
Bone Remodeling Interaction with Magnesium Alloy Implants Studied by SEM and EDX
 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biomaterial Preparation
2.2. Surgical Procedure
2.3. Bioresorption Monitoring
3. Results
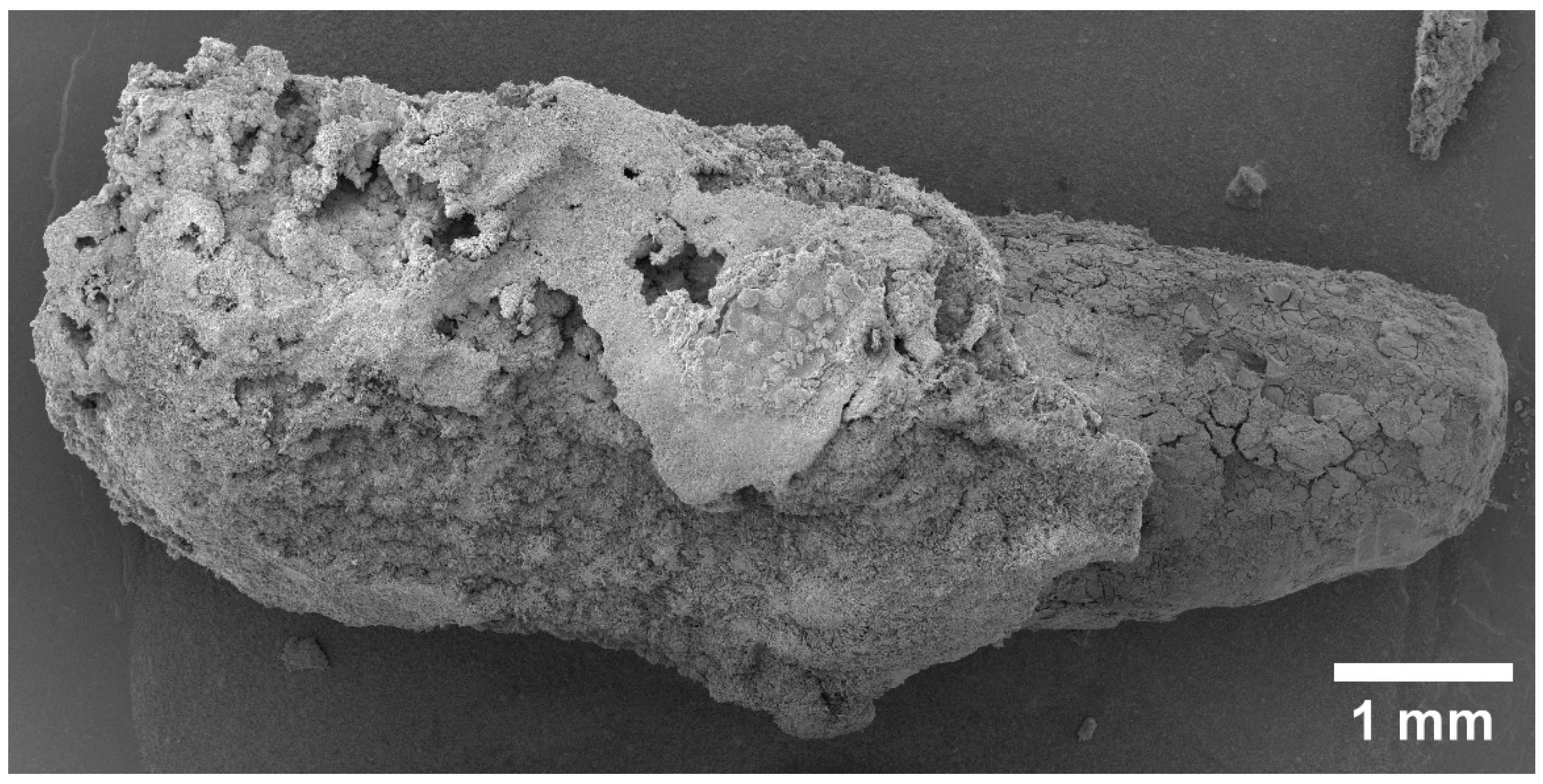
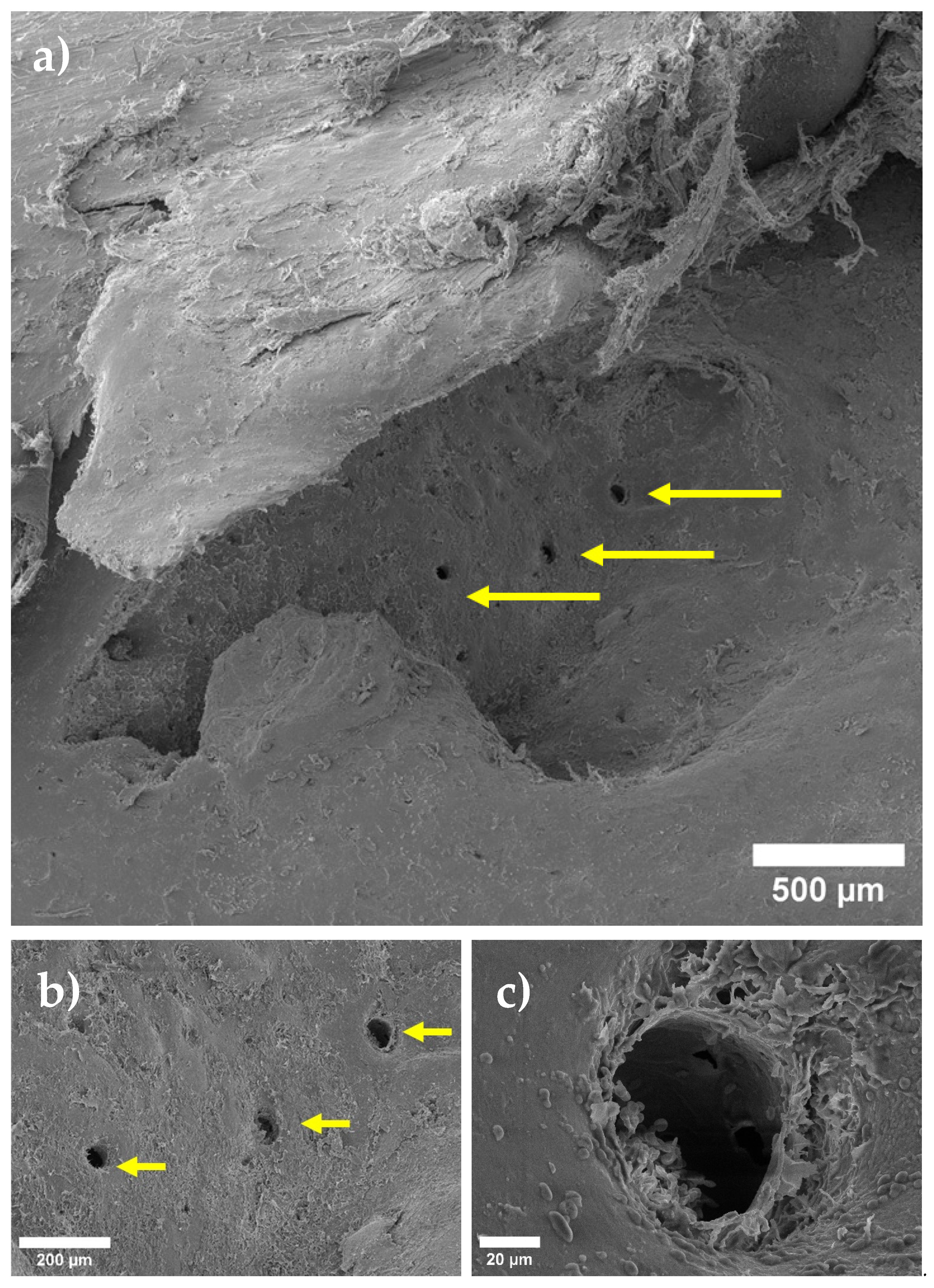
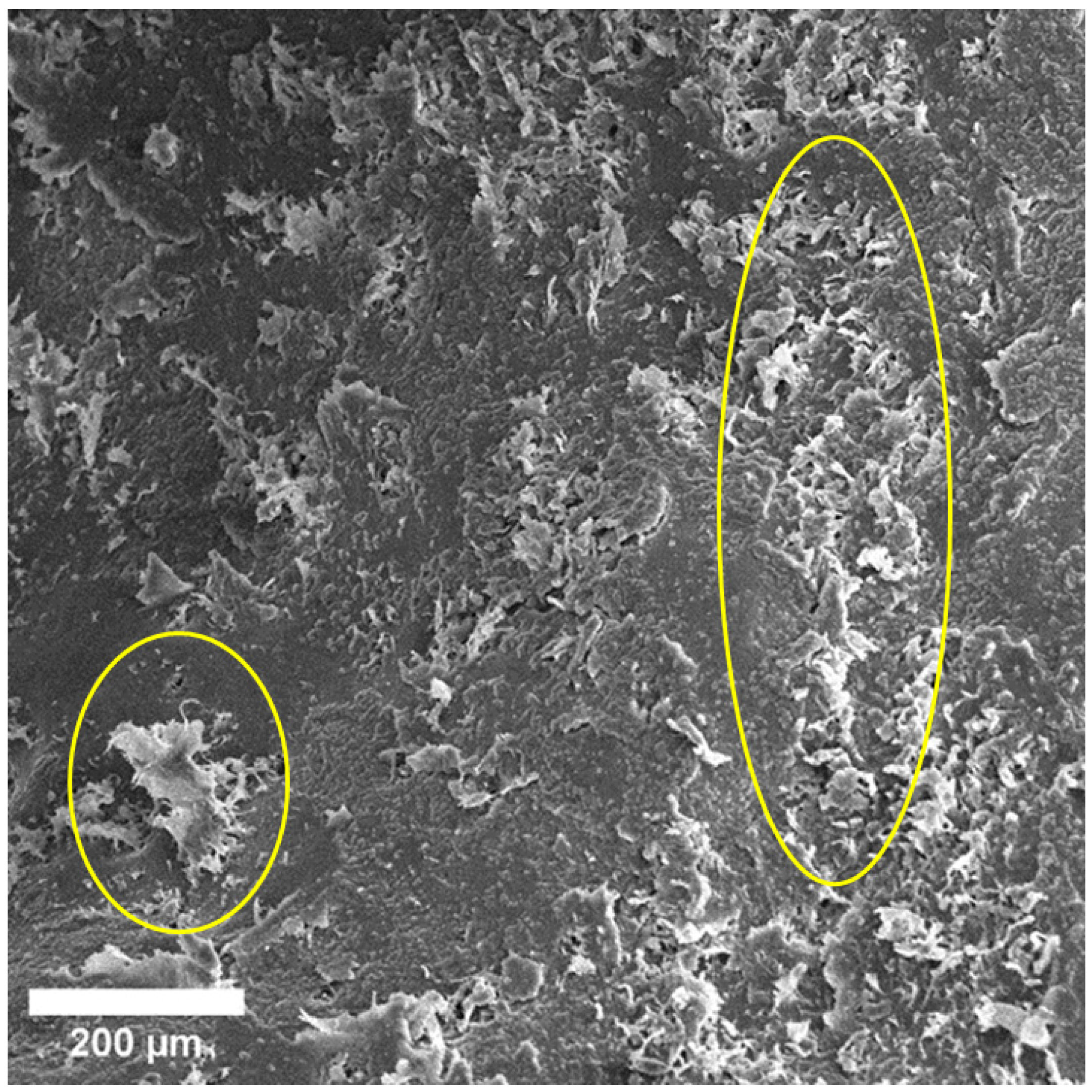
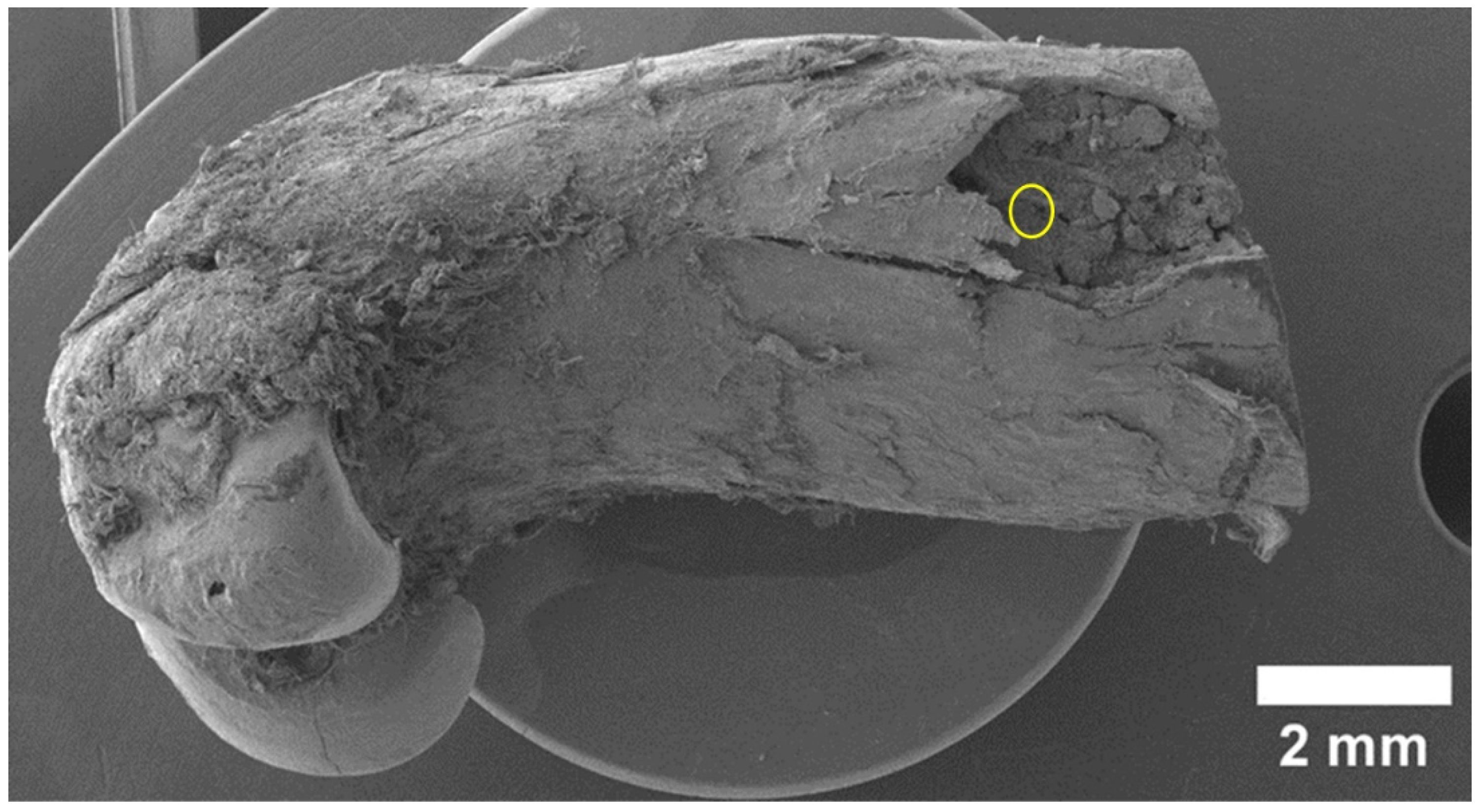
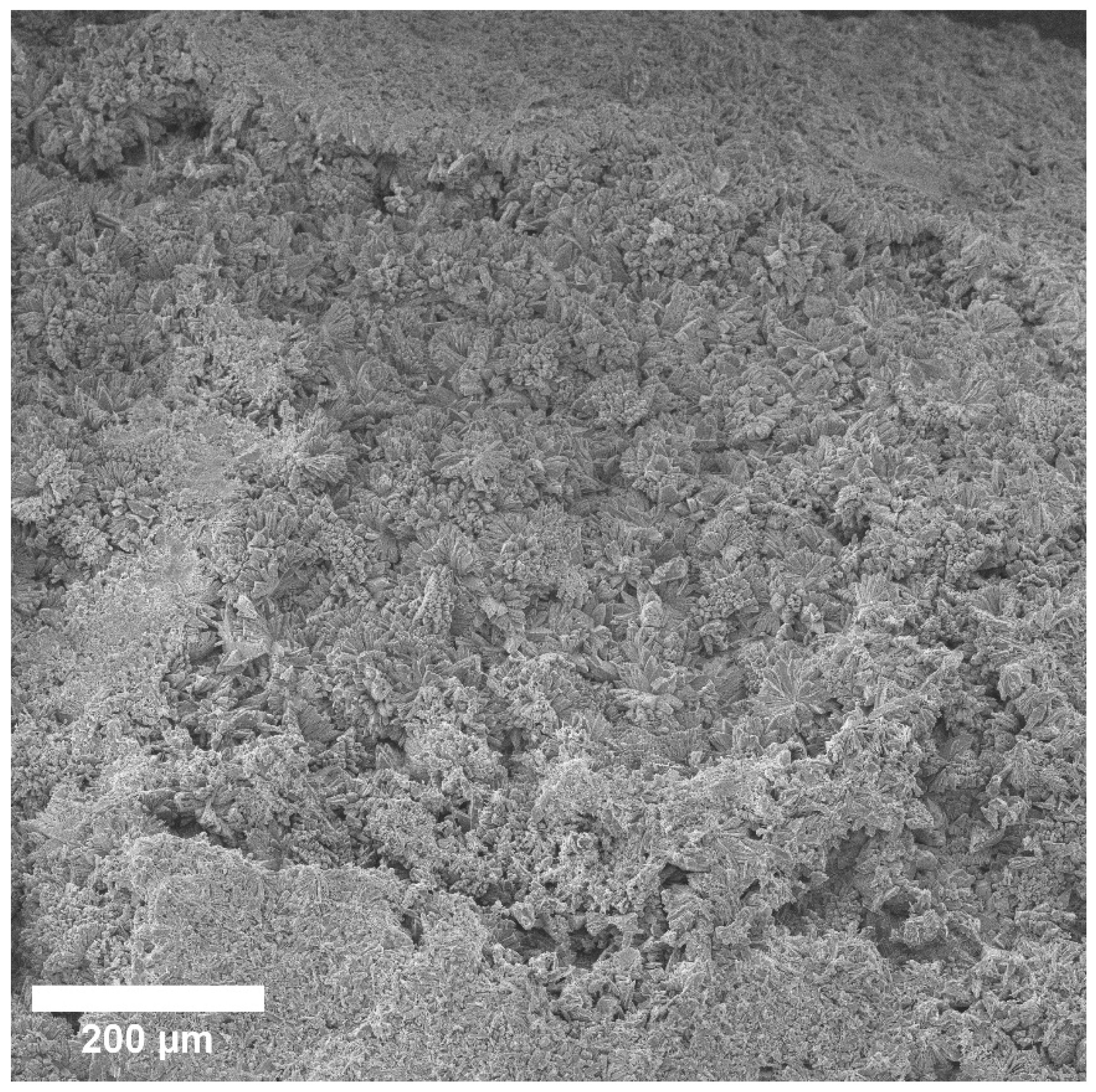
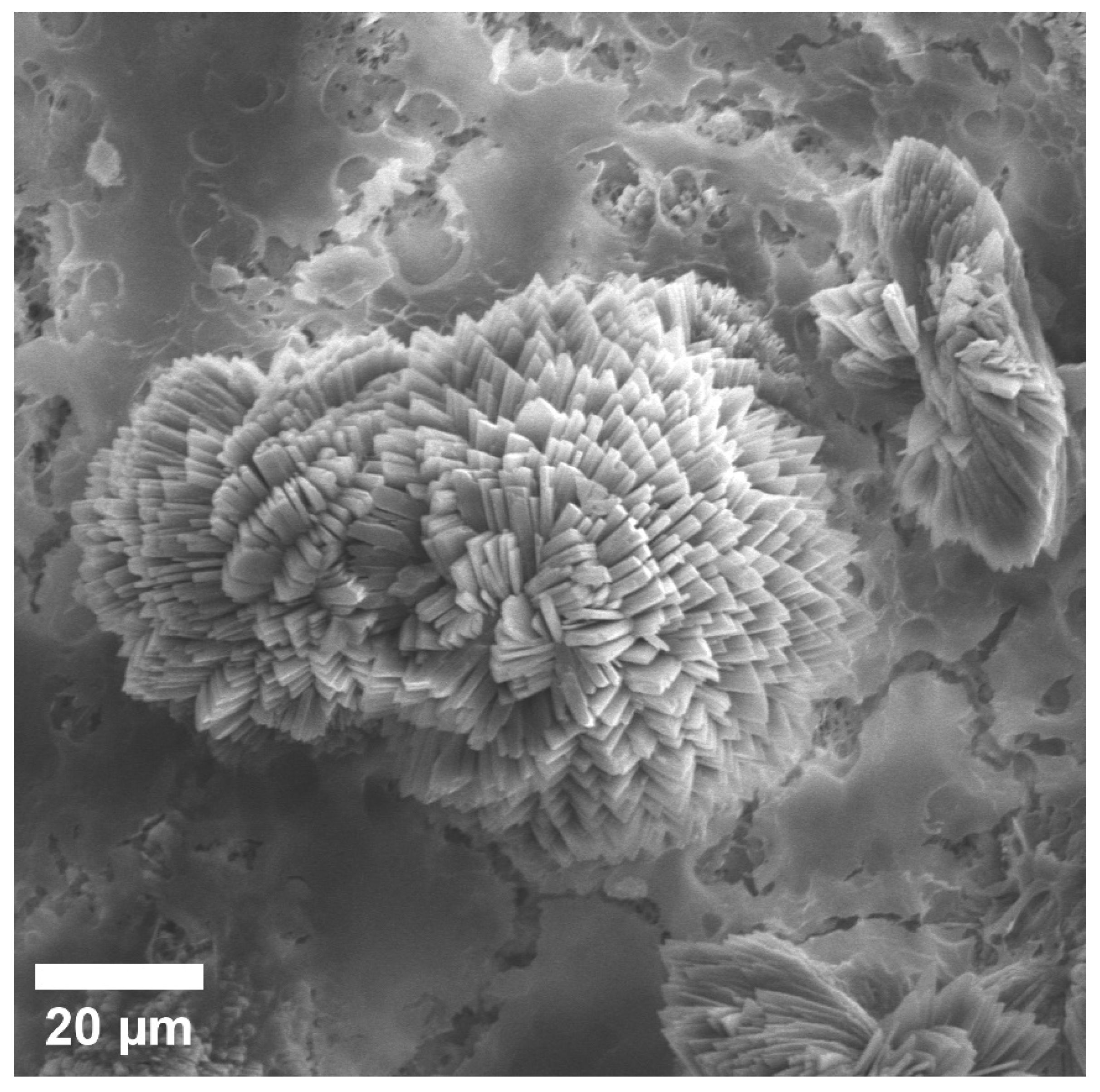
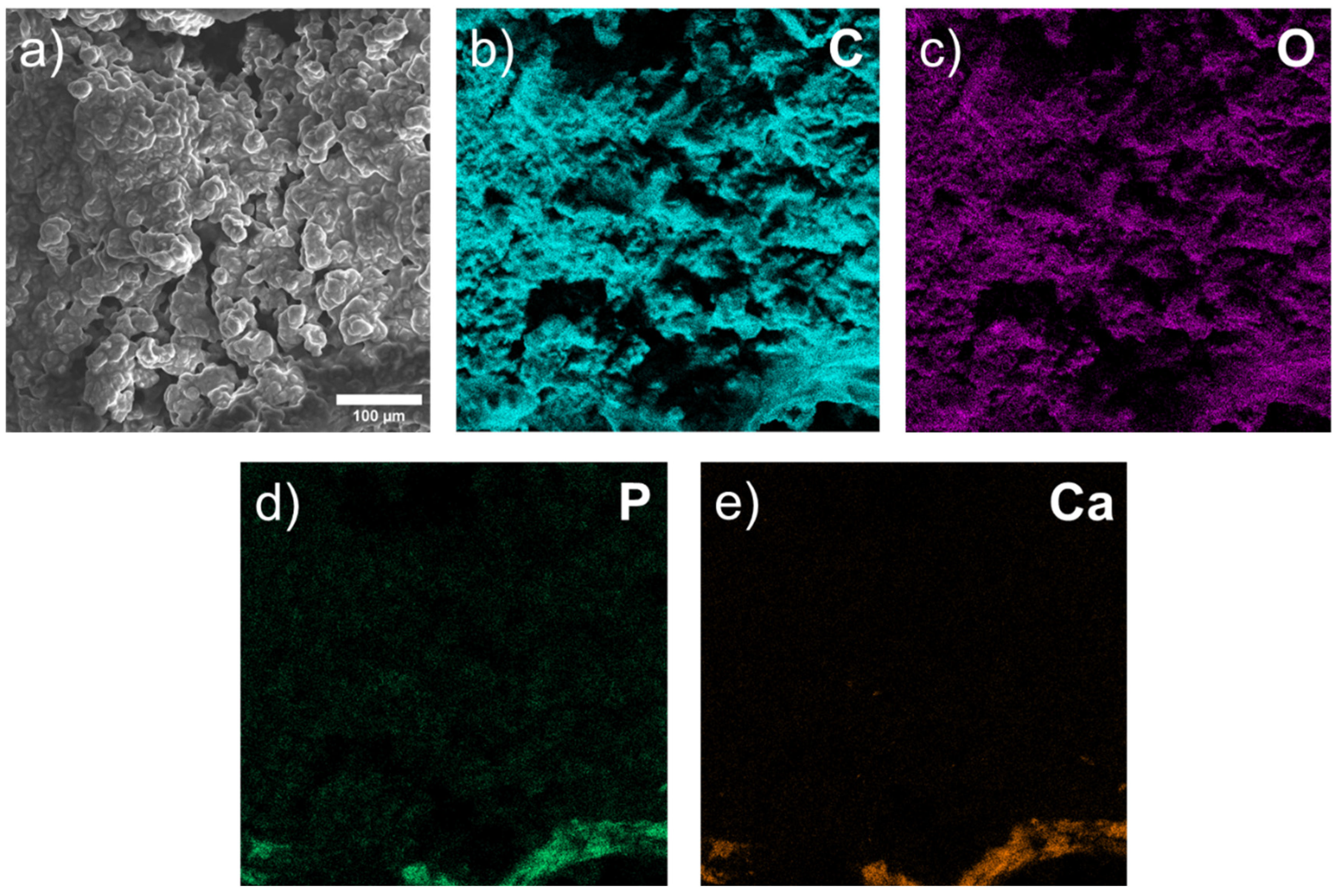
3.1. Scanning Electron Microscopy (SEM) of Biopsy Preparations




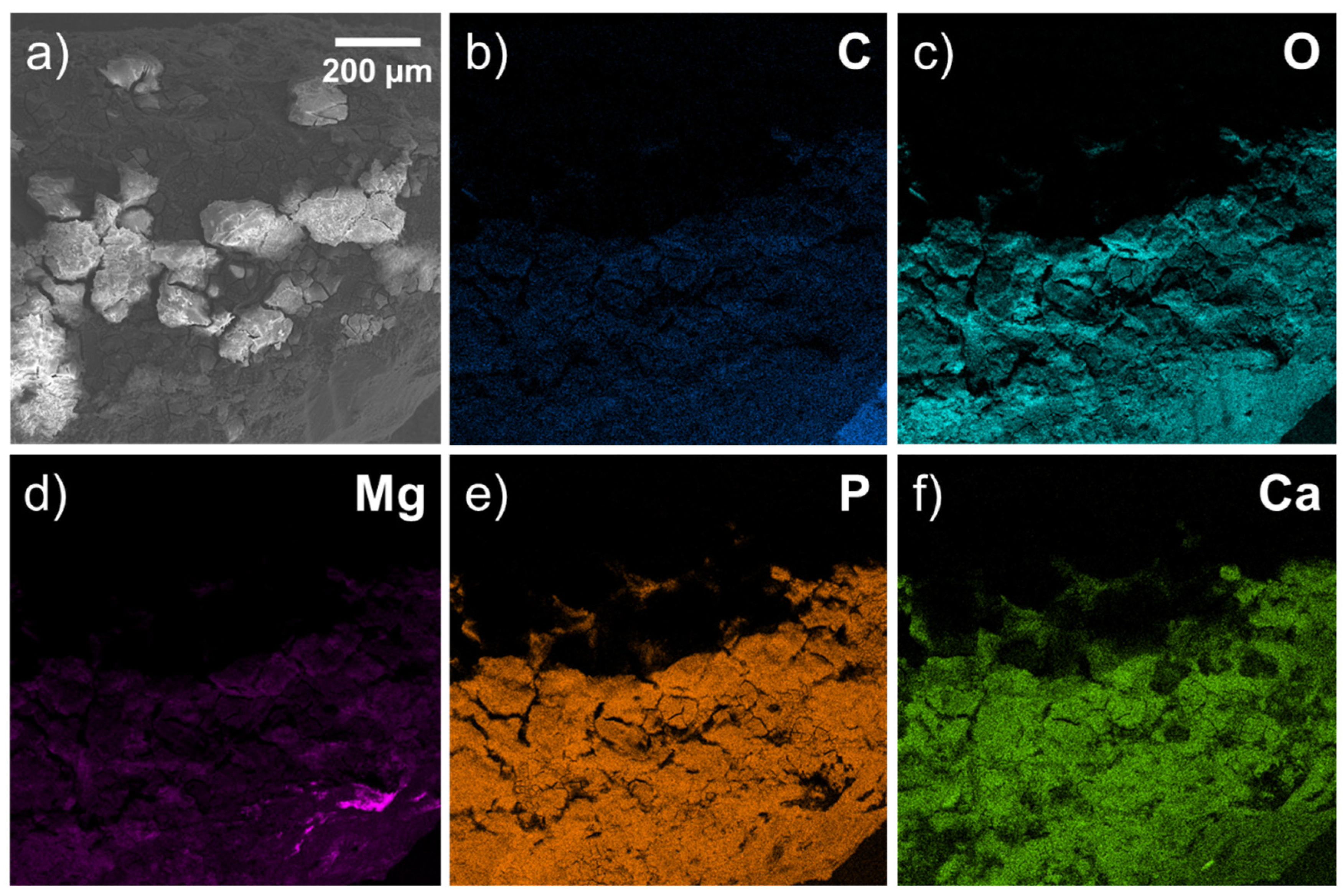
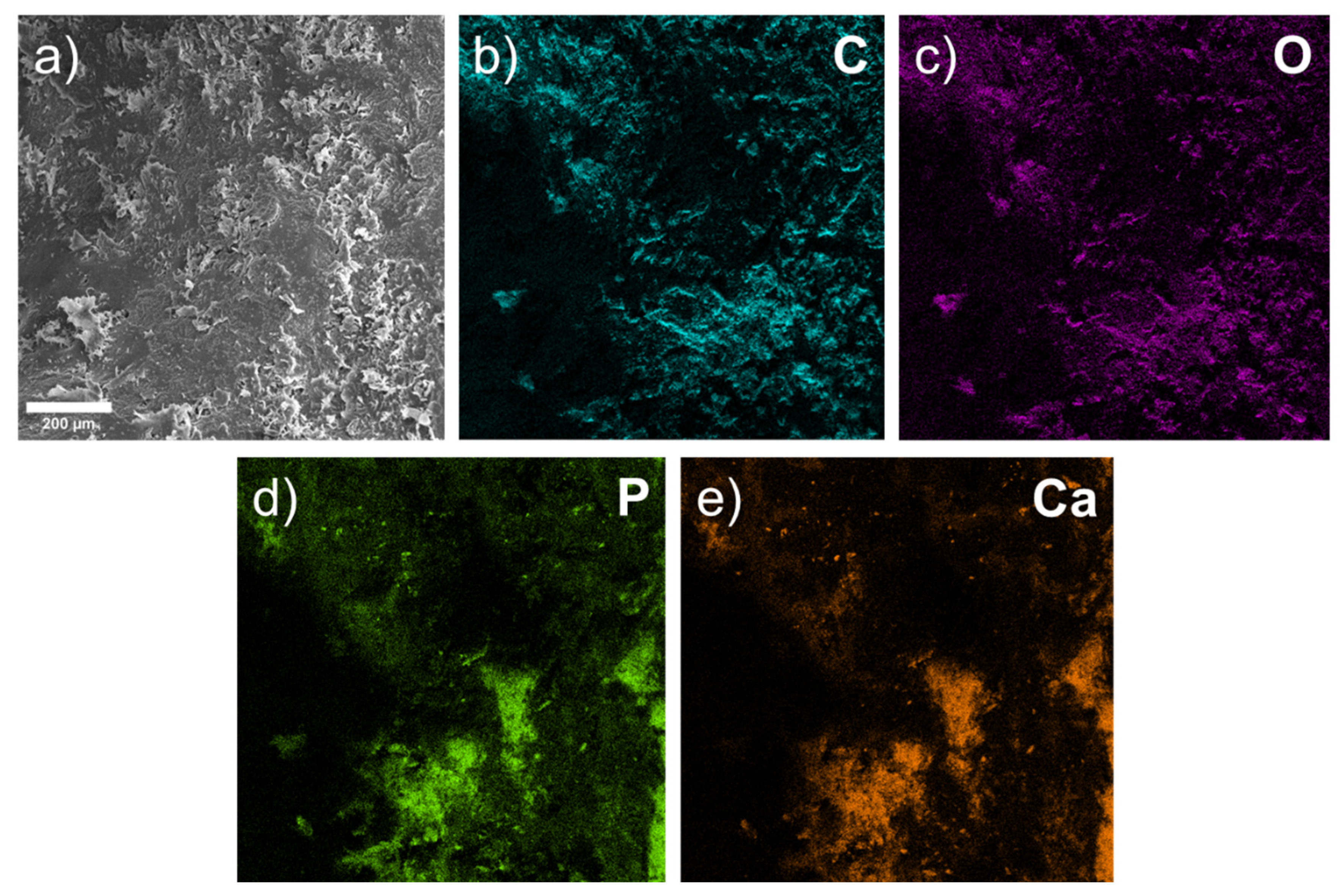
3.2. EDX Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ding, W. Opportunities and challenges for the biodegradable magnesium alloys as next-generation biomaterials. Regen. Biomater. 2016, 3, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Pogorielov, M.; Husak, Y.; Solodivnik, A.; Zhdanov, S. Magnesium-based biodegradable alloys: Degradation, application, and alloying elements. Interv. Med. Appl. Sci. 2017, 9, 27–38. [Google Scholar] [CrossRef]
- Witte, F. The history of biodegradable magnesium implants: A review. Acta Biomater. 2010, 6, 1680–1692. [Google Scholar]
- Bozo, I.Y.; Drobyshev, A.Y.; Redko, N.A.; Komlev, V.S.; Isaev, A.A.; Deev, R.V. Bringing a Gene-Activated Bone Substitute into Clinical Practice: From Bench to Bedside. Front. Bioeng. Biotechnol. 2021, 9, 599300. [Google Scholar] [CrossRef]
- Zhang, W.; Zhang, H.; Wang, L.; Fan, J.; Li, X.; Zhu, L.; Chen, S.; Roven, H.J.; Zhang, S. Microstructure Evolution and Mechanical Properties of AZ31 Magnesium Alloy Sheets Prepared by Low-Speed Extrusion with Different Temperature. Crystals 2020, 10, 644. [Google Scholar] [CrossRef]
- May, H.; Kati, Y.A.; Gumussuyu, G.; Emre, T.Y.; Unal, M.; Kose, O. Bioabsorbable magnesium screw versus conventional titanium screw fixation for medial malleolar fractures. J. Orthop. Traumatol. 2020, 21, 9. [Google Scholar] [CrossRef]
- Kamrani, S.; Fleck, C. Biodegradable magnesium alloys as temporary orthopaedic implants: A review. J. Biometals 2019, 23, 185–193. [Google Scholar]
- Sun, Y.; Helmholz, H.; Willumeit-Römer, R. Preclinical in vivo research of magnesium-based implants for fracture treatment: A systematic review of animal model selection and study design. J. Magnes. Alloy. 2021, 9, 351–361. [Google Scholar] [CrossRef]
- Gonzalez, J.; Hou, R.Q.; Nidadavolu, E.P.S.; Willumeit-Römer, R.; Feyerabend, F. Magnesium degradation under physiological conditions—Best practice. Bioact. Mater. 2018, 3, 174–185. [Google Scholar]
- Bazhenov, V.E.; Li, A.V.; Komissarov, A.A.; Koltygin, A.V.; Tavolzhanskii, S.A.; Bautin, V.A.; Voropaeva, O.O.; Mukhametshina, A.M.; Tokar, A.A. Microstructure and mechanical and corrosion properties of hot-extruded Mg–Zn–Ca–(Mn) biodegradable alloys. J. Magnes. Alloy. 2021, 9, 1428–1442. [Google Scholar]
- Amukarimi, S.; Mozafari, M. Biodegradable magnesium-based biomaterials: An overview of challenges and opportunities. MedComm 2021, 2, 123–144. [Google Scholar] [CrossRef]
- Jung, O.; Hesse, B.; Stojanovic, S.; Seim, C.; Weitkamp, T.; Batinic, M.; Goerke, O.; Kačarević, P.; Rider, P.; Najman, S.; et al. Biocompatibility Analyses of HF-Passivated Magnesium Screws for Guided Bone Regeneration (GBR). Int. J. Mol. Sci. 2021, 22, 12567. [Google Scholar] [CrossRef]
- Amukarimi, S.; Mozafari, M. Biodegradable Magnesium Biomaterials—Road to the Clinic. Bioengineering 2022, 9, 107. [Google Scholar] [CrossRef]
- Sharma, S.K.; Saxena, K.K.; Malik, V.; Mohammed, K.A.; Prakash, C.; Buddhi, D.; Dixit, S. Significance of Alloying Elements on the Mechanical Characteristics of Mg-Based Materials for Biomedical Applications. Crystals 2022, 12, 1138. [Google Scholar] [CrossRef]
- Chen, J.; Xu, Y.; Kolawole, S.K.; Wang, J.; Su, X.; Tan, L.; Yang, K. Systems, Properties, Surface Modification and Applications of Biodegradable Magnesium-Based Alloys: A Review. Materials 2022, 15, 5031. [Google Scholar] [CrossRef]
- Bazhenov, V.; Koltygin, A.; Komissarov, A.; Li, A.; Bautin, V.A.; Khasenova, R.; Anishchenko, A.; Seferyan, A.; Komissarova, J.; Estrin, Y. Gallium-containing magnesium alloy for potential use as temporary implants in osteosynthesis. J. Magnes. Alloy. 2020, 8, 352–363. [Google Scholar] [CrossRef]
- Shi, H.; Pan, K.; Dai, M.; Wei, W.; Liu, X.; Li, X. A Gallic Acid-Doped Polypyrrole Coating with Anticorrosion and Antibacterial Properties on Magnesium Alloy. ACS Appl. Bio. Mater. 2022, 5, 4244–4255. [Google Scholar] [CrossRef]
- Kubásek, J.; Vojtěch, D.; Dvorský, D. Structural and mechanical study on Mg–xLM (x = 0–5 wt.%, LM = Sn, Ga) alloys. Int. J. Mater. Res. 2016, 107, 459–471. [Google Scholar] [CrossRef]
- Xie, K.; Wang, L.; Guo, Y.; Zhao, S.; Yang, Y.; Dong, D.; Ding, W.; Dai, K.; Gong, W.; Yuan, G.; et al. Effectiveness and safety of biodegradable Mg-Nd-Zn-Zr alloy screws for the treatment of medial malleolar fractures. J. Orthop. Transl. 2021, 27, 96–100. [Google Scholar] [CrossRef]
- Hu, Y.; Guo, X.; Qiao, Y.; Wang, X.; Lin, Q. Preparation of medical Mg–Zn alloys and the effect of different zinc contents on the alloy. J. Mater. Sci. Mater. Med. 2022, 33, 1–13. [Google Scholar] [CrossRef]
- Bazhenov, V.; Lyskovich, A.; Li, A.; Bautin, V.; Komissarov, A.; Koltygin, A.; Bazlov, A.; Tokar, A.; Ten, D.; Mukhametshina, A. Effect of Heat Treatment on the Mechanical and Corrosion Properties of Mg–Zn–Ga Biodegradable Mg Alloys. Materials 2021, 14, 7847. [Google Scholar] [CrossRef]
- Hernández-Cortés, A.A.; Escobedo-Bocardo, J.C.; Cortés-Hernández, D.A.; Vazquez-Montiel, R.H.; Peralta-Montes, J.S.; Almanza-Robles, J.M. Microstructure, corrosion rate, and mechanical properties of unidirectionally and cross-rolled Mg-0. 375Ga and Mg-0. 750Ga alloys. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 646–659. [Google Scholar] [CrossRef]
- Bahmani, A.; Arthanari, S.; Shin, K.S. Corrosion behavior of Mg–Mn–Ca alloy: Influences of Al, Sn and Zn. J. Magnes. Alloy. 2019, 7, 38–46. [Google Scholar]
- Valappil, S.P.; Ready, D.; Abou Neel, E.A.; Pickup, D.M.; Chrzanowski, W.; O’Dell, L.A.; Newport, R.J.; Smith, M.E.; Wilson, M.; Knowles, J.C. Antimicrobial Gallium-Doped Phosphate-Based Glasses. Adv. Funct. Mater. 2008, 18, 732–741. [Google Scholar] [CrossRef]
- Miculescu, F.; Luță, C.; Constantinescu, A.; Maidaniuc, A.; Mocanu, A.-C.; Miculescu, M.; Voicu, Ș.I.; Ciocan, L. Considerations and Influencing Parameters in EDS Microanalysis of Biogenic Hydroxyapatite. J. Funct. Biomater. 2020, 11, 82. [Google Scholar] [CrossRef]
- Burge, R.; Dawson-Hughes, B.; Solomon, D.H.; Wong, J.B.; King, A.; Tosteson, A. Incidence and Economic Burden of Osteoporosis-Related Fractures in the United States, 2005–2025. J. Bone Miner. Res. 2006, 22, 465–475. [Google Scholar] [CrossRef]
- Li, J.; Qin, L.; Yang, K.; Ma, Z.; Wang, Y.; Cheng, L.; Zhao, D. Materials evolution of bone plates for internal fixation of bone fractures: A review. J. Mater. Sci. Technol. 2020, 36, 190–208. [Google Scholar] [CrossRef]
- Wu, A.-M.; Bisignano, C.; James, S.L.; Abady, G.G.; Abedi, A.; Abu-Gharbieh, E.; Alhassan, R.K.; Alipour, V.; Arabloo, J.; Asaad, M.; et al. Global, regional, and national burden of bone fractures in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet Healthy Longev. 2021, 2, e580–e592. [Google Scholar] [CrossRef]
- Ho-Shui-Ling, A.; Bolander, J.; Rustom, L.E.; Johnson, A.W.; Luyten, F.P.; Picart, C. Bone regeneration strategies: Engineered scaffolds, bioactive molecules and stem cells current stage and future perspectives. Biomaterials 2018, 180, 143–162. [Google Scholar] [CrossRef]
- Buijs, G.; Stegenga, B.; Bos, R. Efficacy and safety of biodegradable osteofixation devices in oral and maxillofacial surgery: A systematic review. J. Dent. Res. 2006, 85, 980–989. [Google Scholar] [CrossRef]
- Gareb, B.; van Bakelen, N.B.; Dijkstra, P.U.; Vissink, A.; Bos, R.R.M.; van Minnen, B. Efficacy and morbidity of biodegradable versus titanium osteosyntheses in orthognathic surgery: A systematic review with meta-analysis and trial sequential analysis. Eur. J. Oral Sci. 2021, 129, e12800. [Google Scholar] [CrossRef]
- Gareb, B.; Van Bakelen, N.B.; Buijs, G.J.; Jansma, J.; De Visscher, J.G.A.M.; Hoppenreijs, T.J.M.; Bergsma, J.E.; Van Minnen, B.; Stegenga, B.; Bos, R.R.M. Comparison of the long-term clinical performance of a biodegradable and a titanium fixation system in maxillofacial surgery: A multicenter randomized controlled trial. PLoS ONE 2017, 12, e0177152. [Google Scholar] [CrossRef]
- Yaremchuk, M.J.; Posnick, J.C. Resolving Controversies Related to Plate and Screw Fixation in the Growing Craniofacial Skeleton. J. Craniofacial Surg. 1995, 6, 525–538. [Google Scholar] [CrossRef]
- Viljanen, J.; Kinnunen, J.; Bondestam, S.; Majola, A.; Rokkanen, P.; Törmälä, P. Bone changes after experimental osteotomies fixed with absorbable self-reinforced poly-l-lactide screws or metallic screws studied by plain radiographs, quantitative computed tomography and magnetic resonance imaging. Biomaterials 1995, 16, 1353–1358. [Google Scholar] [CrossRef]
- Destatis. Vollstationär Behandelte Patientinnen Und Patienten in Krankenhäuser 2018; Destatis Statistisches Bundesamt: Wiesbaden, Germany, 2019; Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Krankenhaeuser/_inhalt.html (accessed on 9 October 2019).
- Prediger, B.; Mathes, T.; Probst, C.; Pieper, D. Elective Removal vs. Retaining of Hardware after Osteosynthesis in Asymptomatic Patients—A Scoping Review. Syst. Rev. 2020, 9, 225. [Google Scholar]
- Minkowitz, R.B.; Bhadsavle, S.; Walsh, M.; Egol, K.A. Removal of Painful Orthopaedic Implants After Fracture Union. J. Bone Jt. Surg. 2007, 89, 1906–1912. [Google Scholar]
- Müller, M.; Mückley, T.; Hofmann, G.O. Kosten und Komplikationen der Materialentfernung. Trauma Berufskrankh. 2007, 9, S297–S301. [Google Scholar] [CrossRef]
- Sanz-Herrera, J.; Reina-Romo, E.; Boccaccini, A. In silico design of magnesium implants: Macroscopic modeling. J. Mech. Behav. Biomed. Mater. 2018, 79, 181–188. [Google Scholar] [CrossRef]
- Nene, S.S.; Kashyap, B.P.; Prabhu, N.; Estrin, Y.; Al-Samman, T. Biocorrosion and biodegradation behavior of ultralight Mg–4Li–1Ca (LC41) alloy in simulated body fluid for degradable implant applications. J. Mater. Sci. 2015, 50, 3041–3050. [Google Scholar] [CrossRef]
- Peron, M.; Cogo, S.; Bjelland, M.; Bin Afif, A.; Dadlani, A.; Greggio, E.; Berto, F.; Torgersen, J. On the evaluation of ALD TiO2, ZrO2 and HfO2 coatings on corrosion and cytotoxicity performances. J. Magnes. Alloy. 2021, 9, 1806–1819. [Google Scholar] [CrossRef]
- Peron, M.; Skaret, P.C.; Fabrizi, A.; Varone, A.; Montanari, R.; Roven, H.J.; Ferro, P.; Berto, F.; Torgersen, J. The effect of Equal Channel Angular Pressing on the stress corrosion cracking susceptibility of AZ31 alloy in simulated body fluid. J. Mech. Behav. Biomed. Mater. 2020, 106, 103724. [Google Scholar] [CrossRef]
- Makkar, P.; Sarkar, S.K.; Padalhin, A.R.; Moon, B.-G.; Lee, Y.S.; Lee, B.T. In vitro and in vivo assessment of biomedical Mg–Ca alloys for bone implant applications. J. Appl. Biomater. Funct. Mater. 2018, 16, 126–136. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.; Cipriano, A.F.; Tian, Q.; Zhang, C.; Lopez, M.; Sallee, A.; Lin, A.; Alcaraz, M.C.C.; Wu, Y.; Zheng, Y.; et al. In vitro evaluation of MgSr and MgCaSr alloys via direct culture with bone marrow derived mesenchymal stem cells. Acta Biomater. 2018, 72, 407–423. [Google Scholar] [CrossRef]
- Kirkland, N.; Birbilis, N.; Staiger, M. Assessing the corrosion of biodegradable magnesium implants: A critical review of current methodologies and their limitations. Acta Biomater. 2012, 8, 925–936. [Google Scholar] [CrossRef]
- Klíma, K.; Ulmann, D.; Bartoš, M.; Španko, M.; Dušková, J.; Vrbová, R.; Pinc, J.; Kubásek, J.; Vlk, M.; Ulmannová, T.; et al. A Complex Evaluation of the In-Vivo Biocompatibility and Degradation of an Extruded ZnMgSr Absorbable Alloy Implanted into Rabbit Bones for 360 Days. Int. J. Mol. Sci. 2021, 22, 13444. [Google Scholar] [CrossRef]
- Harandi, S.E.; Mirshahi, M.; Koleini, S.; Idris, M.H.; Jafari, H.; Kadir, M.R.A. Effect of calcium content on the microstructure, hardness and in-vitro corrosion behavior of biodegradable Mg-Ca binary alloy. Mater. Res. 2012, 16, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Peron, M.; Bertolini, R.; Ghiotti, A.; Torgersen, J.; Bruschi, S.; Berto, F. Enhancement of stress corrosion cracking of AZ31 magnesium alloy in simulated body fluid thanks to cryogenic machining. J. Mech. Behav. Biomed. Mater. 2020, 101, 103429. [Google Scholar] [CrossRef]
- Peron, M.; Bin Afif, A.; Dadlani, A.; Berto, F.; Torgersen, J. Comparing physiologically relevant corrosion performances of Mg AZ31 alloy protected by ALD and sputter coated TiO2. Surf. Coat. Technol. 2020, 395, 125922. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, C.; Jing, Y.; Lv, S.; Liu, S.; Fang, D.; Zhuang, J.; Zhang, M.; Wu, R. New horizon for high performance Mg-based biomaterial with uniform degradation behavior: Formation of stacking faults. Sci. Rep. 2015, 5, srep13933. [Google Scholar] [CrossRef] [Green Version]
- Bian, D.; Zhou, W.; Liu, Y.; Li, N.; Zheng, Y.; Sun, Z. Fatigue behaviors of HP-Mg, Mg–Ca and Mg–Zn–Ca biodegradable metals in air and simulated body fluid. Acta Biomater. 2016, 41, 351–360. [Google Scholar] [CrossRef]
- Su, Z.; Liu, C.; Wan, Y. Microstructures and mechanical properties of high-performance Mg-4Y-2.4 Nd-0.2 Zn-0.4 Zr alloy. Mater. Des. 2013, 45, 466–472. [Google Scholar]
- Lesz, S.; Hrapkowicz, B.; Karolus, M.; Gołombek, K. Characteristics of the Mg-Zn-Ca-Gd Alloy after Mechanical Alloying. Materials 2021, 14, 226. [Google Scholar] [CrossRef]
- Chu, P.-W.; Le Mire, E.; Marquis, E. Microstructure of localized corrosion front on Mg alloys and the relationship with hydrogen evolution. Corros. Sci. 2017, 128, 253–264. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, X.; Zhao, C.; Li, J.; Song, Y.; Xie, C.; Tao, H.; Zhang, Y.; He, Y.; Jiang, Y.; et al. Research on an Mg–Zn alloy as a degradable biomaterial. Acta Biomater. 2010, 6, 626–640. [Google Scholar] [CrossRef]
- Su, Y.; Yang, H.; Gao, J.; Qin, Y.; Zheng, Y.; Zhu, D. Interfacial Zinc Phosphate is the Key to Controlling Biocompatibility of Metallic Zinc Implants. Adv. Sci. 2019, 6, 1900112. [Google Scholar] [CrossRef]
- Levy, G.K.; Goldman, J.; Aghion, E. The Prospects of Zinc as a Structural Material for Biodegradable Implants—A Review Paper. Metals 2017, 7, 402. [Google Scholar] [CrossRef] [Green Version]
- Pinc, J.; Španko, M.; Lacina, L.; Kubásek, J.; Ashcheulov, P.; Veřtát, P.; Školáková, A.; Kvítek, O.; Vojtěch, D.; Čapek, J. Influence of the pre-exposure of a Zn-0.8Mg-0.2Sr absorbable alloy in bovine serum albumin containing media on its surface changes and their impact on the cytocompatibility of the material. Mater. Today Commun. 2021, 28. [Google Scholar] [CrossRef]
- Sikora-Jasinska, M.; Mostaed, E.; Goldman, J.; Drelich, J.W. Albumins inhibit the corrosion of absorbable Zn alloys at initial stages of degradation. Surf. Innov. 2020, 8, 234–249. [Google Scholar] [CrossRef]
- Hybasek, V.; Kubasek, J.; Capek, J.; Alferi, D.; Pinc, J.; Jiru, J.; Fojt, J. Influence of model environment complexity on corrosion mechanism of biodegradable zinc alloys. Corros. Sci. 2021, 187, 109520. [Google Scholar] [CrossRef]
- Chou, A.H.K.; LeGeros, R.Z.; Chen, Z.; Li, Y. Antibacterial Effect of Zinc Phosphate Mineralized Guided Bone Regeneration Membranes. Implant Dent. 2007, 16, 89–100. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Element | Line Type | Weight % | Sigma Weight % | Atom % |
|---|---|---|---|---|
| C | K-series | 15.58 | 0.09 | 25.60 |
| O | K-series | 41.46 | 0.06 | 51.14 |
| Mg | K-series | 11.80 | 0.02 | 9.58 |
| P | K-series | 13.46 | 0.02 | 8.58 |
| Ca | K-series | 5.32 | 0.01 | 2.62 |
| Element | Line Type | Weight % | Sigma Weight % | Atom % |
|---|---|---|---|---|
| C | K-series | 60.09 | 0.07 | 82.36 |
| O | K-series | 12.35 | 0.05 | 12.71 |
| P | K-series | 1.95 | 0.01 | 1.04 |
| Ca | K-series | 3.93 | 0.01 | 1.62 |
| Element | Line Type | Weight % | Sigma Weight % | Atom % |
|---|---|---|---|---|
| C | K-series | 78.78 | 0.05 | 86.39 |
| O | K-series | 15.83 | 0.05 | 13.03 |
| P | K-series | 0.23 | 0.01 | 0.10 |
| Ca | K-series | 0.35 | 0.00 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drobyshev, A.; Komissarov, A.; Redko, N.; Gurganchova, Z.; Statnik, E.S.; Bazhenov, V.; Sadykova, I.; Miterev, A.; Romanenko, I.; Yanushevich, O. Bone Remodeling Interaction with Magnesium Alloy Implants Studied by SEM and EDX. Materials 2022, 15, 7529. https://doi.org/10.3390/ma15217529
Drobyshev A, Komissarov A, Redko N, Gurganchova Z, Statnik ES, Bazhenov V, Sadykova I, Miterev A, Romanenko I, Yanushevich O. Bone Remodeling Interaction with Magnesium Alloy Implants Studied by SEM and EDX. Materials. 2022; 15(21):7529. https://doi.org/10.3390/ma15217529
Chicago/Turabian StyleDrobyshev, Alexey, Alexander Komissarov, Nikolay Redko, Zaira Gurganchova, Eugene S. Statnik, Viacheslav Bazhenov, Iuliia Sadykova, Andrey Miterev, Igor Romanenko, and Oleg Yanushevich. 2022. "Bone Remodeling Interaction with Magnesium Alloy Implants Studied by SEM and EDX" Materials 15, no. 21: 7529. https://doi.org/10.3390/ma15217529