
Lithium Disilicate Ceramic Endocrown Biomechanical Response According to Different Pulp Chamber Extension Angles and Filling Materials

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biacchi, G.R.; Basting, R.T. Comparison of fracture strength of endocrowns and glass fiber post-retained conventional crowns. Oper. Dent. 2012, 37, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topkara, C.; Keleş, A. Examining the adaptation of modified endocrowns prepared with CAD-CAM in maxillary and mandibular molars: A microcomputed tomography study. J. Prosthet. Dent. 2021, 13, S0022–3913. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.O.; de Jager, N.; Bottino, M.A.; de Kok, P.; Kleverlaan, C.J. Full-crown versus endocrown approach: A 3D-analysis of both restorations and the effect of ferrule and restoration material. J. Prosthodont. 2020, 28. [Google Scholar] [CrossRef] [PubMed]
- Al-Dabbagh, R.A. Survival and success of endocrowns: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 125, 415.e1–415.e9. [Google Scholar] [CrossRef]
- Fages, M.; Bennasar, B. The endocrown: A different type of all-ceramic reconstruction for molars. J. Can. Dent. Assoc. 2013, 79, d140. [Google Scholar] [PubMed]
- Dejak, B.; Młotkowski, A. A comparison of mvM stress of inlays, onlays and endocrowns made from various materials and their bonding with molars in a computer simulation of mastication—FEA. Dent. Mater. 2020, 36, 854–864. [Google Scholar] [CrossRef]
- Zhu, J.; Wang, D.; Rong, Q.; Qian, J.; Wang, X. Effect of central retainer shape and abduction angle during preparation of teeth on dentin and cement layer stress distributions in endocrown-restored mandibular molars. Dent. Mater. J. 2020, 21, 464–470. [Google Scholar] [CrossRef] [Green Version]
- de Kuijper, M.; Cune, M.S.; Tromp, Y.; Gresnigt, M.M.M. Cyclic loading and load to failure of lithium disilicate endocrowns: Influence of the restoration extension in the pulp chamber and the enamel outline. J. Mech. Behav. Biomed. Mater. 2020, 105, 103670. [Google Scholar] [CrossRef]
- Ghoul, W.E.; Özcan, M.; Tribst, J.P.M.; Salameh, Z. Fracture resistance, failure mode and stress concentration in a modified endocrown design. Biomater. Investig. Dent. 2020, 7, 110–119. [Google Scholar] [CrossRef]
- Eskitaşçioğlu, M.; Küçük, O.; Eskitaşçioğlu, G.; Eraslan, O.; Belli, S. The effect of different materials and techniques on stress distribution in CAD/CAM endocrowns. Strength Mater. 2020, 52, 812–819. [Google Scholar] [CrossRef]
- El Ghoul, W.; Özcan, M.; Silwadi, M.; Salameh, Z. Fracture resistance and failure modes of endocrowns manufactured with different CAD/CAM materials under axial and lateral loading. J. Esthet. Restor. Dent. 2019, 31, 378–387. [Google Scholar] [CrossRef]
- Sağlam, G.; Cengiz, S.; Karacaer, Ö. Marginal adaptation and fracture strength of endocrowns manufactured with different restorative materials: SEM and mechanical evaluation. Microsc. Res. Tech. 2021, 84, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Elashmawy, Y.; Elshahawy, W.; Seddik, M.; Aboushelib, M. Influence of fatigue loading on fracture resistance of endodontically treated teeth restored with endocrowns. J. Prosthodont. Res. 2020, 9, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Dogui, H.; Abdelmalek, F.; Amor, A.; Douki, N. Endocrown: An alternative approach for restoring endodontically treated molars with large coronal destruction. Case Rep. Dent. 2018, 30, 1581952. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Lin, Z.; Zheng, Z. Effect of different restorative crown design and materials on stress distribution in endodontically treated molars: A finite element analysis study. BMC Oral Health 2020, 18, 226. [Google Scholar] [CrossRef] [PubMed]
- Darwish, H.A.; Morsi, T.S.; El Dimeery, A.G. Internal fit of lithium disilicate and resin nano-ceramic endocrowns with different preparation designs. Future Dent. J. 2017, 3, 67–72. [Google Scholar] [CrossRef]
- Haralur, S.B.; Alamrey, A.A.; Alshehri, S.A.; Alzahrani, D.S.; Alfarsi, M. Effect of different preparation designs and all ceramic materials on fracture strength of molar endocrowns. J. Appl. Biomater. Funct. Mater. 2020, 18, 2280800020947329. [Google Scholar] [CrossRef]
- Tribst, J.P.; Dal Piva, A.O.; Madruga, C.F.; Valera, M.C.; Bresciani, E.; Bottino, M.A.; de Melo, R.M. The impact of restorative material and ceramic thickness on CAD\CAM endocrowns. J. Clin. Exp. Dent. 2019, 1, e969–e977. [Google Scholar] [CrossRef]
- Seddik, T.; Derelioglu, S. Effect of endocrowns on fracture strength and microleakage of endodontically treated primary molar teeth. J. Adv. Oral Res. 2019, 10, 113–119. [Google Scholar] [CrossRef]
- Thomas, R.M.; Kelly, A.; Tagiyeva, N.; Kanagasingam, S. Comparing endocrown restorations on permanent molars and premolars: A systematic review and meta-analysis. Br. Dent. J. 2020, 14. [Google Scholar] [CrossRef]
- Menezes-Silva, R.; Espinoza, C.A.V.; Atta, M.T.; de Lima Navarro, M.F.; Ishikiriama, S.K.; Mondelli, R.F.L. Endocrown: A conservative approach. Braz. Dent. Sci. 2016, 19, 121–131. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.O.; Madruga, C.F.L.; Valera, M.C.; Borges, A.L.S.; Bresciani, E.; de Melo, R.M. Endocrown restorations: Influence of dental remnant and restorative material on stress distribution. Dent. Mater. 2018, 34, 1466–1473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Guess, P.C.; Zhang, Y. Load-bearing properties of minimal-invasive monolithic lithium disilicate and zirconia occlusal onlays: Finite element and theoretical analyses. Dent. Mater. 2013, 29, 742–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Lo Giudice, R.; Borges, A.L.S.; Bottino, M.A.; Epifania, E.; Ausiello, P. The influence of custom-milled framework design for an implant-supported full-arch fixed dental prosthesis: 3D-FEA study. Int. J. Environ. Res. Public Health 2020, 17, 4040. [Google Scholar] [CrossRef]
- Rees, J.S.; Jacobsen, P.H. Elastic modulus of the periodontal ligament. Biomaterials 1997, 18, 995–999. [Google Scholar] [CrossRef]
- Correia, A.; Andrade, M.R.; Tribst, J.; Borges, A.; Caneppele, T. Influence of bulk-fill restoration on polymerization shrinkage stress and marginal gap formation in class V restorations. Oper. Dent. 2020, 1, E207–E216. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.; Ciaramella, S.; De Benedictis, A.; Lanzotti, A.; Tribst, J.P.M.; Watts, D.C. The use of different adhesive filling material and mass combinations to restore class II cavities under loading and shrinkage effects: A 3D-FEA. Comput. Methods Biomech. Biomed. Eng. 2020, 22, 1–11. [Google Scholar] [CrossRef]
- Pai, S.; Naik, N.; Patil, V.; Kaur, J.; Awasti, S.; Nayak, N. Evaluation and comparison of stress distribution in restored cervical lesions of mandibular premolars: Three-dimensional finite element analysis. J. Int. Soc. Prev. Community Dent. 2019, 4, 605–611. [Google Scholar] [CrossRef]
- Ausiello, P.P.; Ciaramella, S.; Lanzotti, A.; Ventre, M.; Borges, A.L.; Tribst, J.P.; Dal Piva, A.; Garcia-Godoy, F. Mechanical behavior of Class I cavities restored by different material combinations under loading and polymerization shrinkage stress. A 3D-FEA study. Am. J. Dent. 2019, 32, 55–60. [Google Scholar]
- Dikova, T.; Vasilev, T.; Hristova, V.; Panov, V. Finite element analysis in setting of fillings of V-shaped tooth defects made with glass-ionomer cement and flowable composite. Processes 2020, 8, 363. [Google Scholar] [CrossRef] [Green Version]
- Antunes, C., Jr.; Mercuri, E.G.F.; Franco, A.P.G.O.; Costa, M.; Karam, L.Z.; Kalinowski, H.J.; Gomes, O.M.M. Bulk fill flow resin contraction using 3D finite element model and calibration by Fiber Bragg Grating measurement. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 1127–1137. [Google Scholar] [CrossRef]
- Srivastava, B.N.; Devi, N.; Gupta, N.; Singh, R. Comparative evaluation of various temperature changes on stress distribution in class II mesial-occlusal-distal preparation restored with different restorative materials: A finite element analysis. Int. J. Clin. Pediatr. Dent. 2018, 11, 167–170. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Borges, A.L.S.; Silva-Concílio, L.R.; Bottino, M.A.; Özcan, M. Effect of restorative material on mechanical response of provisional endocrowns: A 3D—FEA study. Materials 2021, 14, 649. [Google Scholar] [CrossRef]
- Ferrari, M.; Keeling, A.; Mandelli, F.; Lo Giudice, G.; Garcia-Godoy, F.; Joda, T. The ability of marginal detection using different intraoral scanning systems: A pilot randomized controlled trial. Am. J. Dent. 2018, 31, 272–276. [Google Scholar]
- Ghajghouj, O.; Taşar-Faruk, S. Evaluation of fracture resistance and microleakage of endocrowns with different intracoronal depths and restorative materials luted with various resin cements. Materials 2019, 12, 2528. [Google Scholar] [CrossRef] [Green Version]
- Belleflamme, M.M.; Geerts, S.O.; Louwette, M.M.; Grenade, C.F.; Vanheusden, A.J.; Mainjot, A.K. No post-no core approach to restore severely damaged posterior teeth: An up to 10-year retrospective study of documented endocrown cases. J. Dent. 2017, 63, 1–7. [Google Scholar] [CrossRef] [PubMed]
- da Fonseca, G.F.; Dal Piva, A.M.; Tribst, J.P.; Borges, A.L. Influence of restoration height and masticatory load orientation on ceramic endocrowns. J. Contemp. Dent. Pract. 2018, 19, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Aktas, G.; Yerlikaya, H.; Akca, K. Mechanical failure of endocrowns manufactured with different ceramic materials: An in vitro biomechanical study. J. Prosthodont. 2018, 27, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Pires, C.W.; Lenzi, T.L.; Soares, F.Z.M.; Rocha, R.O. Zinc oxide eugenol paste jeopardises the adhesive bonding to primary dentine. Eur. Arch. Paediatr. Dent. 2018, 19, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Khosravani, M.R. Mechanical behavior of restorative dental composites under various loading conditions. J. Mech. Behav. Biomed. Mater. 2019, 93, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Habib, A.N.A.; Waly, G.H. The degree of conversion and class II cavity microleakage of different bulk fill composites placed with different restorative techniques. Future Dent. J. 2018, 4, 231–238. [Google Scholar] [CrossRef]
- Giudice, R.L.; Famà, F. Health care and health service digital revolution. Int. J. Environ. Res. Public Health 2020, 17, 4913. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
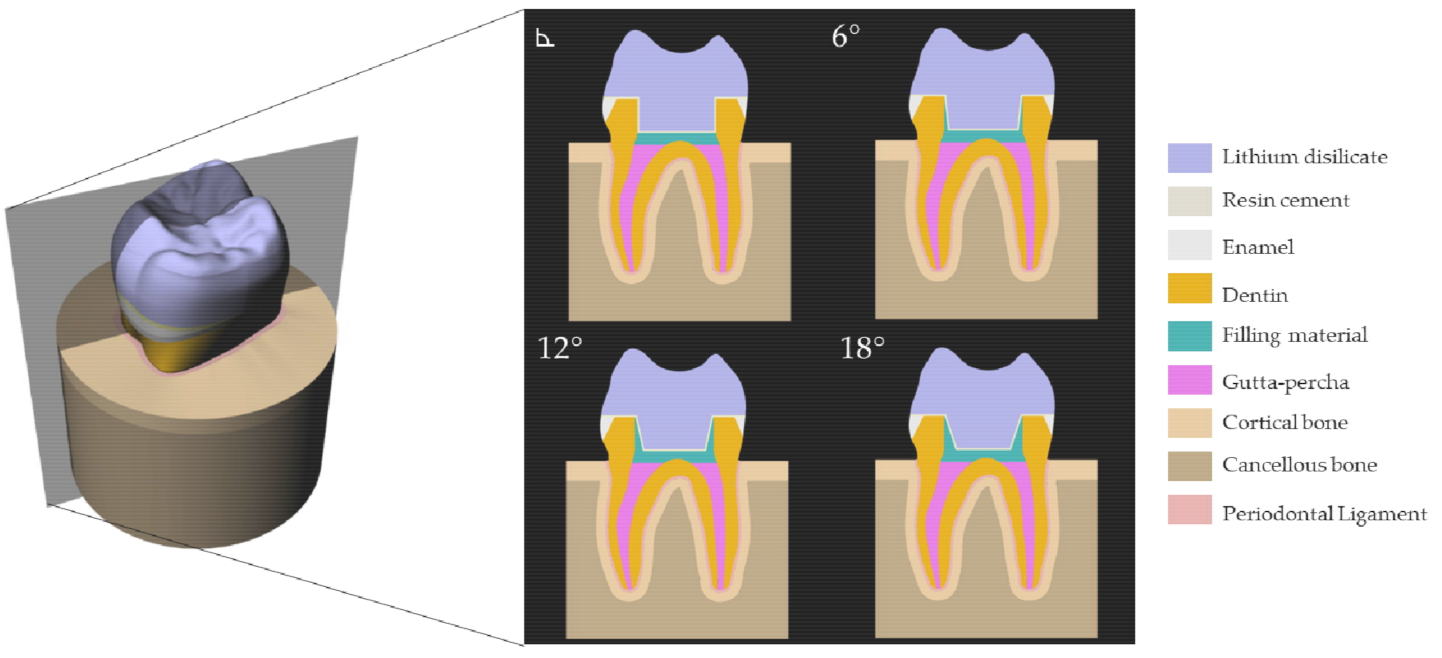
| Abbreviation | Materials/Structures | Elastic Modulus (GPa) | Poisson Ratio | References |
|---|---|---|---|---|
| - | Lithium disilicate | 95 | 0.30 | [23] |
| - | Enamel Tissue | 70 | 0.30 | [23] |
| - | Dentin Tissue | 18 | 0.30 | [23] |
| - | Cancellous bone | 1.37 | 0.30 | [24] |
| - | Cortical bone | 13.7 | 0.30 | [24] |
| - | Periodontal Ligament | 0.05 | 0.45 | [25] |
| RC | Resin composite | 13.45 | 0.17 | [26] |
| BF | Bulk-fill resin composite | 13.46 | 0.18 | [26] |
| AK | Alkasite | 13.00 | 0.30 | [28] |
| FRC | Flowable resin composite | 8.0 | 0.20 | [27] |
| GIC | Glass Ionomer Cement | 8.0 | 0.25 | [29] |
| AGIC | Autocured resin-reinforcedGlass ionomer cement | 8.32 | 0.27 | [30] |
| CM | Resin Cement | 8.6 | 0.18 | [23] |
| BFF | Bulk-fill flowable resin composite | 3.70 | 0.30 | [31] |
| ZO | Zinc oxide cement | 1.35 | 0.30 | [32] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tribst, J.P.M.; Lo Giudice, R.; dos Santos, A.F.C.; Borges, A.L.S.; Silva-Concílio, L.R.; Amaral, M.; Lo Giudice, G. Lithium Disilicate Ceramic Endocrown Biomechanical Response According to Different Pulp Chamber Extension Angles and Filling Materials. Materials 2021, 14, 1307. https://doi.org/10.3390/ma14051307
Tribst JPM, Lo Giudice R, dos Santos AFC, Borges ALS, Silva-Concílio LR, Amaral M, Lo Giudice G. Lithium Disilicate Ceramic Endocrown Biomechanical Response According to Different Pulp Chamber Extension Angles and Filling Materials. Materials. 2021; 14(5):1307. https://doi.org/10.3390/ma14051307
Chicago/Turabian StyleTribst, João Paulo Mendes, Roberto Lo Giudice, Alison Flavio Campos dos Santos, Alexandre Luiz Souto Borges, Laís Regiane Silva-Concílio, Marina Amaral, and Giuseppe Lo Giudice. 2021. "Lithium Disilicate Ceramic Endocrown Biomechanical Response According to Different Pulp Chamber Extension Angles and Filling Materials" Materials 14, no. 5: 1307. https://doi.org/10.3390/ma14051307