
Application of Texture and Fractal Dimension Analysis to Evaluate Subgingival Cement Surfaces in Terms of Biocompatibility


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
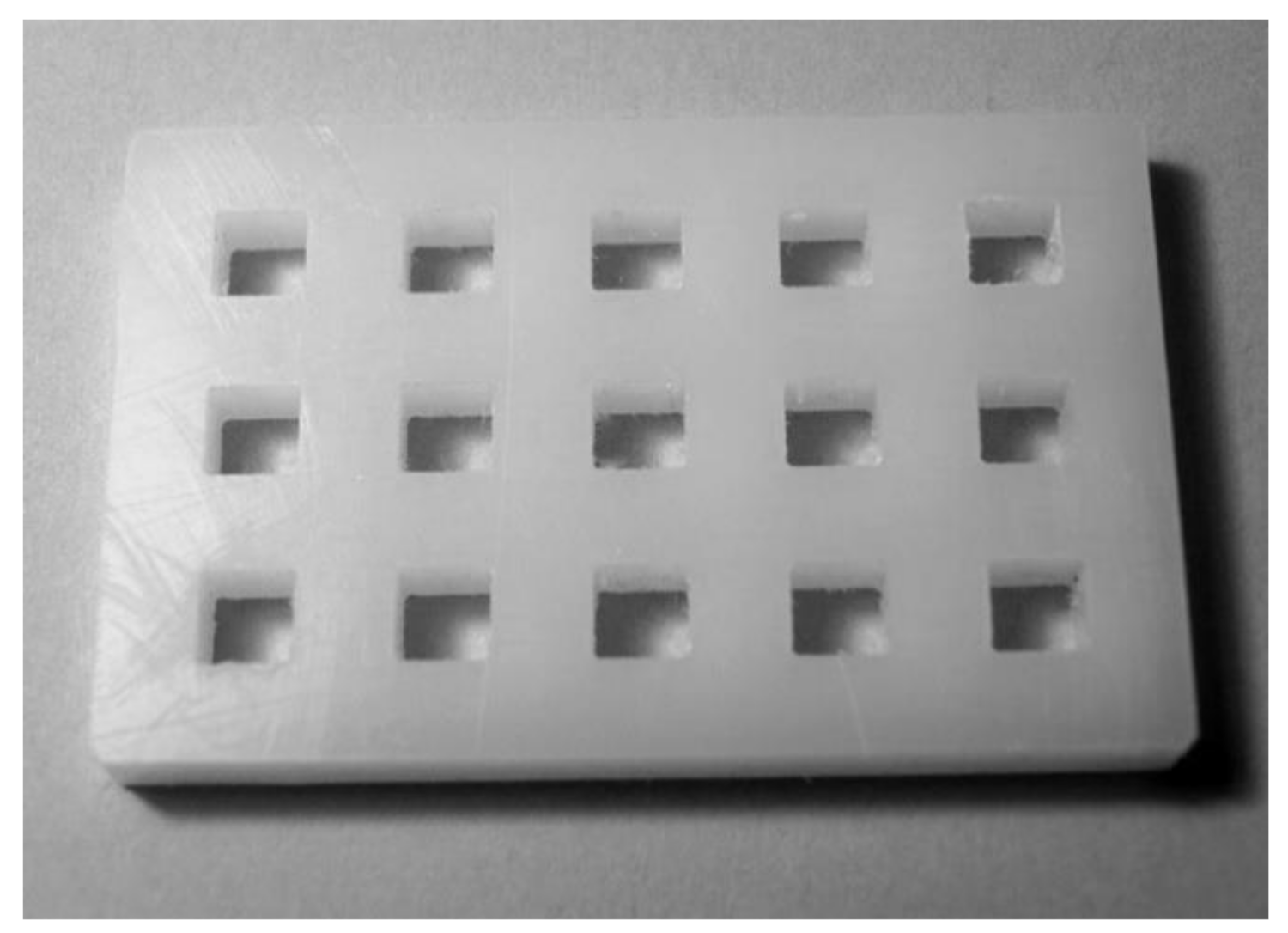
2.1. Procedure for Preparing the Cement Samples
2.2. Biological Evaluation
2.2.1. Cell Line
2.2.2. Determination of Cytotoxicity
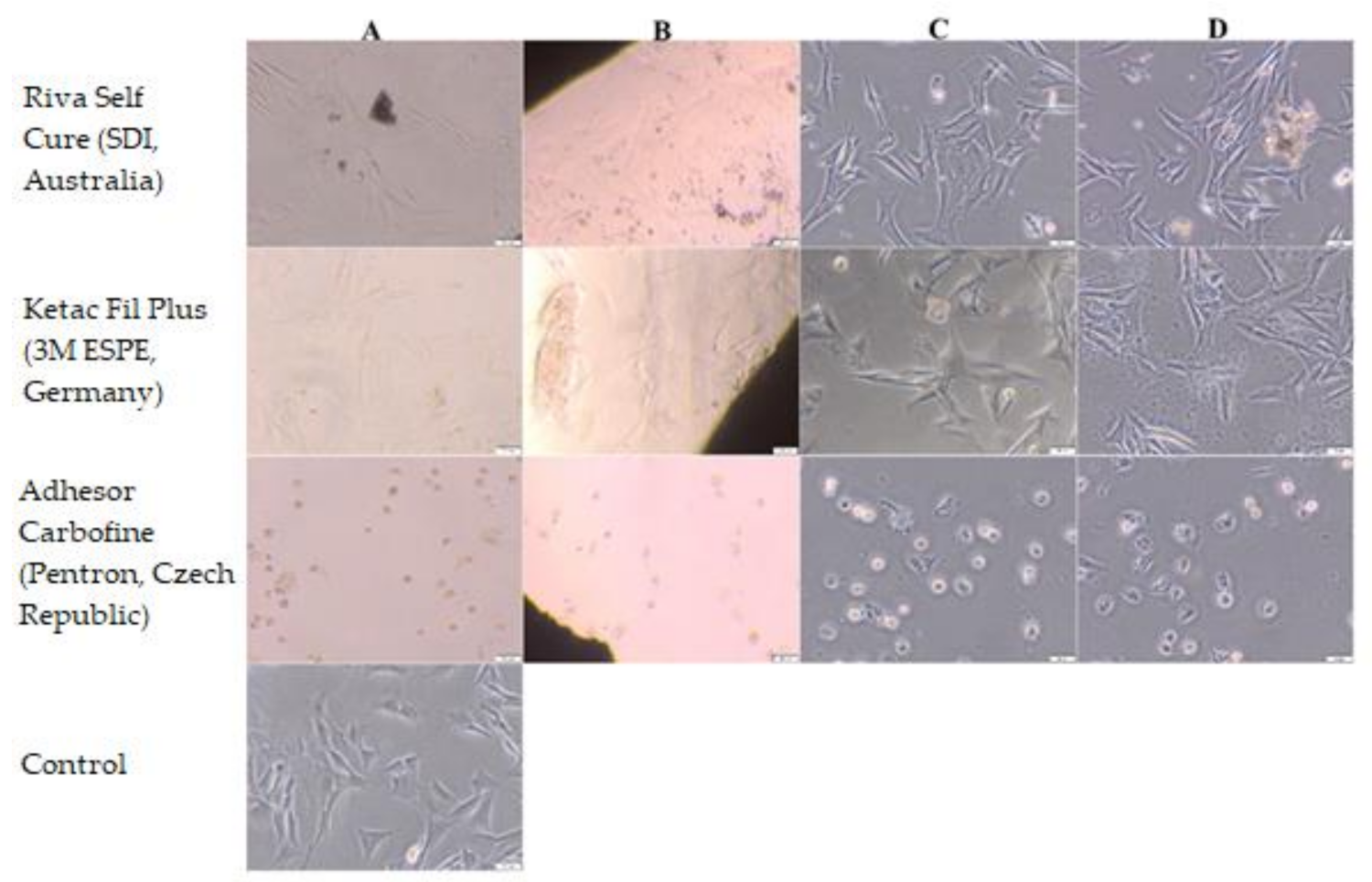
2.2.3. Cell Adhesion
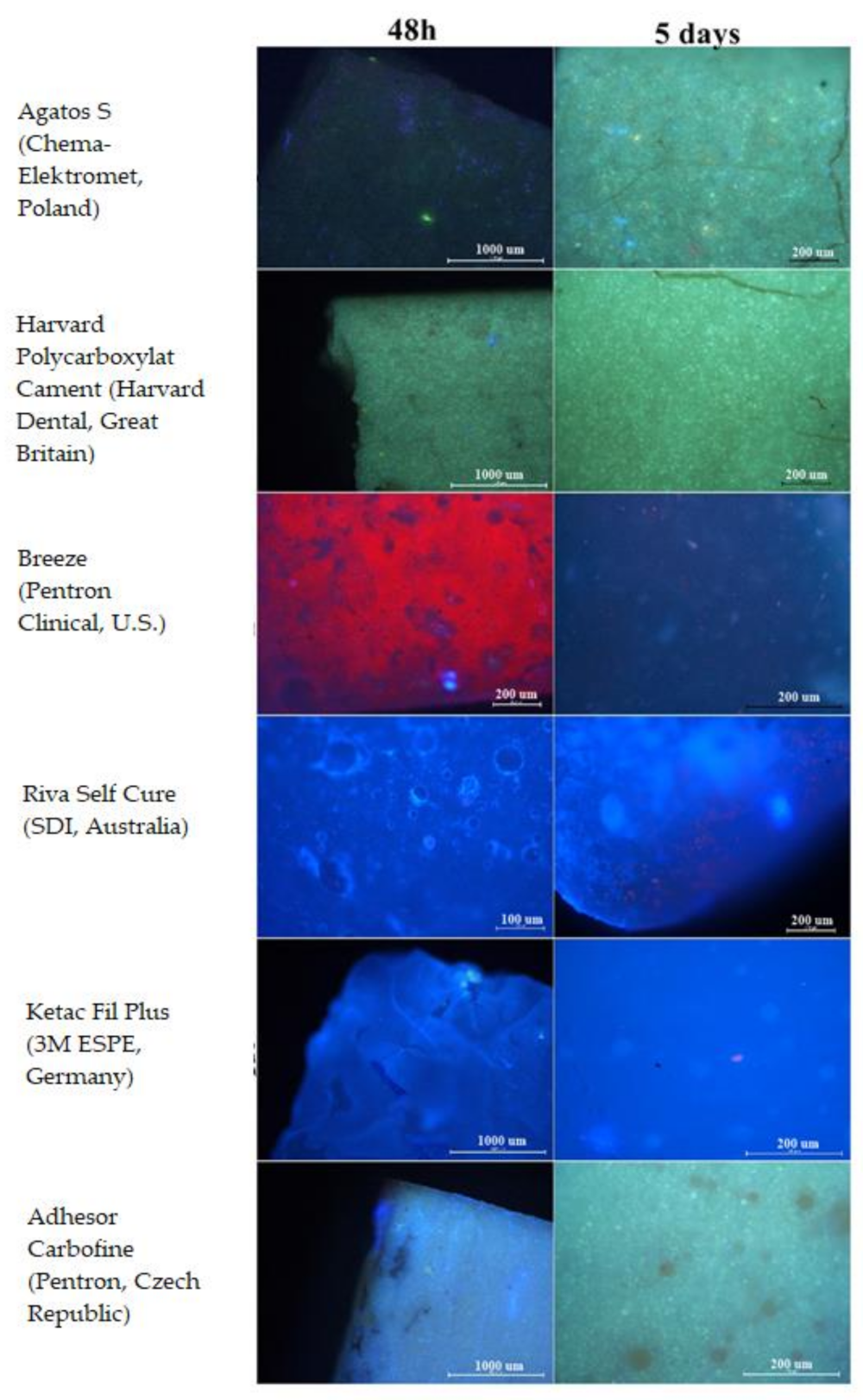
2.3. Taking Images
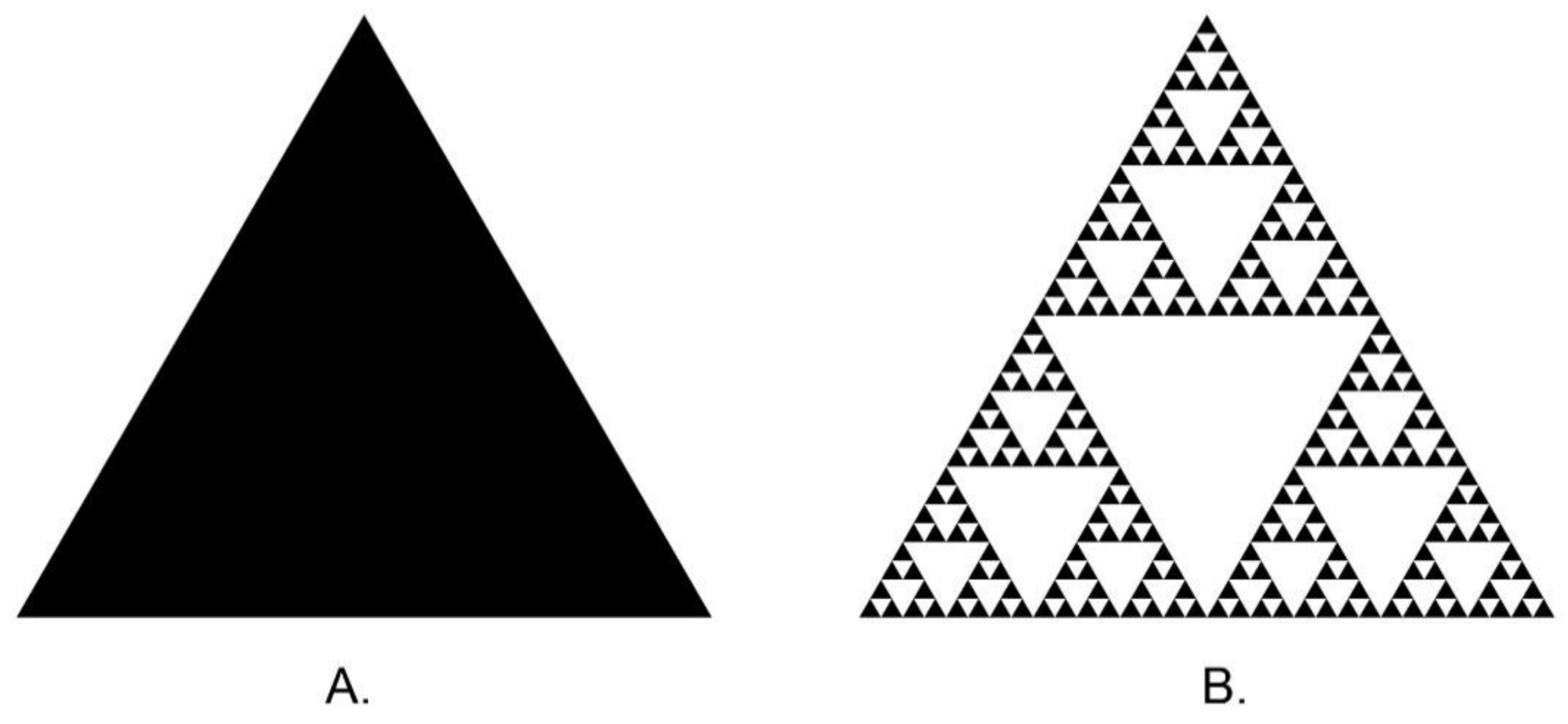
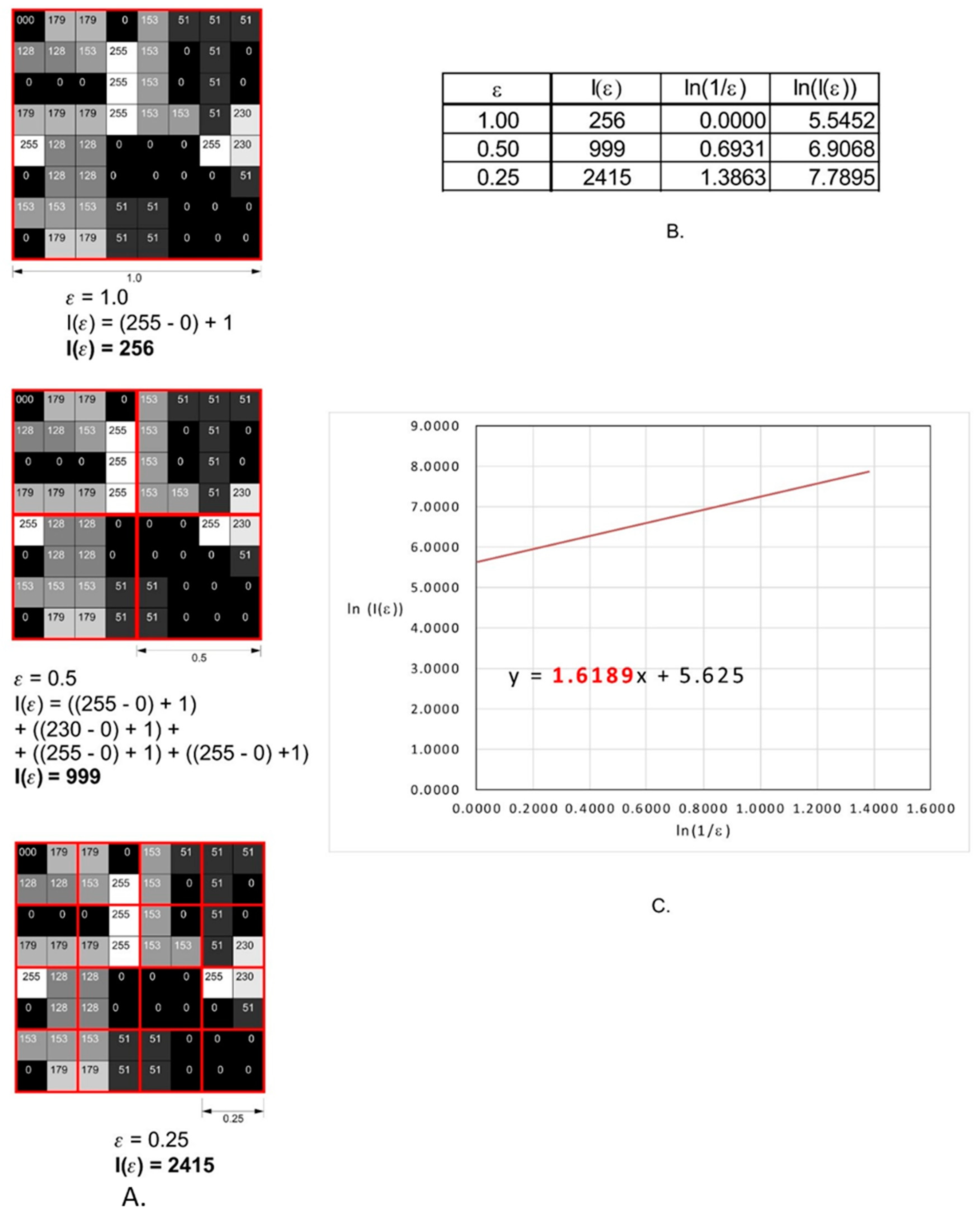
2.4. Fractal Dimension Analysis
2.5. Texture Analysis
2.6. Statistical Analysis
3. Results
3.1. Fractal Dimension
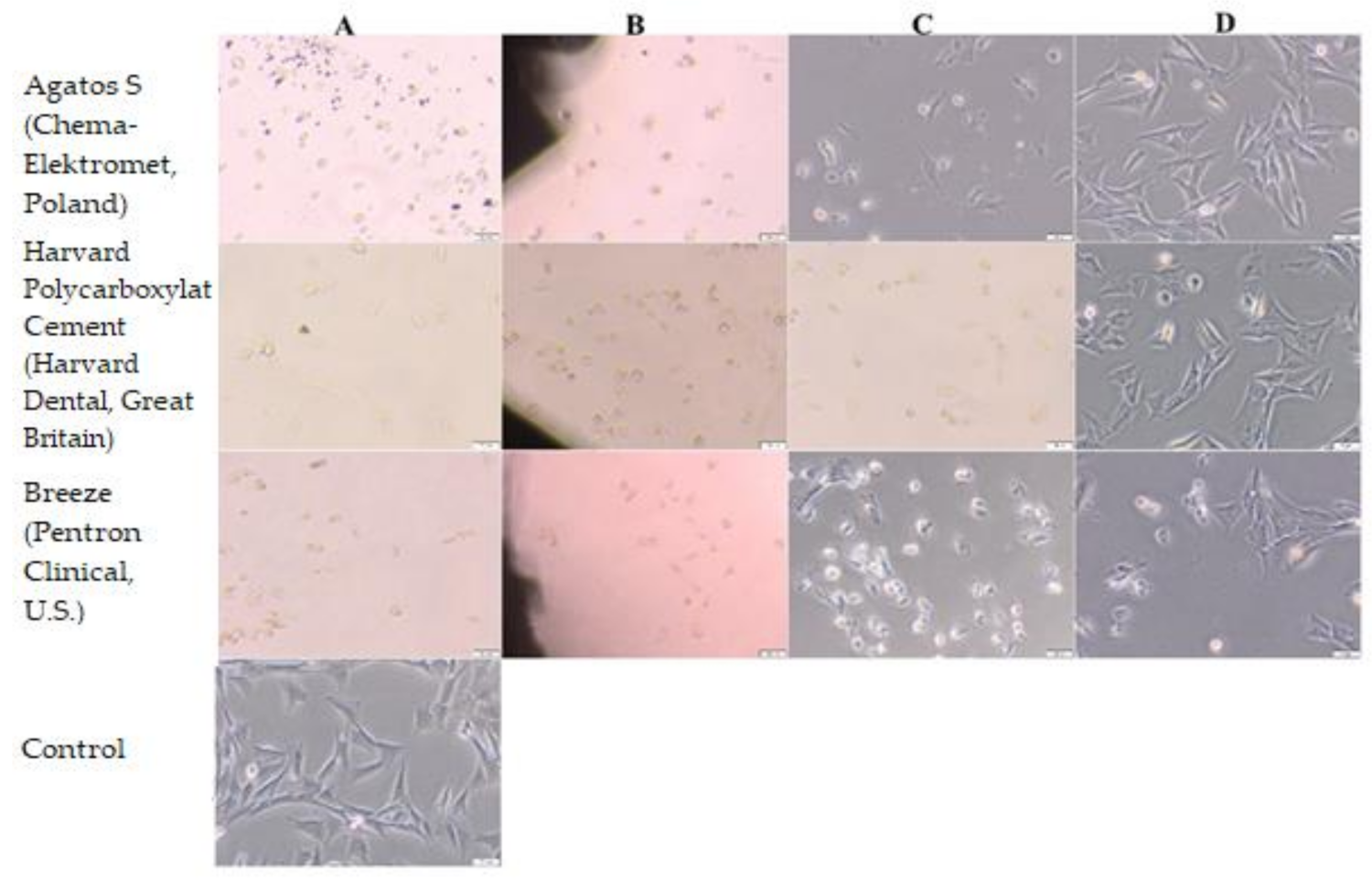
3.2. Biological Evaluation
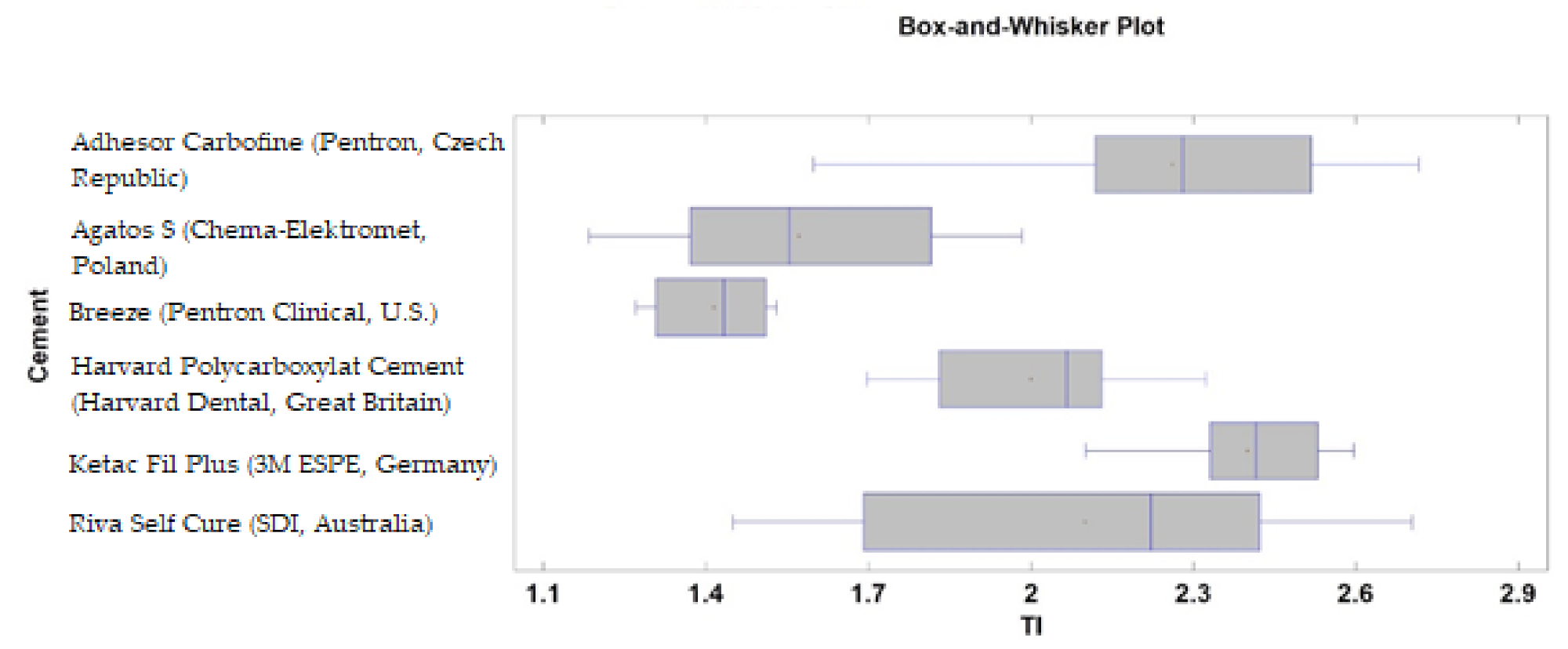
3.3. Texture Analysis
4. Discussion
5. Conclusions
- The Ketac Fil Plus (3M ESPE, Germany) and Riva Self Cure (SDI, Australia) cements provided the most favorable conditions for fibroblast adhesion, despite the statistically significant differences in the fractal dimension between them. Insofar as the surface texture is considered, Ketac Fil Plus (3M ESPE, Germany) cement should be indicated here.
- Ketac Fil Plus (3M ESPE, Germany) and Riva Self Cure (SDI, Australia) also showed no cytotoxicity potential. In contrast, Adhesor Carbofine (Pentron, Czech Republic) caused a severe cytotoxicity effect. Other cements, Agatos S (Chema-Elektromet, Poland), Harvard Polycarboxylat Cement (Harvard Dental, Great Britain), and Breeze (Pentron Clinical, USA), showed a moderate cytotoxicity effect on Balb/3T3 cells.
- Moderate positive correlation was observed between fractal dimension (FD) and the amounts of cells after 48 h. The correlation coefficient was decreased to a weak positive linear after 5 days.
- The study revealed a moderate negative linear correlation between texture index (TI), Bone index (BI), and the amounts of cells after 48 h of incubation. The correlation coefficient decreased to weak negative linear after 5 days.
6. Study Limitations
- Flat surfaces of cements were investigated to simplify taking microscopic photos for analysis. In real restorations, the surface is most commonly a cylinder; this may affect fibroblast culturing.
- Some of the examined cements: Ketac Fil Plus (3M ESPE, Germany) and Riva Self Cure (SDI, Australia) may release fluoride ions which may affect cytotoxicity.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anderson, J.M. Biological Responses to Materials. Annu. Rev. Mater. Res. 2001, 31, 81–110. [Google Scholar] [CrossRef]
- Wataha, J.C. Principles of biocompatibility of dental practicioners. J. Prosthet. Dent. 2001, 86, 203–209. [Google Scholar] [CrossRef]
- Costa, C.A.D.S.; Hebling, J.; Scheffel, D.L.; Soares, D.G.; Basso, F.G.; Ribeiro, A.P.D. Methods to evaluate and strategies to improve the biocompatibility of dental materials and operative techniques. Dent. Mater. 2014, 30, 769–784. [Google Scholar] [CrossRef]
- Mallineni, S.K.; Nuvvula, S.; Matinlinna, J.P.; You, C.K.; King, N.M. Biocompatibility of various dental materials in contem-porary dentistry: A narrative insight. J. Investig. Clin. Dent. 2013, 4, 9–19. [Google Scholar] [CrossRef]
- Bertoldi, C.; Monari, E.; Cortellini, P.; Generali, L.; Lucchi, A.; Spinato, S.; Zaffe, D. Clinical and histological reaction of peri-odontal tissues to subgingival resin composite restorations. Clin. Oral Investig. 2020, 24, 1001–1011. [Google Scholar] [CrossRef]
- Binaljadm, T.; Moorehead, R.; Almela, T.; Franklin, K.; Tayebi, L.; Moharamzadeh, K. Biomodification of a Class-V Restorative Material by Incorporation of Bioactive Agents. Dent. J. 2019, 7, 110. [Google Scholar] [CrossRef] [Green Version]
- Forster, A.; Ungvári, K.; Györgyey, A.; Kukovecz, A.; Turzó, K.; Nagy, K. Human epithelial tissue culture study on restorative materials. J. Dent. 2014, 42, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Caughman, W.F.; Caughman, G.B.; Dominy, W.T.; Schuster, G.S. Glass ionomer and composite resin cements: Effects on oral cells. J. Prosthet. Dent. 1990, 63, 513–521. [Google Scholar] [CrossRef]
- Schmidt, J.C.; Sahrmann, P.; Weiger, R.; Schmidlin, P.R.; Walter, C. Biologic width dimensions—A systematic review. J. Clin. Periodontol. 2013, 40, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.R.; Lucchesi, J.A.; Cortelli, S.C.; Amaral, C.M.; Feres, M.; Duarte, P.M. Effects of Glass Ionomer and Microfilled Composite Subgingival Restorations on Periodontal Tissue and Subgingival Biofilm: A 6-Month Evaluation. J. Periodontol. 2007, 78, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Tyas, M.J. The Class V lesion—Aethiology and restoration. Aust. Dent. J. 1995, 40, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Paolantonio, M.; D’ercole, S.; Perinetti, G.; Tripodi, D.; Catamo, G.; Serra, E.; Brue, C.; Piccolomini, R. Clinical and microbio-logical effects of different restorative materials on the periodontal tissues adjacent to subgingival class V restorations. J. Clin. Periodontol. 2004, 31, 200–207. [Google Scholar] [CrossRef]
- Biniraj, K.R.; Sagir, M.; Sunil, M.M.; Janardhanan, M. Clinical attachment level gain and bone regeneration around a glass ionomer restoration on root surface wall of periodontal pocket. J. Indian Soc. Periodontol. 2012, 16, 442–445. [Google Scholar] [CrossRef] [PubMed]
- Mickenautsch, S.; Mount, G.; Yengopal, V. Therapeutic effect of glass-ionomers: An overview of evidence. Aust. Dent. J. 2011, 56, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, S.K.; Carrick, T.E.; McCabe, J.F. Temperature mediated coefficient of dimensional change of dental tooth-colored re-storative materials. Dent. Mater. 2004, 20, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-Y.; Lee, H.-H.; Kim, H.-W. Bioactive sol–gel glass added ionomer cement for the regeneration of tooth structure. J. Mater. Sci. Mater. Electron. 2008, 19, 3287–3294. [Google Scholar] [CrossRef]
- Fuhrmann, D.; Murchison, D.; Whipple, S.; Vandewalle, K. Properties of New Glass-Ionomer Restorative Systems Marketed for Stress-Bearing Areas. Oper. Dent. 2020, 45, 104–110. [Google Scholar] [CrossRef]
- Khoroushi, M.; Keshani, F. A review of glass-ionomers: From conventional glass-ionomer to bioactive glass-ionomer. Dent. Res. J. 2013, 10, 411–420. [Google Scholar]
- Hill, E.E. Dental Cements for Definitive Luting: A Review and Practical Clinical Considerations. Dent. Clin. North Am. 2007, 51, 643–658. [Google Scholar] [CrossRef]
- Boing, T.F.; De Geus, J.L.; Wambier, L.M.; Loguercio, A.D.; Reis, A.; Gomes, O.M.M. Are Glass-Ionomer Cement Restorations in Cervical Lesions More Long-Lasting than Resin-based Composite Resins? A Systematic Review and Meta-Analysis. J. Adhes Dent. 2018, 20, 435–452. [Google Scholar]
- Manso, A.P.; Carvalho, R.M. Dental Cements for Luting and Bonding Restorations: Self-Adhesive Resin Cements. Dent. Clin. North Am. 2017, 61, 821–834. [Google Scholar] [CrossRef] [PubMed]
- Makkar, S.; Malhotra, N. Self-adhesive resin cements: A new perspective in luting technology. Dent. Updat. 2013, 40, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yu, H.Y. Does dental zinc phosphate cement really shrink in clinical applications? Med. Hypotheses 2009, 73, 257–258. [Google Scholar] [CrossRef]
- Donovan, E.T.; Cho, G.C. Contemporary evaluation of dental cements. Compend. Contin. Educ. Dent. 1999, 20, 197–199, 202–208, 210. [Google Scholar]
- Ali, M.N.; Edwards, M.; Nicholson, J.W. Zinc polycarboxylate dental cement for the controlled release of an active organic substance: Proof of concept. J. Mater. Sci. Mater. Electron. 2009, 21, 1249–1253. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, W. Dental Materials and Their Selection, 3rd ed.; Quintessence: Chicago, IL, USA, 2002; pp. 133–155. [Google Scholar]
- Bodrumlu, E. Biocompatibility of retrograde root filling materials: A review. Aust. Endod. J. 2008, 34, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Qutieshat, A.S.; Al-Hiyasat, A.S.; Darmani, H. Biocompatibility evaluation of Jordanian Portland cement for potential future dental application. J. Conserv. Dent. 2019, 22, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Armi, L.; Fekri-Ershad, S. Texture Analysis and texture classification methods—A review. Int. Online J. Image Process. Pattern Recognit. 2019, 2, 1–29. [Google Scholar]
- Castellano, G.; Bonilha, L.; Li, L.; Cendes, F. Texture analysis of medical images. Clin. Radiol. 2004, 59, 1061–1069. [Google Scholar] [CrossRef]
- Gonçalves, B.C.; De Araújo, E.C.; Nussi, A.D.; Bechara, N.; Sarmento, D.; Oliveira, M.S.; Santamaria, M.P.; Costa, A.L.F.; Lopes, S. Texture analysis of cone-beam computed tomography images assists the detection of furcal lesion. J. Periodontol. 2020, 91, 1159–1166. [Google Scholar] [CrossRef]
- Lee, K.M.; Kim, H.G.; Lee, Y.H.; Kim, E.J. mDixon-based texture analysis of an intraosseous lipoma: A case report and current review for the dental clinician. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, e67–e71. [Google Scholar] [CrossRef]
- Jatti, A.; Joshi, R. Characterization of dental pathologies using digital panoramic X-ray images based on texture analysis. In Proceedings of the 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC) 2017, Jeju Island, Korea, 11–15 July 2017; pp. 592–595. [Google Scholar] [CrossRef]
- Sánchez, I.; Uzcátegui, G. Fractals in dentistry. J. Dent. 2011, 39, 273–292. [Google Scholar] [CrossRef]
- Kato, C.N.; Barra, S.G.; Tavares, N.P.; Amaral, T.M.; Brasileiro, C.B.; Mesquita, A.R.; Abreu, L.G. Use of fractal analysis in dental images: A systematic review. Dentomaxillofacial Radiol. 2020, 49, 20180457. [Google Scholar] [CrossRef] [PubMed]
- Risović, D.; Pavlović, Z. Performance assessment of methods for estimation of fractal dimension from scanning electron mi-croscope images. Scanning 2013, 35, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Mahovic Poljacek, S.; Risovic, D.; Furic, K.; Gojo, M. Comparison of fractal and profilometric methods for Surface topography charakterization. Appl. Surf. Sci. 2008, 254, 3449–3458. [Google Scholar] [CrossRef]
- Schestatsky, R.; Zucuni, C.P.; Dapieve, K.S.; Burgo, T.A.L.; Spazzin, A.O.; Bacchi, A.; Valandro, L.F.; Pereira, G.K.R. Micro-structure, topography, surface roughness, fractal dimension, internal and marginal adaptation of pressed and milled lithium-disilicate monolithic restorations. J. Prosthodont. Res. 2020, 64, 12–19. [Google Scholar] [CrossRef]
- Jodha, K.S.; Marocho, S.M.S.; Scherrer, S.S.; Griggs, J.A. Fractal analysis at varying locations of clinically failed zirconia dental implants. Dent. Mater. 2020, 36, 1052–1058. [Google Scholar] [CrossRef] [PubMed]
- Salerno, M.; Giacomelli, L.; Derchi, G.; Patra, N.; Diaspro, A. Atomic force microscopy in vitro study of surface roughness and fractal character of a dental restoration composite after air-polishing. Biomed. Eng. Online 2010, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ISO. ISO 10993-5: Biological Evaluation of Medical Devices—Part 3: Tests for Genotoxicity, Carcino-genicity and Reproductive Toxicity; ISO: Geneva, Switzerland, 2003. [Google Scholar]
- Machałowski, T.; Rusak, A.; Wiatrak, B.; Haczkiewicz-Leśniak, K.; Popiel, A.; Jaroszewicz, J.; Żak, A.; Podhorska-Okołów, M.; Jesionowski, T. Naturally Formed Chitinous Skeleton Isolated from the Marine Demosponge Aplysina fistularis as a 3D Scaffold for Tissue Engineering. Materials 2021, 14, 2992. [Google Scholar] [CrossRef]
- Tomanik, M.; Kobielarz, M.; Filipiak, J.; Szymonowicz, M.; Rusak, A.; Mroczkowska, K.; Antończak, A.; Pezowicz, C. Laser Texturing as a Way of Influencing the Micromechanical and Biological Properties of the Poly(L-Lactide) Surface. Materials 2020, 13, 3786. [Google Scholar] [CrossRef] [PubMed]
- Szymonowicz, M.; Korczynski, M.; Dobrzynski, M.; Szyszka, K.; Mikulewicz, M.; Karuga-Kuzniewska, E.; Zywickab, B.; Rybak, Z.; Wiglusz, R.J.; Zywicka, B. Cytotoxicity Evaluation of High-Temperature Annealed Nanohydroxyapatite in Contact with Fibroblast Cells. Materials 2017, 10, 590. [Google Scholar] [CrossRef] [Green Version]
- Haralick, R.M. Statistical and structural approaches to texture. Proc. IEEE 1979, 67, 786–804. [Google Scholar] [CrossRef]
- Materka, A.; Strzelecki, M. Texture Analysis Methods—A Review, COST B11 Report (presented and distributed at MC meeting and workshop in Brussels, June 1998); Technical University of Lodz: Lods, Poland, 1998. [Google Scholar]
- Kozakiewicz, M.; Wach, T. New Oral Surgery Materials for Bone Reconstruction—A Comparison of Five Bone Substitute Materials for Dentoalveolar Augmentation. Materials 2020, 13, 2935. [Google Scholar] [CrossRef] [PubMed]
- Kozakiewicz, M.; Szymor, P.; Wach, T. Influence of General Mineral Condition on Collagen-Guided Alveolar Crest Aug-mentation. Materials 2020, 13, 3649. [Google Scholar] [CrossRef] [PubMed]
- Kilic, D.; Kesim, S.; Liman, N.; Sumer, Z.; Ozturk, A. In VitroComparison of the Effects of Dental Filling Materials on Mouse Fibroblasts. Biotechnol. Biotechnol. Equip. 2012, 26, 3155–3162. [Google Scholar] [CrossRef]
- Costa, C.A.D.S.; Hebling, J.; Garcia-Godoy, F.; Hanks, C.T. In vitro cytotoxicity of five glass-ionomer cements. Biomaterials 2003, 24, 3853–3858. [Google Scholar] [CrossRef]
- Lang, O.; Kohidai, L.; Kohidai, Z.; Dobo-Nagy, C.; Csomo, K.B.; Lajko, M.; Mozes, M.; Keki, S.; Deak, G.; Tian, K.V.; et al. Cell physiological effects of glass ionomer cements on fibroblast cells. Toxicol. Vitro 2019, 61, 104627. [Google Scholar] [CrossRef]
- Milhem, M.M.; Al-Hiyasat, A.S.; Darmani, H. Toxicity Testing of Restorative Dental Materials Using Brine Shrimp Larvae (Artemia salina). J. Appl. Oral Sci. 2008, 16, 297–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid-Schwap, M.; Franz, A.; König, F.; Bristela, M.; Lucas, T.; Piehslinger, E.; Watts, D.; Schedle, A. Cytotoxicity of four categories of dental cements. Dent. Mater. 2009, 25, 360–368. [Google Scholar] [CrossRef]
- Jerg, A.; Schulz, S.; Tomakidi, P.; Hellwig, E.; Polydorou, O. Modulation of gingival cell response towards dental composites. Dent. Mater. 2018, 34, 412–426. [Google Scholar] [CrossRef]
- Ţălu, Ş.; Bramowicz, M.; Kulesza, S.; Lainović, T.; Vilotić, M.; Blažić, L. Influence of the artificial saliva storage on 3-D surface texture characteristics of contemporary dental nanocomposites. J. Microsc. 2016, 264, 198–206. [Google Scholar]
- Reddy, D.S.; Kumar, R.A.; Venkatesan, S.M.; Narayan, G.S.; Duraivel, D.; Indra, R. Influence of citric acid on the surface texture of glass ionomer restorative materials. J. Conserv. Dent. 2014, 17, 436–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayek, E.; Aoun, G.; Geha, H.; Nasseh, I. Image-based Bone Density Classification Using Fractal Dimensions and Histological Analysis of Implant Recipient Site. Acta Inform. Medica. 2020, 28, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Belgin, C.A.; Serindere, G. Evaluation of trabecular bone changes in patients with periodontitis using fractal analysis: A periapical radiography study. J. Periodontol. 2019, 91, 933–937. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cement | Adhesor Carbofine (Pentron, Czech Republic) | Agatos S (Chema-Elektromet, Poland) | Breeze (Pentron Clinical, USA) | Harvard Polycarboxylat Cement (Harvard Dental, Great Britain) | Ketac Fil Plus (3M ESPE, Germany) | Riva Self Cure (SDI, Australia) |
|---|---|---|---|---|---|---|
| Mean FD | 1.593 ± 0.033 | 1.554 ± 0.019 | 1.425 ± 0.013 | 1.577 ± 0.032 | 1.590 ± 0.031 | 1.565 ± 0.038 |
| Amount of cells after 48 h | lack of cells--- (0) | few cells--- (1) | lack of cells--- (0) | few cells--- (1) | cluster of cells (3) | few cells--- (1) |
| Amount of cells after 5 days | lack of cells--- (0) | few cells--- (1) | lack of cells--- (0) | lack of cells--- (0) | cells on surface (2) | cluster of cells (3) |
| Cytotoxicity | severe--- (2) | moderate--- (1) | moderate--- (1) | moderate--- (1) | none--- (0) | none--- (0) |
| Cement | FD | |
|---|---|---|
| 1 | Adhesor Carbofine (Pentron, Czech Republic) | 1.593 ± 0.030 2,3,6 |
| 2 | Agatos S (Chema-Elektromet, Poland) | 1.554 ± 0.019 1,3,5 |
| 3 | Breeze (Pentron Clinical, USA) | 1.425 ± 0.013 1,2,4,5,6 |
| 4 | Harvard Polycarboxylat Cement (Harvard Dental, Great Britain) | 1.577 ± 0.032 3 |
| 5 | Ketac Fil Plus (3M ESPE, Germany) | 1.590 ± 0.031 2,3,6 |
| 6 | Riva Self Cure (SDI, Australia) | 1.565 ± 0.038 1,3,5 |
| Cement | Morphological Changes in Cell Culture | Cell Culture Evaluation | Cytotoxicity |
|---|---|---|---|
| Agatos S (Chema-Elektromet, Poland) | cells degeneration and lysis observed under the sample and in zone up to 1 cm around the sample | 3 | moderate |
| Harvard Polycarboxylat Cement (Harvard Dental, Great Britain) | cells degeneration and lysis observed under the sample and in zone up to 1 cm around the sample | 3 | moderate |
| Breeze (Pentron Clinical, USA) | cells degeneration and lysis observed under the sample and in zone up to 1 cm around the sample | 3 | moderate |
| Riva Self Cure (SDI, Australia) | no morphological changes in cells under and around the sample | 0 | none |
| Ketac Fil Plus (3M ESPE, Germany) | no morphological changes in cells under and around the sample | 0 | none |
| Adhesor Carbofine (Pentron, Czech Republic) | cells degeneration and lysis observed under the sample and in zone around the sample and over the entire surface of the well | 4 | severe |
| Cement | TI | BI | |
|---|---|---|---|
| 1 | Adhesor Carbofine (Pentron, Czech Republic) | 2.26 ± 0.37 2,3,4 | 0.97 ± 0.18 2,3,4,6 |
| 2 | Agatos S (Chema-Elektromet, Poland) | 1.57 ± 0.24 1,4,5,6 | 0.64 ± 0.10 1,4,5,6 |
| 3 | Breeze (Pentron Clinical, USA) | 1.41 ± 0.10 1,4,5,6 | 0.56 ± 0.04 1,4,5,6 |
| 4 | Harvard Polycarboxylat Cement (Harvard Dental, Great Britain) | 2.00 ± 0.19 1,2,3,5 | 0.83 ± 0.09 1,2,3,5 |
| 5 | Ketac Fil Plus (3M ESPE, Germany) | 2.40 ± 0.15 2,3,4,6 | 0.99 ± 0.09 2,3,4,6 |
| 6 | Riva Self Cure (SDI, Australia) | 2.10 ± 0.41 2,3,5 | 0.87 ± 0.19 1,2,3,5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skośkiewicz-Malinowska, K.; Mysior, M.; Rusak, A.; Kuropka, P.; Kozakiewicz, M.; Jurczyszyn, K. Application of Texture and Fractal Dimension Analysis to Evaluate Subgingival Cement Surfaces in Terms of Biocompatibility. Materials 2021, 14, 5857. https://doi.org/10.3390/ma14195857
Skośkiewicz-Malinowska K, Mysior M, Rusak A, Kuropka P, Kozakiewicz M, Jurczyszyn K. Application of Texture and Fractal Dimension Analysis to Evaluate Subgingival Cement Surfaces in Terms of Biocompatibility. Materials. 2021; 14(19):5857. https://doi.org/10.3390/ma14195857
Chicago/Turabian StyleSkośkiewicz-Malinowska, Katarzyna, Martyna Mysior, Agnieszka Rusak, Piotr Kuropka, Marcin Kozakiewicz, and Kamil Jurczyszyn. 2021. "Application of Texture and Fractal Dimension Analysis to Evaluate Subgingival Cement Surfaces in Terms of Biocompatibility" Materials 14, no. 19: 5857. https://doi.org/10.3390/ma14195857