
Biomechanical Analyses of Porous Designs of 3D-Printed Titanium Implant for Mandibular Segmental Osteotomy Defects

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
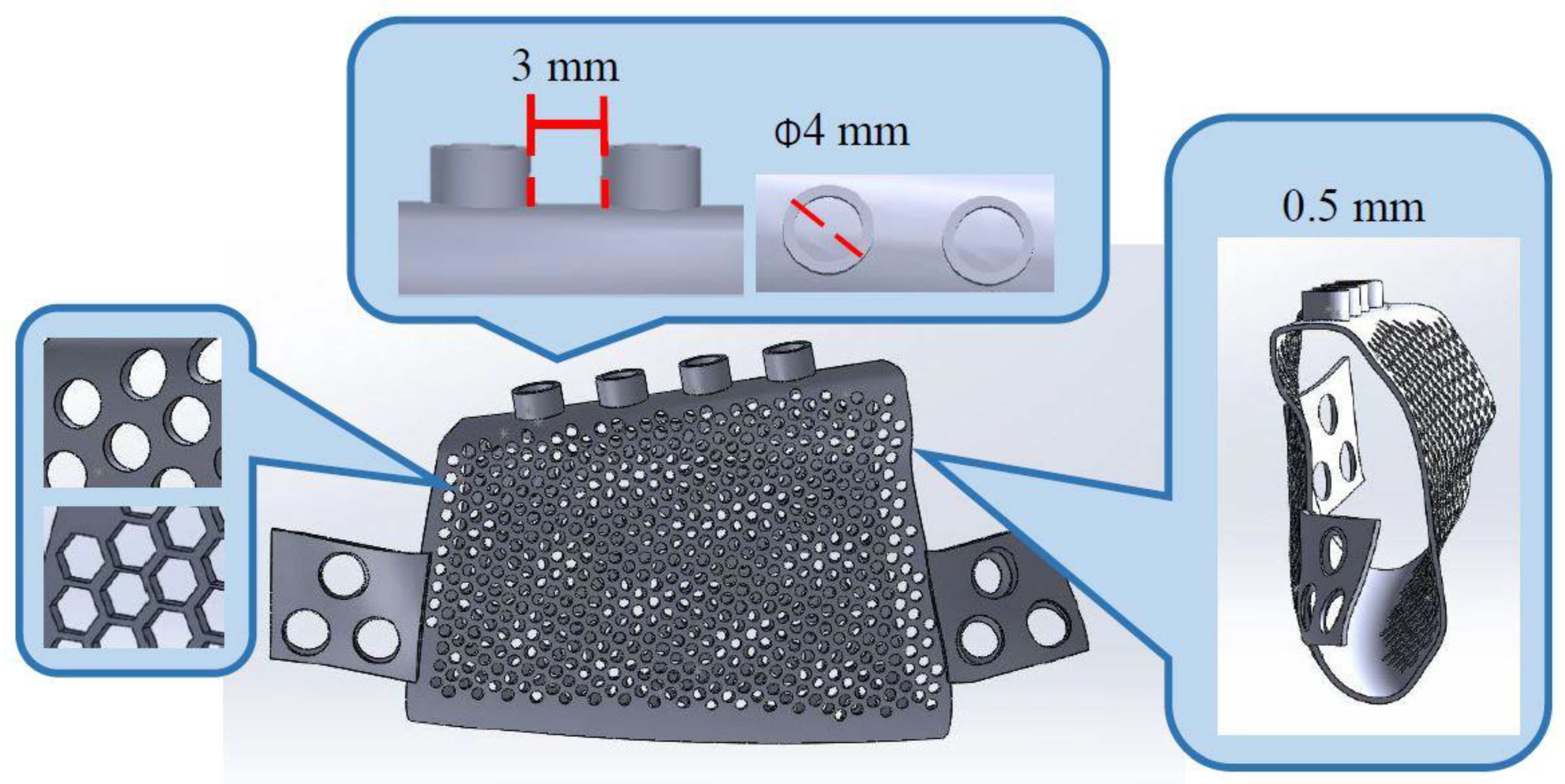
2.1. 3D Computer Model Establishment
2.2. FEA
2.3. 3D Printing and In Vitro Experiments
3. Results
3.1. In Vitro Experiments
3.2. FEA
3.2.1. Von Mises Stress of the Implant Body
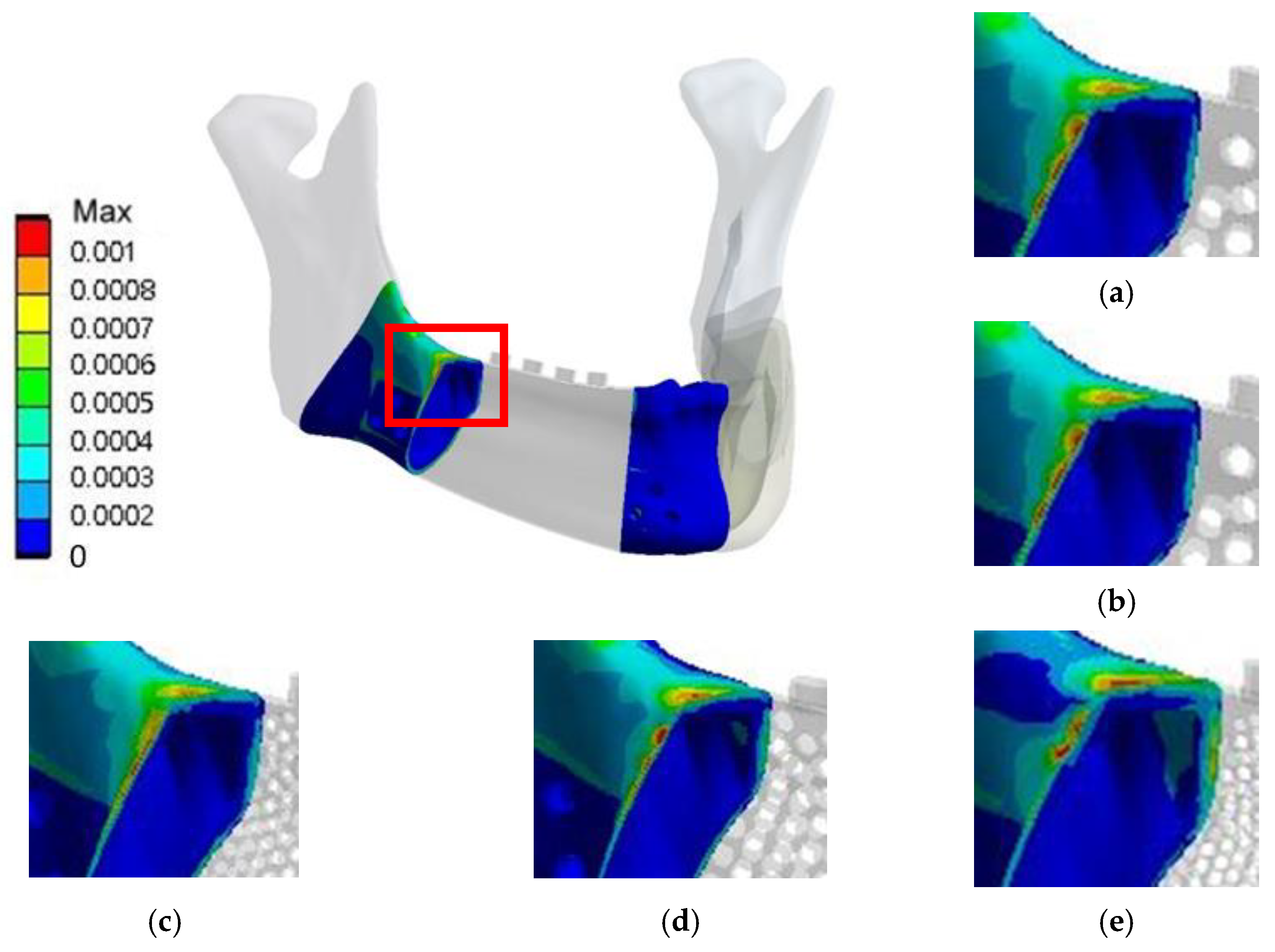
3.2.2. Von Mises Strain in the Bone around the Implant
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seikaly, H.; Chau, J.; Li, F.; Driscoll, B.; Seikaly, D.; Calhoun, J.; Calhoun, K.H. Bone that best matches the properties of the mandible. J. Otolaryngol. 2003, 32, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Bak, M.; Jacobson, A.S.; Buchbinder, D.; Urken, M.L. Contemporary reconstruction of the mandible. Oral Oncol. 2010, 46, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Foster, R.D.; Anthony, J.P.; Sharma, A.; Pogrel, M.A. Vascularized bone flaps versus nonvascularized bone grafts for mandibular reconstruction: An outcome analysis of primary bony union and endosseous implant success. Head Neck J. Sci. Spec. Head Neck 1999, 21, 66–71. [Google Scholar] [CrossRef]
- Batstone, M. Reconstruction of major defects of the jaws. Aust. Dent. J. 2018, 63, S108–S113. [Google Scholar] [CrossRef] [Green Version]
- Likhterov, I.; Roche, A.M.; Urken, M.L. Contemporary osseous reconstruction of the mandible and the maxilla. Oral Maxillofac. Surg. Clin. 2019, 31, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; D’Addazio, G.; De Tullio, I.; Traini, T.; Caputi, S. Peri-Implant Bone Resorption during Healing Abutment Placement: The Effect of a 0.20 Chlorhexidine Gel vs. Placebo—A Randomized Double Blind Controlled Human Study. BioMed Res. Int. 2018, 2018, 5326340. [Google Scholar] [CrossRef] [Green Version]
- D’Ercole, S.; D’Addazio, G.; Di Lodovico, S.; Traini, T.; Di Giulio, M.; Sinjari, B. Porphyromonas Gingivalis load is balanced by 0.20% chlorhexidine gel. A randomized, double-blind, controlled, microbiological and immunohistochemical human study. J. Clin. Med. 2020, 9, 284. [Google Scholar] [CrossRef] [Green Version]
- Sinibaldi, R.; Conti, A.; Sinjari, B.; Spadone, S.; Pecci, R.; Palombo, M.; Komlev, V.; Ortore, M.; Tromba, G.; Capuani, S. Multimodal-3D imaging based on μMRI and μCT techniques bridges the gap with histology in visualization of the bone regeneration process. J. Tissue Eng. Regen. Med. 2018, 12, 750–761. [Google Scholar] [CrossRef] [PubMed]
- Vaish, A.; Vaish, R. 3D printing and its applications in Orthopedics. J. Clin. Orthop. Trauma 2018, 9, S74–S75. [Google Scholar] [CrossRef]
- Frizziero, L.; Santi, G.M.; Liverani, A.; Giuseppetti, V.; Trisolino, G.; Maredi, E.; Stilli, S. Paediatric orthopaedic surgery with 3D printing: Improvements and cost reduction. Symmetry 2019, 11, 1317. [Google Scholar] [CrossRef] [Green Version]
- Eshkalak, S.K.; Ghomi, E.R.; Dai, Y.; Choudhury, D.; Ramakrishna, S. The role of three-dimensional printing in healthcare and medicine. Mater. Des. 2020, 108940. [Google Scholar] [CrossRef]
- Eltorai, A.E.; Nguyen, E.; Daniels, A.H. Three-dimensional printing in orthopedic surgery. Orthopedics 2015, 38, 684–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinescu, R.; Popescu, D.; Laptoiu, D. A Review on 3D-Printed Templates for Precontouring Fixation Plates in Orthopedic Surgery. J. Clin. Med. 2020, 9, 2908. [Google Scholar] [CrossRef]
- Nadagouda, M.N.; Rastogi, V.; Ginn, M. A review on 3D printing techniques for medical applications. Curr. Opin. Chem. Eng. 2020, 28, 152–157. [Google Scholar] [CrossRef]
- Cheng, L.; Shoma Suresh, K.; He, H.; Rajput, R.S.; Feng, Q.; Ramesh, S.; Wang, Y.; Krishnan, S.; Ostrovidov, S.; Camci-Unal, G. 3D printing of micro-and nanoscale bone substitutes: A review on technical and translational perspectives. Int. J. Nanomed. 2021, 16, 4289–4319. [Google Scholar] [CrossRef] [PubMed]
- Memon, A.R.; Wang, E.; Hu, J.; Egger, J.; Chen, X. A review on computer-aided design and manufacturing of patient-specific maxillofacial implants. Expert Rev. Med. Devices 2020, 17, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Du, R.; Su, Y.-X.; Yan, Y.; Choi, W.S.; Yang, W.-F.; Zhang, C.; Chen, X.; Curtin, J.P.; Ouyang, J.; Zhang, B. A Systematic Approach for Making 3D-Printed Patient-Specific Implants for Craniomaxillofacial Reconstruction. Engineering 2020, 6, 1291–1301. [Google Scholar] [CrossRef]
- Bianchi, G.; Frisoni, T.; Spazzoli, B.; Lucchese, A.; Donati, D. Computer Assisted Surgery and 3D Printing in Orthopaedic Oncology: A Lesson Learned by Cranio-Maxillo-Facial Surgery. Appl. Sci. 2021, 11, 8584. [Google Scholar] [CrossRef]
- Huang, S.-N.; Shie, M.-Y.; Shen, Y.-W.; Hsu, J.-T.; Huang, H.-L.; Fuh, L.-J. Biomechanical Assessment of Design Parameters on a Self-Developed 3D-Printed Titanium-Alloy Reconstruction/Prosthetic Implant for Mandibular Segmental Osteotomy Defect. Metals 2019, 9, 597. [Google Scholar] [CrossRef] [Green Version]
- Yao, C.; Chen, D.; Zheng, Z.; Wang, Q.; Fu, K. Research on porous titanium implants and its animal experiments. Rapid Prototyp. J. 2020, 27, 13–23. [Google Scholar] [CrossRef]
- Korioth, T.W.; Hannam, A.G. Mandibular forces during simulated tooth clenching. J. Orofac. Pain 1994, 8, 178–189. [Google Scholar] [PubMed]
- Huang, H.-L.; Su, K.-C.; Fuh, L.-J.; Chen, M.Y.; Wu, J.; Tsai, M.-T.; Hsu, J.-T. Biomechanical analysis of a temporomandibular joint condylar prosthesis during various clenching tasks. J. Cranio-Maxillofac. Surg. 2015, 43, 1194–1201. [Google Scholar] [CrossRef] [PubMed]
- Moiduddin, K. Implementation of computer-assisted design, analysis, and additive manufactured customized mandibular implants. J. Med. Biol. Eng. 2018, 38, 744–756. [Google Scholar] [CrossRef]
- Frost, H.M. Bone “mass” and the “mechanostat”: A proposal. Anat. Rec. 1987, 219, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hubbell, Z.R. Mechanostat. Int. Encycl. Biol. Anthropol. 2018, 1–2. [Google Scholar]
- Biewener, A.A. Safety factors in bone strength. Calcif. Tissue Int. 1993, 53, S68–S74. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Young’s Modulus (MPa) | Poisson’s Ratio |
|---|---|---|
| 3D-printed titanium alloy | 129,000 | 0.34 |
| Titanium alloy | 110,000 | 0.33 |
| Cortical bone | 13,400 | 0.3 |
| Trabecular bone | 790 | 0.3 |
| Clenching Tasks | Side | Direction | Muscular Force | Occlusal Force | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| SM | DM | MP | AT | MT | PT | |||||
| RMOL | Right | Force | 137.1 | 58.8 | 146.8 | 115.3 | 63.1 | 44.6 | Fx Fy Fz | −100 |
| Fx | −28.1 | −32.1 | 71.4 | −17.2 | −14.0 | −9.3 | ||||
| Fy | −57.4 | 21.0 | −54.8 | −5.1 | 31.5 | 38.1 | ||||
| Fz | 121.2 | 44.5 | 116.1 | 114.0 | 52.8 | 21.1 | ||||
| Left | Force | 114.2 | 49.0 | 104.9 | 91.6 | 64.1 | 29.5 | |||
| Fx | 23.6 | 26.7 | −51.0 | 13.7 | 14.2 | 6.1 | ||||
| Fy | −47.9 | 17.5 | −39.1 | −4.0 | 32.0 | 25.2 | ||||
| Fz | 101.0 | 37.1 | 83.0 | 90.5 | 53.6 | 14.0 | ||||
| RGF | Right | Force | 34.3 | 29.4 | 12.2 | 104.3 | 61.2 | 46.9 | Fx Fy Fz | −100 |
| Fx | −7.1 | −16.0 | 6.0 | −15.5 | −13.6 | 9.8 | ||||
| Fy | −14.4 | 10.5 | −4.6 | −4.6 | 30.6 | 40.1 | ||||
| Fz | 30.3 | 22.3 | 9.7 | 103.0 | 51.2 | 22.2 | ||||
| Left | Force | 51.4 | 21.2 | 132.8 | 11.1 | 5.7 | 4.5 | |||
| Fx | 10.6 | 11.6 | −64.6 | 1.7 | −1.3 | −0.9 | ||||
| Fy | −21.5 | 7.6 | −49.6 | −0.5 | 2.9 | 3.9 | ||||
| Fz | 45.4 | 16.1 | 105.1 | 10.9 | 4.8 | 2.2 | ||||
| Position | Control | Experiment | p | ||
|---|---|---|---|---|---|
| Max principal strain (μ strain) | A | Median | 715.23 | −90.61 | 0.021 |
| IQR | 221.00 | 738.48 | |||
| B | Median | 1270.42 | 3114.37 | 0.021 | |
| IQR | 260.84 | 419.94 | |||
| C | Median | 480.41 | 1109.03 | 0.021 | |
| IQR | 89.44 | 2442.460 | |||
| Min principal strain (μ strain) | A | Median | −1525.53 | −2246.89 | 0.021 |
| IQR | 218.18 | 96.52 | |||
| B | Median | −1240.42 | −1077.21 | 0.083 | |
| IQR | 174.62 | 184.85 | |||
| C | Median | −1497.91 | −514.52 | 0.021 | |
| IQR | 148.19 | 461.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, Y.-W.; Tsai, Y.-S.; Hsu, J.-T.; Shie, M.-Y.; Huang, H.-L.; Fuh, L.-J. Biomechanical Analyses of Porous Designs of 3D-Printed Titanium Implant for Mandibular Segmental Osteotomy Defects. Materials 2022, 15, 576. https://doi.org/10.3390/ma15020576
Shen Y-W, Tsai Y-S, Hsu J-T, Shie M-Y, Huang H-L, Fuh L-J. Biomechanical Analyses of Porous Designs of 3D-Printed Titanium Implant for Mandibular Segmental Osteotomy Defects. Materials. 2022; 15(2):576. https://doi.org/10.3390/ma15020576
Chicago/Turabian StyleShen, Yen-Wen, Yuen-Shan Tsai, Jui-Ting Hsu, Ming-You Shie, Heng-Li Huang, and Lih-Jyh Fuh. 2022. "Biomechanical Analyses of Porous Designs of 3D-Printed Titanium Implant for Mandibular Segmental Osteotomy Defects" Materials 15, no. 2: 576. https://doi.org/10.3390/ma15020576