
Effects of Gamma Radiation-Induced Crosslinking of Collagen Type I Coated Dental Titanium Implants on Osseointegration and Bone Regeneration

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Materials
2.2. In Vitro Study
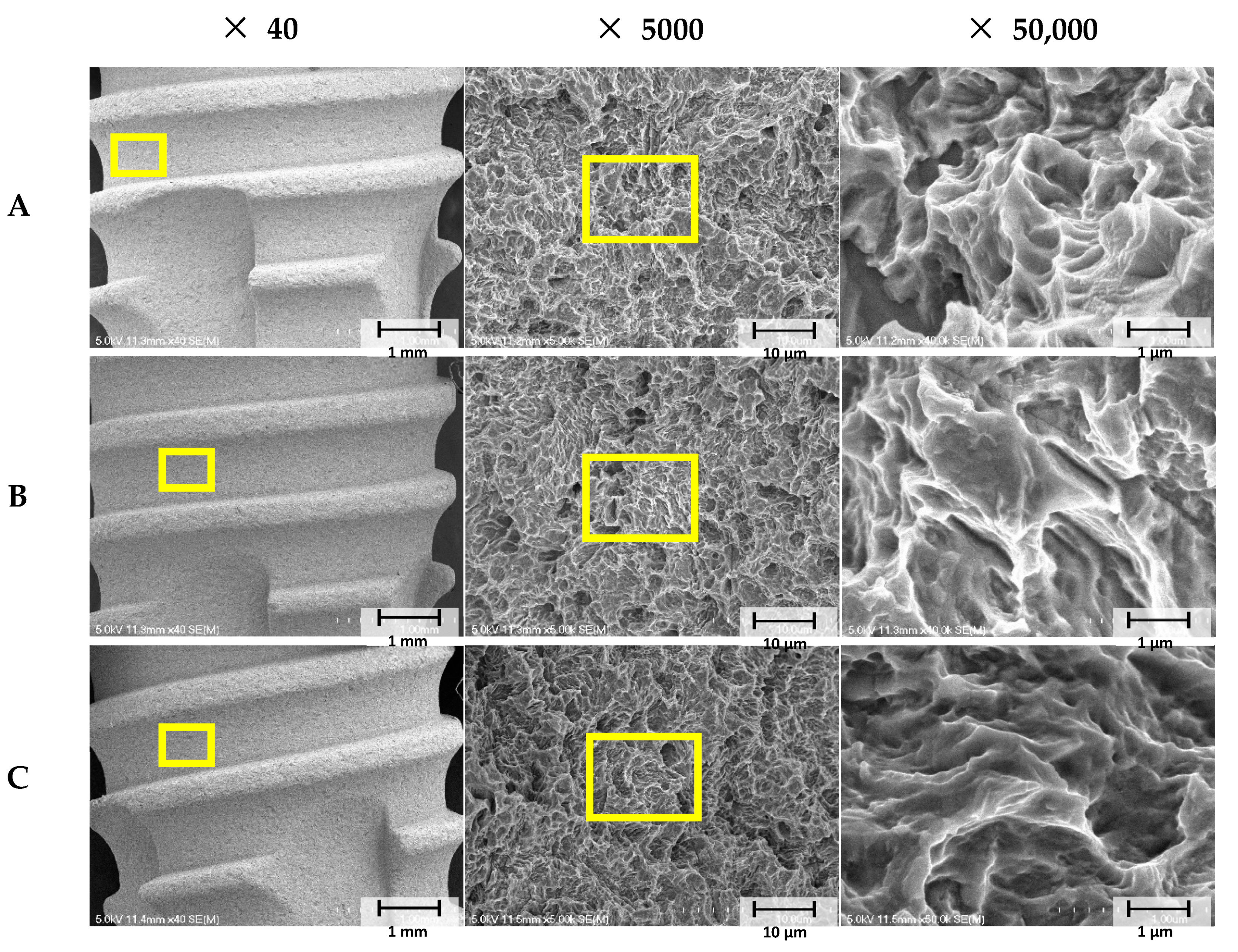
2.2.1. Scanning Electron Microscopy (SEM) Analysis
2.2.2. X-ray Photoelectron Spectroscopy (XPS)
2.3. In Vivo Experiment
2.3.1. Experimental Animals
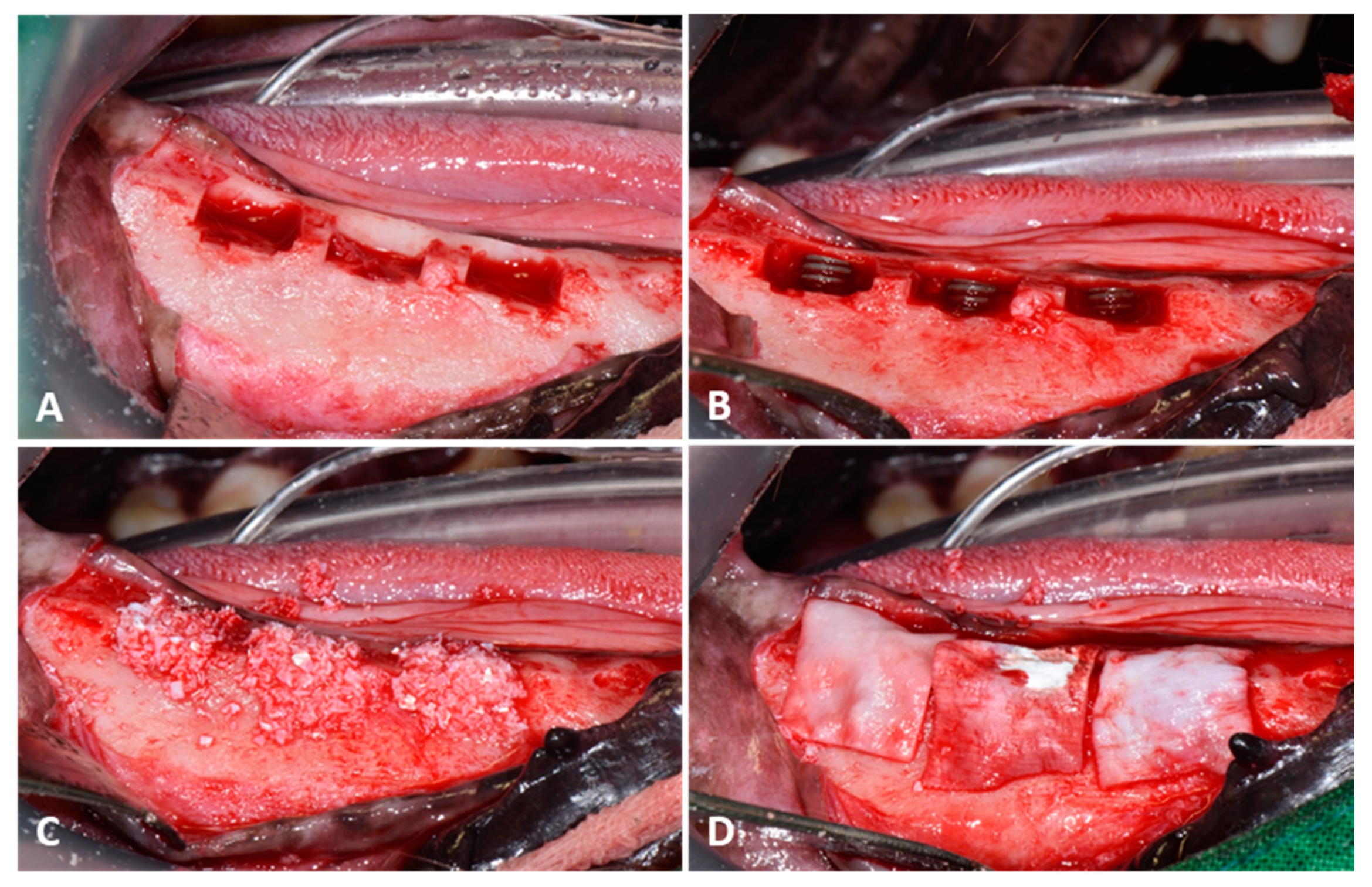
2.3.2. Surgical Procedure
- -
- Group SLA (n = 12): Non-treated SLA implants.
- -
- Group GA (n = 12): SLA implants coated with GA crosslinked collagen type I.
- -
- Group GR (n = 12): SLA implants coated with 25 kGy 60Co gamma radiation crosslinked collagen type I.
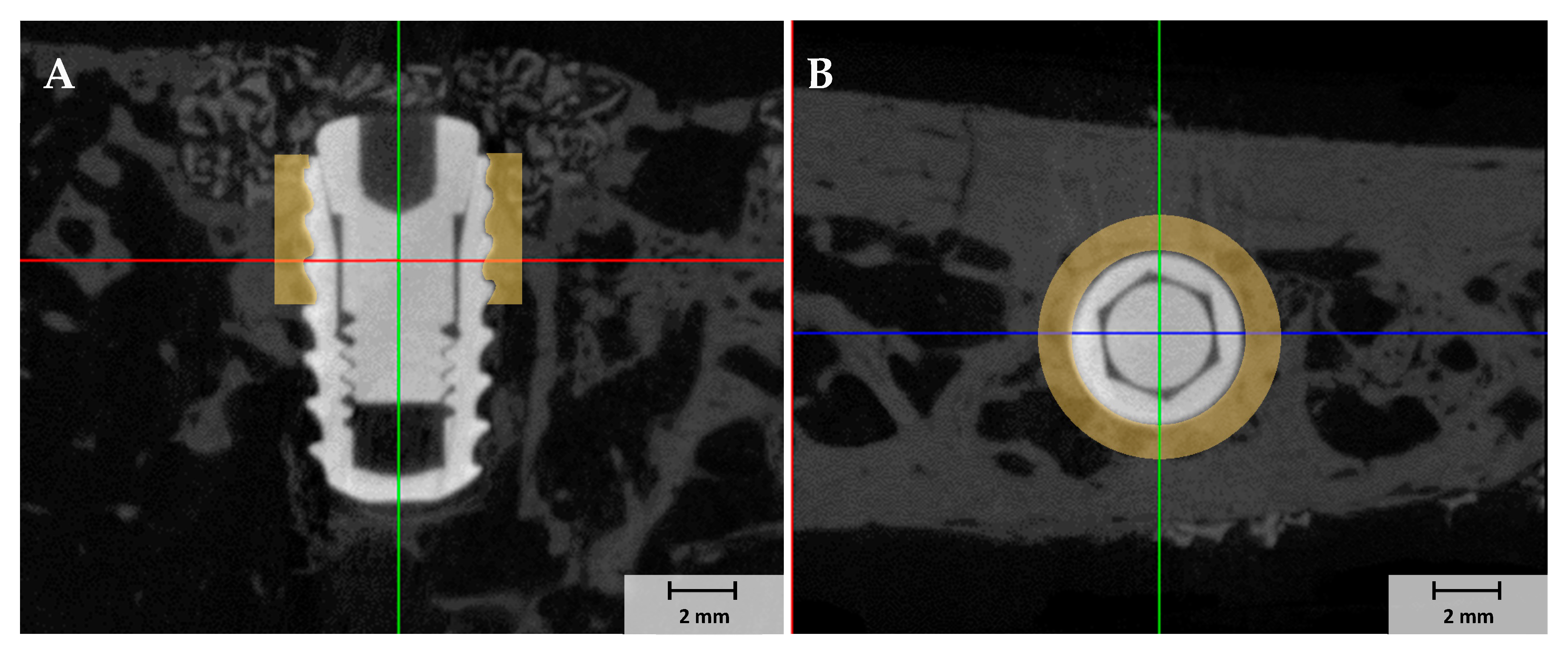
2.3.3. Micro-Computed Tomography (µCT) Analysis
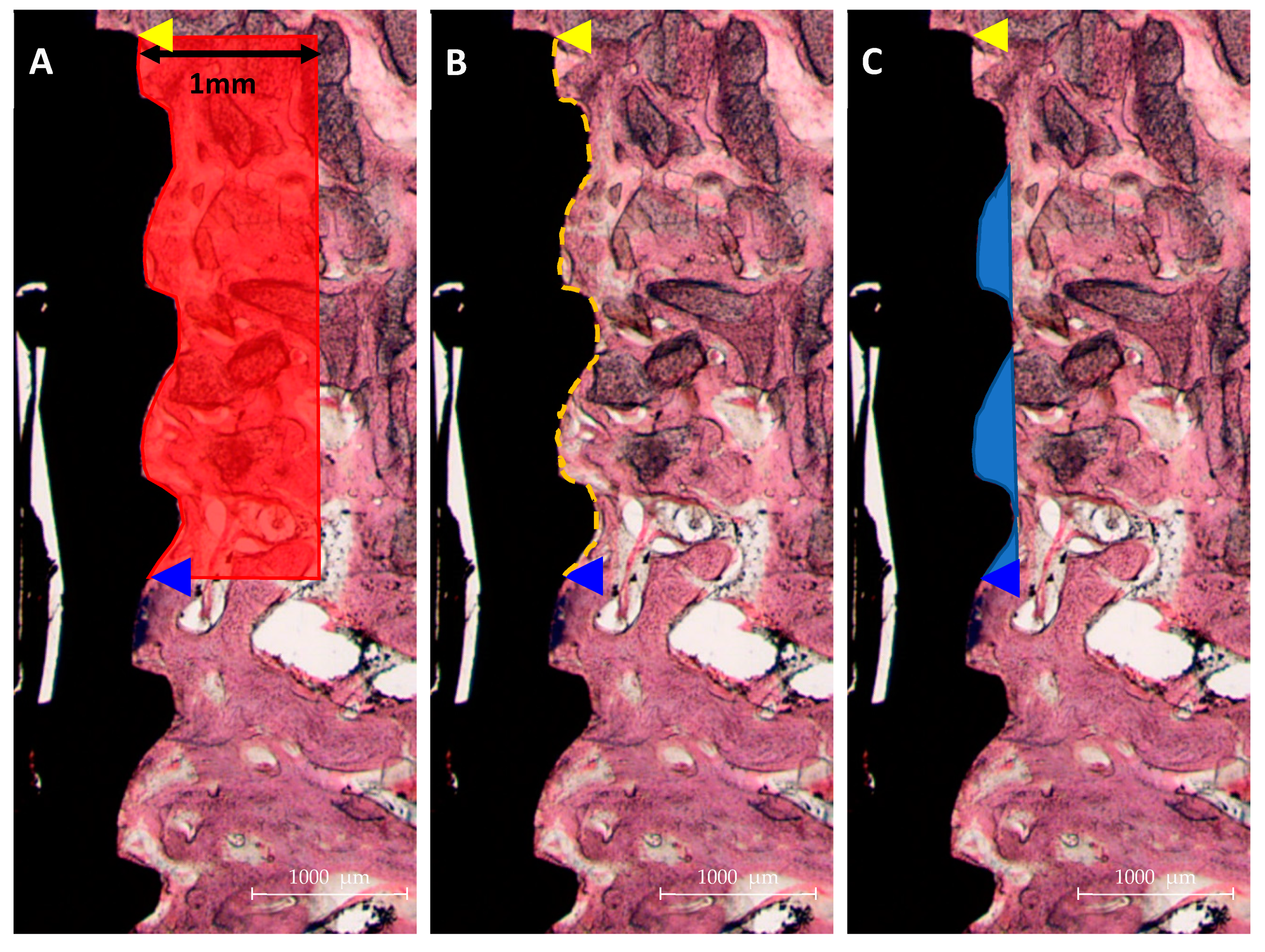
2.3.4. Histologic Analysis
2.3.5. Statistical Analysis
3. Results
3.1. In-Vitro Study
3.1.1. Collagen Crosslinked Ti Implant Surface Morphologies
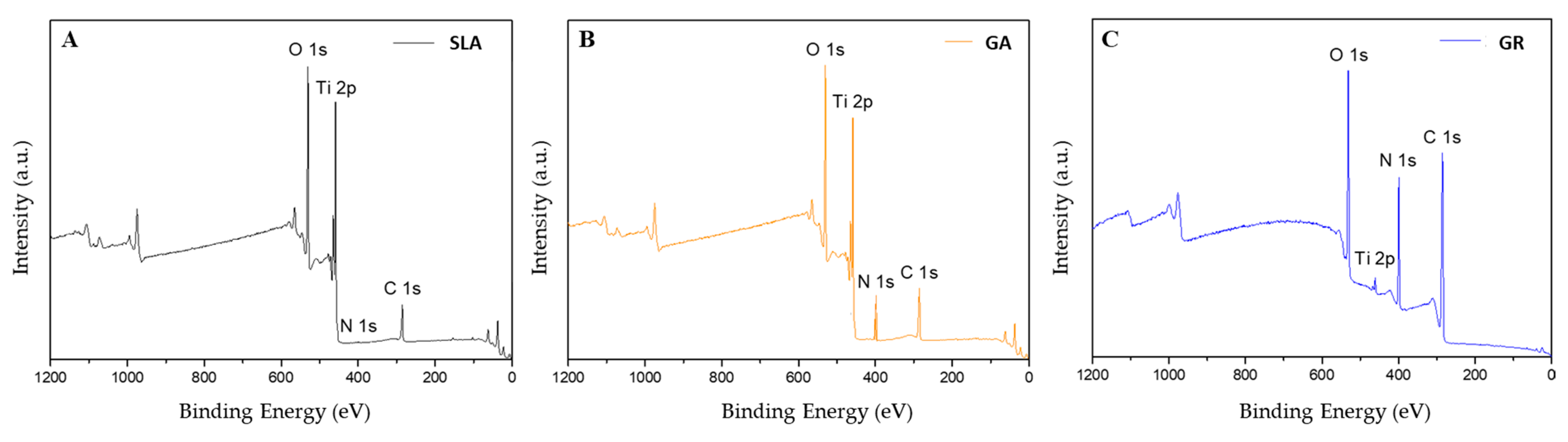
3.1.2. XPS Findings
3.2. In Vivo Study
3.2.1. Clinical Findings
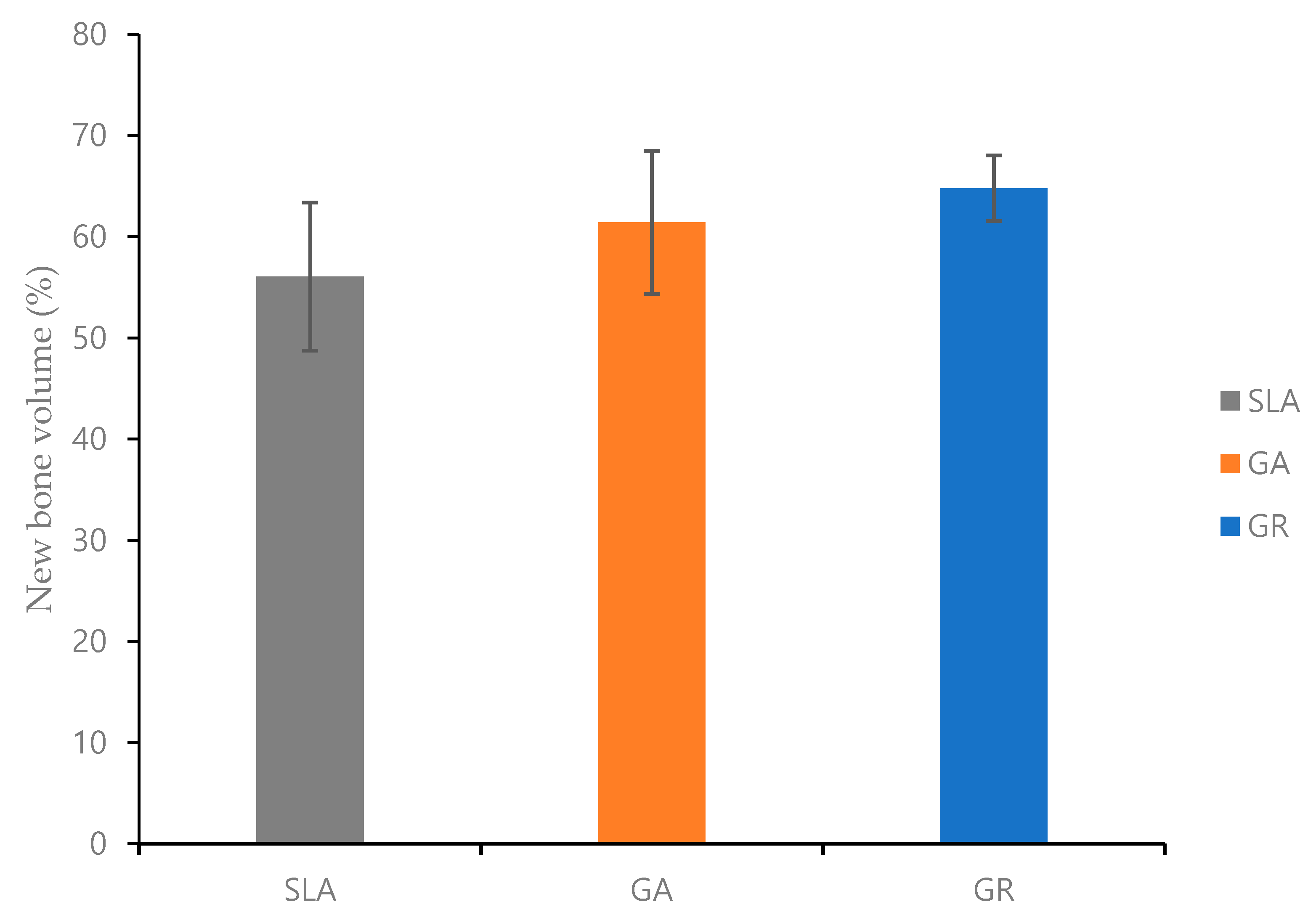
3.2.2. Micro-Computed Tomography (µCT) Findings
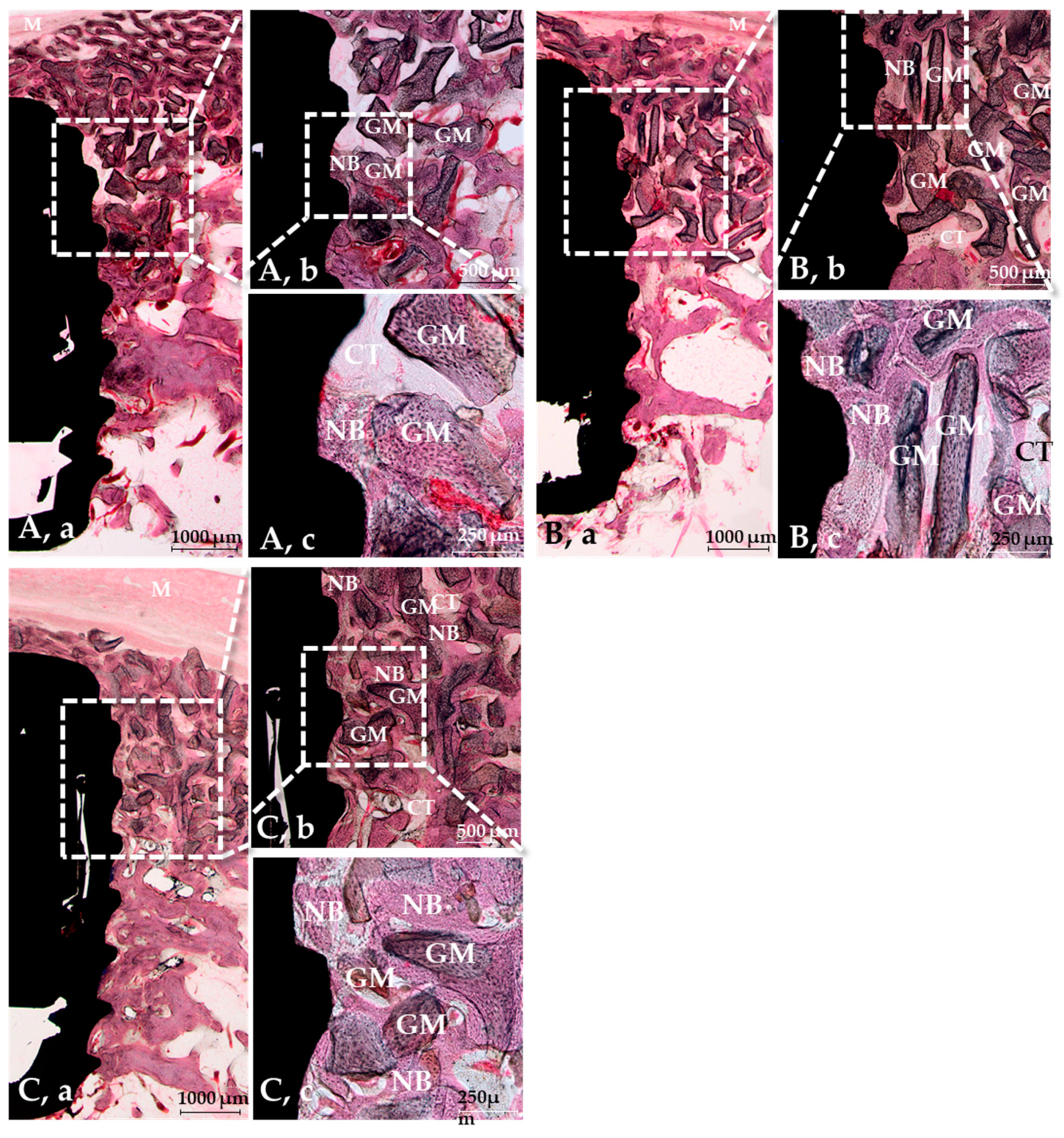
3.2.3. Histological Findings
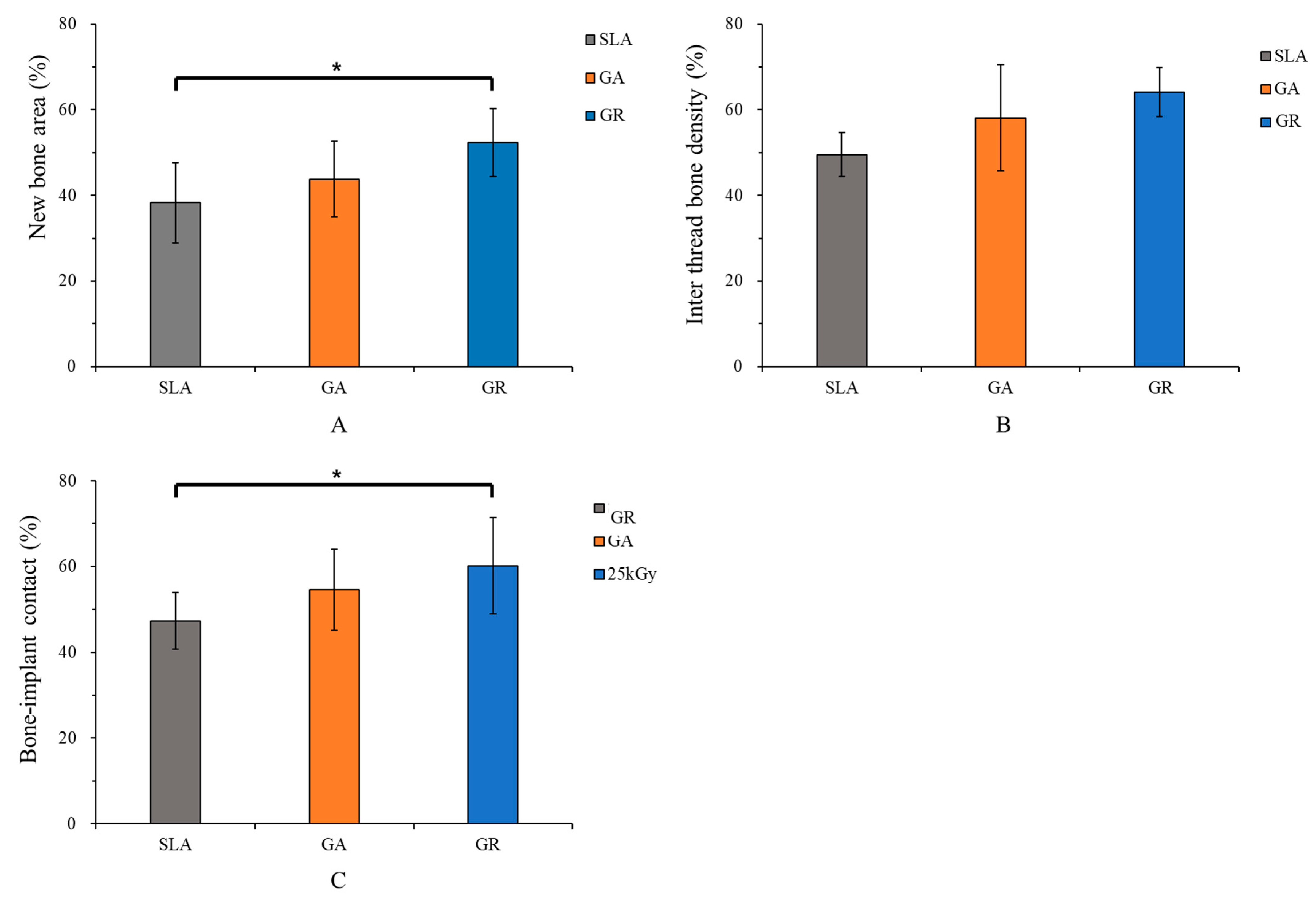
3.2.4. Histometric Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rocci, A.; Calcaterra, R.; Di Girolamo, M.; Rocci, M.; Rocci, C.; Baggi, L. The influence of micro and macro-geometry in term of bone-implant interface in two implant systems: An histomorphometrical study. Oral Implantol. 2015, 8, 87–95. [Google Scholar]
- Textor, M.; Sittig, C.; Frauchiger, V.; Tosatti, S.; Brunette, D. Properties and biological significance of natural oxide films on titanium and its alloys. In Titanium in Medicine; Springer: Berlin/Heidelberg, Germany, 2001; pp. 171–230. [Google Scholar]
- Morra, M. Biochemical modification of titanium surfaces: Peptides and ECM proteins. Eur. Cells Mater. 2006, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Le Guéhennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Müeller, W.D.; Gross, U.; Fritz, T.; Voigt, C.; Fischer, P.; Berger, G.; Rogaschewski, S.; Lange, K.P. Evaluation of the interface between bone and titanium surfaces being blasted by aluminium oxide or bioceramic particles. Clin. Oral Implants Res. 2003, 14, 349–356. [Google Scholar] [CrossRef]
- Ueno, T.; Takeuchi, M.; Hori, N.; Iwasa, F.; Minamikawa, H.; Igarashi, Y.; Anpo, M.; Ogawa, T. Gamma ray treatment enhances bioactivity and osseointegration capability of titanium. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 2279–2287. [Google Scholar] [CrossRef]
- Hwang, S.-T.; Han, I.-H.; Huh, J.-B.; Kang, J.-K.; Ryu, J.-J. Review of the developmental trend of implant surface modification using organic biomaterials. J. Korean Acad. Prosthodont. 2011, 49, 254–262. [Google Scholar] [CrossRef] [Green Version]
- Reyes, C.D.; García, A.J. Engineering integrin-specific surfaces with a triple-helical collagen-mimetic peptide. J. Biomed. Mater. Res. A 2003, 65, 511–523. [Google Scholar] [CrossRef]
- Costa, D.G.; Ferraz, E.P.; Abuna, R.P.; de Oliveira, P.T.; Morra, M.; Beloti, M.M.; Rosa, A.L. The effect of collagen coating on titanium with nanotopography on in vitro osteogenesis. J. Biomed. Mater. Res. A 2017, 105, 2783–2788. [Google Scholar] [CrossRef]
- Nagai, M.; Hayakawa, T.; Fukatsu, A.; Yamamoto, M.; Fukumoto, M.; Nagahama, F.; Mishima, H.; Yoshinari, M.; Nemoto, K.; Kato, T. In vitro study of collagen coating of titanium implants for initial cell attachment. Dent. Mater. J. 2002, 21, 250–260. [Google Scholar] [CrossRef]
- Gelse, K.; Pöschl, E.; Aigner, T. Collagens—structure, function, and biosynthesis. Adv. Drug. Deliv. Rev. 2003, 55, 1531–1546. [Google Scholar] [CrossRef] [Green Version]
- Brodsky, B.; Ramshaw, J.A. The collagen triple-helix structure. Matrix Biol. 1997, 15, 545–554. [Google Scholar] [CrossRef]
- Zhang, X.; Xu, L.; Huang, X.; Wei, S.; Zhai, M. Structural study and preliminary biological evaluation on the collagen hydrogel crosslinked by γ-irradiation. J. Biomed. Mater. Res. A 2012, 100, 2960–2969. [Google Scholar] [CrossRef]
- Damink, L.O.; Dijkstra, P.; Van Luyn, M.; Van Wachem, P.; Nieuwenhuis, P.; Feijen, J. Glutaraldehyde as a crosslinking agent for collagen-based biomaterials. J. Mater. Sci. Mater. Med. 1995, 6, 460–472. [Google Scholar] [CrossRef] [Green Version]
- De Assis, A.F.; Beloti, M.M.; Crippa, G.E.; De Oliveira, P.T.; Morra, M.; Rosa, A.L. Development of the osteoblastic phenotype in human alveolar bone-derived cells grown on a collagen type I-coated titanium surface. Clin. Oral Implants Res. 2009, 20, 240–246. [Google Scholar] [CrossRef]
- Harjula, A.; Nickels, J.; Mattila, S. Histological study of glutaraldehyde-processed vascular grafts of biological origin. Ann. Chir. Gynaecol. 1980, 69, 256–262. [Google Scholar]
- Cooke, A.; Oliver, R.; Edward, M. An in vitro cytotoxicity study of aldehyde-treated pig dermal collagen. Br. J. Exp. Pathol. 1983, 64, 172–176. [Google Scholar]
- Charulatha, V.; Rajaram, A. Influence of different crosslinking treatments on the physical properties of collagen membranes. Biomaterials 2003, 24, 759–767. [Google Scholar] [CrossRef]
- Zeugolis, D.I.; Paul, G.R.; Attenburrow, G. Cross-linking of extruded collagen fibers—A biomimetic three-dimensional scaffold for tissue engineering applications. J. Biomed. Mater. Res. A 2009, 89, 895–908. [Google Scholar] [CrossRef]
- Sionkowska, A.; Wisniewski, M.; Skopinska, J.; Poggi, G.; Marsano, E.; Maxwell, C.; Wess, T.J. Thermal and mechanical properties of UV irradiated collagen/chitosan thin films. Polym. Degrad. Stab. 2006, 91, 3026–3032. [Google Scholar] [CrossRef]
- Cataldo, F.; Ursini, O.; Lilla, E.; Angelini, G. Radiation-induced crosslinking of collagen gelatin into a stable hydrogel. J. Radioanal. Nucl. Chem. 2008, 275, 125–131. [Google Scholar] [CrossRef]
- Türker, N.S.; Özer, A.Y.; Kutlu, B.; Nohutcu, R.; Sungur, A.; Bilgili, H.; Ekizoglu, M.; Özalp, M. The effect of gamma radiation sterilization on dental biomaterials. Tissue Eng. Regen. Med. 2014, 11, 341–349. [Google Scholar] [CrossRef]
- Wach, R.A.; Mitomo, H.; Nagasawa, N.; Yoshii, F. Radiation crosslinking of methylcellulose and hydroxyethylcellulose in concentrated aqueous solutions. Nucl. Instrum. Methods B 2003, 211, 533–544. [Google Scholar] [CrossRef]
- Chen, C.-C.; Chueh, J.-Y.; Tseng, H.; Huang, H.-M.; Lee, S.-Y. Preparation and characterization of biodegradable PLA polymeric blends. Biomaterials 2003, 24, 1167–1173. [Google Scholar] [CrossRef]
- Almeida, O.M.D.; Jorgetti, W.; Oksman, D.; Jorgetti, C.; Rocha, D.L.; Gemperli, R. Comparative study and histomorphometric analysis of bone allografts lyophilized and sterilized by autoclaving, gamma irradiation and ethylene oxide in rats. Acta Cir. Bras. 2013, 28, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Azorin, E.; Gonzalez-Martinez, P.; Azorin, J. Collagen I confers gamma radiation resistance. Appl. Radiat. Isot. 2012, 71, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Schwartz, Z.; Wieland, M.; Rupp, F.; Geis-Gerstorfer, J.; Cochran, D.L.; Boyan, B. High surface energy enhances cell response to titanium substrate microstructure. J. Biomed. Mater. Res. A 2005, 74, 49–58. [Google Scholar] [CrossRef]
- Bae, E.-B.; Yoo, J.-H.; Jeong, S.-I.; Kim, M.-S.; Lim, Y.-M.; Ahn, J.-J.; Lee, J.-J.; Lee, S.-H.; Kim, H.-J.; Huh, J.-B. Effect of titanium implants coated with radiation-crosslinked collagen on stability and osseointegration in rat tibia. Materials 2018, 11, 2520. [Google Scholar] [CrossRef] [Green Version]
- Anesi, A.; Di Bartolomeo, M.; Pellacani, A.; Palumbo, C.; Chiarini, L. Bone healing evaluation following different osteotomic techniques in animal models: A suitable method for clinical insights. Appl. Sci. 2020, 10, 7165. [Google Scholar] [CrossRef]
- Chang, M.C.; Tanaka, J. XPS study for the microstructure development of hydroxyapatite–collagen nanocomposites cross-linked using glutaraldehyde. Biomaterials 2002, 23, 3879–3885. [Google Scholar] [CrossRef]
- Montes, C.C.; Pereira, F.A.; Thome, G.; Alves, E.D.M.; Acedo, R.V.; de Souza, J.R.; Melo, A.C.M.; Trevilatto, P.C. Failing factors associated with osseointegrated dental implant loss. Implant Dent. 2007, 16, 404–412. [Google Scholar] [CrossRef] [Green Version]
- Howe, M.-S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef]
- Walton, T.R. The up-to-14-year survival and complication burden of 256 TiUnite implants supporting one-piece cast abutment/metal-ceramic implant-supported single crowns. Int. J. Oral Maxillofac. Implant. 2016, 31, 1349–1358. [Google Scholar] [CrossRef] [Green Version]
- Degidi, M.; Nardi, D.; Piattelli, A. 10-year follow-up of immediately loaded implants with TiUnite porous anodized surface. Clin. Implants Dent. Relat. Res. 2012, 14, 828–838. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M. Immediate loading of implants inserted in edentulous arches using multiple mucosa-supported stereolithographic surgical templates: A 10-year prospective cohort study. Int. J. Oral Maxillofac. Surg. 2016, 45, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Fugazzotto, P.A. Success and failure rates of osseointegrated implants in function in regenerated bone for 72 to 133 months. Int. J. Oral Maxillofac. Implant. 2005, 20, 77–83. [Google Scholar]
- Goodacre, C.J.; Kan, J.Y.; Rungcharassaeng, K. Clinical complications of osseointegrated implants. J. Prosthet. Dent. 1999, 81, 537–552. [Google Scholar] [CrossRef]
- Kulkarni, M.; Mazare, A.; Schmuki, P.; Iglič, A. Biomaterial surface modification of titanium and titanium alloys for medical applications. Nanomedicine 2014, 111, 111. [Google Scholar]
- Morra, M.; Cassinelli, C.; Cascardo, G.; Cahalan, P.; Cahalan, L.; Fini, M.; Giardino, R. Surface engineering of titanium by collagen immobilization. Surface characterization and in vitro and in vivo studies. Biomaterials 2003, 24, 4639–4654. [Google Scholar] [CrossRef]
- Wu, X.; Liu, A.; Wang, W.; Ye, R. Improved mechanical properties and thermal stability of collagen fiber based film by crosslinking with casein, keratin or SPI: Effect of crosslinking process and concentrations of proteins. Int. J. Biol. Macromol. 2018, 109, 1319–1328. [Google Scholar] [CrossRef]
- Jaikumar, D.; Baskaran, B.; Vaidyanathan, V. Effect of chromium (III) gallate complex on stabilization of collagen. Int. J. Biol. Macromol. 2017, 96, 429–435. [Google Scholar] [CrossRef]
- Gu, L.; Shan, T.; Ma, Y.-x.; Tay, F.R.; Niu, L. Novel biomedical applications of crosslinked collagen. Trends Biotechnol. 2019, 37, 464–491. [Google Scholar] [CrossRef]
- Casali, D.M.; Yost, M.J.; Matthews, M.A. Eliminating glutaraldehyde from crosslinked collagen films using supercritical CO2. J. Biomed. Mater. Res. A 2018, 106, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Schliephake, H.; Aref, A.; Scharnweber, D.; Bierbaum, S.; Roessler, S.; Sewing, A. Effect of immobilized bone morphogenic protein 2 coating of titanium implants on peri-implant bone formation. Clin. Oral Implants Res. 2005, 16, 563–569. [Google Scholar] [CrossRef]
- Sartori, M.; Giavaresi, G.; Parrilli, A.; Ferrari, A.; Aldini, N.N.; Morra, M.; Cassinelli, C.; Bollati, D.; Fini, M. Collagen type I coating stimulates bone regeneration and osteointegration of titanium implants in the osteopenic rat. Int. Orthop. 2015, 39, 2041–2052. [Google Scholar] [CrossRef] [PubMed]
- Kilpadi, D.V.; Lemons, J.E.; Liu, J.; Raikar, G.N.; Weimer, J.J.; Vohra, Y. Cleaning and heat-treatment effects on unalloyed titanium implant surfaces. Int. J. Oral Maxillofac. Implant. 2000, 15, 219–230. [Google Scholar]
- Massaro, C.; Rotolo, P.; De Riccardis, F.; Milella, E.; Napoli, A.; Wieland, M.; Textor, M.; Spencer, N.; Brunette, D. Comparative investigation of the surface properties of commercial titanium dental implants. Part I: Chemical composition. J. Mater. Sci. Mater. Med. 2002, 13, 535–548. [Google Scholar] [CrossRef]
- Morra, M.; Cassinelli, C.; Bruzzone, G.; Carpi, A.; Santi, G.D.; Giardino, R.; Fini, M. Surface chemistry effects of topographic modification of titanium dental implant surfaces: 1. Surface analysis. Int. J. Oral. Maxillofac. Implant. 2003, 18, 40–45. [Google Scholar]
- Ueno, T.; Yamada, M.; Hori, N.; Suzuki, T.; Ogawa, T. Effect of ultraviolet photoactivation of titanium on osseointegration in a rat model. Int. J. Oral. Maxillofac. Implant. 2010, 25, 287–294. [Google Scholar]
- Crespi, R.; Capparè, P.; Gherlone, E. Sinus floor elevation by osteotome: Hand mallet versus electric mallet. A prospective clinical study. Int. J. Oral. Maxillofac. Implant. 2012, 27, 1144–1150. [Google Scholar]
- D’Orto, B.; Tetè, G.; Polizzi, E. Osseointegrated dental implants supporting fixed prostheses in patients affected by Sjögren’s Sindrome: A narrative review. J. Biol. Regul. Homeost. Agents 2020, 34, 89–91. [Google Scholar]
- Misch, C.E. Occlusal considerations for implant supported prostheses. In Comtemporary Implant Dentistry; Elsevier: Amsterdam, The Netherlands, 1999; pp. 609–628. [Google Scholar]
- Ciancaglini, R.; Gherlone, E.F.; Redaelli, S.; Radaelli, G. The distribution of occlusal contacts in the intercuspal position and temporomandibular disorder. J. Oral Rehabil. 2002, 29, 1082–1090. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elements | Group | ||
|---|---|---|---|
| SLA | GA | GR | |
| C | 20.5 ± 0.33 | 29.87 ± 0.25 | 64.77 ± 0.42 |
| O | 58.22 ± 0.79 | 46.64 ± 0.49 | 16.67 ± 0.09 |
| Ti | 20.96 ± 0.36 | 17.27 ± 0.27 | 0.93 ± 0.03 |
| N | 0.33 ± 0.17 | 6.22 ± 0.13 | 17.64 ± 0.30 |
| Measurement | Group | Mean ± SD | p-Value |
|---|---|---|---|
| NBA (%) | SLA | 38.27 ± 9.34 | 0.033 * |
| GA | 43.77 ± 8.81 | ||
| GR | 52.37 ± 7.93 | ||
| ITBD (%) | SLA | 49.52 ± 5.11 | 0.053 |
| GA | 58.10 ± 12.33 | ||
| GR | 64.10 ± 5.65 | ||
| BIC (%) | SLA | 47.3 ± 6.58 | 0.046 * |
| GA | 54.61 ± 9.4 | ||
| GR | 60.19 ± 11.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, W.-T.; Kim, S.-Y.; Jung, S.-I.; Kang, S.-S.; Kim, S.-E.; Hwang, S.-H.; Jeong, C.-M.; Huh, J.-B. Effects of Gamma Radiation-Induced Crosslinking of Collagen Type I Coated Dental Titanium Implants on Osseointegration and Bone Regeneration. Materials 2021, 14, 3268. https://doi.org/10.3390/ma14123268
Cho W-T, Kim S-Y, Jung S-I, Kang S-S, Kim S-E, Hwang S-H, Jeong C-M, Huh J-B. Effects of Gamma Radiation-Induced Crosslinking of Collagen Type I Coated Dental Titanium Implants on Osseointegration and Bone Regeneration. Materials. 2021; 14(12):3268. https://doi.org/10.3390/ma14123268
Chicago/Turabian StyleCho, Won-Tak, So-Yeun Kim, Sung-In Jung, Seong-Soo Kang, Se-Eun Kim, Su-Hyun Hwang, Chang-Mo Jeong, and Jung-Bo Huh. 2021. "Effects of Gamma Radiation-Induced Crosslinking of Collagen Type I Coated Dental Titanium Implants on Osseointegration and Bone Regeneration" Materials 14, no. 12: 3268. https://doi.org/10.3390/ma14123268