
Implants Survival Rate in Regenerated Sites with Innovative Graft Biomaterials: 1 Year Follow-Up

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
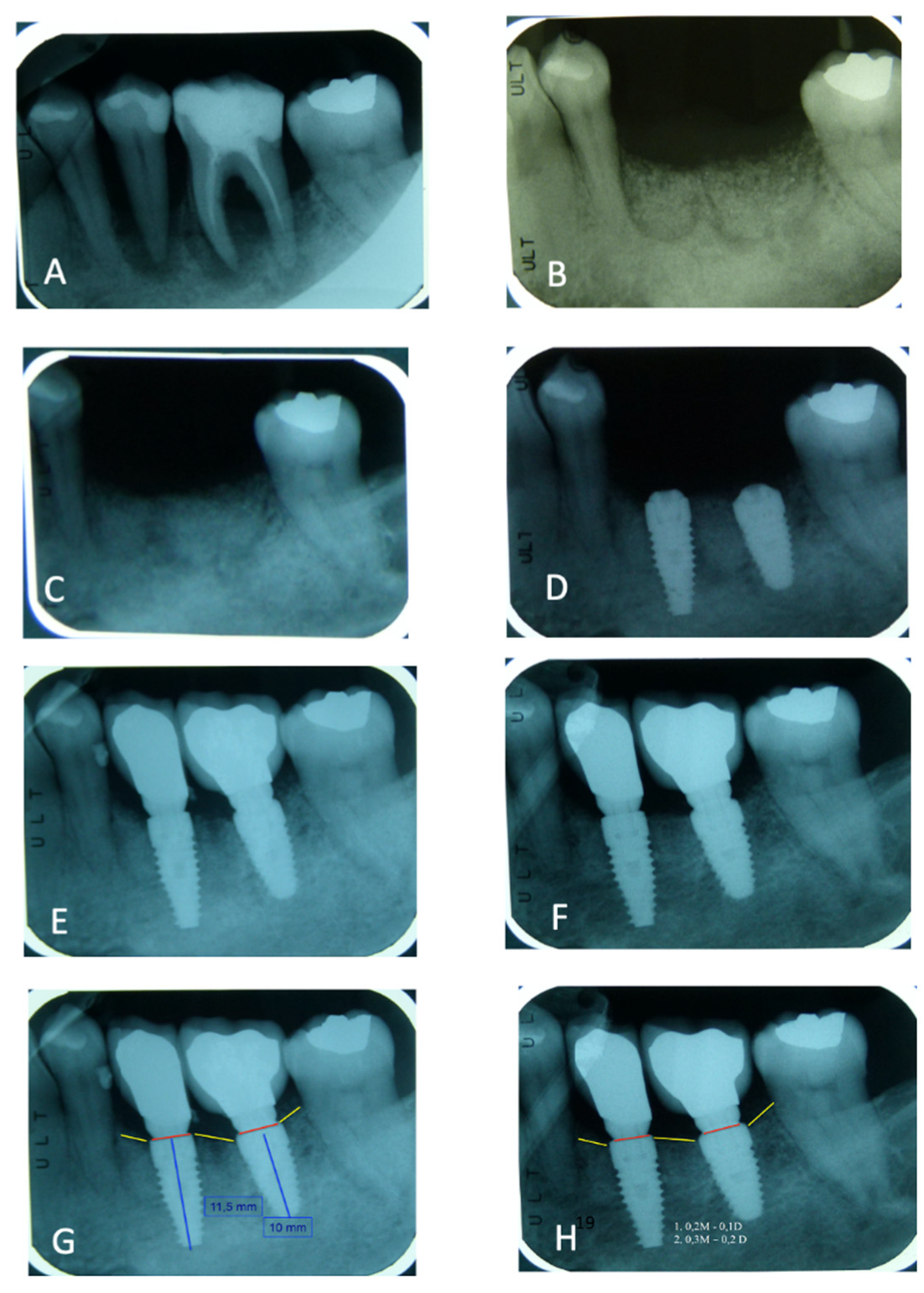
2.2. Surgical Procedures and Follow-Up
2.3. Histological Technique
2.4. Complications
2.5. Patient’s Satisfaction
2.6. Failure
3. Results
3.1. Peri-Implant Bone Loss Evaluation
3.2. Asp Implant Failure and Complications
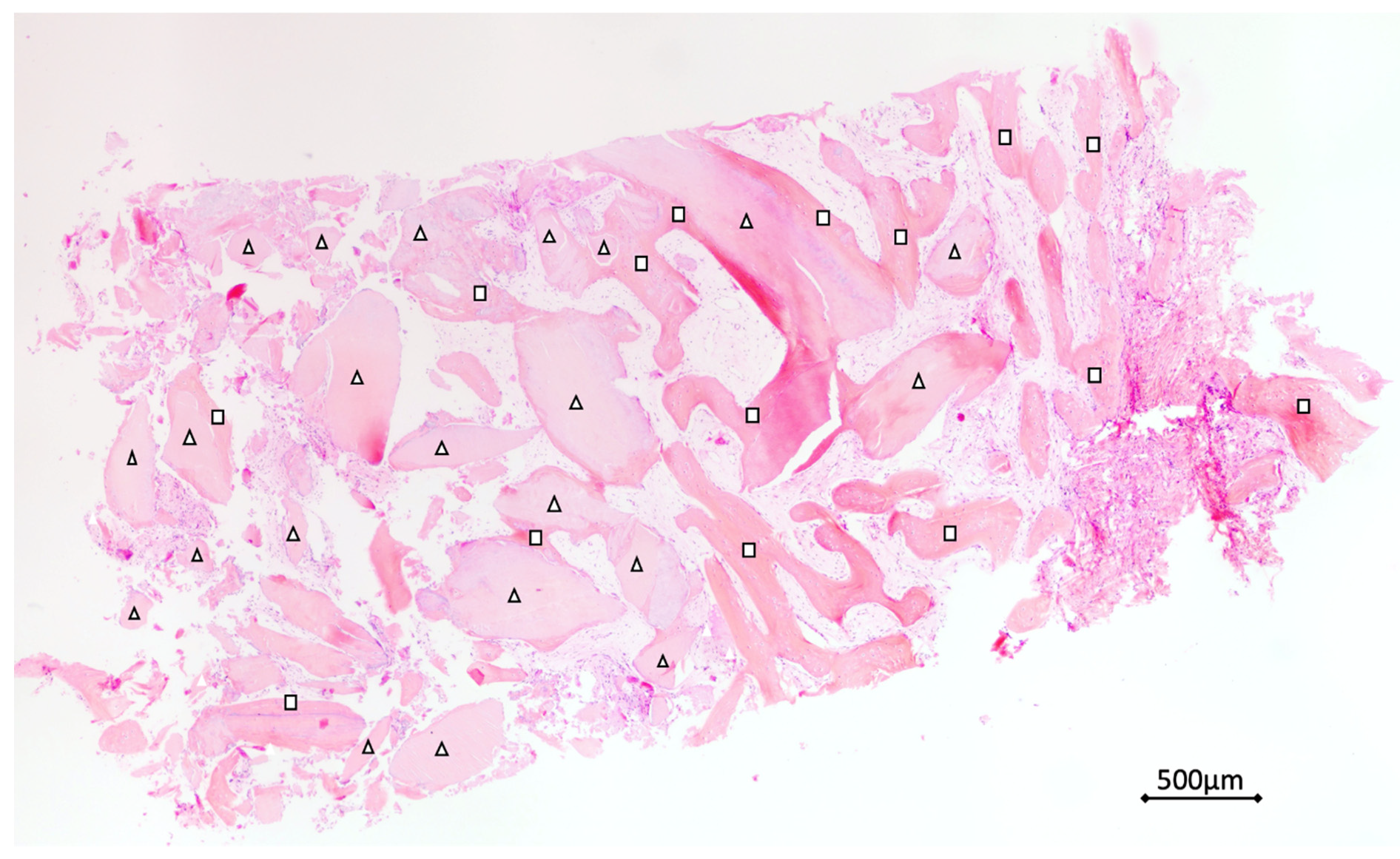
3.3. Histological Analysis
3.4. Peri-Implant Bone Loss
3.5. Patient’s Satisfaction Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Emami, E.; de Souza, R.F.; Kabawat, M.; Feine, J.S. The Impact of Edentulism on Oral and General Health. Int. J. Dent. 2013, 2013, 498305. [Google Scholar] [CrossRef]
- Hong, D.G.K.; Oh, J.H. Recent advances in dental implants. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 33. [Google Scholar] [CrossRef] [Green Version]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implantsupported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implant. Res. 2012, 23, 22–38. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Timing of implant placement after tooth extraction: Immediate, immediatedelayed or delayed implants? A Cochrane systematic review. Eur. J. Oral Implantol. 2010, 3, 189–205. [Google Scholar]
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3, 1758736012456543. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Pun, L.; Lau, K.Y.; Wong, M.C. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin. Oral Implant. Res. 2012, 23, 39–66. [Google Scholar] [CrossRef]
- Albrektsson, T.; Donos, N.; Working, G. Implant survival and complications: The Third EAO consensus conference 2012. Clin. Implant. Res. 2012, 23, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Schropp, L.; Wenzel, A. Timing of single implant placement and long-term observation of marginal bone levels. Eur. J Oral Implantol. 2016, 9, S107–S122. [Google Scholar] [PubMed]
- Araújo, M.G.; Lindhe, J. Ridge alterations following tooth extraction with and without flap elevation: An experimental study in the dog. Clin. Oral Implant. Res. 2009, 20, 545–549. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Polizzi, E.M.; Gherlone, E.F. Tissue remodeling after bone expansion in grafted and ungrafted sockets. Int. J. Oral Maxillofac. Implant. 2014, 29, 699–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chappuis, V.; Araújo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontol. 2000 2017, 73, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wei, Y.; Xu, T.; Zhang, B.; Hu, W.; Chung, K.H. Changes in alveolar process dimensions following extraction of molars with advanced periodontal disease: A clinical pilot study. Clin. Oral Implant. Res. 2019, 30, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Bittner, N.; Planzos, L.; Volchonok, A.; Tarnow, D.; Schulze-Späte, U. Evaluation of Horizontal and Vertical Buccal Ridge Dimensional Changes After Immediate Implant Placement and Immediate Temporization with and without Bone Augmentation Procedures: Short-Term, 1-Year Results. A Randomized Controlled Clinical Trial. Int. J. Periodontics Restor. Dent. 2020, 40, 83–93. [Google Scholar] [CrossRef]
- Borges, T.; Fernandes, D.; Almeida, B.; Pereira, M.; Martins, D.; Azevedo, L.; Marques, T. Correlation between alveolar bone morphology and volumetric dimensional changes in immediate maxillary implant placement: A 1-year prospective cohort study. J. Periodontol. 2020, 91, 1167–1176. [Google Scholar] [CrossRef]
- Bauer, T.W.; Muschler, C.F. Bone graft materials: An overview of the basic science. Clin. Orthop. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Von Arx, T.; Hardt, N.; Walkmann, B. The time technique:a new technique for localized alveolar ridge augmentation prior to placement of dental implants. Int. J. Oral Maxillofac. Implant. 1996, 11, 387–394. [Google Scholar]
- Tomasi, C.; Donati, M.; Cecchinato, D.; Szathvary, I.; Corrà, E.; Lindhe, J. Effect of socket grafting with deproteinized bone mineral: An RCT on dimensional alterations after 6 months. Clin. Oral Implant. Res. 2018, 29, 435–442. [Google Scholar] [CrossRef]
- Mastrangelo, F.; Quaresima, R.; Grilli, A.; Tettamanti, L.; Vinci, R.; Sammartino, G.; Tetè, S.; Gherlone, E. A comparison of bovine bone and hydroxyapatite scaffolds during initial bone regeneration: An in vitro evaluation. Implant. Dent. 2013, 22, 613–622. [Google Scholar] [CrossRef]
- Di Raimondo, R.; Sanz-Esporrín, J.; Sanz-Martin, I.; Plá, R.; Luengo, F.; Vignoletti, F.; Nuñez, J.; Sanz, M. Hard and soft tissue changes after guided bone regeneration using two different barrier membranes: An experimental in vivo investigation. Clin. Oral Investig. 2021, 25, 2213–2227. [Google Scholar] [CrossRef]
- Manavella, V.; Romano, F.; Corano, L.; Bignardi, C.; Aimetti, M. Three-Dimensional Volumetric Changes in Severely Resorbed Alveolar Sockets after Ridge Augmentation with Bovine-Derived Xenograft and Resorbable Barrier: A Preliminary Study on CBCT Imaging. Int. J. Oral Maxillofac. Implant. 2018, 33, 373–382. [Google Scholar] [CrossRef]
- Mastrangelo, F.; Gastaldi, G.; Vinci, R.; Troiano, G.; Tettamanti, L.; Gherlone, E.; Lo Muzio, L. Immediate Postextractive Implants With and Without Bone Graft: 3-year Follow-up Results From a Multicenter Controlled Randomized Trial. Implant. Dent. 2018, 27, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Botilde, G.; Colin, P.E.; González-Martín, O.; Lecloux, G.; Rompen, E.; Lambert, F. Hard and soft tissue analysis of alveolar ridge preservation in esthetic zone using deproteinized bovine bone mineral and a saddle connective tissue graft: A long-term prospective case series. Clin. Implant. Dent. Relat. Res. 2020, 22, 387–396. [Google Scholar] [CrossRef]
- Zizzari, V.L.; Zara, S.; Tetè, G.; Vinci, R.; Gherlone, E.; Cataldi, A. Biologic and clinical aspects of integration of different bone substitutes in oral surgery: A literature review. Oral Surg. Orla Med. Pathol. Oral Radiol. 2016, 122, 392–402. [Google Scholar] [CrossRef]
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implant. Res. 2012, 23, 2–21. [Google Scholar] [CrossRef]
- Compton, S.M.; Clark, D.; Chan, S.; Kuc, I.; Wubie, B.A.; Levin, L. Dental implants in the elderly population: A long term follow-up. Int. J. Oral Maxillofac. Implant. 2017, 32, 164–170. [Google Scholar] [CrossRef]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef]
- Nassani, M.Z. What is the survival rate of dental implants placed at sites of failed implants? Evid. Based Dent. 2019, 20, 95–96. [Google Scholar] [CrossRef]
- Alghamdi, H.S.; Jansen, J.A. The development and future of dental implants. Dent. Mater. J. 2020, 39, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.L.; Shiau, H.J.; Reynolds, M.A. Survival of dental implants at sites after implant failure: A systematic review. J. Prosthet. Dent. 2020, 123, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manz, M. Factors Associated With Radiographic Vertical Bone Loss Around Implants Placed in a Clinical Study. Ann. Periodontol. 2000, 5, 137–151. [Google Scholar] [CrossRef]
- Apostolopoulos, P.; Darby, I. Retrospective success and survival rates of dental implants placed after a ridge preservation procedure. Clin. Oral Implant. Res. 2016, 26, 461–468. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Deflorian, M.; Testori, T.; Mandelli, F.; Nagursky, H.; Vinci, R. Alveolar socket preservation with demineralised bovine bone mineral and a collagen matrix. J. Periodontal Implant. Sci. 2017, 47, 194–210. [Google Scholar] [CrossRef] [Green Version]
- Crespi, R.; Toti, P.; Covani, U.; Crespi, G.; Brevi, B.; Menchini, G.B. fabris Bone assessment in grafted and ungrafted pocket after dental implant placement: A 10 year follow up study. Int. J. Oral Maxillofac. Implant. 2020, 35, 576–584. [Google Scholar] [CrossRef]
- Minetti, E.; Palermo, A.; Contessi, M.; Gambardella, U.; Schmitz, J.H.; Giacometti, E.; Celko, M.; Trisi, P. Autologous tooth graft for maxillary sinus augmentation: A multicenter clinical study. Int. J. Growth Factors Stem. Cells Dent. 2019, 2, 45–51. [Google Scholar] [CrossRef]
- Minetti, E.; Berardini, M.; Trisi, P. A new tooth processing apparatous allowing to obtain dentin grafts for bone augmentation: The tooth transformer. Open Dent. J. 2019, 13, 6–14. [Google Scholar] [CrossRef]
- Minetti, E.; Palermo, A.; Ferrante, F.; Schmitz, J.; Ho, H.K.H.; Haan SNg, D.; Giacometti, E.; Gambardella, U.; Contessi, M.; Celko, M.; et al. Autologous tooth graft after endodontical treated used for socket preservation: A multicenter clinical study. Appl. Sci. 2019, 9, 5396. [Google Scholar] [CrossRef] [Green Version]
- Minetti, E.; Giacometti, E.; Gambardella, U.; Contessi, M.; Celko, M.; Marenzi, G.; Mastrangelo, F. Alevolar socket preservation with different autologous graft materials: Preliminary results of a multicenter pilot study in human. Materials 2020, 13, 1153. [Google Scholar] [CrossRef] [Green Version]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minetti, E.; Casasco, A.; Casasco, M.; Corbella, S.; Giacometti, E.; Ho, H.K.L.; Palermo, A.; Savadori, P.; Taschieri, S. Bone Regeneration in Implantology: Tooth as a Graft, 2021 EDRA ed.; Edra Publishing US: Palm Beach Gardens, FL, USA; ISBN 978-88-214-5353-3.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
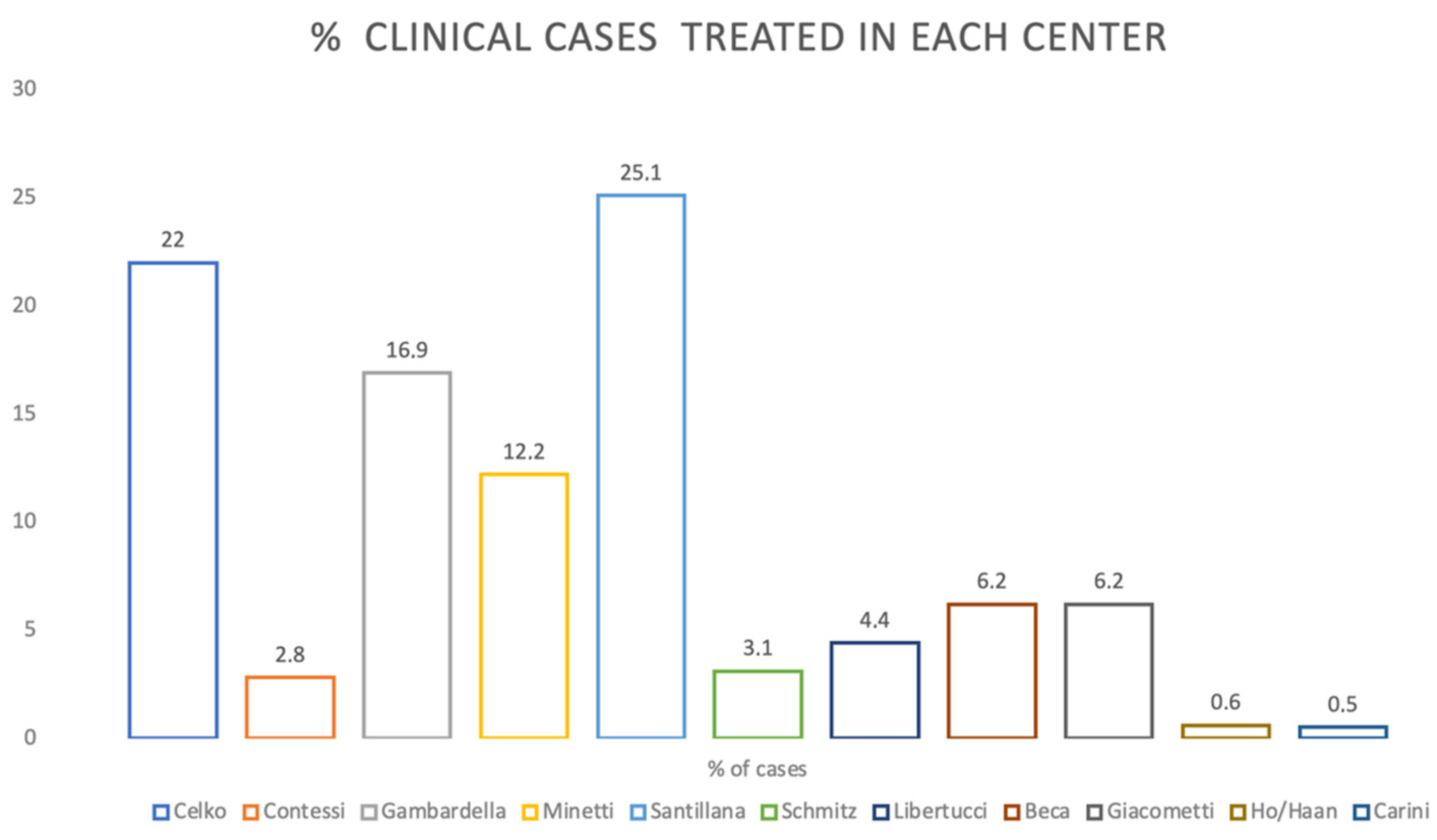
| Dental Clinic Surgeons | 13 |
| Sample Size | 504 (269 Female–235 Male) |
| Average Age | 54.09 (Range 22–85) |
| Total Extracted Teeth Incisive Canine Premolars Molars | 524 Incisive 104 Canine 42 Premolars 184 Molars 194 |
| Extraction Reasons | Crown Trauma Eternal Root Resorption Periodontitis Root Fracture Infected Root |
| Total Socket Sites Treated | 483 (Maxilla 278–Mandible 205) |
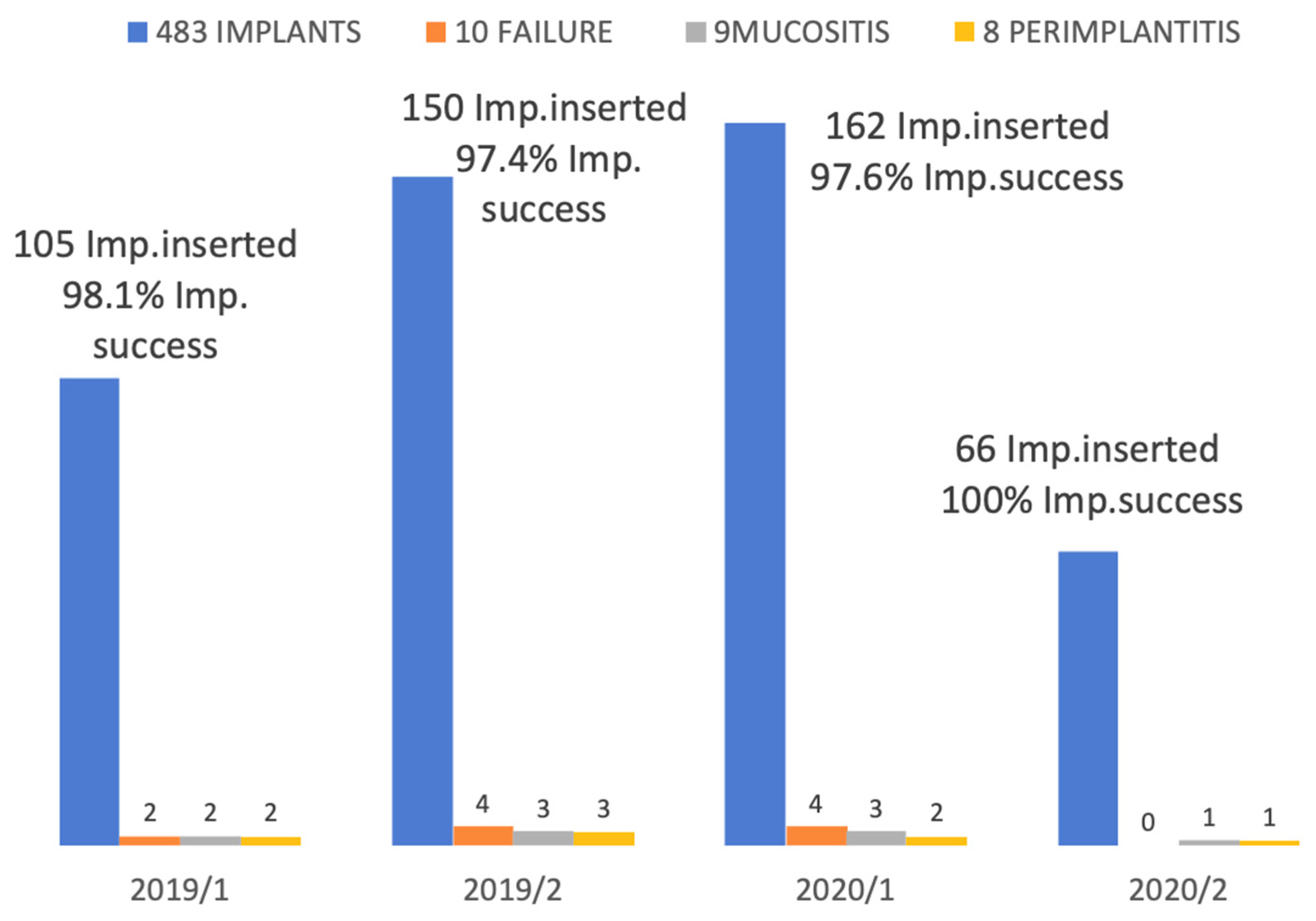
| Dental Implants | 483 |
| Average Implant Length | 10.83mm (±1.17) |
| IMPLANT FAILURE |  | |
| Site where the implants were failed | 23–12-14–25–25–21-26–46–34–36 | |
| Implant failure rate | 1.75% | |
| Number of failed implants for each dimensions | N°2 (4 × 8.5 mm) N°1 (4 × 10 mm) N°1 (5 × 13 mm) N°2 (4 × 11 mm) N°1 (3.75 × 10 mm) N°2 (4.1 × 12.5 mm) N°1 (6 × 11 mm) | |
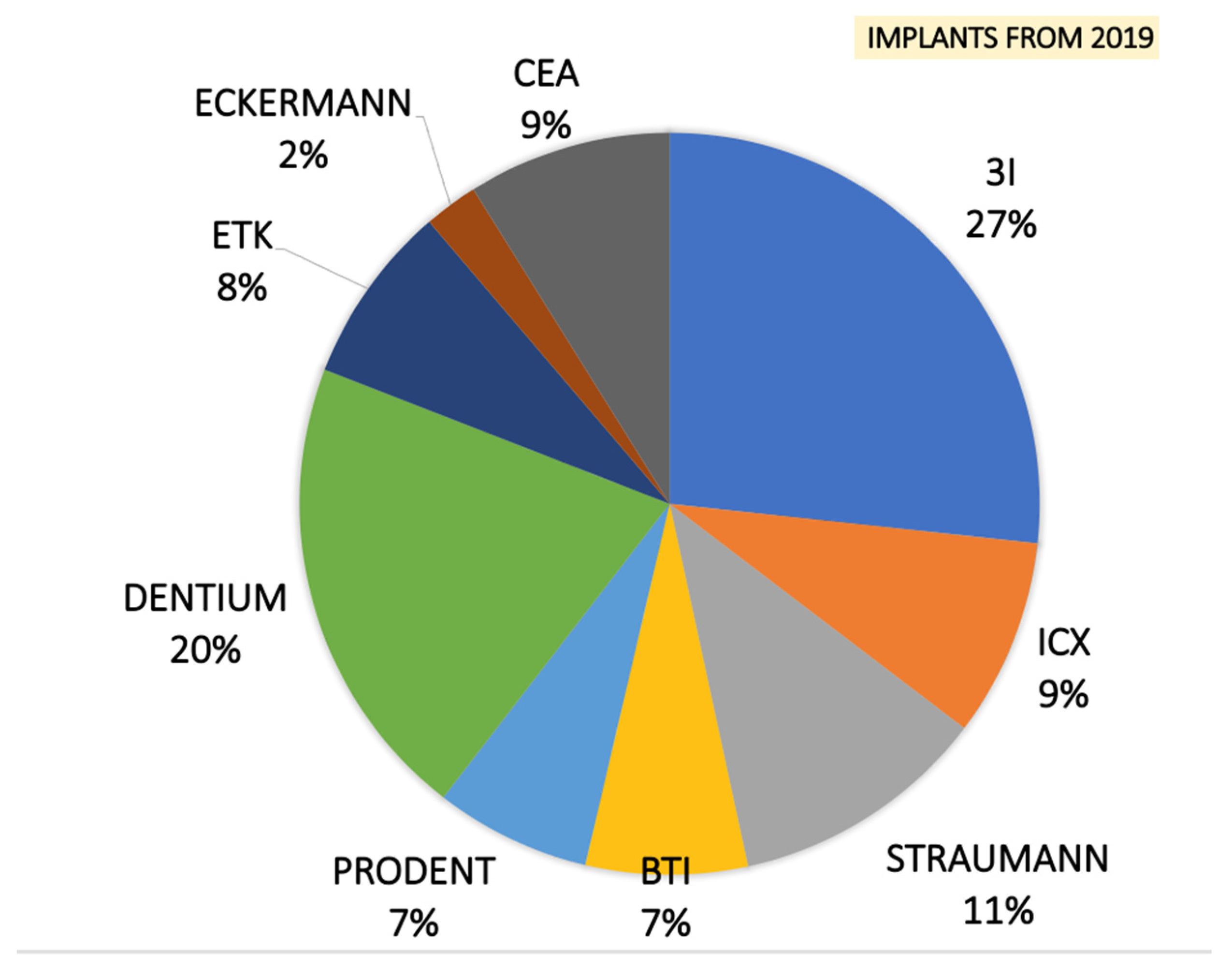
| Number of implants lost for each producer | N°7 3I N°3 ICX | |
| PATIENT SATISFACTION SCORE | |||
|---|---|---|---|
| YES | YES/NO | NO | |
| Satisfaction to use tooth as graft | 90% | 10% | |
| Morbidity | 5.5% | 15% | 79.5% |
| Swelling | 10% | 12% | 78% |
| Would you do it again? | 88% | 12% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minetti, E.; Celko, M.; Contessi, M.; Carini, F.; Gambardella, U.; Giacometti, E.; Santillana, J.; Beca Campoy, T.; Schmitz, J.H.; Libertucci, M.; et al. Implants Survival Rate in Regenerated Sites with Innovative Graft Biomaterials: 1 Year Follow-Up. Materials 2021, 14, 5292. https://doi.org/10.3390/ma14185292
Minetti E, Celko M, Contessi M, Carini F, Gambardella U, Giacometti E, Santillana J, Beca Campoy T, Schmitz JH, Libertucci M, et al. Implants Survival Rate in Regenerated Sites with Innovative Graft Biomaterials: 1 Year Follow-Up. Materials. 2021; 14(18):5292. https://doi.org/10.3390/ma14185292
Chicago/Turabian StyleMinetti, Elio, Martin Celko, Marcello Contessi, Fabrizio Carini, Ugo Gambardella, Edoardo Giacometti, Jesus Santillana, Tomas Beca Campoy, Johannes H. Schmitz, Mauro Libertucci, and et al. 2021. "Implants Survival Rate in Regenerated Sites with Innovative Graft Biomaterials: 1 Year Follow-Up" Materials 14, no. 18: 5292. https://doi.org/10.3390/ma14185292