosnowski, D.K.; Lee, T.Y.; Keshavarz-Bahaghighat, H.; Seubert, J.M. Insights into the cardioprotective properties of n-3 PUFAs against ischemic heart disease via modulation of the innate immune system. Chem. Biol. Interact. 2019, 308, 20–44. [Google Scholar] [CrossRef]
- Lorente-Cebrian, S.; Costa, A.G.; Navas-Carretero, S.; Zabala, M.; Laiglesia, L.M.; Martinez, J.A.; Moreno-Aliaga, M.J. An update on the role of omega-3 fatty acids on inflammatory and degenerative diseases. J. Physiol. Biochem. 2015, 71, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N.; Levy, B.D. Resolvins in inflammation: emergence of the pro-resolving superfamily of mediators. J. Clin. Investig. 2018, 128, 2657–2669. [Google Scholar] [CrossRef] [PubMed]
- Back, M.; Hansson, G.K. Omega-3 fatty acids, cardiovascular risk, and the resolution of inflammation. FASEB J. 2019, 33, 1536–1539. [Google Scholar] [CrossRef] [PubMed]
- Laguna-Fernandez, A.; Checa, A.; Carracedo, M.; Artiach, G.; Petri, M.H.; Baumgartner, R.; Forteza, M.J.; Jiang, X.; Andonova, T.; Walker, M.E.; et al. ERV1/ChemR23 Signaling Protects Against Atherosclerosis by Modifying Oxidized Low-Density Lipoprotein Uptake and Phagocytosis in Macrophages. Circulation 2018, 138, 1693–1705. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, M.; Parolini, C.; Caligari, S.; Gilio, D.; Manzini, S.; Busnelli, M.; Cinquanta, P.; Camera, M.; Brambilla, M.; Sirtori, C.R.; et al. Rosuvastatin does not affect human apolipoprotein A-I expression in genetically modified mice: a clue to the disputed effect of statins on HDL. Br. J. Pharmacol. 2011, 164, 1460–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pradhan, A.D.; Manson, J.E. Update on the Vitamin D and OmegA-3 trial (VITAL). J. Steroid Biochem. Mol. Biol. 2016, 155, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Lingwood, D.; Simons, K. Lipid rafts as a membrane-organizing principle. Science 2010, 327, 46–50. [Google Scholar] [CrossRef]
- Nicolau, D.V., Jr.; Burrage, K.; Parton, R.G.; Hancock, J.F. Identifying optimal lipid raft characteristics required to promote nanoscale protein-protein interactions on the plasma membrane. Mol. Cell. Biol. 2006, 26, 313–323. [Google Scholar] [CrossRef]
- Calder, P.C. Marine omega-3 fatty acids and inflammatory processes: Effects, mechanisms and clinical relevance. Biochim. Biophys. Acta 2015, 1851, 469–484. [Google Scholar] [CrossRef]
- Hou, T.Y.; McMurray, D.N.; Chapkin, R.S. Omega-3 fatty acids, lipid rafts, and T cell signaling. Eur. J. Pharmacol. 2016, 785, 2–9. [Google Scholar] [CrossRef]
- Whelan, J.; Gowdy, K.M.; Shaikh, S.R. N-3 polyunsaturated fatty acids modulate B cell activity in pre-clinical models: Implications for the immune response to infections. Eur. J. Pharmacol. 2016, 785, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Miron, N.; Cristea, V. Enterocytes: active cells in tolerance to food and microbial antigens in the gut. Clin. Exp. Immunol. 2012, 167, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, T. The overlap in the genetic pathogenesis of ulcerative colitis and irritable bowel syndrome. Dig. Dis. Sci. 2013, 58, 3379–3381. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Samson, S.E.; Grover, A.K. Antioxidant Supplements and Gastrointestinal Diseases: A Critical Appraisal. Med. Princ. Pract. 2017, 26, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Worthington, J.J.; Reimann, F.; Gribble, F.M. Enteroendocrine cells-sensory sentinels of the intestinal environment and orchestrators of mucosal immunity. Mucosal. Immunol. 2018, 11, 3–20. [Google Scholar] [CrossRef]
- Sender, R.; Fuchs, S.; Milo, R. Are We Really Vastly Outnumbered? Revisiting the Ratio of Bacterial to Host Cells in Humans. Cell 2016, 164, 337–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, J.M.; Murphy, K.; Stanton, C.; Ross, R.P.; Kober, O.I.; Juge, N.; Avershina, E.; Rudi, K.; Narbad, A.; Jenmalm, M.C.; et al. The composition of the gut microbiota throughout life, with an emphasis on early life. Microb. Ecol. Health Dis. 2015, 26, 26050. [Google Scholar] [CrossRef]
- Marques, T.M.; Wall, R.; Ross, R.P.; Fitzgerald, G.F.; Ryan, C.A.; Stanton, C. Programming infant gut microbiota: influence of dietary and environmental factors. Curr. Opin. Biotechnol. 2010, 21, 149–156. [Google Scholar] [CrossRef]
- Bezirtzoglou, E.; Tsiotsias, A.; Welling, G.W. Microbiota profile in feces of breast- and formula-fed newborns by using fluorescence in situ hybridization (FISH). Anaerobe 2011, 17, 478–482. [Google Scholar] [CrossRef]
- Parolini, C.; Busnelli, M.; Ganzetti, G.S.; Dellera, F.; Manzini, S.; Scanziani, E.; Johnson, J.L.; Sirtori, C.R.; Chiesa, G. Magnetic resonance imaging visualization of vulnerable atherosclerotic plaques at the brachiocephalic artery of apolipoprotein E knockout mice by the blood-pool contrast agent B22956/1. Mol. Imaging 2014, 13. [Google Scholar] [CrossRef]
- Tanaka, M.; Nakayama, J. Development of the gut microbiota in infancy and its impact on health in later life. Allergol. Int. 2017, 66, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, S.R.; Walker, W.A. Immune factors in breast milk and the development of atopic disease. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Palmeira, P.; Carneiro-Sampaio, M. Immunology of breast milk. Rev. Assoc. Med. Bras. 2016, 62, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Fallani, M.; Young, D.; Scott, J.; Norin, E.; Amarri, S.; Adam, R.; Aguilera, M.; Khanna, S.; Gil, A.; Edwards, C.A.; et al. Intestinal microbiota of 6-week-old infants across Europe: geographic influence beyond delivery mode, breast-feeding, and antibiotics. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Toscano, M.; Rodighiero, V.; De Vecchi, E.; Mogna, G. Cultivable and pyrosequenced fecal microflora in centenarians and young subjects. J. Clin. Gastroenterol. 2012, 46, S81–S84. [Google Scholar] [CrossRef] [PubMed]
- Farkas, A.M.; Panea, C.; Goto, Y.; Nakato, G.; Galan-Diez, M.; Narushima, S.; Honda, K.; Ivanov, I.I. Induction of Th17 cells by segmented filamentous bacteria in the murine intestine. J. Immunol. Methods 2015, 421, 104–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, T.G.; Sefik, E.; Geva-Zatorsky, N.; Kua, L.; Naskar, D.; Teng, F.; Pasman, L.; Ortiz-Lopez, A.; Jupp, R.; Wu, H.J.; et al. Identifying species of symbiont bacteria from the human gut that, alone, can induce intestinal Th17 cells in mice. Proc. Natl. Acad. Sci. USA 2016, 113, E8141–E8150. [Google Scholar] [CrossRef]
- Gaffen, S.L.; Hernandez-Santos, N.; Peterson, A.C. IL-17 signaling in host defense against Candida albicans. Immunol. Res. 2011, 50, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Guglani, L.; Khader, S.A. Th17 cytokines in mucosal immunity and inflammation. Curr. Opin. HIV AIDS 2010, 5, 120–127. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Yosef, N.; Gaublomme, J.; Wu, C.; Lee, Y.; Clish, C.B.; Kaminski, J.; Xiao, S.; Meyer Zu Horste, G.; Pawlak, M.; et al. CD5L/AIM Regulates Lipid Biosynthesis and Restrains Th17 Cell Pathogenicity. Cell 2015, 163, 1413–1427. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Awasthi, A.; Yosef, N.; Quintana, F.J.; Xiao, S.; Peters, A.; Wu, C.; Kleinewietfeld, M.; Kunder, S.; Hafler, D.A.; et al. Induction and molecular signature of pathogenic TH17 cells. Nat. Immunol. 2012, 13, 991–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Qie, Y.; Park, J.; Kim, C.H. Gut Microbial Metabolites Fuel Host Antibody Responses. Cell Host Microbe 2016, 20, 202–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arpaia, N.; Campbell, C.; Fan, X.; Dikiy, S.; van der Veeken, J.; deRoos, P.; Liu, H.; Cross, J.R.; Pfeffer, K.; Coffer, P.J.; et al. Metabolites produced by commensal bacteria promote peripheral regulatory T-cell generation. Nature 2013, 504, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Berod, L.; Friedrich, C.; Nandan, A.; Freitag, J.; Hagemann, S.; Harmrolfs, K.; Sandouk, A.; Hesse, C.; Castro, C.N.; Bahre, H.; et al. De novo fatty acid synthesis controls the fate between regulatory T and T helper 17 cells. Nat. Med. 2014, 20, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Ma, N.; He, T.; Johnston, L.J.; Ma, X. Tryptophan (Trp) modulates gut homeostasis via aryl hydrocarbon receptor (AhR). Crit. Rev. Food Sci. Nutr. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Postler, T.S.; Ghosh, S. Understanding the Holobiont: How Microbial Metabolites Affect Human Health and Shape the Immune System. Cell Metab. 2017, 26, 110–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michael, A.J. Biosynthesis of polyamines and polyamine-containing molecules. Biochem. J. 2016, 473, 2315–2329. [Google Scholar] [CrossRef]
- O’Neill, L.A.; Kishton, R.J.; Rathmell, J. A guide to immunometabolism for immunologists. Nat. Rev. Immunol. 2016, 16, 553–565. [Google Scholar] [CrossRef] [Green Version]
- Parolini, C.; Caligari, S.; Gilio, D.; Manzini, S.; Busnelli, M.; Montagnani, M.; Locatelli, M.; Diani, E.; Giavarini, F.; Caruso, D.; et al. Reduced biliary sterol output with no change in total faecal excretion in mice expressing a human apolipoprotein A-I variant. Liver Inter. 2012, 32, 1363–1371. [Google Scholar] [CrossRef]
- Levy, M.; Thaiss, C.A.; Elinav, E. Metabolites: Messengers between the microbiota and the immune system. Genes Dev. 2016, 30, 1589–1597. [Google Scholar] [CrossRef]
- Kunisawa, J.; Sugiura, Y.; Wake, T.; Nagatake, T.; Suzuki, H.; Nagasawa, R.; Shikata, S.; Honda, K.; Hashimoto, E.; Suzuki, Y.; et al. Mode of Bioenergetic Metabolism during B Cell Differentiation in the Intestine Determines the Distinct Requirement for Vitamin B1. Cell Rep. 2015, 13, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Whiting, C.V.; Bland, P.W.; Tarlton, J.F. Dietary n-3 polyunsaturated fatty acids reduce disease and colonic proinflammatory cytokines in a mouse model of colitis. Inflamm. Bowel Dis. 2005, 11, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.D.; Molbak, L.; Michaelsen, K.F.; Lauritzen, L. Molecular fingerprints of the human fecal microbiota from 9 to 18 months old and the effect of fish oil supplementation. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Balfego, M.; Canivell, S.; Hanzu, F.A.; Sala-Vila, A.; Martinez-Medina, M.; Murillo, S.; Mur, T.; Ruano, E.G.; Linares, F.; Porras, N.; et al. Effects of sardine-enriched diet on metabolic control, inflammation and gut microbiota in drug-naive patients with type 2 diabetes: A pilot randomized trial. Lipids Health Dis. 2016, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Watson, H.; Mitra, S.; Croden, F.C.; Taylor, M.; Wood, H.M.; Perry, S.L.; Spencer, J.A.; Quirke, P.; Toogood, G.J.; Lawton, C.L.; et al. A randomised trial of the effect of omega-3 polyunsaturated fatty acid supplements on the human intestinal microbiota. Gut 2018, 67, 1974–1983. [Google Scholar] [CrossRef] [PubMed]
- Robertson, R.C.; Seira Oriach, C.; Murphy, K.; Moloney, G.M.; Cryan, J.F.; Dinan, T.G.; Paul Ross, R.; Stanton, C. Omega-3 polyunsaturated fatty acids critically regulate behaviour and gut microbiota development in adolescence and adulthood. Brain Behav. Immun. 2017, 59, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Provensi, G.; Schmidt, S.D.; Boehme, M.; Bastiaanssen, T.F.S.; Rani, B.; Costa, A.; Busca, K.; Fouhy, F.; Strain, C.; Stanton, C.; et al. Preventing adolescent stress-induced cognitive and microbiome changes by diet. Proc. Natl. Acad. Sci. USA 2019, 116, 9644–9651. [Google Scholar] [CrossRef] [PubMed]
- Ganzetti, G.S.; Rigamonti, E.; Brambilla, R.; Parolini, C. Microarray analysis of liver gene expression in apoA-I and apoA-IMilano knock-in mouse models. Clin. Res. Nephrol. Kidney Dis. 2019, 1, 1001. [Google Scholar]
- Ogura, Y.; Bonen, D.K.; Inohara, N.; Nicolae, D.L.; Chen, F.F.; Ramos, R.; Britton, H.; Moran, T.; Karaliuskas, R.; Duerr, R.H.; et al. A frameshift mutation in NOD2 associated with susceptibility to Crohn’s disease. Nature 2001, 411, 603–606. [Google Scholar] [CrossRef]
- Parolini, C.; Chiesa, G.; Gong, E.; Caligari, S.; Cortese, M.M.; Koga, T.; Forte, T.M.; Rubin, E.M. Apolipoprotein A-I and the molecular variant apoA-I(Milano): Evaluation of the antiatherogenic effects in knock-in mouse model. Atherosclerosis 2005, 183, 222–229. [Google Scholar] [CrossRef]
- Consortium, U.I.G.; Barrett, J.C.; Lee, J.C.; Lees, C.W.; Prescott, N.J.; Anderson, C.A.; Phillips, A.; Wesley, E.; Parnell, K.; Zhang, H.; et al. Genome-wide association study of ulcerative colitis identifies three new susceptibility loci, including the HNF4A region. Nat. Genet. 2009, 41, 1330–1334. [Google Scholar] [CrossRef]
- Hugot, J.P.; Chamaillard, M.; Zouali, H.; Lesage, S.; Cezard, J.P.; Belaiche, J.; Almer, S.; Tysk, C.; O’Morain, C.A.; Gassull, M.; et al. Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn’s disease. Nature 2001, 411, 599–603. [Google Scholar] [CrossRef] [PubMed]
- McGovern, D.P.; Gardet, A.; Torkvist, L.; Goyette, P.; Essers, J.; Taylor, K.D.; Neale, B.M.; Ong, R.T.; Lagace, C.; Li, C.; et al. Genome-wide association identifies multiple ulcerative colitis susceptibility loci. Nat. Genet. 2010, 42, 332–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wait, R.; Chiesa, G.; Parolini, C.; Miller, I.; Begum, S.; Brambilla, D.; Galluccio, L.; Ballerio, R.; Eberini, I.; Gianazza, E. Reference maps of mouse serum acute-phase proteins: Changes with LPS-induced inflammation and apolipoprotein A-I and A-II transgenes. Proteomics 2005, 5, 4245–4253. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Shi, R.; Zhang, H.; Li, K.; Zhao, Y.; Zhang, R. The Toll-like receptor 4 D299G and T399I polymorphisms are associated with Crohn’s disease and ulcerative colitis: A meta-analysis. Digestion 2010, 81, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Pierik, M.; Joossens, S.; Van Steen, K.; Van Schuerbeek, N.; Vlietinck, R.; Rutgeerts, P.; Vermeire, S. Toll-like receptor-1, -2, and -6 polymorphisms influence disease extension in inflammatory bowel diseases. Inflamm. Bowel. Dis. 2006, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Duchmann, R.; May, E.; Heike, M.; Knolle, P.; Neurath, M.; Meyer zum Buschenfelde, K.H. T cell specificity and cross reactivity towards enterobacteria, bacteroides, bifidobacterium, and antigens from resident intestinal flora in humans. Gut 1999, 44, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Landers, C.J.; Cohavy, O.; Misra, R.; Yang, H.; Lin, Y.C.; Braun, J.; Targan, S.R. Selected loss of tolerance evidenced by Crohn’s disease-associated immune responses to auto- and microbial antigens. Gastroenterology 2002, 123, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Cinquetti, R.; Badi, I.; Campione, M.; Bortoletto, E.; Chiesa, G.; Parolini, C.; Camesasca, C.; Russo, A.; Taramelli, R.; Acquati, F. Transcriptional deregulation and a missense mutation define ANKRD1 as a candidate gene for total anomalous pulmonary venous return. Hum. Mutat. 2008, 29, 468–474. [Google Scholar] [CrossRef]
- Nagao-Kitamoto, H.; Shreiner, A.B.; Gillilland, M.G., 3rd; Kitamoto, S.; Ishii, C.; Hirayama, A.; Kuffa, P.; El-Zaatari, M.; Grasberger, H.; Seekatz, A.M.; et al. Functional Characterization of Inflammatory Bowel Disease-Associated Gut Dysbiosis in Gnotobiotic Mice. Cell Mol. Gastroenterol. Hepatol. 2016, 2, 468–481. [Google Scholar] [CrossRef]
- Machiels, K.; Joossens, M.; Sabino, J.; De Preter, V.; Arijs, I.; Eeckhaut, V.; Ballet, V.; Claes, K.; Van Immerseel, F.; Verbeke, K.; et al. A decrease of the butyrate-producing species Roseburia hominis and Faecalibacterium prausnitzii defines dysbiosis in patients with ulcerative colitis. Gut 2014, 63, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Kho, Z.Y.; Lal, S.K. The Human Gut Microbiome—A Potential Controller of Wellness and Disease. Front. Microbiol. 2018, 9, 1835. [Google Scholar] [CrossRef] [PubMed]
- Vik, R.; Busnelli, M.; Parolini, C.; Bjorndal, B.; Holm, S.; Bohov, P.; Halvorsen, B.; Brattelid, T.; Manzini, S.; Ganzetti, G.S.; et al. An immunomodulating fatty acid analogue targeting mitochondria exerts anti-atherosclerotic effect beyond plasma cholesterol-lowering activity in apoe(-/-) mice. PLoS ONE 2013, 8, e81963. [Google Scholar] [CrossRef] [PubMed]
- Chassaing, B.; Etienne-Mesmin, L.; Gewirtz, A.T. Microbiota-liver axis in hepatic disease. Hepatology 2014, 59, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.M.; Brummer, R.J.; Derrien, M.; MacDonald, T.T.; Troost, F.; Cani, P.D.; Theodorou, V.; Dekker, J.; Meheust, A.; de Vos, W.M.; et al. Homeostasis of the gut barrier and potential biomarkers. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G171–G193. [Google Scholar] [CrossRef] [PubMed]
- Manzini, S.; Pinna, C.; Busnelli, M.; Cinquanta, P.; Rigamonti, E.; Ganzetti, G.S.; Dellera, F.; Sala, A.; Calabresi, L.; Franceschini, G.; et al. Beta2-adrenergic activity modulates vascular tone regulation in lecithin:cholesterol acyltransferase knockout mice. Vasc. Pharmacol. 2015, 74, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Serban, D.E. Microbiota in Inflammatory Bowel Disease Pathogenesis and Therapy: Is It All About Diet? Nutr. Clin. Pract. 2015, 30, 760–779. [Google Scholar] [CrossRef]
- Gruber, L.; Kisling, S.; Lichti, P.; Martin, F.P.; May, S.; Klingenspor, M.; Lichtenegger, M.; Rychlik, M.; Haller, D. High fat diet accelerates pathogenesis of murine Crohn’s disease-like ileitis independently of obesity. PLoS ONE 2013, 8, e71661. [Google Scholar] [CrossRef]
- Pendyala, S.; Walker, J.M.; Holt, P.R. A high-fat diet is associated with endotoxemia that originates from the gut. Gastroenterology. 2012, 142, 1100–1101. [Google Scholar] [CrossRef]
- Cani, P.D.; Bibiloni, R.; Knauf, C.; Waget, A.; Neyrinck, A.M.; Delzenne, N.M.; Burcelin, R. Changes in gut microbiota control metabolic endotoxemia-induced inflammation in high-fat diet-induced obesity and diabetes in mice. Diabetes 2008, 57, 1470–1481. [Google Scholar] [CrossRef]
- Badi, I.; Cinquetti, R.; Frascoli, M.; Parolini, C.; Chiesa, G.; Taramelli, R.; Acquati, F. Intracellular ANKRD1 protein levels are regulated by 26S proteasome-mediated degradation. FEBS Lett. 2009, 583, 2486–2492. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.A.; Gu, W.; Lee, I.A.; Joh, E.H.; Kim, D.H. High fat diet-induced gut microbiota exacerbates inflammation and obesity in mice via the TLR4 signaling pathway. PLoS ONE 2012, 7, e47713. [Google Scholar] [CrossRef] [PubMed]
- Steinhoff-Wagner, J.; Zitnan, R.; Schonhusen, U.; Pfannkuche, H.; Hudakova, M.; Metges, C.C.; Hammon, H.M. Diet effects on glucose absorption in the small intestine of neonatal calves: Importance of intestinal mucosal growth, lactase activity, and glucose transporters. J. Dairy Sci. 2014, 97, 6358–6369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrett, J.S.; Irving, P.M.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Comparison of the prevalence of fructose and lactose malabsorption across chronic intestinal disorders. Aliment. Pharmacol. Ther. 2009, 30, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Medina, M.; Denizot, J.; Dreux, N.; Robin, F.; Billard, E.; Bonnet, R.; Darfeuille-Michaud, A.; Barnich, N. Western diet induces dysbiosis with increased E coli in CEABAC10 mice, alters host barrier function favouring AIEC colonisation. Gut 2014, 63, 116–124. [Google Scholar] [CrossRef] [PubMed]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Derrien, M.; Belzer, C.; de Vos, W.M. Akkermansia muciniphila and its role in regulating host functions. Microb. Pathog. 2017, 106, 171–181. [Google Scholar] [CrossRef]
- Bellenger, J.; Bellenger, S.; Escoula, Q.; Bidu, C.; Narce, M. N-3 polyunsaturated fatty acids: An innovative strategy against obesity and related metabolic disorders, intestinal alteration and gut microbiota dysbiosis. Biochimie 2019, 159, 66–71. [Google Scholar] [CrossRef]
- Everard, A.; Belzer, C.; Geurts, L.; Ouwerkerk, J.P.; Druart, C.; Bindels, L.B.; Guiot, Y.; Derrien, M.; Muccioli, G.G.; Delzenne, N.M.; et al. Cross-talk between Akkermansia muciniphila and intestinal epithelium controls diet-induced obesity. Proc. Natl. Acad. Sci. USA 2013, 110, 9066–9071. [Google Scholar] [CrossRef]
- Jeong, D.Y.; Kim, S.; Son, M.J.; Son, C.Y.; Kim, J.Y.; Kronbichler, A.; Lee, K.H.; Shin, J.I. Induction and maintenance treatment of inflammatory bowel disease: A comprehensive review. Autoimmun. Rev. 2019, 18, 439–454. [Google Scholar] [CrossRef]
- Hudcovic, T.; Stepankova, R.; Cebra, J.; Tlaskalova-Hogenova, H. The role of microflora in the development of intestinal inflammation: Acute and chronic colitis induced by dextran sulfate in germ-free and conventionally reared immunocompetent and immunodeficient mice. Folia Microbiol. (Praha) 2001, 46, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Parolini, C.; Chiesa, G.; Zhu, Y.; Forte, T.; Caligari, S.; Gianazza, E.; Sacco, M.G.; Sirtori, C.R.; Rubin, E.M. Targeted replacement of mouse apolipoprotein A-I with human ApoA-I or the mutant ApoA-IMilano. Evidence of APOA-IM impaired hepatic secretion. J. Biol. Chem. 2003, 278, 4740–4746. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, S.R.; Britton, G.J.; Contijoch, E.J.; Vennaro, O.H.; Mortha, A.; Colombel, J.F.; Grinspan, A.; Clemente, J.C.; Merad, M.; Faith, J.J. Interactions Between Diet and the Intestinal Microbiota Alter Intestinal Permeability and Colitis Severity in Mice. Gastroenterology 2018, 154, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Chirlaque, C.; Aranda, C.J.; Ocon, B.; Capitan-Canadas, F.; Ortega-Gonzalez, M.; Carrero, J.J.; Suarez, M.D.; Zarzuelo, A.; Sanchez de Medina, F.; Martinez-Augustin, O. Germ-free and Antibiotic-treated Mice are Highly Susceptible to Epithelial Injury in DSS Colitis. J. Crohn’s Colitis 2016, 10, 1324–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, H.; Pamp, S.J.; Hill, J.A.; Surana, N.K.; Edelman, S.M.; Troy, E.B.; Reading, N.C.; Villablanca, E.J.; Wang, S.; Mora, J.R.; et al. Gut immune maturation depends on colonization with a host-specific microbiota. Cell 2012, 149, 1578–1593. [Google Scholar] [CrossRef]
- Yu, L.C. Microbiota dysbiosis and barrier dysfunction in inflammatory bowel disease and colorectal cancers: exploring a common ground hypothesis. J. Biomed. Sci. 2018, 25, 79. [Google Scholar] [CrossRef] [PubMed]
- Buck, M.D.; Sowell, R.T.; Kaech, S.M.; Pearce, E.L. Metabolic Instruction of Immunity. Cell 2017, 169, 570–586. [Google Scholar] [CrossRef]
- Kuhn, R.; Lohler, J.; Rennick, D.; Rajewsky, K.; Muller, W. Interleukin-10-deficient mice develop chronic enterocolitis. Cell 1993, 75, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Joossens, M.; De Preter, V.; Ballet, V.; Verbeke, K.; Rutgeerts, P.; Vermeire, S. Effect of oligofructose-enriched inulin (OF-IN) on bacterial composition and disease activity of patients with Crohn’s disease: Results from a double-blinded randomised controlled trial. Gut 2012, 61, 958. [Google Scholar] [CrossRef]
- Wang, Y.; Kasper, L.H. The role of microbiome in central nervous system disorders. Brain Behav. Immun. 2014, 38, 1–12. [Google Scholar] [CrossRef]
- Parian, A.M.; Limketkai, B.N.; Shah, N.D.; Mullin, G.E. Nutraceutical Supplements for Inflammatory Bowel Disease. Nutr. Clin. Pract. 2015, 30, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Belluzzi, A.; Boschi, S.; Brignola, C.; Munarini, A.; Cariani, G.; Miglio, F. Polyunsaturated fatty acids and inflammatory bowel disease. Am. J. Clin. Nutr. 2000, 71, 339S–342S. [Google Scholar] [CrossRef] [PubMed]
- Nieto, N.; Torres, M.I.; Rios, A.; Gil, A. Dietary polyunsaturated fatty acids improve histological and biochemical alterations in rats with experimental ulcerative colitis. J. Nutr. 2002, 132, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Hudert, C.A.; Weylandt, K.H.; Lu, Y.; Wang, J.; Hong, S.; Dignass, A.; Serhan, C.N.; Kang, J.X. Transgenic mice rich in endogenous omega-3 fatty acids are protected from colitis. Proc. Natl. Acad. Sci. USA 2006, 103, 11276–11281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arita, M.; Yoshida, M.; Hong, S.; Tjonahen, E.; Glickman, J.N.; Petasis, N.A.; Blumberg, R.S.; Serhan, C.N. Resolvin E1, an endogenous lipid mediator derived from omega-3 eicosapentaenoic acid, protects against 2,4,6-trinitrobenzene sulfonic acid-induced colitis. Proc. Natl. Acad. Sci. USA 2005, 102, 7671–7676. [Google Scholar] [CrossRef] [Green Version]
- Bidu, C.; Escoula, Q.; Bellenger, S.; Spor, A.; Galan, M.; Geissler, A.; Bouchot, A.; Dardevet, D.; Morio, B.; Cani, P.D.; et al. The Transplantation of omega3 PUFA-Altered Gut Microbiota of fat-1 Mice to Wild-Type Littermates Prevents Obesity and Associated Metabolic Disorders. Diabetes 2018, 67, 1512–1523. [Google Scholar] [CrossRef] [PubMed]
- Raphael, W.; Sordillo, L.M. Dietary polyunsaturated fatty acids and inflammation: The role of phospholipid biosynthesis. Int. J. Mol. Sci. 2013, 14, 21167–21188. [Google Scholar] [CrossRef]
- Tsujikawa, T.; Satoh, J.; Uda, K.; Ihara, T.; Okamoto, T.; Araki, Y.; Sasaki, M.; Fujiyama, Y.; Bamba, T. Clinical importance of n-3 fatty acid-rich diet and nutritional education for the maintenance of remission in Crohn’s disease. J. Gastroenterol. 2000, 35, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Belluzzi, A. N-3 fatty acids for the treatment of inflammatory bowel diseases. Proc. Nutr. Soc. 2002, 61, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Uranga, J.A.; Lopez-Miranda, V.; Lombo, F.; Abalo, R. Food, nutrients and nutraceuticals affecting the course of inflammatory bowel disease. Pharmacol. Rep. 2016, 68, 816–826. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Iheozor-Ejiofor, Z.; Gjuladin-Hellon, T.; Parian, A.; Matarese, L.E.; Bracewell, K.; MacDonald, J.K.; Gordon, M.; Mullin, G.E. Dietary interventions for induction and maintenance of remission in inflammatory bowel disease. Cochrane Database Syst. Rev. 2019, 2, CD012839. [Google Scholar] [CrossRef] [PubMed]
- Statovci, D.; Aguilera, M.; MacSharry, J.; Melgar, S. The Impact of Western Diet and Nutrients on the Microbiota and Immune Response at Mucosal Interfaces. Front. Immunol. 2017, 8, 838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endres, S.; Lorenz, R.; Loeschke, K. Lipid treatment of inflammatory bowel disease. Curr. Opin. Clin. Nutr. Metab. Care 1999, 2, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Sandborn, W.J.; Mittmann, U.; Bar-Meir, S.; D’Haens, G.; Bradette, M.; Cohen, A.; Dallaire, C.; Ponich, T.P.; McDonald, J.W.; et al. Omega-3 free fatty acids for the maintenance of remission in Crohn disease: The EPIC Randomized Controlled Trials. JAMA 2008, 299, 1690–1697. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Shah, P.S.; Steinhart, A.H.; Zlotkin, S.; Griffiths, A.M. Maintenance of remission in inflammatory bowel disease using omega-3 fatty acids (fish oil): A systematic review and meta-analyses. Inflamm. Bowel Dis. 2011, 17, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Romano, C.; Cucchiara, S.; Barabino, A.; Annese, V.; Sferlazzas, C. Usefulness of omega-3 fatty acid supplementation in addition to mesalazine in maintaining remission in pediatric Crohn’s disease: A double-blind, randomized, placebo-controlled study. World J. Gastroenterol. 2005, 11, 7118–7121. [Google Scholar] [CrossRef] [PubMed]
- Belluzzi, A.; Brignola, C.; Campieri, M.; Pera, A.; Boschi, S.; Miglioli, M. Effect of an enteric-coated fish-oil preparation on relapses in Crohn’s disease. N. Engl. J. Med. 1996, 334, 1557–1560. [Google Scholar] [CrossRef]
- Stenson, W.F.; Cort, D.; Rodgers, J.; Burakoff, R.; DeSchryver-Kecskemeti, K.; Gramlich, T.L.; Beeken, W. Dietary supplementation with fish oil in ulcerative colitis. Ann. Intern. Med. 1992, 116, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, D.S.; Cecchini, R.; El Kadri, M.Z.; Rodriguez, M.A.; Burini, R.C.; Dichi, I. Decreased oxidative stress in patients with ulcerative colitis supplemented with fish oil omega-3 fatty acids. Nutrition 2003, 19, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, H.; Daneshzad, E.; Larijani, B.; Bellissimo, N.; Azadbakht, L. Dietary intake of fish, n-3 polyunsaturated fatty acids, and risk of inflammatory bowel disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N.; Khalili, H.; Konijeti, G.G.; Higuchi, L.M.; de Silva, P.; Fuchs, C.S.; Willett, W.C.; Richter, J.M.; Chan, A.T. Long-term intake of dietary fat and risk of ulcerative colitis and Crohn’s disease. Gut 2014, 63, 776–784. [Google Scholar] [CrossRef] [PubMed]
- IBD in EPIC Study Investigators; Tjonneland, A.; Overvad, K.; Bergmann, M.M.; Nagel, G.; Linseisen, J.; Hallmans, G.; Palmqvist, R.; Sjodin, H.; Hagglund, G.; et al. Linoleic acid, a dietary n-6 polyunsaturated fatty acid, and the aetiology of ulcerative colitis: A nested case-control study within a European prospective cohort study. Gut 2009, 58, 1606–1611. [Google Scholar] [CrossRef] [PubMed]
- Marlow, G.; Ellett, S.; Ferguson, I.R.; Zhu, S.; Karunasinghe, N.; Jesuthasan, A.C.; Han, D.Y.; Fraser, A.G.; Ferguson, L.R. Transcriptomics to study the effect of a Mediterranean-inspired diet on inflammation in Crohn’s disease patients. Hum. Genom. 2013, 7, 24. [Google Scholar] [CrossRef] [PubMed]
- Prossomariti, A.; Scaioli, E.; Piazzi, G.; Fazio, C.; Bellanova, M.; Biagi, E.; Candela, M.; Brigidi, P.; Consolandi, C.; Balbi, T.; et al. Short-term treatment with eicosapentaenoic acid improves inflammation and affects colonic differentiation markers and microbiota in patients with ulcerative colitis. Sci. Rep. 2017, 7, 7458. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, M.A.; Sonnenburg, J.L. Eating for two: How metabolism establishes interspecies interactions in the gut. Cell Host Microbe 2011, 10, 336–347. [Google Scholar] [CrossRef] [PubMed]
- Caligari, S.; Chiesa, G.; Johnson, S.K.; Camisassi, D.; Gilio, D.; Marchesi, M.; Parolini, C.; Rubio, L.A.; Sirtori, C.R. Lupin (Lupinus albus) protein isolate (L-ISO) has adequate nutritional value and reduces large intestinal weight in rats after restricted and ad libitum feeding. Ann. Nutr. Metab. 2006, 50, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, M.; Parolini, C.; Diani, E.; Rigamonti, E.; Cornelli, L.; Arnoldi, A.; Sirtori, C.R.; Chiesa, G. Hypolipidaemic and anti-atherosclerotic effects of lupin proteins in a rabbit model. Br. J. Nutr. 2008, 100, 707–710. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Hu, C.A.; Kovacs-Nolan, J.; Mine, Y. Bioactive dietary peptides and amino acids in inflammatory bowel disease. Amino Acids 2015, 47, 2127–2141. [Google Scholar] [CrossRef]
- Faure, M.; Mettraux, C.; Moennoz, D.; Godin, J.P.; Vuichoud, J.; Rochat, F.; Breuille, D.; Obled, C.; Corthesy-Theulaz, I. Specific amino acids increase mucin synthesis and microbiota in dextran sulfate sodium-treated rats. J. Nutr. 2006, 136, 1558–1564. [Google Scholar] [CrossRef]
- Kim, C.J.; Kovacs-Nolan, J.; Yang, C.; Archbold, T.; Fan, M.Z.; Mine, Y. L-cysteine supplementation attenuates local inflammation and restores gut homeostasis in a porcine model of colitis. Biochim. Biophys. Acta 2009, 1790, 1161–1169. [Google Scholar] [CrossRef]
- Marchesi, M.; Parolini, C.; Valetti, C.; Mangione, P.; Obici, L.; Giorgetti, S.; Raimondi, S.; Donadei, S.; Gregorini, G.; Merlini, G.; et al. The intracellular quality control system down-regulates the secretion of amyloidogenic apolipoprotein A-I variants: A possible impact on the natural history of the disease. Biochim. Biophys. Acta 2011, 1812, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinn, S.J.; Ye, C.P.; Diaz, R.; Kifor, O.; Bai, M.; Vassilev, P.; Brown, E. The Ca2+-sensing receptor: A target for polyamines. Am. J. Physiol. 1997, 273, C1315–C1323. [Google Scholar] [CrossRef] [PubMed]
- Parolini, C.; Manzini, S.; Busnelli, M.; Rigamonti, E.; Marchesi, M.; Diani, E.; Sirtori, C.R.; Chiesa, G. Effect of the combinations between pea proteins and soluble fibres on cholesterolaemia and cholesterol metabolism in rats. Br. J. Nutr. 2013, 110, 1394–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990-2020: A systematic review and meta-analysis. Lancet. Glob. Health. 2017, 5, e1221–e1234. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K.; Leducq Transatlantic Network on, A. Inflammation in atherosclerosis: From pathophysiology to practice. J. Am. Coll. Cardiol. 2009, 54, 2129–2138. [Google Scholar] [CrossRef] [PubMed]
- Parolini, C.; Marchesi, M.; Chiesa, G. HDL therapy for the treatment of cardiovascular diseases. Curr. Vasc. Pharmacol. 2009, 7, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Pronin, A.; Pham, D.; An, W.; Dvoriantchikova, G.; Reshetnikova, G.; Qiao, J.; Kozhekbaeva, Z.; Reiser, A.E.; Slepak, V.Z.; Shestopalov, V.I. Inflammasome Activation Induces Pyroptosis in the Retina Exposed to Ocular Hypertension Injury. Front. Mol. Neurosci. 2019, 12, 36. [Google Scholar] [CrossRef] [Green Version]
- Xavier, R.J.; Podolsky, D.K. Unravelling the pathogenesis of inflammatory bowel disease. Nature 2007, 448, 427–434. [Google Scholar] [CrossRef]
- Ridker, P.M.; Howard, C.P.; Walter, V.; Everett, B.; Libby, P.; Hensen, J.; Thuren, T.; Group, C.P.I. Effects of interleukin-1beta inhibition with canakinumab on hemoglobin A1c, lipids, C-reactive protein, interleukin-6, and fibrinogen: A phase IIb randomized, placebo-controlled trial. Circulation 2012, 126, 2739–2748. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- SanGiovanni, J.P.; Chew, E.Y. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Progr. Retin. Eye Res. 2005, 24, 87–138. [Google Scholar] [CrossRef] [PubMed]
- Parolini, C.; Marchesi, M.; Lorenzon, P.; Castano, M.; Balconi, E.; Miragoli, L.; Chaabane, L.; Morisetti, A.; Lorusso, V.; Martin, B.J.; et al. Dose-related effects of repeated ETC-216 (recombinant apolipoprotein A-I Milano/1-palmitoyl-2-oleoyl phosphatidylcholine complexes) administrations on rabbit lipid-rich soft plaques: In vivo assessment by intravascular ultrasound and magnetic resonance imaging. J. Am. Coll. Cardiol. 2008, 51, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.L.; Bazan, N.G. Membrane docosahexaenoate is supplied to the developing brain and retina by the liver. Proc. Natl. Acad. Sci. USA 1989, 86, 2903–2907. [Google Scholar] [CrossRef] [PubMed]
- de Urquiza, A.M.; Liu, S.; Sjoberg, M.; Zetterstrom, R.H.; Griffiths, W.; Sjovall, J.; Perlmann, T. Docosahexaenoic acid, a ligand for the retinoid X receptor in mouse brain. Science 2000, 290, 2140–2144. [Google Scholar] [CrossRef] [PubMed]
- Oresic, M.; Seppanen-Laakso, T.; Yetukuri, L.; Backhed, F.; Hanninen, V. Gut microbiota affects lens and retinal lipid composition. Exp. Eye Res. 2009, 89, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Horai, R.; Zarate-Blades, C.R.; Dillenburg-Pilla, P.; Chen, J.; Kielczewski, J.L.; Silver, P.B.; Jittayasothorn, Y.; Chan, C.C.; Yamane, H.; Honda, K.; et al. Microbiota-Dependent Activation of an Autoreactive T Cell Receptor Provokes Autoimmunity in an Immunologically Privileged Site. Immunity 2015, 43, 343–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, Y.K.; Janowitz, C.; Metea, C.; Asquith, M.; Karstens, L.; Rosenbaum, J.T.; Lin, P. Short chain fatty acids ameliorate immune-mediated uveitis partially by altering migration of lymphocytes from the intestine. Sci. Rep. 2017, 7, 11745. [Google Scholar] [CrossRef]
- Wen, X.; Hu, X.; Miao, L.; Ge, X.; Deng, Y.; Bible, P.W.; Wei, L. Epigenetics, microbiota, and intraocular inflammation: New paradigms of immune regulation in the eye. Prog. Retin. Eye Res. 2018, 64, 84–95. [Google Scholar] [CrossRef]
- Pedrosa, A.C.; Sousa, T.; Pinheiro-Costa, J.; Beato, J.; Falcao, M.S.; Falcao-Reis, F.; Carneiro, A. Treatment of Neovascular Age-Related Macular Degeneration with Anti-VEGF Agents: Predictive Factors of Long-Term Visual Outcomes. J. Ophthalmol. 2017, 2017, 4263017. [Google Scholar] [CrossRef]
- Horani, M.; Mahmood, S.; Aslam, T.M. Macular Atrophy of the Retinal Pigment Epithelium in Patients with Neovascular Age-Related Macular Degeneration: What is the Link? Part I: A Review of Disease Characterization and Morphological Associations. Ophthalmol. Ther. 2019. [Google Scholar] [CrossRef]
- Jager, R.D.; Mieler, W.F.; Miller, J.W. Age-related macular degeneration. N. Engl. J. Med. 2008, 358, 2606–2617. [Google Scholar] [CrossRef]
- Anderson, D.H.; Radeke, M.J.; Gallo, N.B.; Chapin, E.A.; Johnson, P.T.; Curletti, C.R.; Hancox, L.S.; Hu, J.; Ebright, J.N.; Malek, G.; et al. The pivotal role of the complement system in aging and age-related macular degeneration: Hypothesis re-visited. Prog. Retin. Eye Res. 2010, 29, 95–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.; Xu, H. Parainflammation, chronic inflammation, and age-related macular degeneration. J. Leukoc. Biol. 2015, 98, 713–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, E.L.; Wang, A.Y.; Jobling, A.I.; Rutar, M.V.; Greferath, U.; Gu, B.; Vessey, K.A. Targeting P2X7 receptors as a means for treating retinal disease. Drug Discov. Today 2019. [Google Scholar] [CrossRef] [PubMed]
- Mares-Perlman, J.A.; Fisher, A.I.; Klein, R.; Palta, M.; Block, G.; Millen, A.E.; Wright, J.D. Lutein and zeaxanthin in the diet and serum and their relation to age-related maculopathy in the third national health and nutrition examination survey. Am. J. Epidemiol. 2001, 153, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Age-Related Eye Disease Study Research Group; SanGiovanni, J.P.; Chew, E.Y.; Clemons, T.E.; Ferris, F.L., 3rd; Gensler, G.; Lindblad, A.S.; Milton, R.C.; Seddon, J.M.; Sperduto, R.D. The relationship of dietary carotenoid and vitamin A, E, and C intake with age-related macular degeneration in a case-control study: AREDS Report No. 22. Arch. Ophthalmol. 2007, 125, 1225–1232. [Google Scholar] [CrossRef] [PubMed]
- Delcourt, C.; Carriere, I.; Delage, M.; Barberger-Gateau, P.; Schalch, W.; Group, P.S. Plasma lutein and zeaxanthin and other carotenoids as modifiable risk factors for age-related maculopathy and cataract: The POLA Study. Investig. Ophthalmol. Vis. Sci. 2006, 47, 2329–2335. [Google Scholar] [CrossRef] [PubMed]
- Tuo, J.; Ross, R.J.; Herzlich, A.A.; Shen, D.; Ding, X.; Zhou, M.; Coon, S.L.; Hussein, N.; Salem, N., Jr.; Chan, C.C. A high omega-3 fatty acid diet reduces retinal lesions in a murine model of macular degeneration. Am. J. Pathol. 2009, 175, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Christen, W.G.; Schaumberg, D.A.; Glynn, R.J.; Buring, J.E. Dietary omega-3 fatty acid and fish intake and incident age-related macular degeneration in women. Arch. Ophthalmol. 2011, 129, 921–929. [Google Scholar] [CrossRef]
- Kvansakul, J.; Rodriguez-Carmona, M.; Edgar, D.F.; Barker, F.M.; Kopcke, W.; Schalch, W.; Barbur, J.L. Supplementation with the carotenoids lutein or zeaxanthin improves human visual performance. Ophthalmic Physiol. Opt. 2006, 26, 362–371. [Google Scholar] [CrossRef]
- Trieschmann, M.; Beatty, S.; Nolan, J.M.; Hense, H.W.; Heimes, B.; Austermann, U.; Fobker, M.; Pauleikhoff, D. Changes in macular pigment optical density and serum concentrations of its constituent carotenoids following supplemental lutein and zeaxanthin: The LUNA study. Exp. Eye Res. 2007, 84, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Connolly, E.E.; Beatty, S.; Thurnham, D.I.; Loughman, J.; Howard, A.N.; Stack, J.; Nolan, J.M. Augmentation of macular pigment following supplementation with all three macular carotenoids: An exploratory study. Curr. Eye Res. 2010, 35, 335–351. [Google Scholar] [CrossRef]
- Group, A.R.; Chew, E.Y.; Clemons, T.; SanGiovanni, J.P.; Danis, R.; Domalpally, A.; McBee, W.; Sperduto, R.; Ferris, F.L. The Age-Related Eye Disease Study 2 (AREDS2): Study design and baseline characteristics (AREDS2 report number 1). Ophthalmology 2012, 119, 2282–2289. [Google Scholar] [CrossRef]
- Krinsky, N.I.; Landrum, J.T.; Bone, R.A. Biologic mechanisms of the protective role of lutein and zeaxanthin in the eye. Annu. Rev. Nutr. 2003, 23, 171–201. [Google Scholar] [CrossRef]
- SanGiovanni, J.P.; Chew, E.Y.; Agron, E.; Clemons, T.E.; Ferris, F.L., 3rd; Gensler, G.; Lindblad, A.S.; Milton, R.C.; Seddon, J.M.; Klein, R.; et al. The relationship of dietary omega-3 long-chain polyunsaturated fatty acid intake with incident age-related macular degeneration: AREDS report no. 23. Arch. Ophthalmol. 2008, 126, 1274–1279. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Cho, E.; Giovannucci, E.L.; Rosner, B.A.; Sastry, S.M.; Willett, W.C.; Schaumberg, D.A. Dietary Intakes of Eicosapentaenoic Acid and Docosahexaenoic Acid and Risk of Age-Related Macular Degeneration. Ophthalmology 2017, 124, 634–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delyfer, M.N.; Buaud, B.; Korobelnik, J.F.; Rougier, M.B.; Schalch, W.; Etheve, S.; Vaysse, C.; Combe, N.; Goff, M.L.; Wolf-Schnurrbusch, U.E.; et al. Association of macular pigment density with plasma omega-3 fatty acids: The PIMAVOSA study. Investig. Ophthalmol. Vis. Sci. 2012, 53, 1204–1210. [Google Scholar] [CrossRef]
- Liu, A.; Chang, J.; Lin, Y.; Shen, Z.; Bernstein, P.S. Long-chain and very long-chain polyunsaturated fatty acids in ocular aging and age-related macular degeneration. J. Lipid Res. 2010, 51, 3217–3229. [Google Scholar] [CrossRef] [Green Version]
- Ramkumar, H.L.; Tuo, J.; Shen, D.F.; Zhang, J.; Cao, X.; Chew, E.Y.; Chan, C.C. Nutrient supplementation with n3 polyunsaturated fatty acids, lutein, and zeaxanthin decrease A2E accumulation and VEGF expression in the retinas of Ccl2/Cx3cr1-deficient mice on Crb1rd8 background. J. Nutr. 2013, 143, 1129–1135. [Google Scholar] [CrossRef]
- Parolini, C.; Rigamonti, E.; Marchesi, M.; Busnelli, M.; Cinquanta, P.; Manzini, S.; Sirtori, C.R.; Chiesa, G. Cholesterol-lowering effect of dietary Lupinus angustifolius proteins in adult rats through regulation of genes involved in cholesterol homeostasis. Food Chem. 2012, 132, 1475–1479. [Google Scholar] [CrossRef]
- Prokopiou, E.; Kolovos, P.; Kalogerou, M.; Neokleous, A.; Papagregoriou, G.; Deltas, C.; Malas, S.; Georgiou, T. Therapeutic potential of omega-3 fatty acids supplementation in a mouse model of dry macular degeneration. BMJ Open Ophthalmol. 2017, 1, e000056. [Google Scholar] [CrossRef] [Green Version]
- Georgiou, T.; Wen, Y.T.; Chang, C.H.; Kolovos, P.; Kalogerou, M.; Prokopiou, E.; Neokleous, A.; Huang, C.T.; Tsai, R.K. Neuroprotective Effects of Omega-3 Polyunsaturated Fatty Acids in a Rat Model of Anterior Ischemic Optic Neuropathy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- Jun, B.; Mukherjee, P.K.; Asatryan, A.; Kautzmann, M.A.; Heap, J.; Gordon, W.C.; Bhattacharjee, S.; Yang, R.; Petasis, N.A.; Bazan, N.G. Elovanoids are novel cell-specific lipid mediators necessary for neuroprotective signaling for photoreceptor cell integrity. Sci. Rep. 2017, 7, 5279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Wu, Y.; Meng, Y.F.; Xing, Q.; Tao, J.J.; Lu, J. Fish Consumption and Age-Related Macular Degeneration Incidence: A Meta-Analysis and Systematic Review of Prospective Cohort Studies. Nutrients 2016, 8, 743. [Google Scholar] [CrossRef] [PubMed]
- Andriessen, E.M.; Wilson, A.M.; Mawambo, G.; Dejda, A.; Miloudi, K.; Sennlaub, F.; Sapieha, P. Gut microbiota influences pathological angiogenesis in obesity-driven choroidal neovascularization. EMBO Mol. Med. 2016, 8, 1366–1379. [Google Scholar] [CrossRef] [PubMed]
- Rowan, S.; Jiang, S.; Korem, T.; Szymanski, J.; Chang, M.L.; Szelog, J.; Cassalman, C.; Dasuri, K.; McGuire, C.; Nagai, R.; et al. Involvement of a gut-retina axis in protection against dietary glycemia-induced age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2017, 114, E4472–E4481. [Google Scholar] [CrossRef]
- Rizzatti, G.; Lopetuso, L.R.; Gibiino, G.; Binda, C.; Gasbarrini, A. Proteobacteria: A Common Factor in Human Diseases. Biomed. Res. Int. 2017, 2017, 9351507. [Google Scholar] [CrossRef]
- Lin, P. Importance of the intestinal microbiota in ocular inflammatory diseases: A review. Clin. Exp. Ophthalmol. 2019, 47, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Chiu, C.J.; Chang, M.L.; Zhang, F.F.; Li, T.; Gensler, G.; Schleicher, M.; Taylor, A. The relationship of major American dietary patterns to age-related macular degeneration. Am. J. Ophthalmol. 2014, 158, 118–127. [Google Scholar] [CrossRef]
- Quigley, H.A. Open-angle glaucoma. N. Engl. J. Med. 1993, 328, 1097–1106. [Google Scholar] [CrossRef]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Sowka, J. Pigment dispersion syndrome and pigmentary glaucoma. Optometry 2004, 75, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Brown, K.M.; Stephan, D.A.; Morrison, J.C.; Johnson, E.C.; Tomarev, S.I. Microarray analysis of changes in mRNA levels in the rat retina after experimental elevation of intraocular pressure. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Tezel, G.; Wax, M.B.; Edward, D.P. Matrix metalloproteinases and tumor necrosis factor alpha in glaucomatous optic nerve head. Arch. Ophthalmol. 2000, 118, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Li, F.; Kong, L.; Tomita, H.; Li, C.; Cao, W. Involvement of inflammation, degradation, and apoptosis in a mouse model of glaucoma. J. Biol. Chem. 2005, 280, 31240–31248. [Google Scholar] [CrossRef] [PubMed]
- Chi, W.; Li, F.; Chen, H.; Wang, Y.; Zhu, Y.; Yang, X.; Zhu, J.; Wu, F.; Ouyang, H.; Ge, J.; et al. Caspase-8 promotes NLRP1/NLRP3 inflammasome activation and IL-1beta production in acute glaucoma. Proc. Natl. Acad. Sci. USA 2014, 111, 11181–11186. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Li, X.; Wang, W.; Mo, J.S.; Kaplan, H.; Cooper, N.G. Early Involvement of Immune/Inflammatory Response Genes in Retinal Degeneration in DBA/2J Mice. Ophthalmol. Eye Dis. 2010, 1, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Conlon, R.; Saheb, H.; Ahmed, I.I. Glaucoma treatment trends: A review. Can. J. Ophthalmol. 2017, 52, 114–124. [Google Scholar] [CrossRef]
- Seddon, J.M.; Cote, J.; Rosner, B. Progression of age-related macular degeneration: Association with dietary fat, transunsaturated fat, nuts, and fish intake. Arch. Ophthalmol. 2003, 121, 1728–1737. [Google Scholar] [CrossRef]
- Smith, W.; Mitchell, P.; Leeder, S.R. Dietary fat and fish intake and age-related maculopathy. Arch. Ophthalmol. 2000, 118, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Hodge, W.G.; Barnes, D.; Schachter, H.M.; Pan, Y.I.; Lowcock, E.C.; Zhang, L.; Sampson, M.; Morrison, A.; Tran, K.; Miguelez, M.; et al. The evidence for efficacy of omega-3 fatty acids in preventing or slowing the progression of retinitis pigmentosa: A systematic review. Can. J. Ophthalmol. 2006, 41, 481–490. [Google Scholar] [CrossRef]
- Tellez-Vazquez, J. Omega-3 fatty acid supplementation improves dry eye symptoms in patients with glaucoma: Results of a prospective multicenter study. Clin. Ophthalmol. 2016, 10, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.; Magulike, N.; Ghebremeskel, K.; Crawford, M. Primary open-angle glaucoma patients have reduced levels of blood docosahexaenoic and eicosapentaenoic acids. Prostaglandins Leukot. Essent. Fatty Acids 2006, 74, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Kalogerou, M.; Kolovos, P.; Prokopiou, E.; Papagregoriou, G.; Deltas, C.; Malas, S.; Georgiou, T. Omega-3 fatty acids protect retinal neurons in the DBA/2J hereditary glaucoma mouse model. Exp. Eye Res. 2018, 167, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Prokopiou, E.; Kolovos, P.; Kalogerou, M.; Neokleous, A.; Nicolaou, O.; Sokratous, K.; Kyriacou, K.; Georgiou, T. Omega-3 Fatty Acids Supplementation: Therapeutic Potential in a Mouse Model of Stargardt Disease. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2757–2767. [Google Scholar] [CrossRef] [PubMed]
- Spite, M.; Claria, J.; Serhan, C.N. Resolvins, specialized proresolving lipid mediators, and their potential roles in metabolic diseases. Cell Metab. 2014, 19, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Lafuente, M.P.; Villegas-Perez, M.P.; Selles-Navarro, I.; Mayor-Torroglosa, S.; Miralles de Imperial, J.; Vidal-Sanz, M. Retinal ganglion cell death after acute retinal ischemia is an ongoing process whose severity and duration depends on the duration of the insult. Neuroscience 2002, 109, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Grozdanic, S.D.; Kwon, Y.H.; Sakaguchi, D.S.; Kardon, R.H.; Sonea, I.M. Functional evaluation of retina and optic nerve in the rat model of chronic ocular hypertension. Exp. Eye Res. 2004, 79, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Mukaida, Y.; Machida, S.; Masuda, T.; Tazawa, Y. Correlation of retinal function with retinal histopathology following ischemia-reperfusion in rat eyes. Curr. Eye Res. 2004, 28, 381–389. [Google Scholar] [CrossRef]
- Mayor-Torroglosa, S.; De la Villa, P.; Rodriguez, M.E.; Lopez-Herrera, M.P.; Aviles-Trigueros, M.; Garcia-Aviles, A.; de Imperial, J.M.; Villegas-Perez, M.P.; Vidal-Sanz, M. Ischemia results 3 months later in altered ERG, degeneration of inner layers, and deafferented tectum: Neuroprotection with brimonidine. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3825–3835. [Google Scholar] [CrossRef]
- Schnebelen, C.; Pasquis, B.; Salinas-Navarro, M.; Joffre, C.; Creuzot-Garcher, C.P.; Vidal-Sanz, M.; Bron, A.M.; Bretillon, L.; Acar, N. A dietary combination of omega-3 and omega-6 polyunsaturated fatty acids is more efficient than single supplementations in the prevention of retinal damage induced by elevation of intraocular pressure in rats. Graefes Arch. Clin. Exp. Ophthalmol. 2009, 247, 1191–1203. [Google Scholar] [CrossRef] [PubMed]
- Bazan, N.G. Cell survival matters: Docosahexaenoic acid signaling, neuroprotection and photoreceptors. Trends Neurosci. 2006, 29, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Schnebelen, C.; Gregoire, S.; Pasquis, B.; Joffre, C.; Creuzot-Garcher, C.P.; Bron, A.M.; Bretillon, L.; Acar, N. Dietary n-3 and n-6 PUFA enhance DHA incorporation in retinal phospholipids without affecting PGE(1) and PGE (2) levels. Lipids 2009, 44, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Rigamonti, E.; Parolini, C.; Marchesi, M.; Diani, E.; Brambilla, S.; Sirtori, C.R.; Chiesa, G. Hypolipidemic effect of dietary pea proteins: Impact on genes regulating hepatic lipid metabolism. Mol. Nutr. Food Res. 2010, 54, S24–S30. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Cho, K.S.; Vu, T.H.K.; Shen, C.H.; Kaur, M.; Chen, G.; Mathew, R.; McHam, M.L.; Fazelat, A.; Lashkari, K.; et al. Commensal microflora-induced T cell responses mediate progressive neurodegeneration in glaucoma. Nat. Commun. 2018, 9, 3209. [Google Scholar] [CrossRef] [PubMed]
- Morita, Y.; Jounai, K.; Sakamoto, A.; Tomita, Y.; Sugihara, Y.; Suzuki, H.; Ohshio, K.; Otake, M.; Fujiwara, D.; Kanauchi, O.; et al. Long-term intake of Lactobacillus paracasei KW3110 prevents age-related chronic inflammation and retinal cell loss in physiologically aged mice. Aging 2018, 10, 2723–2740. [Google Scholar] [CrossRef] [PubMed]
- Veckman, V.; Miettinen, M.; Matikainen, S.; Lande, R.; Giacomini, E.; Coccia, E.M.; Julkunen, I. Lactobacilli and streptococci induce inflammatory chemokine production in human macrophages that stimulates Th1 cell chemotaxis. J. Leukoc. Biol. 2003, 74, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Schunck, W.H.; Konkel, A.; Fischer, R.; Weylandt, K.H. Therapeutic potential of omega-3 fatty acid-derived epoxyeicosanoids in cardiovascular and inflammatory diseases. Pharmacol. Ther. 2018, 183, 177–204. [Google Scholar] [CrossRef]
- Markowiak, P.; Slizewska, K. Effects of Probiotics, Prebiotics, and Synbiotics on Human Health. Nutrients 2017, 9, 1021. [Google Scholar] [CrossRef]
- Sommer, F.; Anderson, J.M.; Bharti, R.; Raes, J.; Rosenstiel, P. The resilience of the intestinal microbiota influences health and disease. Nat. Rev. Microbiol. 2017, 15, 630–638. [Google Scholar] [CrossRef]
Figure 1.
The therapeutic potential of marine n-3 polyunsaturated fatty acids (PUFAs) in human disease.
Figure 1.
The therapeutic potential of marine n-3 polyunsaturated fatty acids (PUFAs) in human disease.

Figure 2.
The specialized pro-resolving mediators (SPMs) biosynthetic route and physiologic actions. EPA, eicosapentaenoic acid; DPA, docosapentaenoic acid; DHA, docosahexaenoic acid; Elovl5, ELOVL fatty Acid Elongase 5; Elovl2, ELOVL fatty Acid Elongase 2; Fads2, Fatty Acid Desaturase 2.
Figure 2.
The specialized pro-resolving mediators (SPMs) biosynthetic route and physiologic actions. EPA, eicosapentaenoic acid; DPA, docosapentaenoic acid; DHA, docosahexaenoic acid; Elovl5, ELOVL fatty Acid Elongase 5; Elovl2, ELOVL fatty Acid Elongase 2; Fads2, Fatty Acid Desaturase 2.

Figure 3.
n-3 PUFAs and SPMs interplay with gut microbiota and the immune system.

Figure 4.
The pathogenic factors involved in the development of Crohn’s disease (CD) and ulcerative colitis (UC).
Figure 4.
The pathogenic factors involved in the development of Crohn’s disease (CD) and ulcerative colitis (UC).

Figure 5.
Altered dietary habits, dysbiosis and leaky gut, and low grade inflammation, together with aging, smoking and light exposure may influence the risk and progression of age-related macular degeneration (AMD) and glaucoma.
Figure 5.
Altered dietary habits, dysbiosis and leaky gut, and low grade inflammation, together with aging, smoking and light exposure may influence the risk and progression of age-related macular degeneration (AMD) and glaucoma.

© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Parolini, C. Effects of Fish n-3 PUFAs on Intestinal Microbiota and Immune System. Mar. Drugs 2019, 17, 374. https://doi.org/10.3390/md17060374
AMA Style
Parolini C. Effects of Fish n-3 PUFAs on Intestinal Microbiota and Immune System. Marine Drugs. 2019; 17(6):374. https://doi.org/10.3390/md17060374
Chicago/Turabian StyleParolini, Cinzia. 2019. "Effects of Fish n-3 PUFAs on Intestinal Microbiota and Immune System" Marine Drugs 17, no. 6: 374. https://doi.org/10.3390/md17060374
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.