Prospect of Metal Ceramic (Titanium-Wollastonite) Composite as Permanent Bone Implants: A Narrative Review

 ,
,
Abstract
:1. Introduction
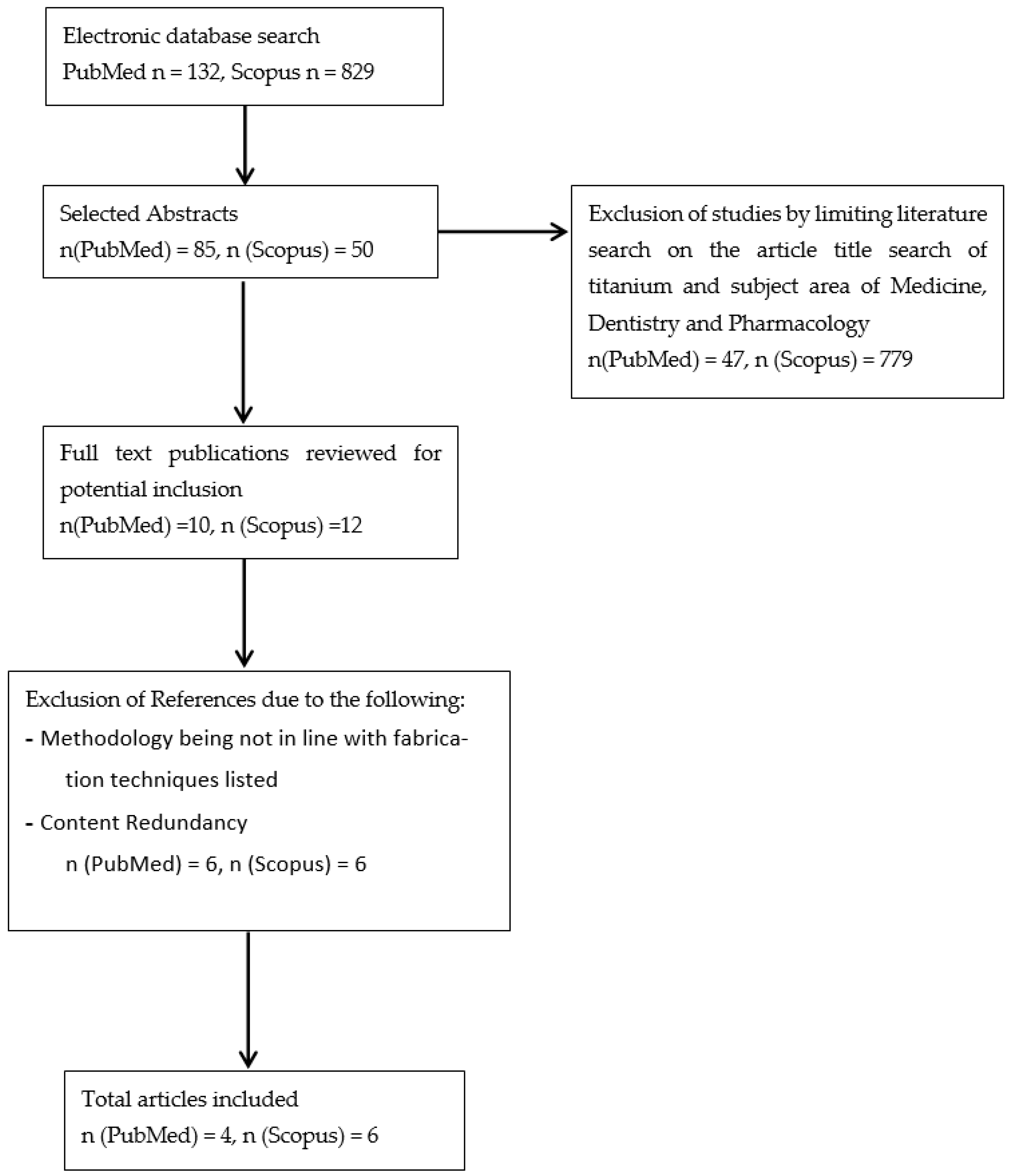
2. Methods
3. Structural Property of Metals and Bioceramics
3.1. Surface Characteristics
3.2. Mechanical Properties of Metals and Ceramics
4. Advantage of Metal-Ceramic Composites as Bone Implants
4.1. Physical Properties of Metal-Ceramic Composites as Biomaterials
4.2. Efficiency of Titanium–Hydroxyapatite as a Metal-Ceramic Hybrid
4.3. The Prospect of Wollastonite in Metal-Ceramic Hybrid
5. Fabrication of Metal-Ceramic Implants
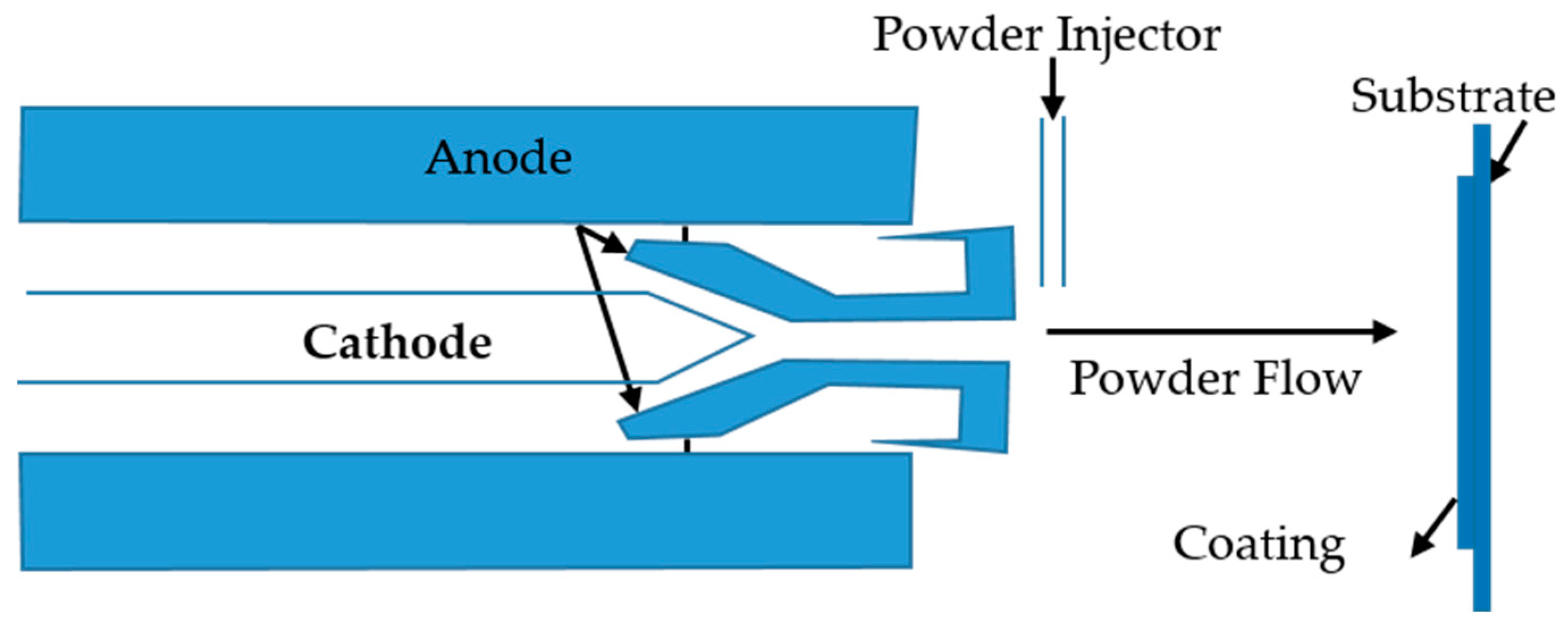
5.1. Plasma Spraying as a Conventional Method
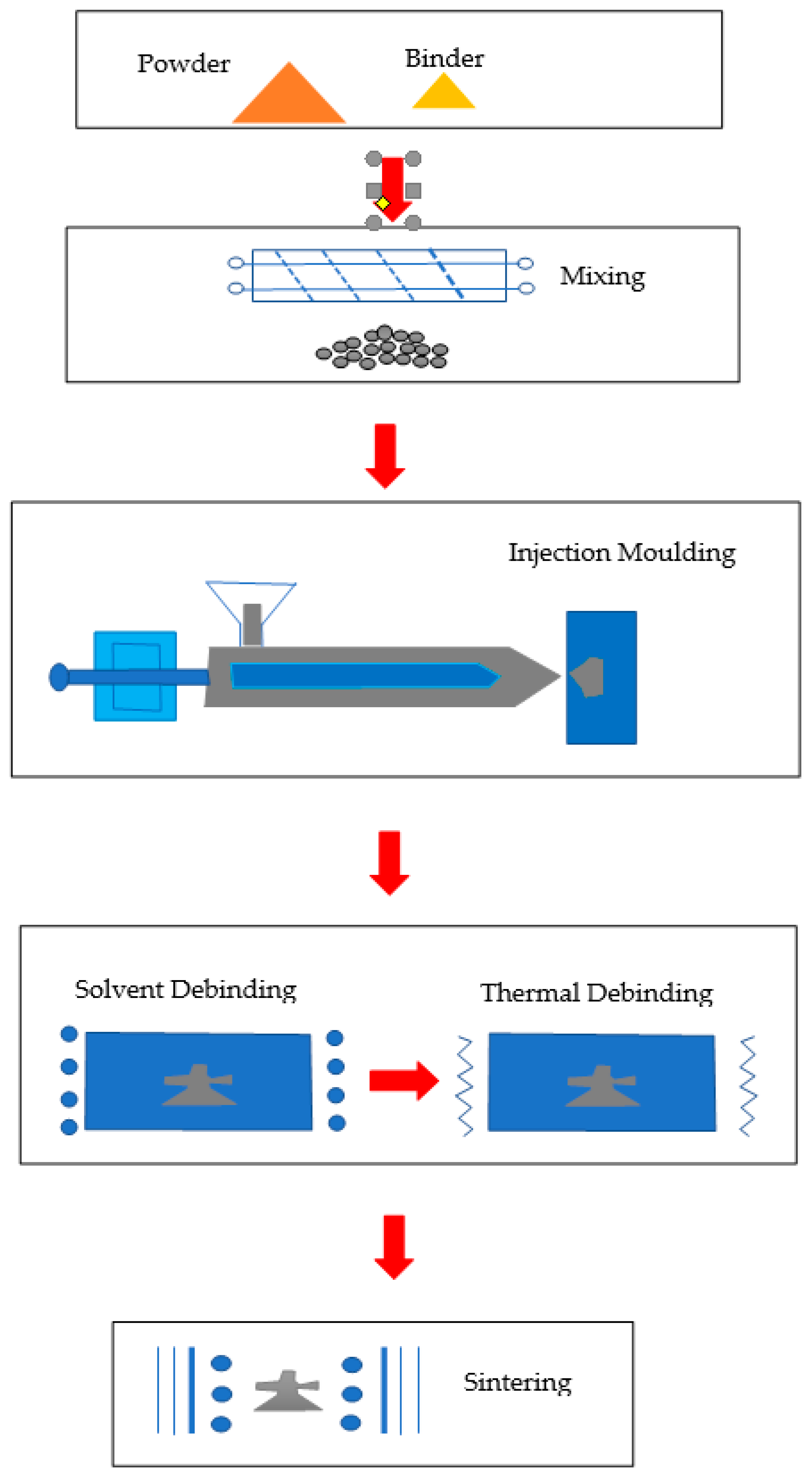
5.2. Powder Injection Moulding
5.3. Powder Compaction
6. Minimal Evaluations Required for New Materials before Clinical Applications
6.1. In Vitro Evaluation
6.2. In Vivo Evaluation
7. Commercialized Metal-Ceramic Implants
Cost of Materials to Manufacture Implants
8. Recommendations
9. Summary
10. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ng, M.H.; Duski, S.; Tan, K.K.; Yusof, M.R.; Low, K.C.; Mohamed Rose, I.; Mohamed, Z.; Bin Saim, A.; Haji Idrus, R.B. Repair of segmental load-bearing bone defect by autologous mesenchymal stem cells and plasma-derived fibrin impregnated ceramic block results in early recovery of limb function. Biomed. Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Haji Idrus, R.B.; Abas, A.; Ab Rahim, F.; Saim, A. Clinical translation of cell therapy, tissue engineering and regenerative medicine product in Malaysia and its regulatory policy. Tissue Eng. Part A 2015, 21. [Google Scholar] [CrossRef] [Green Version]
- Tan, K.K.; Tan, G.H.; Shamsul, B.S.; Chua, K.H.; Ng, M.H.; Ruszymah, B.H.; Aminuddin, B.S.; Loqman, M.Y. Bone graft substitute using hydroxyapatite scaffold seeded with tissue engineered autologous osteoprogenitor cells in spinal fusion: Early result in a sheep model. Med. J. Malays. 2005, 60, 53–58. [Google Scholar]
- Sulaiman, S.B.; Keong, T.K.; Cheng, C.H.; Saim, A.; Bin, H.J.; Idrus, R.B. Tricalcium phosphate/hydroxyapatite (TCP-HA) bone scaffold as potential candidate for the formation of tissue engineered bone. Indian J. Med. Res. 2013, 137, 1093–1101. [Google Scholar] [PubMed]
- Ng, A.M.H.; Tan, K.K.; Phang, M.Y.; Aziyati, O.; Tan, G.H.; Isa, M.R.; Aminuddin, B.S.; Naseem, M.; Fauziah, O.; Ruszymah, B.H.I. Differential osteogenic activity of osteoprogenitor cells on HA and TCP/HA scaffold of tissue engineered bone. J. Biomed. Mater. Res. Part A 2008, 85, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Zhou, W.; Liu, X.; Xian, F.; Liu, Z.; Zheng, Y.; An, Z. Peat records of human impacts on the atmosphere in Northwest China during the late Neolithic and Bronze Ages. Palaeogeogr. Palaeoclimatol. Palaeoecol. 2010, 286, 17–22. [Google Scholar] [CrossRef]
- Dorozhkin, S. Medical application of calcium orthophosphate bioceramics. Bio 2011, 1, 1–51. [Google Scholar] [CrossRef]
- Reza, E.; Aidin, S.; Reusmaazran, Y.; Rusnah, M.; Ng, M.H. Fabrcating and evaluating the different ratio of TCP:HA as scaffold for bone tissue engineering. J. Tissue Eng. Regen. Med. 2012, 6, 1–465. [Google Scholar] [CrossRef] [Green Version]
- Sadeghilar, A.; Ng, A.; Hwei, M.; Haflah, N.H.M.; Rose, I.M.; Firouzi, S. Local tissue reaction and biodegradation of Hydroxyapatite/Tricalcium Phosphate composites. World J. Med. Sci. 2014, 11, 301–305. [Google Scholar] [CrossRef]
- Shamsudin, R.; Abdul Azam, F.A.; Abdul Hamid, M.A.; Ismail, H. Bioactivity and cell compatibility of β-wollastonite derived from rice husk ash and limestone. Materials 2017, 10, 1188. [Google Scholar] [CrossRef] [Green Version]
- Azam, F.A.A.; Shamsudin, R.; Ng, M.H.; Zainuddin, Z.; Hamid, M.A.A.; Rashid, R.A. Mechanical and bioactive properties of mullite reinforced pseudowollastonite biocomposite. Sains Malays. 2018, 47, 2141–2149. [Google Scholar] [CrossRef]
- Le Huec, J.C.; Schaeverbeke, T.; Clement, D.; Faber, J.; Le Rebeller, A. Influence of porosity on the mechanical resistance of hydroxyapatite ceramics under compressive stress. Biomaterials 1995, 16, 113–118. [Google Scholar] [CrossRef]
- Hannink, G.; Arts, J.J.C. Bioresorbability, porosity and mechanical strength of bone substitutes: What is optimal for bone regeneration? Injury 2011, 42, S22–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsell, R.; Einhorn, T.A. The biology of fracture healing. Injury 2012, 42, 551–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saini, M. Implant biomaterials: A comprehensive review. World J. Clin. Cases 2015, 3, 52. [Google Scholar] [CrossRef]
- Aubret, S.; Merlini, L.; Fessy, M.; Besse, J.L. Poor outcomes of fusion with Trabecular Metal implants after failed total ankle replacement: Early results in 11 patients. Orthop. Traumatol. Surg. Res. 2018, 104, 231–237. [Google Scholar] [CrossRef]
- Takagi, M. Bone-implant interface biology. Foreign body reaction and periprosthetic osteolysis in artificial hip joints. J. Clin. Exp. Hematop. 2001, 41, 81–87. [Google Scholar] [CrossRef]
- Jiang, Y.; Jia, T.; Wooley, P.H.; Yang, S.Y. Current research in the pathogenesis of aseptic implant loosening associated with particulate wear debris. Acta Orthop. Belg. 2013, 79, 1–9. [Google Scholar]
- Jiang, Y.; Han, Y.; Wang, J.; Lv, F.; Yi, Z.; Ke, Q.; Xu, H. Space-oriented nanofibrous scaffold with silicon-doped amorphous calcium phosphate nanocoating for diabetic wound healing. ACS Appl. Bio Mater. 2019, 2, 787–795. [Google Scholar] [CrossRef]
- Ramli, M.I.; Sulong, A.B.; Muhamad, N.; Muchtar, A.; Zakaria, M.Y. Effect of sintering on the microstructure and mechanical properties of alloy titanium-wollastonite composite fabricated by powder injection moulding process. Ceram. Int. 2019, 45, 11648–11653. [Google Scholar] [CrossRef]
- Brie, I.C.; Soritau, O.; Dirzu, N.; Berce, C.; Vulpoi, A.; Popa, C.; Todea, M.; Simon, S.; Perde-Schrepler, M.; Virag, P.; et al. Comparative In Vitro study regarding the biocompatibility of titanium-base composites infiltrated with hydroxyapatite or silicatitanate. J. Biol. Eng. 2014, 8, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, R.; Faramarzi, R.; Jungwirth, F.; Kleffner, B.V.; Mumme, T.; Weber, M.; Wirtz, D.C. Silikatbeschichtung zementierter Titanschäfte für die Reduzierung aseptischer Lockerungsraten Silicate Coating of Cemented Titanium-Based Shafts in Hip Prosthetics Reduces High Aseptic Loosening. Zeitschrift Orthopädie Unfallchirurgie 2009, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Yoo, Y.; Jang, S.; Oh, K.; Kim, J.; Kim, Y. Influences of Passivating elements on the corrosion and biocompatibility of super stainless steels. J. Biomed. Mater. Res. Part B Appl. Biomater. Off. J.Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2007. [Google Scholar] [CrossRef]
- Hyslop, D.J.S.; Abdelkader, A.M.; Cox, A.; Fray, D.J. Electrochemical synthesis of a biomedically important Co—Cr alloy. Acta Mater. 2010, 58, 3124–3130. [Google Scholar] [CrossRef]
- Suchanek, W.; Yoshimura, M. Processing and properties of hydroxyapatite-based biomaterials for use as hard tissue replacement implants. J. Mater. Res. 1998, 13, 94–117. [Google Scholar] [CrossRef]
- Points, P. Allergic reaction to vanadium causes a diffuse eczematous eruption and titanium alloy orthopedic implant failure. Cutis 2017, 99, 245–249. [Google Scholar]
- Sinha, S.; Begam, H.; Kumar, V.; Nandi, S.K.; Kubacki, J.; Chanda, A. Improved performance of the functionalized nitinol as a prospective bone implant material. J. Mater. Res. 2018, 33, 2554–2564. [Google Scholar] [CrossRef]
- Jenko, M.; Godec, M.; Kocijan, A.; Rudolf, R.; Dolinar, D.; Ovsenik, M.; Gorenšek, M.; Mozetic, M. A new route to biocompatible Nitinol based on a rapid treatment with H 2 /O 2 gaseous plasma. Appl. Surf. Sci. 2019, 473, 976–984. [Google Scholar] [CrossRef]
- Shabalovskaya, S.; Anderegg, J.; Van Humbeeck, J. Critical overview of Nitinol surfaces and their modifications for medical applications. Acta Biomater. 2008, 4, 447–467. [Google Scholar] [CrossRef]
- Rubitschek, F.; Niendorf, T.; Karaman, I.; Maier, H.J. Corrosion fatigue behavior of a biocompatible ultrafine-grained niobium alloy in simulated body fluid. J. Mech. Behav. Biomed. Mater. 2012, 5, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Pawar, V.; Weaver, C.; Jani, S. Physical characterization of a new composition of oxidized zirconium-2.5 wt% niobium produced using a two step process for biomedical applications. Appl. Surf. Sci. 2011, 257, 6118–6124. [Google Scholar] [CrossRef]
- Miyazaki, S.; Kim, H.Y. Basic Characteristics of Titanium–Nickel (Ti–Ni)-Based and Titanium–Niobium (Ti–Nb)-Based Alloys; Woodhead Publishing Limited: Cambridge, UK, 2011. [Google Scholar] [CrossRef]
- Kayhan, S.M.; Tahmasebifar, A.; Koç, M.; Usta, Y.; Tezcaner, A.; Evis, Z. Experimental and numerical investigations for mechanical and microstructural characterization of micro-manufactured AZ91D magnesium alloy disks for biomedical applications. Mater. Des. 2016, 93, 397–408. [Google Scholar] [CrossRef]
- Gu, X.N.; Zhou, W.R.; Zheng, Y.F.; Cheng, Y.; Wei, S.C.; Zhong, S.P.; Xi, T.F.; Chen, L.J. Corrosion fatigue behaviors of two biomedical Mg alloys—AZ91D and WE43—In simulated body fluid. Acta Biomater. 2010, 6, 4605–4613. [Google Scholar] [CrossRef]
- Lehr, I.L.; Saidman, S.B. Corrosion protection of AZ91D magnesium alloy by a cerium-molybdenum coating. The effect of citric acid as an additive. J. Magnes. Alloy. 2018, 6, 356–365. [Google Scholar] [CrossRef]
- Oonishi, H.; Kushitani, S.; Yasukawa, E.; Iwaki, H.; Hench, L.L.; Wilson, J.; Tsuji, E.; Sugihara, T. Particulate bioglass compared with hydroxyapatite as a bone graft substitute. Clin. Orthop. Relat. Res. 1997, 334, 316–325. [Google Scholar] [CrossRef]
- Descamps, M.; Richart, O.; Hardouin, P.; Hornez, J.C.; Leriche, A. Synthesis of macroporous b -tricalcium phosphate with controlled porous architectural. Ceram. Int. 2008, 34, 1131–1137. [Google Scholar] [CrossRef]
- Seebach, C.; Schultheiss, J.; Wilhelm, K.; Frank, J.; Henrich, D. Comparison of six bone-graft substitutes regarding to cell seeding efficiency, metabolism and growth behaviour of human mesenchymal stem cells (MSC) In Vitro. Injury 2010, 41, 731–738. [Google Scholar] [CrossRef]
- Ducheyne, P. Bioglass coatings and bioglass composites as implant materials. J. Biomed. Mater. Res. 1985, 19, 273–291. [Google Scholar] [CrossRef]
- Hench, L.L. The story of Bioglass. Mater. Med. 2006, 967–978. [Google Scholar] [CrossRef]
- Fabbri, P.; Cannillo, V.; Sola, A.; Dorigato, A.; Chiellini, F. Highly porous polycaprolactone-45S5 Bioglass Ò scaffolds for bone tissue engineering. Compos. Sci. Technol. 2010, 70, 1869–1878. [Google Scholar] [CrossRef] [Green Version]
- Aina, V.; Malavasi, G.; Fiorio Pla, A.; Munaron, L.; Morterra, C. Zinc-containing bioactive glasses: Surface reactivity and behaviour towards endothelial cells. Acta Biomater. 2009, 5, 1211–1222. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Lakshmi, T. Bioglass: A novel biocompatible innovation. J. Adv. Pharm. Technol. Res. 2013, 4, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Siriphannon, P.; Kameshima, Y.; Yasumori, A. Formation of hydroxyapatite on CaSiO 3 powders in simulated body fluid. J. Eur. Ceram. Soc. 2002, 22, 511–520. [Google Scholar] [CrossRef]
- De Aza, P.N.; Luklinska, Z.B.; Anseau, M.R.; Hector, M.; Guitia, F.; De Aza, S. Reactivity of a wollastonite tricalcium phosphate Bioeutectic ceramic in human parotid saliva. Biomaterials 2000, 21, 1735–1741. [Google Scholar] [CrossRef]
- Xu, S.; Lin, K.; Wang, Z.; Chang, J.; Wang, L.; Lu, J.; Ning, C. Reconstruction of calvarial defect of rabbits using porous calcium silicate bioactive ceramics. Biomaterials 2008, 29, 2588–2596. [Google Scholar] [CrossRef]
- Bratton, E.M.; Durairaj, V.D. Orbital implants for fracture repair. Curr. Opin. Ophthalmol. 2011, 22, 400–406. [Google Scholar] [CrossRef]
- Gomez d’Ayala, G.; De Rosa, A.; Laurienzo, P.; Malinconico, M. Elastin Blends for Tissue Engineering Scaffolds. J. Biomed. Mater. Res. Part A 2006, 79, 963–973. [Google Scholar] [CrossRef]
- Vlad, M.D.; Şindilar, E.V.; Mariñoso, M.L.; Poeată, I.; Torres, R.; López, J.; Barracó, M.; Fernández, E. Osteogenic biphasic calcium sulphate dihydrate/iron-modified α-tricalcium phosphate bone cement for spinal applications: In vivo study. Acta Biomater. 2010, 6, 607–616. [Google Scholar] [CrossRef]
- Yashavantha Kumar, C.; Nalini, K.B.; Menon, J.; Patro, D.K.; Banerji, B.H. Calcium sulfate as bone graft substitute in the treatment of osseous bone defects, a prospective study. J. Clin. Diagn. Res. 2013, 7, 2926–2928. [Google Scholar] [CrossRef]
- Wahl, P.; Livio, F.; Jacobi, M.; Gautier, E.; Buclin, T. Systemic exposure to tobramycin after local antibiotic treatment with calcium sulphate as carrier material. Arch. Orthop. Trauma Surg. 2011, 131, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Biradar, S.; Ravichandran, P.; Gopikrishnan, R.; Goornavar, V.; Hall, J.C.; Ramesh, V.; Baluchamy, S.; Jeffers, R.B.; Govindarajan, R.T. Calcium carbonate nanoparticles: Synthesis, characterization and biocompatibility. J. Nanosci. Nanotechnol. 2011, 11, 6868–6874. [Google Scholar] [CrossRef] [PubMed]
- Dizaj, S.M.; Barzegar-Jalali, M.; Hossein Zarrintan, M.; Adibkia, K.; Lotfipour, F. Calcium carbonate nanoparticles; Potential in bone and tooth disorders. Pharm. Sci. 2015, 20, 175–182. [Google Scholar] [CrossRef]
- Wang, C.; Chen, S.; Yu, Q.; Hu, F.; Yuan, H. Taking advantage of the disadvantage: Employing the high aqueous instability of amorphous calcium carbonate to realize burst drug release within cancer cells. J. Mater. Chem. B 2017, 5, 2068–2073. [Google Scholar] [CrossRef]
- Almeida, J.C.; Wacha, A.; Gomes, P.S.; Fernandes, M.H.R.; Fernandes, M.H.V.; Salvado, I.M.M. PDMS-SiO2-TiO2-CaO hybrid materials—Cytocompatibility and nanoscale surface features. Mater. Sci. Eng. C 2016, 64, 74–86. [Google Scholar] [CrossRef]
- Wu, Y.; Zitelli, J.P.; TenHuisen, K.S.; Yu, X.; Libera, M.R. Differential response of Staphylococci and osteoblasts to varying titanium surface roughness. Biomaterials 2011, 32, 951–960. [Google Scholar] [CrossRef]
- Ma, X.; Feng, Y.; Ma, Z.; Li, X.; Wang, J.; Wang, L. Biomaterials The promotion of osteointegration under diabetic conditions using chitosan/hydroxyapatite composite coating on porous titanium surfaces. Biomaterials 2014, 35, 7259–7270. [Google Scholar] [CrossRef]
- Carano, R.A.D.D.; Filvaroff, E.H.; Carano, R.A.D.D.; Filvaroff, E.H. Angiogenesis and bone repair. Drug Discov. Today 2003, 8, 980–989. [Google Scholar] [CrossRef]
- Zardiackas, L.D.; Parsell, D.E.; Dillon, L.D.; Mitchell, D.W.; Nunnery, L.A.; Poggie, R. Structure, metallurgy, and mechanical properties of a porous tantalum foam. J. Biomed. Mater. Res. 2001, 58, 180–187. [Google Scholar] [CrossRef]
- Balla, V.K.; Bodhak, S.; Bose, S.; Bandyopadhyay, A. Porous tantalum structures for bone implants: Fabrication, mechanical and in vitro biological properties. Acta Biomater. 2010, 6, 3349–3359. [Google Scholar] [CrossRef] [Green Version]
- Karageorgiou, V.; Kaplan, D. Porosity of 3D biomaterial scaffolds and osteogenesis. Biomaterials 2005, 26, 5474–5491. [Google Scholar] [CrossRef] [PubMed]
- Itl, A.I.; Ylnen, H.O.; Ekholm, C.; Karlsson, K.H.; Aro, H.T. Pore diameter of more than 100 μm is not requisite for bone ingrowth in rabbits. J. Biomed. Mater. Res. 2001, 58, 679–683. [Google Scholar] [CrossRef]
- Liu, F.H. Fabrication of bioceramic bone scaffolds for tissue engineering. J. Mater. Eng. Perform. 2014, 23, 3762–3769. [Google Scholar] [CrossRef]
- Deligianni, D.D.; Katsala, N.D.; Koutsoukos, P.G.; Missirlis, Y.F. Effect of surface roughness of hydroxyapatite on human bone marrow cell adhesion, proliferation, differentiation and detachment strength. Biomaterials 2000, 22, 87–96. [Google Scholar] [CrossRef]
- Hench, L.L. Bioceramics: From concept to clinic. J. Am. Ceram. Soc. 1991, 74, 1487–1510. [Google Scholar] [CrossRef]
- Heakal, F.E.T.; Shehata, O.S.; Tantawy, N.S. Integrity of metallic medical implants in physiological solutions. Int J. Electrochem. Sci. 2014, 9, 1986–2004. [Google Scholar]
- Koseki, H.; Tomita, M.; Yonekura, A.; Higuchi, T.; Sunagawa, S.; Baba, K.; Osaki, M. Effect of carbon ion implantation on the tribology of metal-on-metal bearings for artificial joints. Int. J. Nanomed. 2017, 12, 4111–4116. [Google Scholar] [CrossRef] [Green Version]
- Tavares, D.; Castro, L.; Soares, G.; Alves, G.; Granjeiro, J. Synthesis and cytotoxicity evaluation of granular magnesium substituted β-tricalcium phosphate. J. Appl. Oral Sci. 2013, 1, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Himanshu, T.; Sp, S.; Ka, S.; Prerna, M.; Ashish, J. Studies on preparation and characterization of 45S5 Bioactive glass doped with (TiO 2 + ZrO 2 ) as bioactive ceramic material. Bioceram. Dev. Appl. 2016, 6, 1–6. [Google Scholar] [CrossRef]
- Arifin, A.; Sulong, A.B.; Muhamad, N.; Syarif, J.; Ramli, M.I. Material processing of hydroxyapatite and titanium alloy (HA/Ti) composite as implant materials using powder metallurgy: A review. Mater. Des. 2014, 55, 165–175. [Google Scholar] [CrossRef]
- Wang, X.; Li, J.; Hu, R.; Kou, H.; Zhou, L. Mechanical properties of porous titanium with different distributions of pore size. Trans. Nonferr. Met. Soc. China 2013, 23, 2317–2322. [Google Scholar] [CrossRef]
- Nakai, M.; Niinomi, M.; Zhao, X.; Zhao, X. Self-adjustment of Young’s modulus in biomedical titanium alloys during orthopaedic operation. Mater. Lett. 2011, 65, 688–690. [Google Scholar] [CrossRef]
- Kuroda, D.; Niinomi, M.; Morinaga, M.; Kato, Y.; Yashiro, T. Design and mechanical properties of new i type titanium alloys for implant materials. Mater. Sci. Eng. A 1998, 243, 244–249. [Google Scholar] [CrossRef]
- Keaveney, S.; Baron, S.; Ahearne, E.; Connolly, P.; Byrne, G. An Assessment of Medical Grade Cobalt Chromium Alloy ASTM F1537 as a Difficult-to-Cut (DTC) Material An Assessment of Medical Grade Cobalt Chromium Alloy ASTM F1537 as a “Difficult-to-Cut (DTC)”; Material. Available online: https://www.researchgate.net/publication/287198713 (accessed on 2 July 2019).
- Kato, K.; Yamamoto, A.; Ochiai, S.; Wada, M.; Daigo, Y.; Kita, K.; Omori, K. Cytocompatibility and mechanical properties of novel porous 316 L stainless steel. Mater. Sci. Eng. C 2013, 33, 2736–2743. [Google Scholar] [CrossRef]
- Mi, Z.R.; Shuib, S.; Hassan, A.Y.; Shorki, A.A.; Ibrahim, M.M. Problem of stress shielding and improvement to the hip implant designs: A Review. J. Med. Sci. 2007, 7, 460–467. [Google Scholar]
- Sumitomo, N.; Noritake, K.; Hattori, T.; Morikawa, K.; Niwa, S.; Sato, K.; Niinomi, M. Experiment study on fracture fixation with low rigidity titanium alloy Plate fixation of tibia fracture model in rabbit. Mat. Med. 2008, 1581–1586. [Google Scholar] [CrossRef]
- Niinomi, M.; Liu, Y.; Nakai, M.; Liu, H.; Li, H. Biomedical titanium alloys with Young’s moduli close to that of cortical bone. Regen. Biomater. 2016. [Google Scholar] [CrossRef] [Green Version]
- Havaldar, R.; Pilli, S.; Putti, B. Insights into the effects of tensile and compressive loadings on human femur bone. Adv. Biomed. Res. 2014, 3, 101. [Google Scholar] [CrossRef]
- Yamada, S.; Tadano, S.; Fukuda, S. Nanostructure and elastic modulus of single trabecula in bovine cancellous bone. J. Biomech. 2014, 47, 3482–3487. [Google Scholar] [CrossRef]
- Cesar, R.; Leivas, T.P.; Pereira, C.A.M.; Boffa, R.S.; Guarniero, R.; de Menezes Reiff, R.B.; Netto, A.M.; Fortulan, C.A.; de Almeida Rollo, J.M.D. Axial compressive strength of human vertebrae trabecular bones classified as normal, osteopenic and osteoporotic by quantitative ultrasonometry of calcaneus. Res. Biomed. Eng. 2017, 33, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Sanyal, A.; Gupta, A.; Bayraktar, H.H.; Kwon, R.Y.; Keaveny, T.M. Shear strength behavior of human trabecular bone. J. Biomech. 2012, 45, 2513–2519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautam, C.R.; Kumar, S.; Biradar, S.; Jose, S.; Mishra, V.K. Synthesis and enhanced mechanical properties of MgO substituted hydroxyapatite: A bone substitute material. RSC Adv. 2016, 6, 67565–67574. [Google Scholar] [CrossRef]
- Mondal, S.; Pal, U.; Dey, A. Natural origin hydroxyapatite scaffold as potential bone tissue engineering substitute. Ceram. Int. 2016, 42, 18338–18346. [Google Scholar] [CrossRef]
- Liang, L.; Rulis, P.; Ching, W.Y. Mechanical properties, electronic structure and bonding of α-and β-tricalcium phosphates with surface characterization. Acta Biomater. 2010, 6, 3763–3771. [Google Scholar] [CrossRef]
- Tian, Y.; Lu, T.; He, F.; Xu, Y.; Shi, H.; Shi, X.; Zuo, F.; Wu, S.; Ye, J. Β-Tricalcium phosphate composite ceramics with high compressive strength, enhanced osteogenesis and inhibited osteoclastic activities. Coll. Surf. B Biointerfaces 2018, 167, 318–327. [Google Scholar] [CrossRef]
- Shim, J.H.; Won, J.Y.; Park, J.H.; Bae, J.H.; Ahn, G.; Kim, C.H.; Lim, D.H.; Cho, D.W.; Yun, W.S.; Bae, E.B.; et al. Effects of 3D-printed polycaprolactone/β-tricalcium phosphate membranes on guided bone regeneration. Int. J. Mol. Sci. 2017, 18, 899. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Yang, X.; Shao, H.; Juan, Y.; Yong, H.; Jianzhong, F.; Changyou, G.; Zhongru, G. Simultaneous mechanical property and biodegradation improvement of wollastonite bioceramic through magnesium dilute doping. J. Mech. Behav. Biomed. Mater. 2016, 54, 60–71. [Google Scholar] [CrossRef]
- Baino, F.; Pons, E. Modelling the relationship between tensile strength and porosity in bioceramic scaffolds. Int. J. Appl. Ceram. Technol. 2019, 16, 1823–1829. [Google Scholar] [CrossRef]
- Baino, F.; Fiume, E. Elastic mechanical properties of 45S5-based bioactive glass-ceramic scaffolds. Materials 2019, 12, 3244. [Google Scholar] [CrossRef] [Green Version]
- Řehořek, L.; Chlup, Z.; Meng, D.; Yunos, D.M.; Boccaccini, A.R.; Dlouhý, I. Response of 45S5 Bioglass® foams to tensile loading. Ceram. Int. 2013, 39, 8015–8020. [Google Scholar] [CrossRef]
- Wang, Q.; Eltit, F.; Wang, R. Corrosion of Orthopedic Implants; Elsevier Inc.: Amsterdam, The Netherlands, 2018; Volumes 1–3. [Google Scholar] [CrossRef]
- Wakily, H.; Dabbagh, A.; Abdullah, H.; Abdul Halim, N.F.; Abu Kasim, N.H. Improved thermal and mechanical properties in hydroxyapatite-titanium composites by incorporating silica-coated titanium. Mater. Lett. 2015, 143, 322–325. [Google Scholar] [CrossRef]
- Wu, S.; Liu, X.; Gao, C. Role of adsorbed proteins on hydroxyapatite-coated titanium in osteoblast adhesion and osteogenic differentiation. Sci. Bull. 2015, 60, 691–700. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-J.; Kwon, T.-Y.; Kim, K.-H.; Kang, S.S.; Choi, S.H.; Kwon, S.T.; Cho, D.H.; Son, J.S. In Vitro evaluation of hydroxyapatite-coated titanium implant with Atmospheric Plasma Treatment. J. Nanosci. Nanotechnol. 2015, 15, 5593–5596. [Google Scholar] [CrossRef] [PubMed]
- Pillai, R.S.; Frasnelli, M.; Sglavo, V.M. HA/β-TCP plasma sprayed coatings on Ti substrate for biomedical applications. Ceram. Int. 2018, 44, 1328–1333. [Google Scholar] [CrossRef]
- Kumari, R.; Majumdar, J.D. Microstructure and surface mechanical properties of plasma spray deposited and post spray heat treated hydroxyapatite (HA) based composite coating on titanium alloy (Ti-6Al-4V) substrate. Mater. Charact. 2017, 131, 12–20. [Google Scholar] [CrossRef]
- Qiao, S.C.; Du, J.; Zhao, J.M.; Shi, J.Y.; Gu, Y.X.; Lai, H.C. Effects of a hydroxyapatite-coated nanotube surface of titanium on MC3T3-E1 cells: An In Vitro study. Implant. Dent. 2015, 24, 204–210. [Google Scholar] [CrossRef]
- Catauro, M. Response In Vitro Human Cells to Hydroxyapatite Coatings on Titanium Substrates Synthesized by Sol-Gel Process. EC Dent. Sci. 2017, 6, 165–173. [Google Scholar]
- Yang, Y.; Kim, K.H.; Agrawal, C.M.; Ong, J.L. Interaction of hydroxyapatite-titanium at elevated temperature in vacuum environment. Biomaterials 2004, 25, 2927–2932. [Google Scholar] [CrossRef]
- Tan, X.W.; Beuerman, R.W.; Shi, Z.L.; Neoh, K.G.; Tan, D.; Khor, K.A.; Mehta, J.S. In Vivo evaluation of titanium oxide and hydroxyapatite as an artificial cornea skirt. J. Mater. Sci. Mater. Med. 2012, 23, 1063–1072. [Google Scholar] [CrossRef]
- Costa De Almeida, C.; Sena, L.Á.; Pinto, M.; Muller, C.A.; Cavalcanti Lima, J.H.; Soares, G.D.A. In Vivo characterization of titanium implants coated with synthetic hydroxyapatite by electrophoresis. Braz. Dent. J. 2005, 16, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Eliaz, N.; Xiang, Z.; Hsu, H.P.; Spector, M.; Hobbs, L.W. Early bone apposition in vivo on plasma-sprayed and electrochemically deposited hydroxyapatite coatings on titanium alloy. Biomaterials 2006, 27, 4192–4203. [Google Scholar] [CrossRef] [PubMed]
- Palakurthy, S.; Samudrala, R.K. In vitro bioactivity and degradation behaviour of β-wollastonite derived from natural waste. Mater. Sci. Eng. C 2019, 98, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Hossain, S.S.; Yadav, S.; Majumdar, S.; Krishnamurthy, S.; Pyare, R.; Roy, P.K. A comparative study of physico-mechanical, bioactivity and hemolysis properties of pseudo-wollastonite and wollastonite glass-ceramic synthesized from solid wastes. Ceram. Int. 2020, 46, 833–843. [Google Scholar] [CrossRef]
- Obeid, M.M. Crystallization of synthetic wollastonite prepared from local raw materials. Int J. Mater. Chem. 2014, 4, 79–87. [Google Scholar] [CrossRef]
- Rahmani, R.; Antonov, M.; Kollo, L.; Holovenko, Y.; Prashanth, K.G. Mechanical behavior of Ti6Al4V scaffolds filled with CaSiO3 for implant applications. Appl. Sci. 2019, 9, 3844. [Google Scholar] [CrossRef] [Green Version]
- Aly, I.H.M.; Abed Alrahim Mohammed, L.; Al-Meer, S.; Elsaid, K.; Barakat, N.A.M. Preparation and characterization of wollastonite/titanium oxide nanofiber bioceramic composite as a future implant material. Ceram. Int. 2016, 42, 11525–11534. [Google Scholar] [CrossRef]
- Solonenko, A.P.; Blesman, A.I.; Polonyankin, D.A. Preparation and in vitro apatite-forming ability of hydroxyapatite and β-wollastonite composite materials. Ceram. Int. 2018, 44, 17824–17834. [Google Scholar] [CrossRef]
- Zhao, X.; Wang, T.; Qian, S.; Liu, X.; Sun, J.; Li, B. Silicon-doped titanium dioxide nanotubes promoted bone formation on titanium implants. Int. J. Mol. Sci. 2016, 17, 292. [Google Scholar] [CrossRef] [Green Version]
- Arora, M.; Arora, E. The promise of silicon: Bone regeneration and increased bone density. J. Arthrosc. Jt. Surg. 2017, 4, 103–105. [Google Scholar] [CrossRef]
- Sampath, S.; Herman, H. Rapid solidification and microstructure development during plasma spray deposition. J. Therm. Spray Technol. 1996, 5, 445–456. [Google Scholar] [CrossRef]
- Fu, Q.; Hong, Y.; Liu, X.; Fan, H.; Zhang, X. A hierarchically graded bioactive scaffold bonded to titanium substrates for attachment to bone. Biomaterials 2011, 32, 7333–7346. [Google Scholar] [CrossRef] [PubMed]
- Flame Spray Technologies. APS Plasma Thermal Spray Coating System. Available online: https://www.fst.nl/thermal-spray-equipment/modular-thermal-spray-systems/plasma-thermal-spray-systems.html (accessed on 12 March 2019).
- Levingstone, T.J.; Ardhaoui, M.; Benyounis, K.; Looney, L.; Stokes, J.T. Plasma sprayed hydroxyapatite coatings: Understanding process relationships using design of experiment analysis. Surf. Coat. Technol. 2015, 283, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Arifin, A.; Sulong, A.B.; Muhamad, N.; Syarif, J.; Ramli, M.I. Powder injection molding of HA/Ti6Al4V composite using palm stearin as based binder for implant material. Mater. Des. 2015, 6, 1028–1034. [Google Scholar] [CrossRef]
- Ramli, M.I.; Sulong, A.B.; Muhamad, N.; Muctar, A.; Ng, M.H.; Shanmuganantha, L. Ti6Al4V/Wollastonite composite through powder injection molding process for bone implant application. In Proceedings of the International Medical Device and Technology Conference, Skudai, Johor, Malaysia, 6–7 September 2017; pp. 256–260. [Google Scholar]
- Chen, L.; Li, T.; Li, Y.; He, H.; Hu, Y. Porous titanium implants fabricated by metal injection molding. Trans. Nonferr. Met. Soc. China 2009, 19, 1174–1179. [Google Scholar] [CrossRef]
- Shivashankar, T.S.; German, R.M. Effective length scale for predicting solvent-debinding times of components produced by powder injection molding. J. Am. Ceram. Soc. 1999, 82, 1146–1152. [Google Scholar] [CrossRef]
- Ye, H.; Yang, X.; Hong, H. Fabrication of metal matrix composites by metal injection molding—A review. J. Mater. Process. Technol. 2007, 200, 12–24. [Google Scholar] [CrossRef] [Green Version]
- Todd, R.H.; Allen, D.K.; Alting, L. Manufacturing Processes Reference Guide, 1st ed.; Industrial Press Inc.: South Norwalk, CT, USA, 2019. [Google Scholar]
- Abida, F.; Elassfouri, M.; Ilou, M.; El, B.; Jamil, M.; Moncif, N. Tricalcium phosphate powder: Preparation, characterization and compaction abilities. Mediterr. J. Chem. 2017, 6, 71–76. [Google Scholar]
- Rodzi, S.N.H.M.; Zuhailawati, H. The effects of processing techniques on magnesium-based composite. AIP Conf. Proc. 2016, 020022. [Google Scholar] [CrossRef] [Green Version]
- Ragurajan, D.; Satgunam, M.; Golieskardi, M.; Sankar, U.; Ng, A.M.H. The effect of titanium oxide and hydroxyapatite on the mechanical properties of wollastonite. Cogent. Eng. 2019, 6. [Google Scholar] [CrossRef]
- Chu, C.; Xue, X.; Zhu, J.; Yin, Z. Fabrication and characterization of titanium-matrix composite with 20 vol% hydroxyapatite for use as heavy load-bearing hard tissue replacement. J. Mater. Sci. Mater. Med. 2006, 17, 245–251. [Google Scholar] [CrossRef]
- Peñarrieta-Juanito, G.M.; Costa, M.; Cruz, M.; Miranda, G.; Henriques, B.; Marques, J.; Magini, R.; Mata, A.; Caramês, J.; Silva, F.; et al. Bioactivity of novel functionally structured titanium-ceramic composites in contact with human osteoblasts. J. Biomed. Mater. Res. Part. A 2018, 106, 1923–1931. [Google Scholar] [CrossRef] [PubMed]
- Limongi, T.; Tirinato, L.; Pagliari, F.; Giugni, A.; Allione, M.; Perozziello, G.; Candeloro, P.; Di Fabrizio, E. Fabrication and applications of micro/nanostructured devices for tissue engineering. Nano Micro Lett. 2017, 9, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bose, S.; Ke, D.; Sahasrabudhe, H.; Bandyopadhyay, A. Progress in materials science additive manufacturing of biomaterials. Prog. Mater. Sci. 2018, 93, 45–111. [Google Scholar] [CrossRef] [PubMed]
- Campoli, G.; Borleffs, M.S.; Amin Yavari, S.; Wauthle, R.; Weinans, H.; Zadpoor, A.A. Mechanical properties of open-cell metallic biomaterials manufactured using additive manufacturing. Mater. Des. 2013, 49, 957–965. [Google Scholar] [CrossRef]
- Melancon, D.; Bagheri, Z.S.; Johnston, R.B.; Liu, L.; Tanzer, M.; Pasini, D. Mechanical characterization of structurally porous biomaterials built via additive manufacturing: Experiments, predictive models, and design maps for load-bearing bone replacement implants. Acta Biomater. 2017, 63, 350–368. [Google Scholar] [CrossRef] [PubMed]
- Vlad, M.D.; Fernández Aguado, E.; Gómez González, S.; Ivanov, I.C.; Şindilar, E.V.; Poeată, I.; Iencean, A.Ş.; Butnaru, M.; Avădănei, E.R.; López, J.L. Novel titanium-apatite hybrid scaffolds with spongy bone-like micro architecture intended for spinal application: In vitro and in vivo study. Mater. Sci. Eng. C 2020, 110, 110658. [Google Scholar] [CrossRef]
- Jaiswal, S.; Kumar, R.M.; Gupta, P.; Kumaraswamy, M.; Roy, P.; Lahiri, D. Mechanical, corrosion and biocompatibility behaviour of Mg-3Zn-HA biodegradable composites for orthopaedic fixture accessories. J. Mech. Behav. Biomed. Mater. 2017. [Google Scholar] [CrossRef]
- Wang, Z.L.; He, R.Z.; Tu, B.; Cao, X.; He, J.S.; Xia, H.S.; Liang, C.; Zou, M.; Wu, S.; Wu, Z.J.; et al. Enhanced biocompatibility and osseointegration of calcium titanate coating on titanium screws in rabbit femur. J. Huazhong Univ. Sci. Technol. Med. Sci. 2017, 37, 362–370. [Google Scholar] [CrossRef]
- Lukaszewska-Kuska, M.; Wirstlein, P.; Majchrowski, R.; Dorocka-Bobkowska, B. Osteoblastic cell behaviour on modified titanium surfaces. Micron 2018, 105, 55–63. [Google Scholar] [CrossRef]
- Spoerke, E.D.; Murray, N.G.; Li, H.; Brinson, L.C.; Dunand, D.C.; Stupp, S.I. A bioactive titanium foam scaffold for bone repair. Acta Biomater. 2005, 1, 523–533. [Google Scholar] [CrossRef]
- Kohn, D.H.; Sarmadi, M.; Helman, J.I.; Krebsbach, P.H. Effects of pH on human bone marrow stromal cells in vitro: Implications for tissue engineering of bone. J. Biomed. Mater. Res. Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2001, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Bergsma, J.E.; Bruijn WCDe Rozema, F.R.; Bos, R.R.M.; Boering, G. Late degradation tissue response to poly ( L-lactide ) bone plates and screws. Biomaterials 1995, 16, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Li, J. Behaviour of titanium and titania-based ceramics In Vitro and In Vivo. Biomaterials 1993, 14, 1–3. [Google Scholar] [CrossRef]
- Fartash, B.; Liao, H.; Li, J.; Fouda, N.; Hermansson, L. Long-term evaluation of titania-based ceramics compared with commercially pure titanium in vivo. J. Mater. Sci. Mater. Med. 1995, 6, 451–454. [Google Scholar] [CrossRef]
- Road, P.; Sachlos, E.; Czernuszka, J.T. Making tissue engineering scaffolds work. Review on the application of solid freeform fabrication technology to the production of tissue engineering scaffolds. Eur. Cell Mater. 2003, 29–40. [Google Scholar] [CrossRef]
- Manivasagam, G.; Dhinasekaran, D.; Rajamanickam, A. Biomedical Implants: Corrosion and its Prevention—A Review. Recent Pat. Corosion Sci. 2010, 2, 40–54. [Google Scholar] [CrossRef] [Green Version]
- Oldani, C.; Dominguez, A.; Eli, T. Titanium as a biomaterial for implants. Recent Adv. Arthroplast. 2012, 218, 149–162. [Google Scholar]
- Stryker. AlloCraft CA Cervical Allograft Spacer. Available online: https://www.stryker.com/us/en/spine/products/allocraft-ca.html (accessed on 17 July 2020).
- Stryker. BIO Wedge. Available online: https://www.stryker.com/us/en/spine/products/bio-wedge.html (accessed on 17 July 2020).
- Stryker. ReUnion RSA. Available online: https://www.stryker.com/us/en/trauma-and-extremities/products/reunion-rsa.html (accessed on 17 July 2020).
- Stryker. ReUnion S Humeral Stem. Available online: https://www.stryker.com/us/en/trauma-and-extremities/products/ReUnion-S.html (accessed on 17 July 2020).
- Stryker. T2 Humeral Fractures Humeral Nailing System. Available online: https://www.stryker.com/us/en/trauma-and-extremities/products/t2-standard-humeral-nail.html (accessed on 17 July 2020).
- Zimmer Biomet. OsseoTi ® Porous Metal Technology. Available online: https://www.zimmerbiomet.com/medical-professionals/common/our-science/osseoti-porous-metal.html (accessed on 17 July 2020).
- Zimmer Biomet. Versa-Fx ® II Femoral Fixation. Available online: https://www.zimmerbiomet.com/medical-professionals/trauma/product/versa-fx-ii-femoral-fixation-system.html (accessed on 17 July 2020).
- Zimmer Biomet. NexGen ® Legacy ® Constrained Condylar Knee ( LCCK ) Tibial and Femoral Augments. Available online: https://www.zimmerbiomet.com/medical-professionals/knee/product/nexgen-lcck.html (accessed on 17 July 2020).
- Zimmer Biomet. Avenir ® Hip System Avenir Cementless Stem Surface Finish and Macro Structure Meant To Last. Available online: https://www.zimmerbiomet.com/content/dam/zimmer-biomet/medical-professionals/hip/avenir-hip-system/0725.1-GLBL-en%20Avenir%20Hip%20System_Brochure_FINAL.pdf (accessed on 2 December 2020).
- TrellOss TM -C Porous Ti Interbody System. Available online: https://www.zimmerbiomet.com/medical-professionals/spine/product/trelloss-ts-porous-ti-interbody-system.html (accessed on 2 December 2020).
- DePuy Synthes. ACTIS® Total Hip System. Available online: https://www.jnjmedicaldevices.com/en-EMEA/product/actis-total-hip-system (accessed on 17 July 2020).
- DePuy Synthes. ATTUNE ® Revision Knee System. Available online: https://www.jnjmedicaldevices.com/en-US/product/attune-revision-knee-system (accessed on 17 July 2020).
- DePuy Synthes. GLOBAL ® CAP Conservative Anatomic Prosthesis & GLOBAL ® CAP CTA TM Cu Tear Arthropathy Conservative Prosthesis Features. Available online: https://www.jnjmedicaldevices.com/en-US/product/globalr-cap-conservative-anatomic-prosthesis-globalr-cap-ctatm-cuff-tear-arthropathy (accessed on 17 July 2020).
- DePuy Synthes. SIGMA ® Total Knee System. Available online: https://www.jnjmedicaldevices.com/en-US/product/sigmar-total-knee-system (accessed on 2 December 2020).
- DePuy Synthes. PROTI 360° TM Ti Integrated Technology. Available online: https://www.jnjmedicaldevices.com/en-US/product/proti-360degtm-ti-integrated-technology (accessed on 17 July 2020).
- Smith and Nephew. Revision Hip System. Available online: https://www.smith-nephew.com/key-products/orthopaedic-reconstruction/redapt/ (accessed on 2 December 2020).
- Smith and Nephew. VERILAST ◊ Technology for Hips. Available online: https://www.smith-nephew.com/professional/products/all-products/verilast-technology/ (accessed on 17 July 2020).
- Smith and Nephew. POLAR3 ◊. Available online: https://www.smith-nephew.com/professional/products/all-products/polar3/ (accessed on 17 July 2020).
- Smith and Nephew. BIOSURE ◊ HA and PK. Available online: https://www.smith-nephew.com/new-zealand/advanced-surgical-devices/key-products/sports-medicine/biosure-ha-and-biosure-pk-interference-screws/ (accessed on 17 July 2020).
- Smith and Nephew. CARGEL ◊ Bioscaffold Proven Performance. Available online: https://www.smith-nephew.com/key-products/sports-medicine/bst-cargel/ (accessed on 17 July 2020).
- Elbuluk, A.M.; Old, A.B.; Bosco, J.A.; Schwarzkopf, R.; Iorio, R. Strategies for reducing implant costs in the revision total knee arthroplasty episode of care. Arthroplast. Today 2017, 3, 286–288. [Google Scholar] [CrossRef] [Green Version]
- Parikh, H.R.; O’Hara, N.; Levy, J.F.; Cunningham, B.P. Value denominator: The fundamentals of costing for orthopaedic surgeons. J. Orthop. Trauma 2019, 33, S56–S61. [Google Scholar] [CrossRef]
- Arliani, G.G.; Sabongi, R.G.; Batista, A.F.; Astur, D.C.; Falotico, G.G.; Cohen, M. Evaluation of the knowledge on cost of orthopedic implants among orthopedic surgeons. Acta Ortop. Bras. 2016, 24, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Xi’an Lyphar Biotech Co. Ltd. Lyphar Provide Most CAS NO 1306-06-5 Competitive Lyphar Provide Most CAS NO 1306-06-5 Competitive. Available online: https://www.cphi-online.com/xian-lyphar-biotech-co-ltd-comp266352.html (accessed on 18 July 2020).
- Xi’an Sgonek Biological Technology Co. Ltd. ISO Certificated Factory Supply CAS 1306-06-5 Calcium Hydroxyapatite Powder Hydroxyapatite. Available online: https://sgonekbio.en.alibaba.com/ (accessed on 18 July 2020).
- Shanghai Ximeng New Materials Technology Co. Ltd. Hydroxyapatite powder CAS. Available online: https://cnshximeng.en.alibaba.com/ (accessed on 18 July 2020).
- Richin International Trade (Dalian) Co. Ltd. Wollastonite Pictures of Wollastonite Product Description of Wollastonite. Available online: http://www.richase.com/ (accessed on 18 July 2020).
- Shanghai CNPC Powder Material Co. Ltd. Low Price Factory Supply Wollastonite Powder Price. Available online: https://cnpcpowder.en.made-in-china.com/ (accessed on 18 July 2020).
- Shenyang Huakuang Trading Co. Ltd. Wollastonite Provider. Available online: http://www.syhkmining.com/contactus (accessed on 17 July 2020).
- Wilson, N.A.; Schneller, E.S.; Montgomery, K.; Bozic, K.J. Hip and knee implants: Current trends and policy considerations. Health Aff. 2008, 27, 1587–1598. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metals | Advantages | Disadvantages |
|---|---|---|
| Titanium Alloy (Ti 6Al-4V) |
|
|
| Stainless Steel 316 |
| |
| Cobalt-Chromium | ||
| Nickel-Titanium(Nitinol) |
| |
| Niobium-Zirconium |
| |
| AZ91D |
|
| Ceramics | Advantages | Disadvantages |
|---|---|---|
| Hydroxyapatite | ||
| Tricalcium Phosphate |
| |
| 45S5 Bioglass | ||
| Wollastonite | ||
| Calcium Sulphate |
| |
| Calcium Carbonate |
|
| No | Articles (Database) | Type of Metal | Type of Ceramic | Methodology | Results | Conclusion |
|---|---|---|---|---|---|---|
| 1 | Spoerke 2005 (Scopus) | Commercially pure Titanium powders (particle size 130 µm) | Organoapatite (OA) which consists of hydroxyapatite mineral, which has been precipitated in the presence of macromolecules incorporating these macromolecules into the mineral phase. | Treatment Groups
|
| In vitro experiments in a rotating bioreactor demonstrated early colonization of organoapatite-coated titanium foams by preosteoblasts |
| 2 | Chu 2004 (Scopus) | Titanium alloy powder (Ti 99.3%, Fe 0.039%, O 0.35%, N 0.035%, C 0.025%, CL 0.034%, H 0.024%, and Si 0.0018%) with mean particle size of 45.2 µm | Hydroxyapatite powder prepared by the reaction between Ca(NO3)2 and (NH4)2HPO4. | Treatment Groups
|
| The most effective group of was the Titanium Hydroxyapatite (40% volume Hydroxyapattie and 60% volume Titanium) as it was proven to be effective in the in vivo study as no fibrous tissues came into being at the interface between the composite implant and newborn bones |
| 3 | Peñarrieta-Juanito 2018 (PubMed) | Commercially pure titanium Grade V | Hydroxyapatite and Beta Tricalcium Phosphate | Treatment Groups
|
| The titanium beta-tricalcium phosphate composite provided a higher viability and alkaline phosphatase activity with noticeable formation of mineral matrix when compared to commercially pure titanium containing or not containing hydroxyapatite |
| 4 | Ramli 2019 (Pubmed) | Titanium alloy(Ti6Al4V) powder | Wollastonite (CaSiO3) created from rice husk ash | Treatment Groups
|
| Titanium wollastonite composite fabricated at a sintering temperature of 1100 °C is biocompatible and contains bioactive properties for bone implant applications |
| Metals | Young’s Modulus | Compressive Strength | Tensile Strength |
|---|---|---|---|
| Titanium 6Al-4V [75] | 114 GPa | 1119 MPa | 940 MPa |
| Stainless Steel 316 [76] | 26.67 GPa | 110.33 MPa | 74.67 MPa |
| Cobalt-Chromium [75] | 283 GPa | 1976 MPa | 1403 MPa |
| Bone Type | Modulus of Elasticity (GPa) | Compressive Strengh | Tensile Strength |
|---|---|---|---|
| Cortical | 10–30 GPa [79] | 141.6 MPa [80] | 39.74 MPa [80] |
| Trabecular | 4.5–23.6 GPa [81] | 2.270 MPa [82] | 4.5 MPa [83] |
| Ceramic | Modulus of Elasticity | Compressive Strength | Tensile Strength |
|---|---|---|---|
| Hydroxyapatite [84] | 119.5 GPa | 520 MPa [85] | 190 MPa [85] |
| β-Tricalcium Phosphate [86] | 23 GPa | 159.4 MPa [87] | 0.17 MPa [88] |
| Wollastonite [89] | 23 GPa | 250 MPa | 7.4 MPa [90] |
| 45S5 Bioglass [91] | 78 GPa | 0.4 MPa | 0.011 MPa [92] |
| Titanium–Ceramic Type | Genetic Expression | Cellular Attachment and Proliferation |
|---|---|---|
| Titanium Pure21 | Large amounts of osteopontin were expressed initially, slowed overtime | Strong cell attachment weak proliferation |
| Titanium Hydroxyapaptite21 | Moderate amounts of osteopontin expressed initially; increased over time until the 21st day then reduced | Strong cell attachment and proliferation |
| Titanium Silicanite21 | Moderate osteopontin expressed; no gain or reduction overtime | Strong cell attachment and proliferation |
| Company Name | Targeted Customers | Product Examples | Material Composition |
|---|---|---|---|
| Stryker | Biomaterials, trauma and spinal implant sectors | AlloCraft CA [144], BIO Wedge [145], ReUnion RSA [146], ReUnion S [147], T2 Humeral [148] | Femoral Allograft (freeze dried), Ti6Al4V |
| Zimmer Biomet | Artificial knees, artificial hips, extremities, trauma products spine | OsseoTi® Porous Metal Tech [149], Versa-Fx® II Femoral Fixation [150], NexGen® Legacy® Constrained Condylar Knee (LCCK) [151], Avenir® Hip System [152], TrellOss™-C [153] | Ti6Al4V, Hydroxyapatitecoating, Cobalt-Chromium |
| DePuy Synthes | Arthroplasty, fixation, trauma and orthopedic solutions | ACTIS® Total Hip System [154], ATTUNE® Revision Knee System [155], GLOBAL® CAP Conservative Anatomic Prosthesis and GLOBAL® CAP CTA™ Cuff Tear Arthropathy Conservative Prosthesis [156], SIGMA® Total Knee System [157], PROTI 360°™ Ti Integrated Technology [158] | Ti6Al4V, Hydroxyapatite coating, Stainless Steel 316 L |
| Smith and Nephew | Hip and knee implants, | Redapt [159], Verilast [160], Polar3 [161], Biosure HA and PK [162], Cargel [163] | Ti6Al4V, Stainless Steel 316 L, Stainless Steel 304 L, Bone Allograft, Hydroxyapatite coating |
| Company Name | Cost per Kilogram |
|---|---|
| Xi’an Lyphar Biotech Co., Ltd. | US $30–350 [167] |
| Xi’an Sgonek Biological Technology Co., Ltd. | US $50–80 [168] |
| Shanghai Ximeng New Materials Technology Co., Ltd. | US $180–250 [169] |
| Company Name | Cost per Metric Tonne |
|---|---|
| Richin International Trade (Dalian) Co., Ltd. | US $120–140 [170] |
| Shanghai CNPC Powder Material Co., Ltd. | US $70–200 [171] |
| Shenyang Huakuang Trading Co., Ltd. | US $113–198 [172] |
| Index | Category of Patients | Mean Cost | Total |
|---|---|---|---|
| Cost | All Patients (n = 47) | $ 708.37 | $ 33,293.59 |
| Symptomatic (n = 6) | $ 613.15 | $ 3678.90 | |
| Cash that cannot be saved | $ 29,614.69 | ||
| Time Lost (Days) | All Patients (n = 47) | 15.4 | 723 |
| Symptomatic (n = 6) | 16.3 | 98 | |
| Time that cannot be saved (days) | 625 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shanmuganantha, L.; Baharudin, A.; Sulong, A.B.; Shamsudin, R.; Ng, M.H. Prospect of Metal Ceramic (Titanium-Wollastonite) Composite as Permanent Bone Implants: A Narrative Review. Materials 2021, 14, 277. https://doi.org/10.3390/ma14020277
Shanmuganantha L, Baharudin A, Sulong AB, Shamsudin R, Ng MH. Prospect of Metal Ceramic (Titanium-Wollastonite) Composite as Permanent Bone Implants: A Narrative Review. Materials. 2021; 14(2):277. https://doi.org/10.3390/ma14020277
Chicago/Turabian StyleShanmuganantha, Lohashenpahan, Azmi Baharudin, Abu Bakar Sulong, Roslinda Shamsudin, and Min Hwei Ng. 2021. "Prospect of Metal Ceramic (Titanium-Wollastonite) Composite as Permanent Bone Implants: A Narrative Review" Materials 14, no. 2: 277. https://doi.org/10.3390/ma14020277