
Does Root Development Status Affect the Outcome of Tooth Autotransplantation? A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient, Intervention, Comparison, Outcome (PICO) Question
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
2.4. Selection of Studies
2.5. Data Extraction
2.6. Quality Assessment
2.7. Statistical Analysis
3. Results
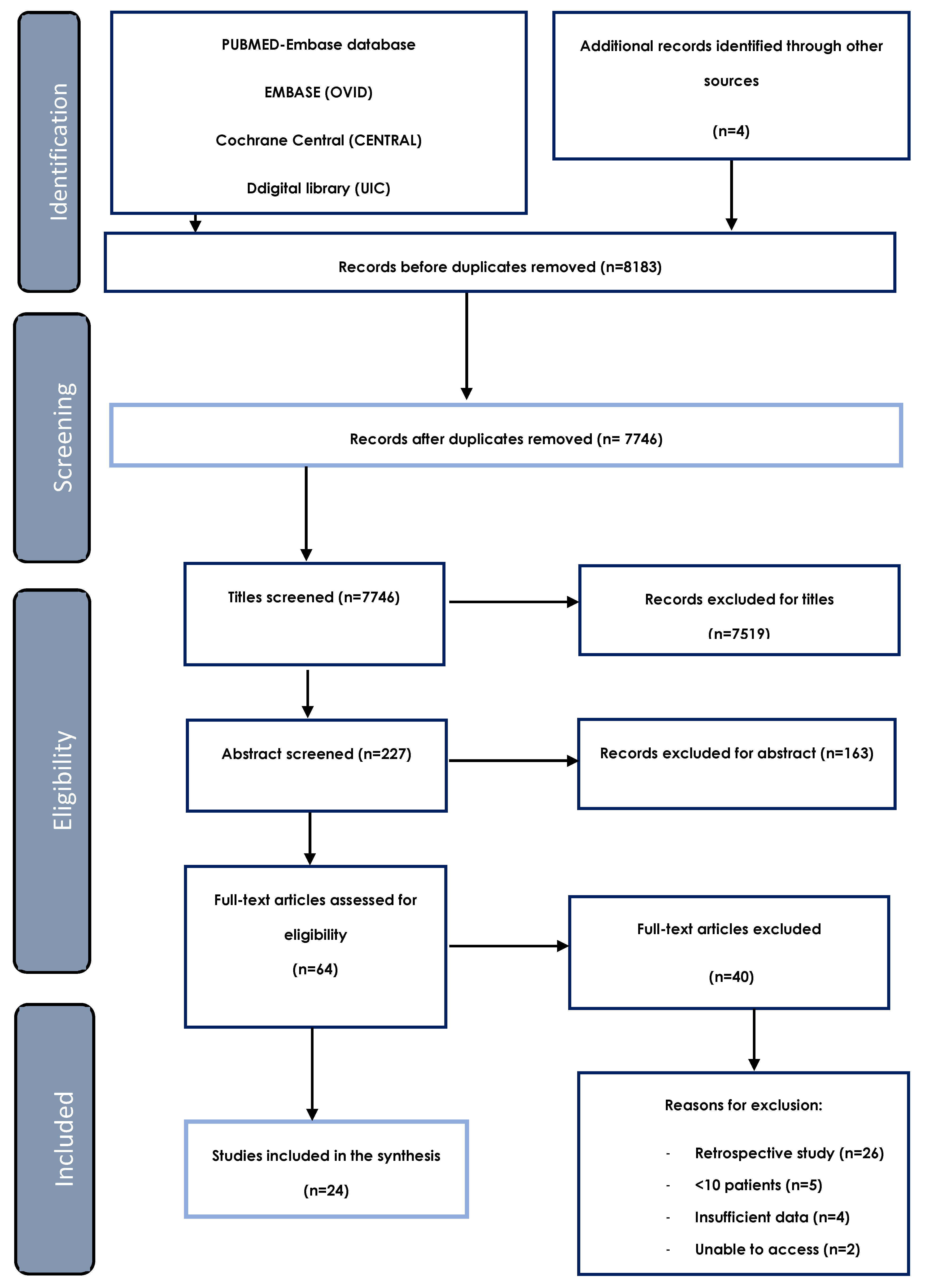
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
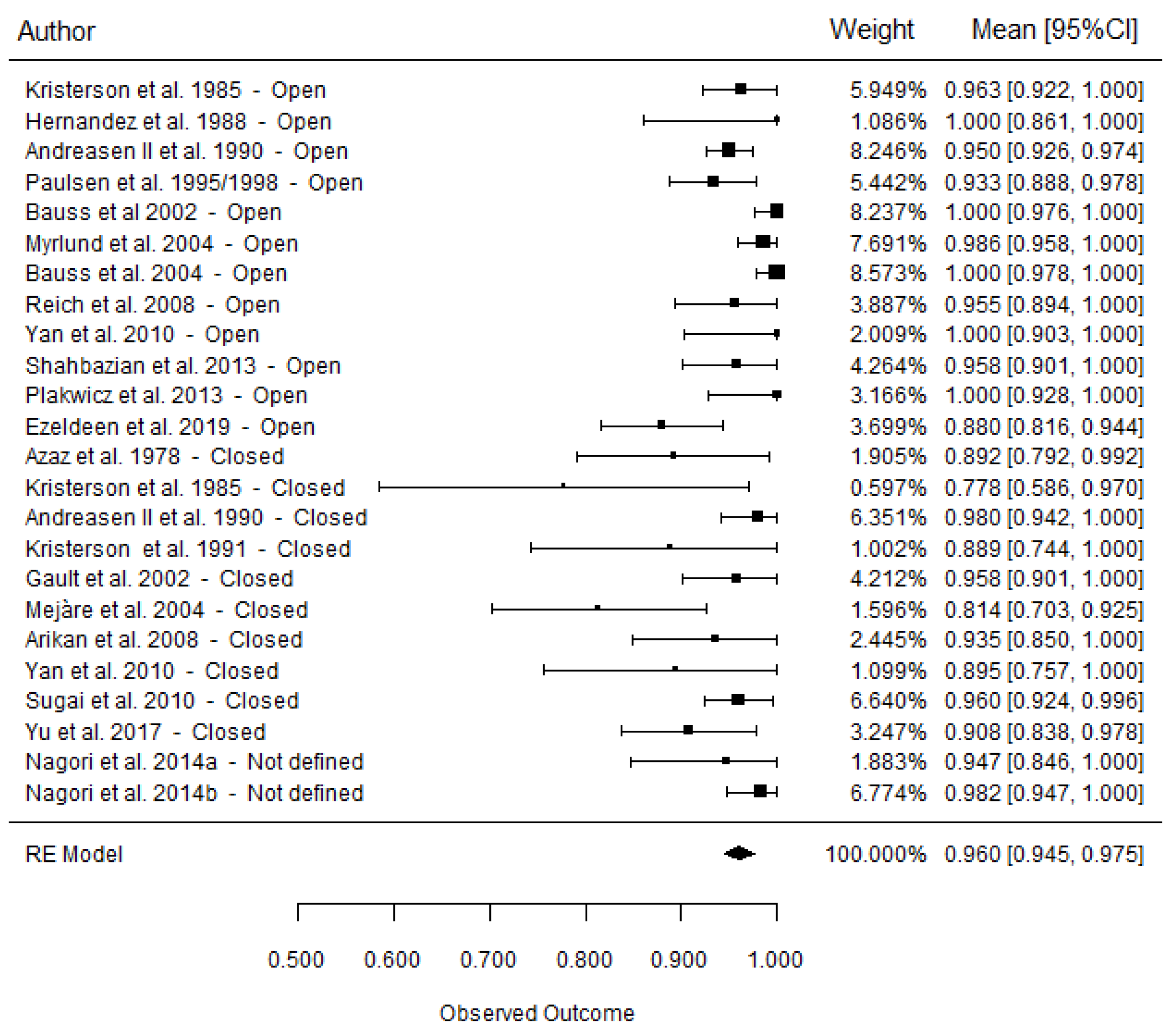
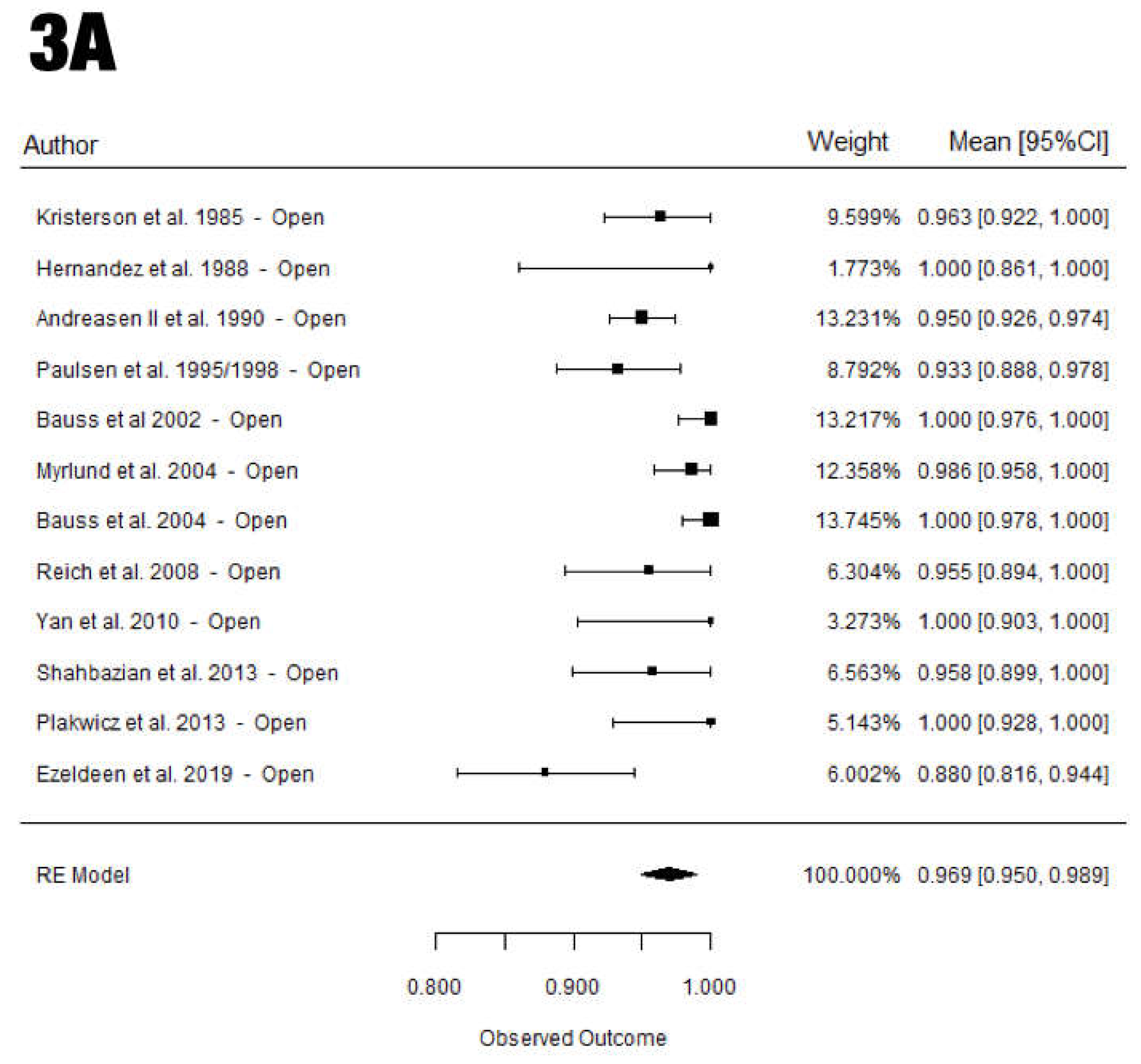
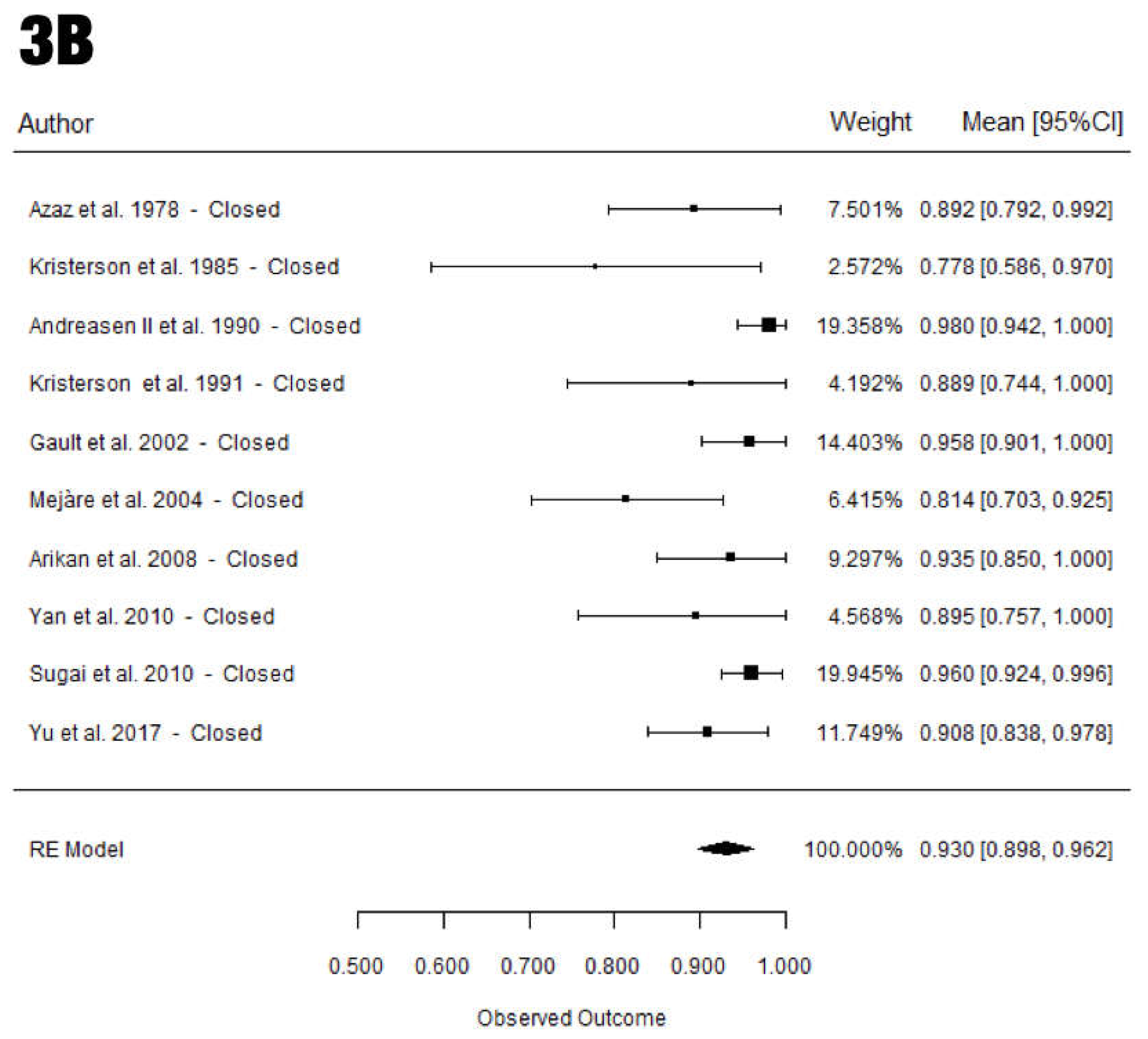
3.4. Survival Rate
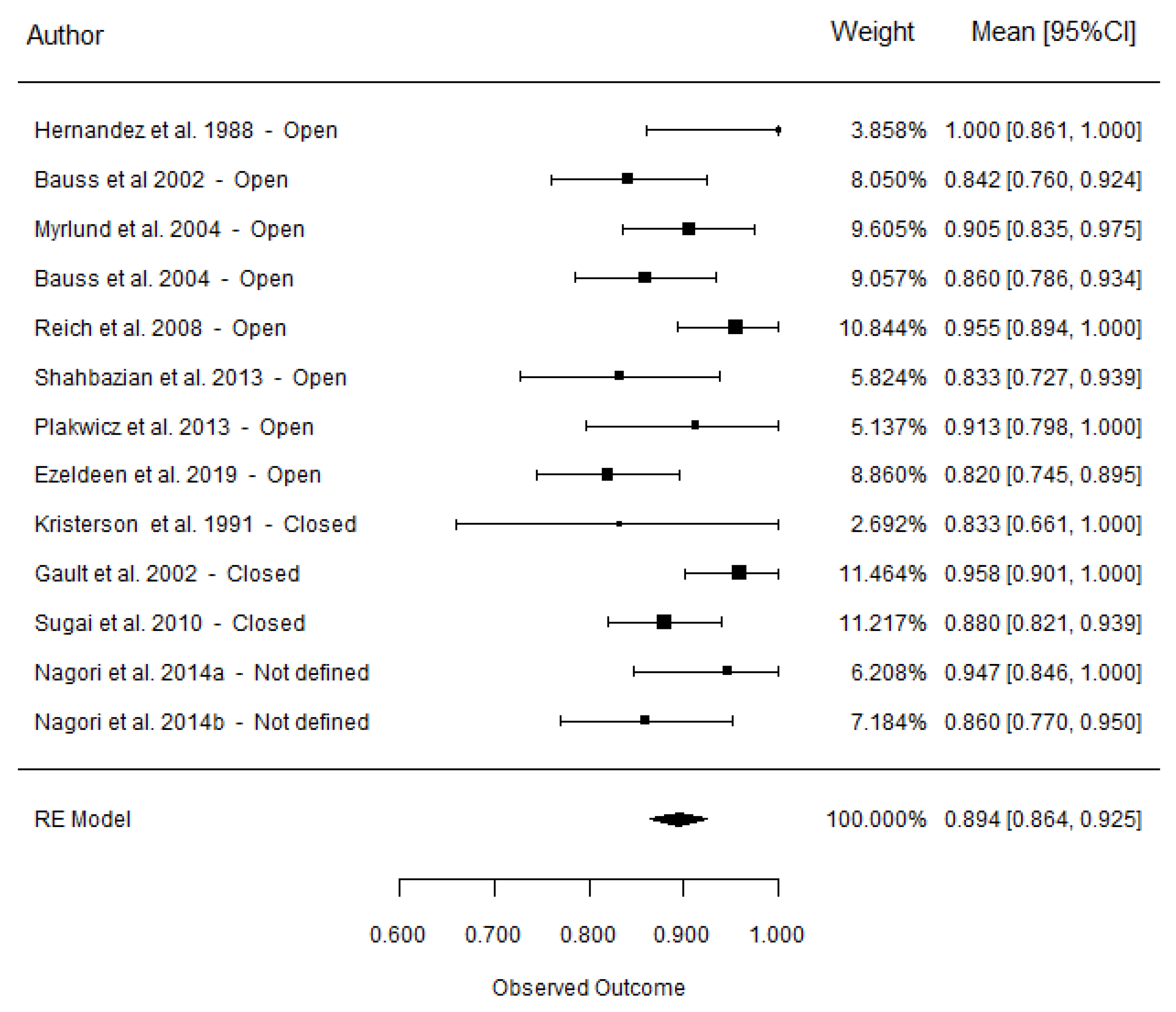
3.5. Success Rate
3.6. Inflammatory Root Resorption
3.7. Replacement Root Resorption
3.8. Root Formation
3.9. Pulp Healing
3.10. Pulp Obliteration
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tsukiboshi, M. Autotransplantation of teeth: Requirements for predictable success. Dent. Traumatol. 2002, 18, 157–180. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.; Pirih, F.; Camargo, P. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Periodontol. 2018, 89, S304–S312. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef]
- Schwarz, F.; Sahm, N.; Schwarz, K.; Becker, J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J. Clin. Periodontol. 2010, 37, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L. Peri-implant diseases: Diagnosis and risk indicators. J. Clin. Periodontol. 2008, 35, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; White, S. Endodontic treatment options after unsuccessful initial root canal treatment: Alternatives to single-tooth implants. J. Am. Dent. Assoc. 2016, 147, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Zachrisson, B.; Stenvik, A.; Haanaes, H. Management of missing maxillary anterior teeth with emphasis on autotransplantation. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 284–288. [Google Scholar] [CrossRef]
- Czochrowska, E.; Stenvik, A.; Bjercke, B.; Zachrisson, B. Outcome of tooth transplantation: Survival and success rates 17–41 years posttreatment. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 110–119. [Google Scholar] [CrossRef]
- Andreasen, J.; Paulsen, H.; Yu, Z. A long-term study of 370 autotransplanted premolars. Part III. Periodontal healing subsequent to transplantation. Eur. J. Orthod. 1990, 12, 25–37. [Google Scholar] [CrossRef]
- Plakwicz, P.; Wojtowicz, A.; Czochrowska, E. Survival and success rates of autotransplanted premolars: A prospective study of the protocol for developing teeth. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.; Paulsen, H.; Yu, Z. A long-term study of 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur. J. Orthod. 1990, 12, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Slagsvold, O.; Bjercke, B. Autotransplantation of premolars with partly formed roots: A radiographic study of root growth. Am. J. Orthod. 1974, 66, 355–366. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Paulsen, H.U.; Yu, Z.; Ahlquist, R.; Bayer, T.; Schwartz, O. A long-term study of 370 autotransplanted premolars. Part, I. Surgical procedures and standardized techniques for monitoring healing. Eur. J. Orthod. 1990, 12, 3–13. [Google Scholar] [CrossRef]
- Jonsson, T.; Sigurdsson, T. Autotransplantation of premolars to premolar sites. A long-term follow-up study of 40 consecutive patients. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Ahlberg, A.; Bystedt, H.; Eliasson, S.; Odenrick, L. Long-term evaluation of autotransplanted maxillary canines with completed root formation. Acta Odontol. Scand. 1983, 41, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, O.; Bergmann, P.; Klausen, B. Autotransplantation of human teeth. A life-table analysis of prognostic factors. Int. J. Oral Surg. 1985, 14, 245–258. [Google Scholar] [CrossRef]
- Sugai, T.; Yoshizawa, M.; Kobayashi, T. Clinical study on prognostic factors for autotransplantation of teeth with complete root formation. Int. J. Oral Maxillofac. Surg. 2010, 39, 1193–1203. [Google Scholar] [CrossRef]
- Lucas-Taulé, E.; Llaquet, M.; Muñoz-Peñalver, J.; Nart, J.; Hernández-Alfaro, F.; Gargallo-Albiol, J. Mid-Term outcomes and periodontal prognostic factors of autotransplanted third molars: A Retrospective Cohort Study. J. Periodontol. 2021, 92, 1776–1787. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Li, B.; Long, X. Immediate autotransplantation of mandibular third molar in China. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 110, 436–440. [Google Scholar] [CrossRef]
- Shahbazian, M.; Jacobs, R.; Wyatt, J.; Denys, D.; Lambrichts, I.; Vinckier, F. Validation of the cone beam computed tomography-based stereolithographic surgical guide aiding autotransplantation of teeth: Clinical case-control study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2013, 115, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Myrlund, S.; Stermer, E.M.; Album, B.; Stenvik, A. Root length in transplanted premolars. Acta Odontol. Scand. 2004, 62, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Bauss, O.; Engelke, W.; Fenske, C.; Schilke, R.; Schwestka-Polly, R. Autotransplantation of immature third molars into edentulous and atrophied jaw sections. Int. J. Oral Maxillofac. Surg. 2004, 33, 558–563. [Google Scholar] [CrossRef] [PubMed]
- EzEldeen, M.; Wyatt, J.; Al-Rimawi, A.; Coucke, W.; Shaheen, E.; Lambrichts, I. Use of CBCT Guidance for Tooth Autotransplantation in Children. J. Dent. Res. 2019, 98, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Kristerson, L. Autotransplantation of human premolars. A clinical and radiographic study of 100 teeth. Int. J. Oral Surg. 1985, 14, 200–213. [Google Scholar] [CrossRef]
- Hernandez, S.L.; Cuestas-Carnero, R. Autogenic Tooth Transplantation: A Report of Ten Cases. J. Oral Maxillofac. Surg. 1988, 46, 1051–1055. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Paulsen, H.U.; Yu, Z.; Bayer, T. A long-term study of 370 autotransplanted premolars. Part IV. Root development subsequent to transplantation. Eur. J. Orthod. 1990, 12, 38–50. [Google Scholar] [CrossRef]
- Paulsen, H.; Andreasen, J.; Schwartz, O. Pulp and periodontal healing, root development and root resorption subsequent to transplantation and orthodontic rotation: A long-term study of autotransplanted premolars. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 630–640. [Google Scholar] [CrossRef]
- Paulsen, H.; Andreasen, J. Eruption of premolars subsequent to autotransplantation. A longitudinal radiographic study. Eur. J. Orthod. 1998, 20, 45–55. [Google Scholar] [CrossRef]
- Bauss, O.; Schilke, R.; Fenske, C.; Engelke, W.; Kiliaridis, S. Autotransplantation of immature third molars: Influence of different splinting methods and fixation periods. Dent. Traumatol. 2002, 18, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Reich, P. Autogenous transplantation of maxillary and mandibular molars. J. Oral Maxillofac. Surg. 2008, 66, 2314–2317. [Google Scholar] [CrossRef]
- Yu, H.J.; Jia, P.; Lv, Z.; Qiu, L.X. Autotransplantation of third molars with completely formed roots into surgically created sockets and fresh extraction sockets: A 10-year comparative study. Int. J. Oral Maxillofac. Surg. 2017, 46, 531–538. [Google Scholar] [CrossRef]
- Arikan, F.; Nizam, N.; Sonmez, S. 5-Year Longitudinal Study of Survival Rate and Periodontal Parameter Changes at Sites of Maxillary Canine Autotransplantation. J. Periodontol. 2008, 79, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Azaz, B.; Zilberman, Y.; Hackak, T. Clinical and roentgenographic evaluation of thirty-seven autotransplanted impacted maxillary canines. Oral Surg. Oral Med. Oral Pathol. 1978, 45, 8–16. [Google Scholar] [CrossRef]
- Kristerson, L.; Johansson, L.; Kisch, J.; Stadler, L. Autotransplantation of third molars as treatment in advanced periodontal disease. J. Clin. Periodontol. 1991, 18, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Gault, P.C.; Warocquier-Clerout, R. Tooth Auto-Transplantation with Double Periodontal Ligament Stimulation to Replace Periodontally Compromised Teeth. J. Periodontol. 2002, 73, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Mejàre, B.; Wannfors, K.; Jansson, L. A prospective study on transplantation of third molars with complete root formation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 97, 231–238. [Google Scholar] [CrossRef]
- Nagori, S.A.; Anson, J.; Bhutia, O.; Roychoudhury, A. Evaluating success of autotransplantation of embedded/impacted third molars harvested using piezosurgery: A pilot study. Acta Odontol. Scand. 2014, 72, 846–885. [Google Scholar] [CrossRef]
- Nagori, S.A.; Bhutia, O.; Roychoudhury, A.; Pandey, R.M. Immediate autotransplantation of third molars: An experience of 57 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2014, 118, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.; Tu, Y.; Lin, Y.; Lu, H. Outcomes of autotransplanted teeth with complete root formation: A systematic review and meta-analysis. J. Clin. Periodontol. 2014, 41, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Almpani, K.; Papageorgiou, S.; Papadopoulos, M. Autotransplantation of teeth in humans: A systematic review and meta-analysis. Clin. Oral Investig. 2015, 19, 1157–1179. [Google Scholar] [CrossRef] [PubMed]
- Machado, L.A.; do Nascimento, R.R.; Ferreira, D.M.T.P.; Mattos, C.T.; Vilella, O.V. Long-term prognosis of tooth autotransplantation: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 610–617. [Google Scholar] [CrossRef]
- Zhang, J.; An, Y.; Gao, L.N.; Zhang, Y.; Jin, Y.; Chen, F.M. The effect of aging on the pluripotential capacity and regenerative potential of human periodontal ligament stem cells. Biomaterials 2012, 33, 6974–6986. [Google Scholar] [CrossRef]
- Bauss, O.; Zonios, I.; Rahman, A. Root development of immature third molars transplanted to surgically created sockets. J. Oral Maxillofac. Surg. 2008, 66, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Verweij, J.; Moin, D.A.; Mensink, G.; Nijkamp, P.; Wismeijer, D.; van Merkesteyn, J.P.R. Autotransplantation of premolars with a 3D printed titanium replica of the donor tooth functioning as a surgical guide: Proof of concept in five transplants. J. Oral Maxillofac. Surg. 2016, 74, 1114–1119. [Google Scholar] [CrossRef]
- Dioguardi, M.; Quarta, C.; Sovereto, D.; Troiano, G.; Melillo, M.; Di Cosola, M. Autotransplantation of the Third Molar: A Therapeutic Alternative to the Rehabilitation of a Missing Tooth: A Scoping Review. Bioengoneering 2021, 2, 120. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, K.; Kariya, N.; Namura, D. Influence of age on tooth autotransplantation with complete root formation. J. Oral Rehabil. 2013, 40, 112–118. [Google Scholar] [CrossRef]
- Huth, K.; Nazet, M.; Paschos, E.; Linsenmann, R.; Hickel, R.; Nolte, D. Autotransplantation and surgical uprighting of impacted or retained teeth: A retrospective clinical study and evaluation of patient satisfaction. Acta Odontol. Scand. 2013, 71, 1538–1546. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J. Periodontal healing after replantation and autotransplantation of incisors in monkeys. Int. J. Oral Surg. 1981, 10, 54–61. [Google Scholar] [CrossRef]
- Kafourou, V.; Tong, H.; Day, P.; Houghton, N.; Spencer, R.; Duggal, M. Outcomes and prognostic factors that influence the success of tooth autotransplantation in children and adolescents. Dent. Traumatol. 2017, 33, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Jung, B.; Pang, N. Outcomes of autotransplanted teeth and prognostic factors: A 10-year retrospective study. Clin. Oral Investig. 2019, 23, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Verweij, J.; Jongkees, F.; Anssari Moin, D.; Wismeijer, D.; van Merkesteyn, J. Autotransplantation of teeth using computer-aided rapid prototyping of a three-dimensional replica of the donor tooth: A systematic literature review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1466–1474. [Google Scholar] [CrossRef]
- Lucas-Taulé, E.; Llaquet, M.; Múñoz-Peñalver, J.; Somoza, J.; Satorres-Nieto, M.; Hernández-Alfaro, F. Fully Guided Tooth Autotransplantation Using a Multidrilling Axis Surgical Stent: Proof of Concept. J. Endod. 2020, 46, 1515–1521. [Google Scholar] [CrossRef]
- Polizzi, E.; Tetè, G.; Bova, F.; Pantaleo, G.; Gastaldi, G.; Capparè, P. Antibacterial properties and side effects of chlorhexidine-based mouthwashes. A prospective, randomized clinical study. J. Osseointegr. 2020, 12, 2–7. [Google Scholar] [CrossRef]
- Lee, S.; Jung, I.; Lee, C.; Choi, S.; Kum, K. Clinical application of computer-aided rapid prototyping for tooth transplantation. Dent. Traumatol. 2001, 17, 114–119. [Google Scholar] [CrossRef]
- Huang, G.; Sonoyama, W.; Liu, Y.; Liu, H.; Wang, S.; Shi, S. The hidden treasure in apical papilla: The potential role in pulp/dentin regeneration and bioroot engineering. J. Endod. 2008, 34, 645–651. [Google Scholar] [CrossRef]
- Andreasen, J.; Borum, M.; Jacobsen, H.; Andreasen, F. Replantation of 400 avulsed permanent incisors. II. Factors related to pulp healing. Endod. Dent. Traumatol. 1994, 11, 59–68. [Google Scholar] [CrossRef]
- Day, P.; Lewis, B.; Spencer, R. The design and development of surgical templates for premolar transplants in adolescents. Int. Endod. J. 2012, 45, 1042–1052. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Design | Follow-Up (Years) | Nº Patients | Nº Teeth | Age Range | Donor Tooth Type | Splinting Procedure | Splinting Duration | Occlusion/Infraocclusion | 3D Replica | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Maxilla | Mandible | Suture | Wire | Suture | Wire | ||||||||
| OPEN APEX | |||||||||||||
| Kristerson et al. 1985 [27]. | PCS | 3–18Y (6.3Y) | NR | 82 | 10.0–19 | PM (84) | Yes (19) | Yes (63) | 1 W | 0 | I/O | NR | |
| Hernandez et al. 1988 [28]. | PCS | 3Y | 10 | 10 | 13–19 | TM (10) | Yes (10) | 0 | 2 W | 0 | I | Yes | |
| Andreasen II et al. 1990 [12]. | PCS | 1–13Y | NR | 317 | 7–35.0 | PM (317) | Yes | Yes | 1 W | 0 | NR | NR | |
| Andreasen III et al. 1990 [10]. | PCS | 1–13Y | NR | 317 | 7–35.0 | PM (317) | Yes | Yes | 1 W | 0 | NR | NR | |
| Andreasen IV et al. 1990 [29]. | PCS | 1–13Y | NR | 317 | 7–35.0 | PM (317) | Yes | Yes | 1 W | 0 | NR | NR | |
| Paulsen et al. 1995 [30] /1998 [31]. | PCS | 6–18Y | NR | 118 | NR | PM (104) | PM (14) | 0 | 0 | 0 | 0 | NR | NR |
| Bauss et al. 2002 [32]. | PCS | 1.0–6.1Y (3.4Y) | 72 | 76 | 16.3–20.3 | TM (40) | TM (36) | Yes (42) | Yes (34) | 1 W | 4 W | I | NR |
| Myrlund et al. 2004 [24]. | PCS | 4 Y | 54 | 68 | 6.5–20 | PM (68) | 0 | 0 | 0 | 0 | I | NR | |
| Bauss et al. 2004 [25]. | PCS | 1–6.3Y (3.4Y) | 79 | 85 | 16.1–20.3 | TM (85) | Yes | Yes | 1 W | 4 W | I | NR | |
| Reich et al. 2008 [33]. | PCS | 6 m–4Y (1.7Y) | 32 | 44 | 11.0–25 | TM (44) | Yes (44) | 0 | 2 W | 0 | I | NR | |
| Yan et al. 2010 [22]. | PCS | 1–11Y (5.2Y) | NR | 16 | 16–39 | TM (16) | Yes (16) | Yes (11) | 1 W | 1 W | NR | NR | |
| Shahbazian et al. 2013 [23]. | PCS | 1Y | 40 | 48 | 9.0–18 | M (4) PM (44) | 0 | Yes (48) | 0 | Few W | I | Yes | |
| Plakwicz et al. 2013 [11]. | PCS | 6–78m (2.11Y) | 19 | 23 | 9.1–17 | 2PM (17) | 2PM (6) | Yes (23) | 0 | 2 W | 0 | I | NR |
| Ezeldeen et al. 2019 [26]. | PCS | 1.1–10.4Y (4.5Y) | 88 | 100 | 8.0–13 | PM (100) | Yes | Yes | 0 | 0 | I | Yes | |
| CLOSED APEX | |||||||||||||
| Azaz et al. 1978 [36]. | PCS | 2–7Y | 31 | 37 | 13–36.0 | Cs (37) | 0 | 0 | Yes (37) | 0 | 10 weeks | NR | NR |
| Kristerson et al. 1985 [27]. | PCS | 3–18Y (6.3Y) | NR | 18 | 15–58.0 | PM (18) | 0 | Yes (18) | 0 | 0 | O | NR | |
| Andreasen II et al. 1990 [12]. | PCS | 1–13Y | NR | 53 | 7–35.0 | PM (53) | Yes | Yes | 1 W | 0 | NR | NR | |
| Andreasen III et al. 1990 [10]. | PCS | 1–13Y | NR | 53 | 7–35.0 | PM (53) | Yes | Yes | 1 W | 0 | NR | NR | |
| Andreasen IV et al. 1990 [29]. | PCS | 1-13Y | NR | 53 | 7–35.0 | PM (53) | Yes | Yes | 1 W | 0 | NR | NR | |
| Kristerson et al.1991 [37]. | PCS | 1.5–6Y | 18 | 18 | 24–58 | TM (18) | Yes (18) | Yes (18) | 1 W | 2-3 W | NR | NR | |
| Gault et al. 2002 [38]. | PCS | 2–7Y (5Y) | 43 | 47 | 33–73 | M (43), PM (2) and C (2) | Yes (47) | 0 | 2 W | 0 | I | NR | |
| Mejàre et al. 2004 [39]. | PCS | 1–10Y(4Y) | 47 | 47 | 21–66 | TM (47) | Yes (47) | Yes (10) | 10 days | 10 days | I | NR | |
| Arikan et al. 2008 [35]. | PCS | 2–8Y(5.87Y) | 30 | 32 | 25–55 | C (31) | 0 | 0 | Yes (32) | 0 | 4 W | NR | NR |
| Yan et al. 2010 [22]. | PCS | 1–11Y (5.2Y) | NR | 19 | 16–39 | TM (19) | Yes (19) | Yes (13) | 1 W | 1 W | NR | NR | |
| Sugai et al. 2010 [18]. | PCS | 1–5.9Y (3.40Y) | 109 | 117 | 11–75.0 | M (40) PM (10) I (1) | M (10) PM (16) | Yes (117) | Yes (117) | 1 W | 3 W | I | NR |
| Yu et al. 2017 [34]. | PCS | 7–13Y (9.9Y) | 60 | 65 | 19–55 | TM (65) | Yes (65) | 0 | 2-3 W | 0 | NR | NR | |
| NOT DEFINED | |||||||||||||
| Nagori et al. 2014a [40]. | PCS | 1.4Y | 19 | 19 | 16–25 | TM (19) | Yes (12) | Yes (7) | 1 W | 2 W | I | NR | |
| Nagori et al. 2014b [41]. | PCS | 1.25–2Y (1.65Y) | 53 | 57 | 15–25 | TM (17) | TM (40) | Yes (57) | Yes (12) | 1 W | 2 W | I | NR |
| Study | Pre-Intervention | At Intervention | Post-Intervention | Overall Risk of Bias | ||||
|---|---|---|---|---|---|---|---|---|
| Bias Due to Confounding | Bias in the Selection of Participants in the Study | Bias in Classification of Intervention | Bias Due to Deviation from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | ||
| Azaz et al. 1978 [36]. | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Kristerson et al. 1985 [27]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Hernandez et al. 1988 [28]. | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Andreasen II et al. 1990 [12]. | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Andreasen III et al. 1990 [10]. | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Andreasen IV et al. 1990 [29]. | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Kristernson et al. 1991 [37]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Paulsen et al. 1995 [30]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Paulsen et al. 1998 [31]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Bauss et al. 2002 [32]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Gault et al. 2002 [38]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Myrlund et al. 2004 [24]. | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Bauss et al. 2004 [25]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Mejàre et al. 2004 [39]. | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Reich et al. 2008 [33]. | Low | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Arikan et al. 2008 [35]. | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Yan et al. 2010 [22]. | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Sugai et al. 2010 [18]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Shahbazian et al. 2013 [23]. | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Plakwicz et al. 2013 [11]. | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Nagori et al. 2014 [40]. | Moderate | Low | Critical | Low | Low | Moderate | Moderate | Moderate |
| Nagori et al. 2014 [41]. | Moderate | Low | Critical | Low | Low | Moderate | Moderate | Moderate |
| Yu et al. 2017 [34]. | Low | Low | Low | Low | Low | Moderate | Low | Low |
| Ezeldeen et al. 2019 [26]. | Low | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Author | Survival (%) | Success (%) | Root Resorption | Pulp Condition | Root Formation | ||||
|---|---|---|---|---|---|---|---|---|---|
| Inflammatory Root Resorption (%) | Replacement Root Resorption (%) | Pulp Healing (%) | Pulp Obliteration (%) | Complete (%) | Incomplete (%) | Arrested (%) | |||
| OPEN APEX | |||||||||
| Kristerson et al. 1985 [27]. | 96.34 | NR | 2.43 | 7.31 | 90.25 | 100 | 57.31 | 42.69 | 0 |
| Hernandez et al. 1988 [28]. | 100 | 100 | 0 | 0 | 100 | NR | NR | NR | NR |
| Andreasen II et al. 1990 [12]. | 95 | NR | NR | NR | 95.9 | NR | NR | NR | NR |
| Andreasen III et al. 1990 [10]. | NR | NR | 2.52 | 3.78 | NR | NR | NR | NR | NR |
| Andreasen IV et al. 1990 [29]. | NR | NR | NR | NR | NR | NR | 21 | 65 | 14 |
| Paulsen et al. 1995 [30] /1998 [31]. | 93.3 | NR | 3.38 | 4.23 | 86.45 | 100 | 26 | 55 | 19 |
| Bauss et al. 2002 [32]. | 100 | 84.2 | NR | 5.3 | 90.8 | 90.8 | NR | NR | NR |
| Myrlund et al. 2004 [24]. | 98.6 | 90.5 | NR | NR | NR | NR | 19.1 | 54.4 | 26.5 |
| Bauss et al. 2004 [25]. | 100 | 86 | 8.23 | 4.7 | NR | 87.05 | NR | NR | 19 |
| Reich et al. 2008 [33]. | 95.5 | 95.5 | 0 | 0 | 100 | NR | 0 | 44 | 0 |
| Yan et al. 2010 [22]. | 100 | NR | 0 | 0 | 87.5 | NR | NR | NR | NR |
| Shahbazian et al. 2013 [23]. | 95.83 | 83.33 | 4.16 | 10.41 | 95.84 | NR | NR | 60.41 | NR |
| Plakwicz et al. 2013 [11]. | 100 | 91.3 | NR | 4.34 | 100 | 100 | NR | NR | NR |
| Ezeldeen et al. 2019 [26]. | 88 | 82 | 5 | 5 | NR | NR | NR | NR | NR |
| CLOSED APEX | |||||||||
| Azaz et al. 1978 [36]. | 89.18 | NR | NR | 32.43 | |||||
| Kristerson et al. 1985 [27]. | 77.77 | NR | 27.77 | 33.33 | |||||
| Andreasen II et al. 1990 [12]. | 98 | NR | NR | NR | |||||
| Andreasen III et al. 1990 [10]. | NR | NR | 18.86 | 16.98 | |||||
| Andreasen IV et al. 1990 [29]. | NR | NR | NR | NR | |||||
| Kristerson et al. 1991 [37]. | 88.88 | 83.33 | 0 | 5.55 | |||||
| Gault et al. 2002 [38]. | 95.75 | 95.75 | 0 | 0 | |||||
| Mejàre et al. 2004 [39]. | 81.4 | NR | NR | 2.12 | |||||
| Arikan et al. 2008 [35]. | 93.5 | NR | NR | NR | |||||
| Yan et al. 2010 [22]. | 89.47 | NR | 10.52 | 0 | |||||
| Sugai et al. 2010 [18]. | 96 | 88 | 4.27 | 4.27 | |||||
| Yu et al. 2017 [34]. | 90.8 | NR | 10.8 | 9.2 | |||||
| NOT DEFINED | |||||||||
| Nagori et al. 2014a [40]. | 94.73 | 94.73 | 0 | 0 | NR | NR | NR | NR | NR |
| Nagori et al. 2014b [41]. | 98.24 | 86 | 10,28 | NR | NR | NR | 21.05 | 78.95 | NR |
| Survival (%) | Success (%) | Root Resorption | ||
|---|---|---|---|---|
| Inflammatory Root Resorption (%) | Replacement Root Resorption (%) | |||
| Overall | 95.9 ± 0.8 | 89.4 ± 1.55 | 3.8 ± 0.8 | 4.3 ± 0.7 |
| Open apex | 96.9 ± 1.0 | 88.6 ± 2.1 | 2.8 ± 0.6 | 4.0 ± 0.7 |
| Closed apex | 93.0 ± 1.7 | 90.9 ± 3.5 | 7.8 ± 3.1 | 9.0 ± 3.4 |
| p-value | p = 0.052 | p = 0.564 | p = 0.233 | p = 0.471 |
| Canines | ||||
| Open apex | (-) | (-) | (-) | (-) |
| Closed apex | 91.6 ± 3.3 | (-) | (-) | (-) |
| p-value | (-) | (-) | (-) | (-) |
| Premolars | ||||
| Open apex | 95.5 ± 1.2 | 87.5 ± 3.2 | 2.9 ± 0.7 | 4.3 ± 0.8 |
| Closed apex | 90.2 ± 9.8 | (-) | 20.7 ± 4.8 | 22.1 ± 0.7 |
| p-value | p = 0.797 | (-) | (-) | p = 0.001 |
| Third molars | ||||
| Open apex | 99.7 ± 0.8 | 90.6 ± 3.5 | 2.6 ± 2.5 | 2.7 ± 1.5 |
| Closed apex | 88.4 ± 2.6 | (-) | 6.8 ± 3.9 | 3.8 ± 2.0 |
| p-value | p = 0.001 | (-) | (-) | p = 0.660 |
| Open apex | ||||
| Premolars | 95.5 ± 1.2 | 87.5 ± 3.2 | 2.9 ± 0.7 | 4.3 ± 0.8 |
| Third Molars | 99.7 ± 0.8 | 90.6 ± 3.5 | 2.6 ± 2.5 | 2.7 ± 1.5 |
| p-value | p = 0.008 | p = 0.534 | p = 0.714 | p = 0.256 |
| Closed apex | ||||
| Premolars | 90.2 ± 9.8 | (-) | 20.7 ± 4.8 | 22.1 ± 0.7 |
| Third Molars | 88.4 ± 2.6 | (-) | 6.8 ± 3.9 | 3.8 ± 2.0 |
| p-value | p = 0.046 | (-) | p = 0.035 | p = 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucas-Taulé, E.; Bofarull-Ballús, A.; Llaquet, M.; Mercade, M.; Hernández-Alfaro, F.; Gargallo-Albiol, J. Does Root Development Status Affect the Outcome of Tooth Autotransplantation? A Systematic Review and Meta-Analysis. Materials 2022, 15, 3379. https://doi.org/10.3390/ma15093379
Lucas-Taulé E, Bofarull-Ballús A, Llaquet M, Mercade M, Hernández-Alfaro F, Gargallo-Albiol J. Does Root Development Status Affect the Outcome of Tooth Autotransplantation? A Systematic Review and Meta-Analysis. Materials. 2022; 15(9):3379. https://doi.org/10.3390/ma15093379
Chicago/Turabian StyleLucas-Taulé, Ernest, Anna Bofarull-Ballús, Marc Llaquet, Montse Mercade, Federico Hernández-Alfaro, and Jordi Gargallo-Albiol. 2022. "Does Root Development Status Affect the Outcome of Tooth Autotransplantation? A Systematic Review and Meta-Analysis" Materials 15, no. 9: 3379. https://doi.org/10.3390/ma15093379