Evaluation of Bone Regeneration in Rat Calvaria Using Bone Autologous Micrografts and Xenografts: Histological and Histomorphometric Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Model
2.2. Experimental Groups
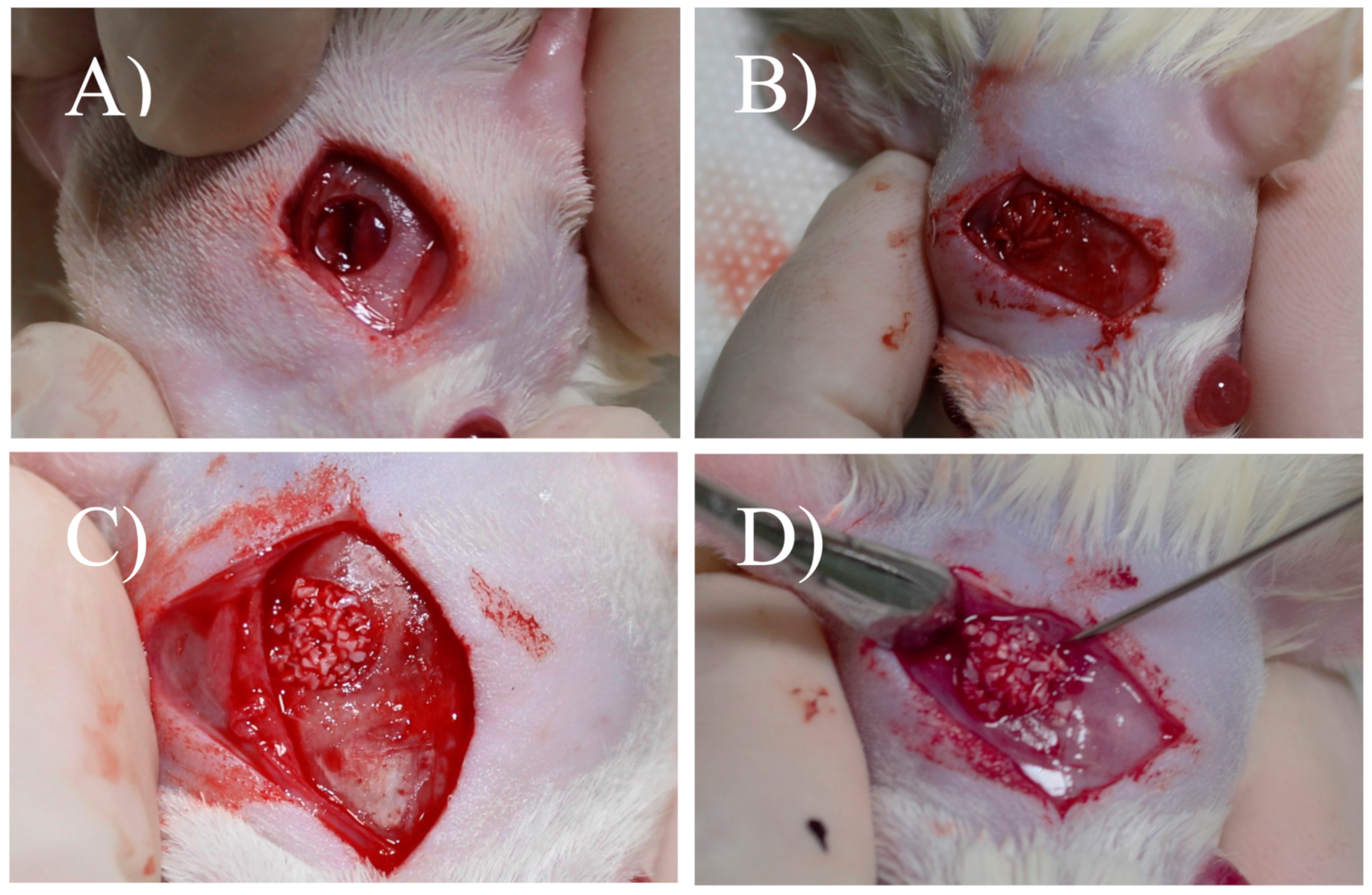
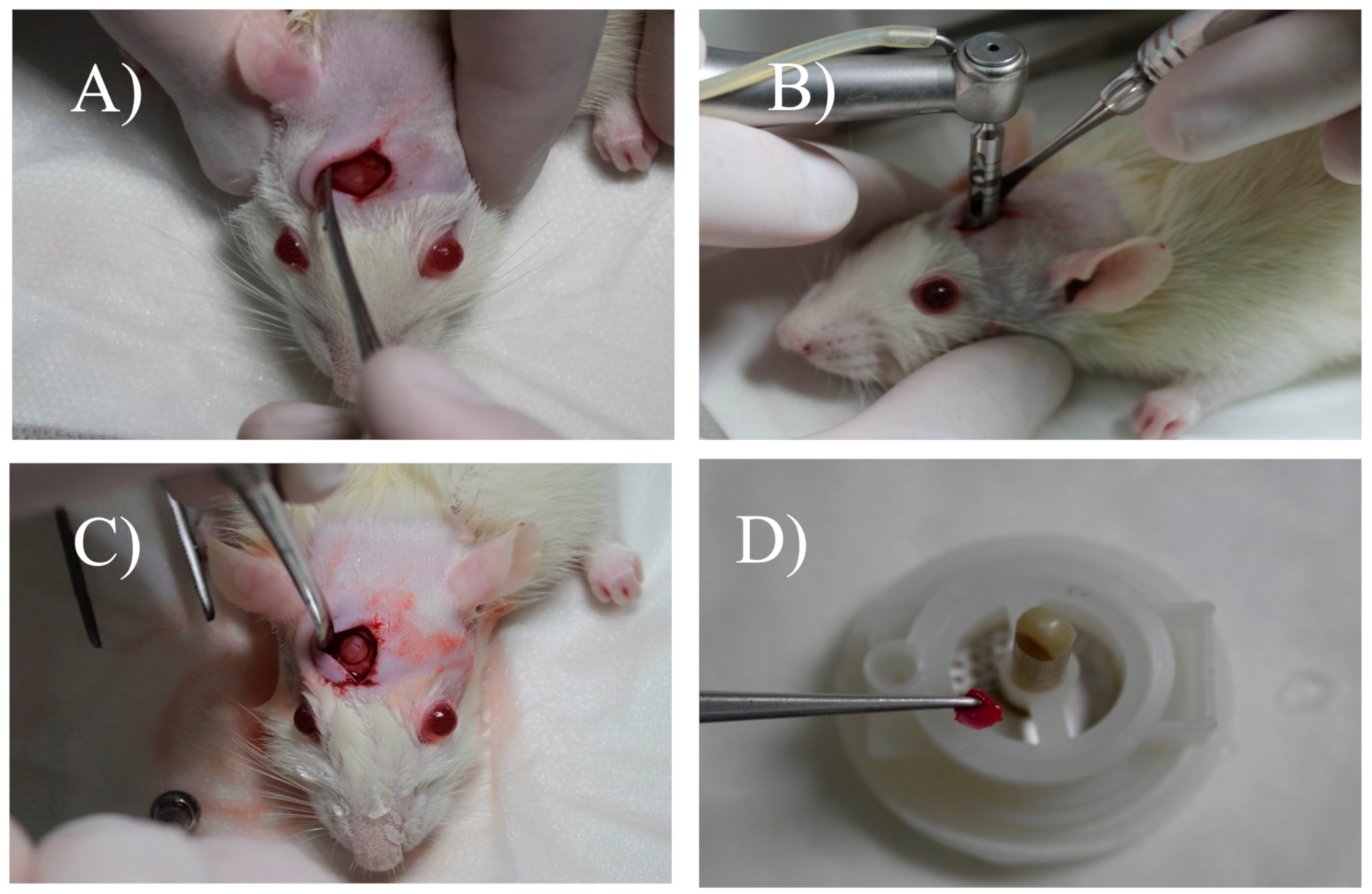
2.3. Surgical Procedure and Defect Management
2.4. Painless Induced Death
2.5. Material Processing
2.6. Histological and Histomorphometric Analysis
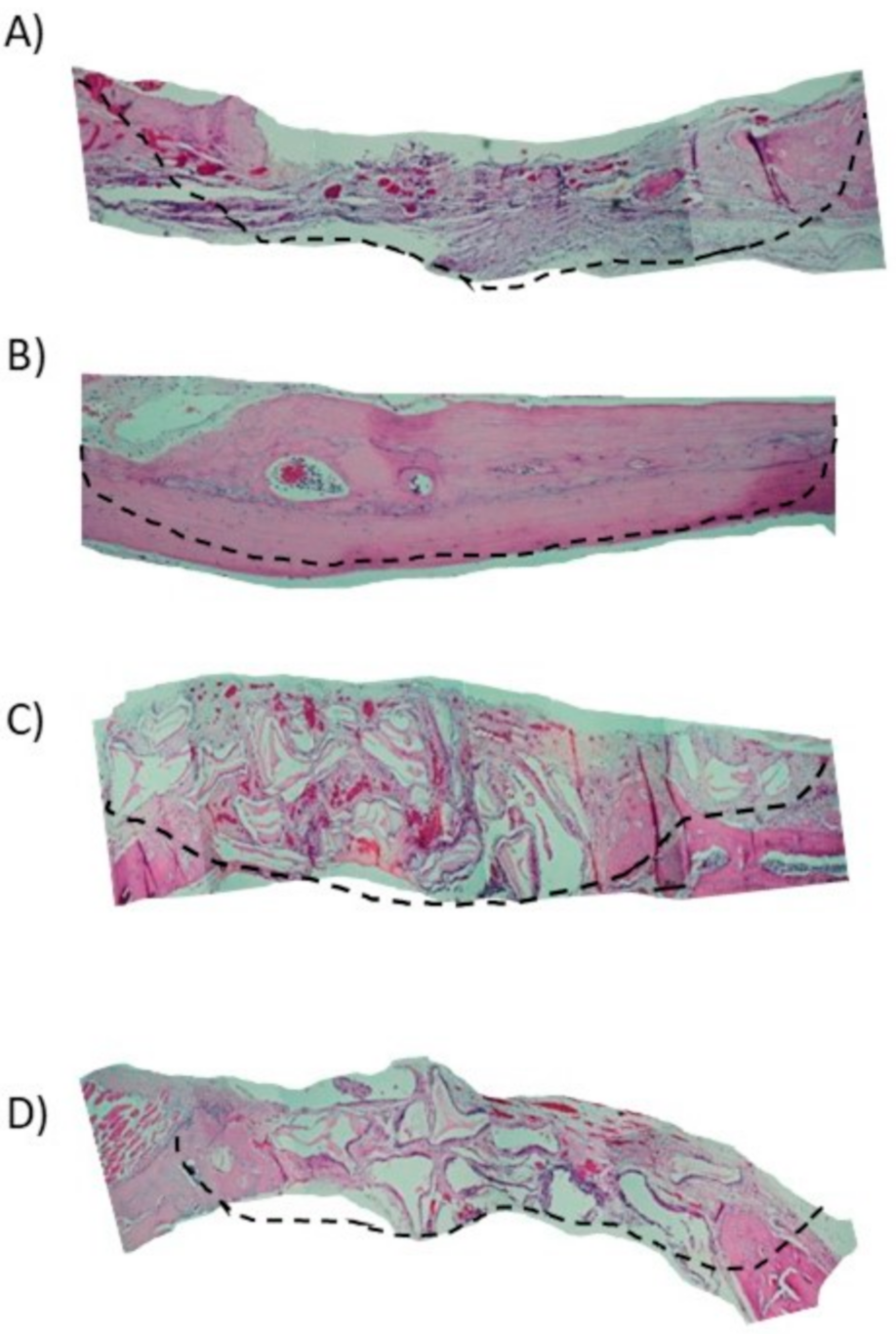
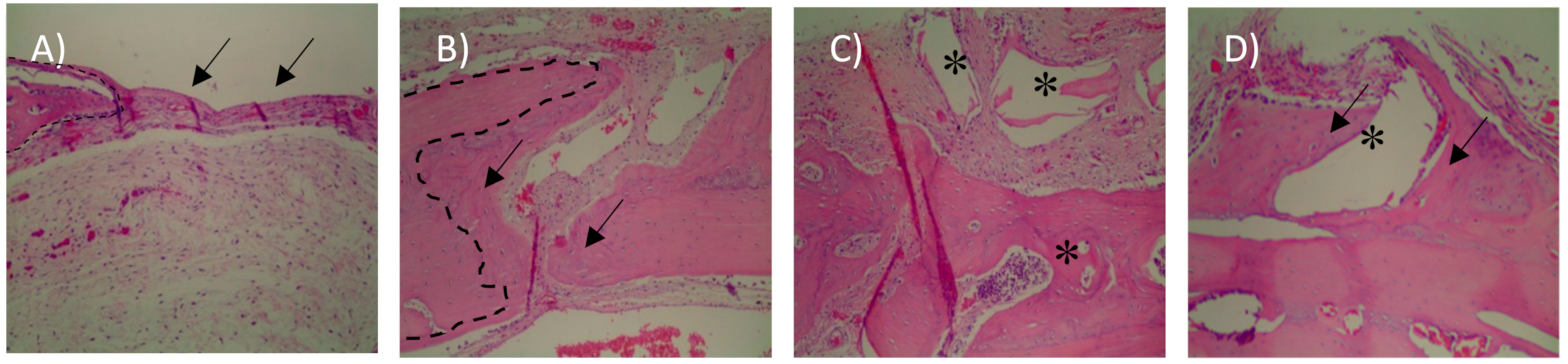
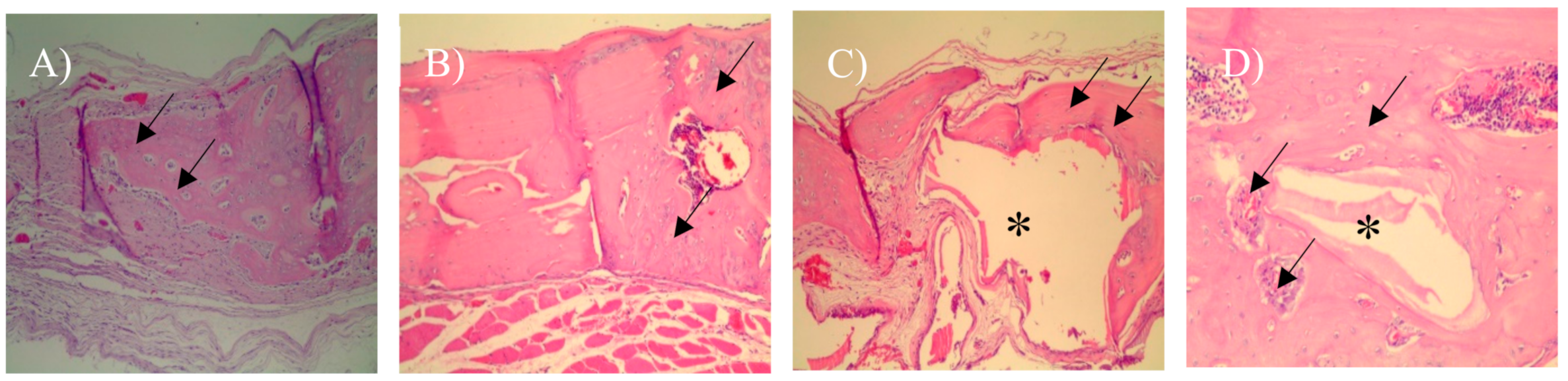
- Vital mineralized tissue (VMT), are characterized by the presence of a mineral phase, responsible for rigidity and hardness. VMT represents newly formed bone, so the higher the VMT the level means that we have a quantity of newly formed bone. In histological slides, where the presence of viable cells associated with mineralized tissue was observed, bone tissue was defined as VMT.
- Non-vital mineralized tissue (NVMT) was defined as xenograft particles (Bio-Oss) defined by polyhedral shapes, without the presence of viable cells and some indicating osseoconduction, High levels of NVMT represent high levels of xenograft remnants.
- Non-mineralized tissue (NMT) was characterized by granulation tissue and connective tissue, so it can be inferred that high levels of NMT are related to low levels of mineralization.
3. Results
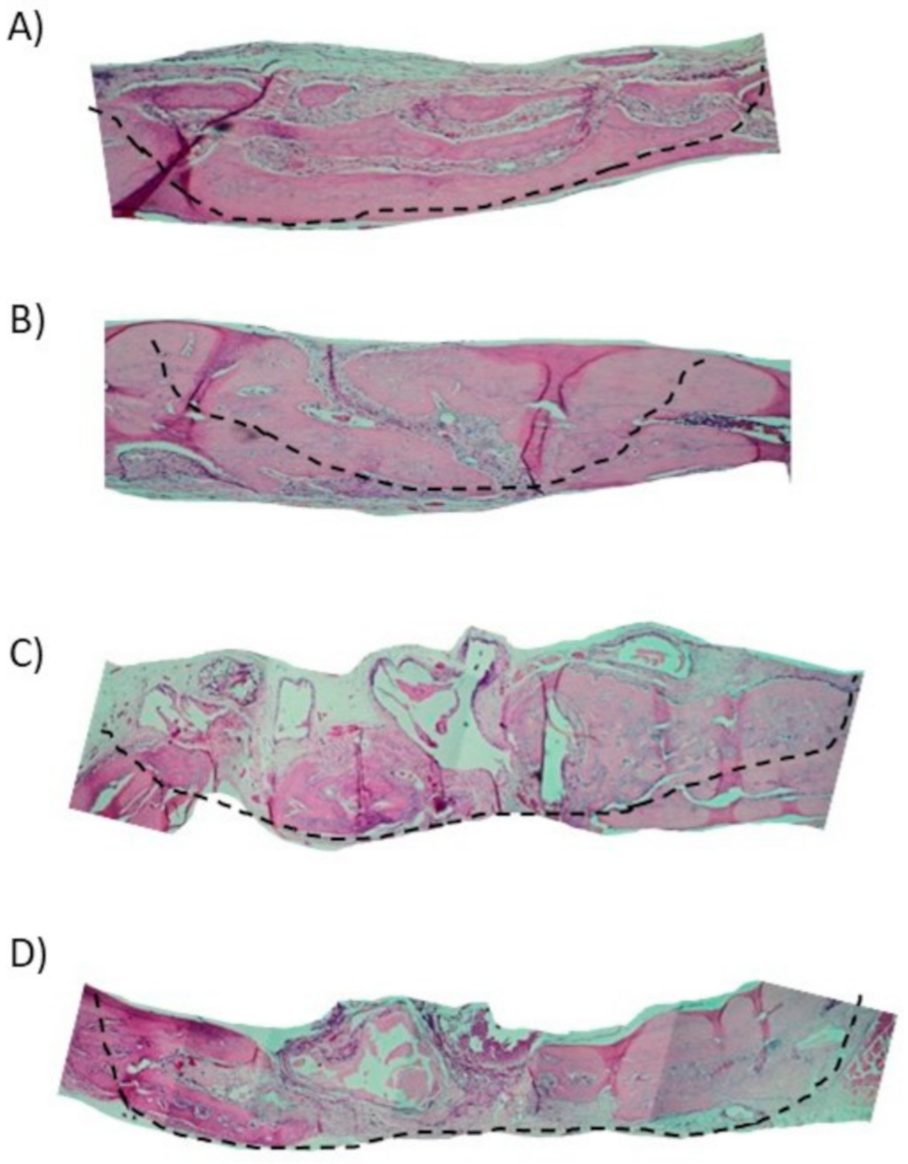
3.1. Histological Analysis
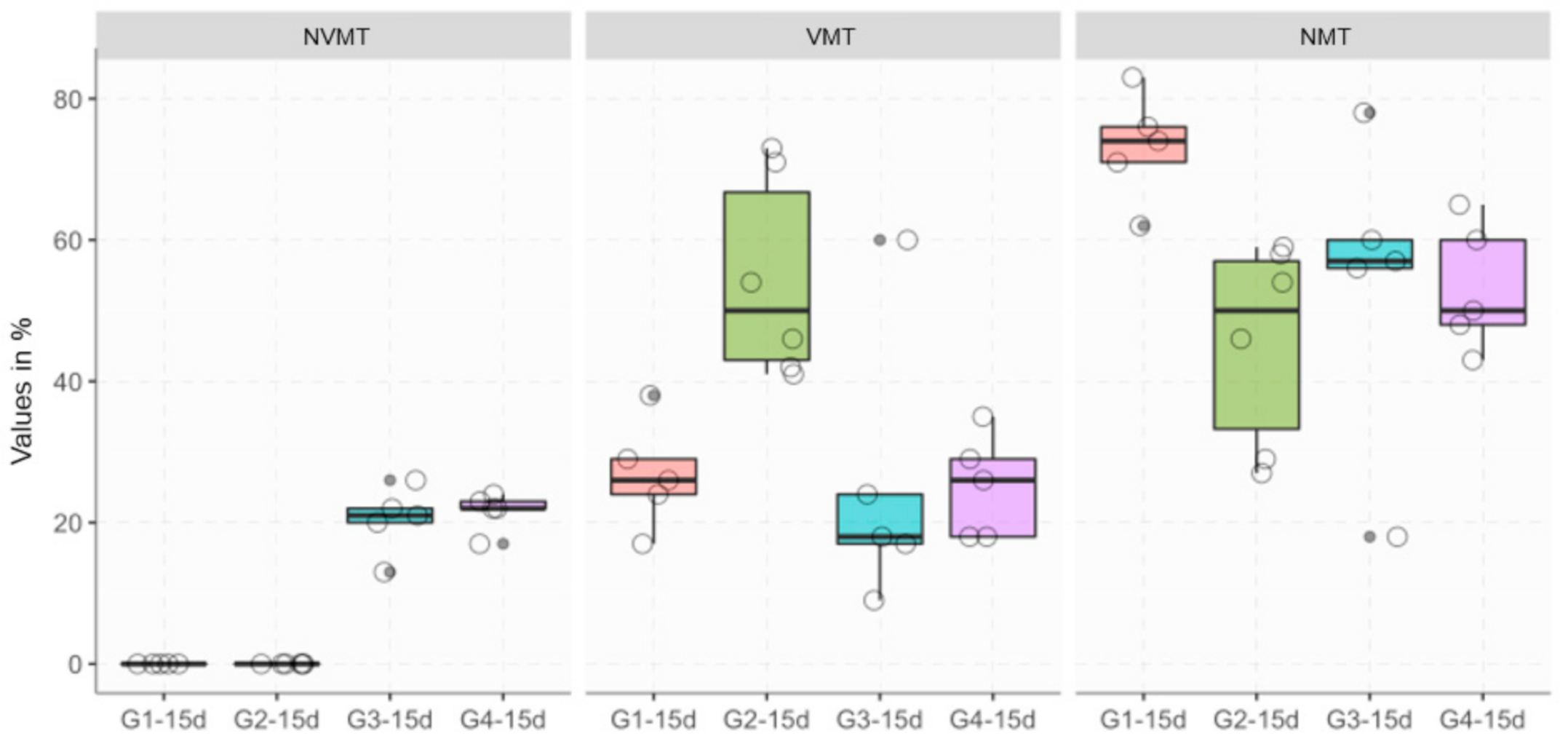
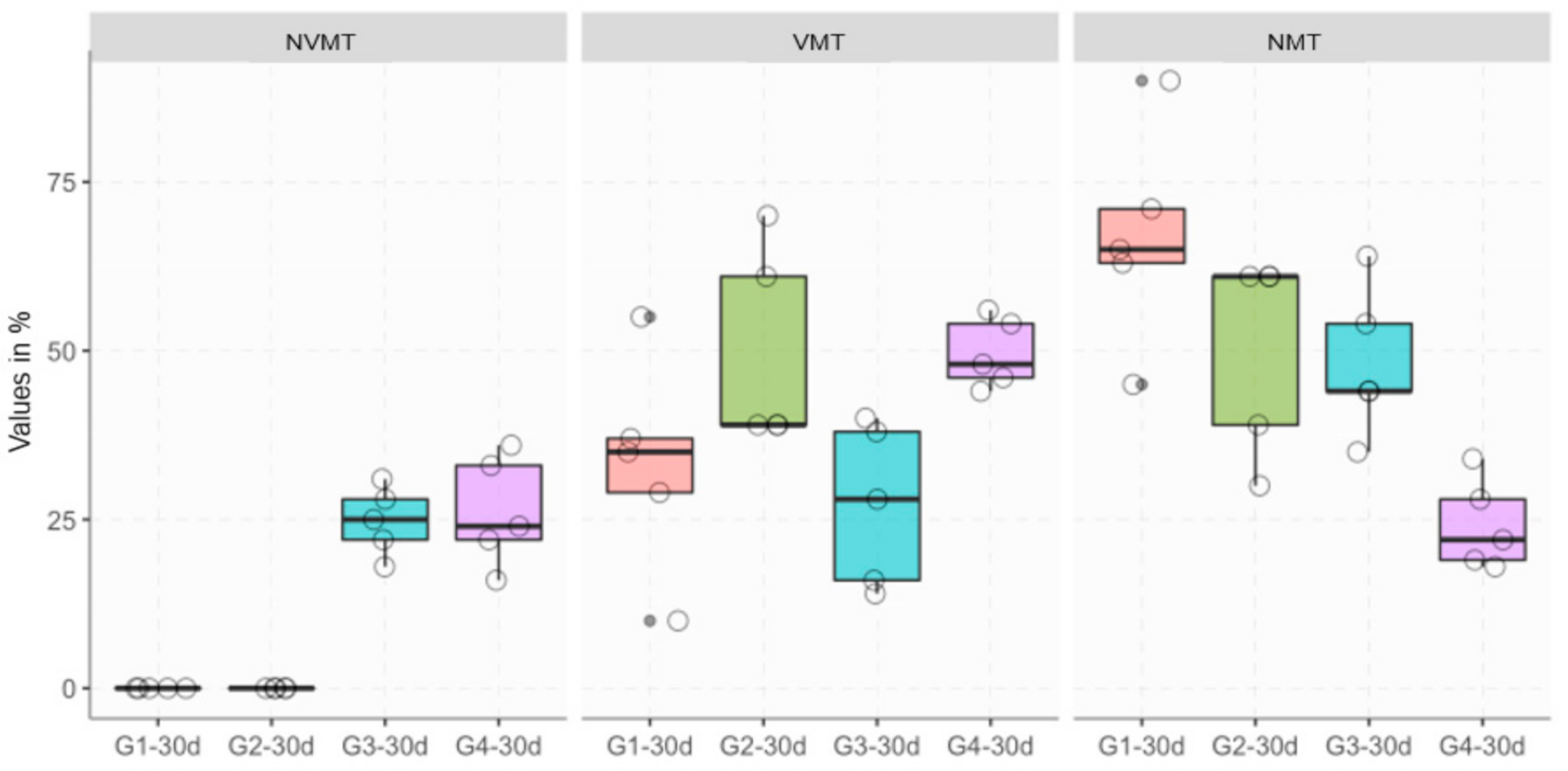
3.2. Histomorphometric Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Yamada, M.; Egusa, H. Current bone substitutes for implant dentistry. J. Prosthodont. Res. 2018, 62, 152–161. [Google Scholar] [CrossRef] [PubMed]
- E Keller, E.; E Tolman, D.; Eckert, S. Surgical-prosthodontic reconstruction of advanced maxillary bone compromise with autogenous onlay block bone grafts and osseointegrated endosseous implants: A 12-year study of 32 consecutive patients. Int. J. Oral Maxillofac. Implant. 1999, 14, 197–209. [Google Scholar]
- Gassling, V.; Purcz, N.; Braesen, J.-H.; Will, M.; Gierloff, M.; Behrens, E.; Açil, Y.; Wiltfang, J. Comparison of two different absorbable membranes for the coverage of lateral osteotomy sites in maxillary sinus augmentation: A preliminary study. J. Cranio-Maxillofac. Surg. 2013, 41, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.-J.; Kwon, T.-K.; Baek, H.-S.; Hwang, D.-S.; Kim, C.-H.; Chung, I.-K.; Jeong, J.-S.; Shin, S.-H. A comparative study of the effectiveness of sinus bone grafting with recombinant human bone morphogenetic protein 2–coated tricalcium phosphate and platelet-rich fibrin–mixed tricalcium phosphate in rabbits. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Trovato, L.; Monti, M.; Del Fante, C.; Cervio, M.; Lampinen, M.; Ambrosio, L.; Redi, C.A.; Perotti, C.; Kankuri, E.; Ambrosio, G.; et al. A New Medical Device Rigeneracons Allows to Obtain Viable Micro-Grafts From Mechanical Disaggregation of Human Tissues. J. Cell. Physiol. 2015, 230, 2299–2303. [Google Scholar] [CrossRef] [PubMed]
- Carinci, F.; Motroni, A.; Graziano, A.; Zollino, I.; Brunelli, G.; D’Aquino, R. Sinus lift tissue engineering using autologous pulp micro-grafts: A case report of bone density evaluation. J. Indian Soc. Periodontol. 2013, 17, 644–647. [Google Scholar] [CrossRef]
- Graziano, A.; Carinci, F.; Scolaro, S. Periodontal tissue generation using autologous dental ligament micro-grafts: Case report with 6 months follow-up. Ann. Oral Maxillofac. Surg. 2013, 1, 20. [Google Scholar] [CrossRef]
- D’Aquino, R.; Trovato, L.; Graziano, A.; Ceccarelli, G.; De Angelis, G.C.; Marangini, A.; Nisio, A.; Galli, M.; Pasi, M.; Finotti, M.; et al. Periosteum-derived micro-grafts for tissue regeneration of human maxillary bone. J. Transl. Sci. 2016, 2, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Baena, R.R.Y.; D’Aquino, R.; Graziano, A.; Trovato, L.; Aloise, A.C.; Ceccarelli, G.; Cusella, G.; Pelegrine, A.A.; Lupi, S.M. Autologous Periosteum-Derived Micrografts and PLGA/HA Enhance the Bone Formation in Sinus Lift Augmentation. Front. Cell Dev. Biol. 2017, 5, 87. [Google Scholar] [CrossRef] [Green Version]
- Mummolo, S.; Mancini, L.; Quinzi, V.; D’Aquino, R.; Marzo, G.; Marchetti, E. Rigenera® Autologous Micrografts in Oral Regeneration: Clinical, Histological, and Radiographical Evaluations. Appl. Sci. 2020, 10, 5084. [Google Scholar] [CrossRef]
- Purpura, V.; Bondioli, E.; Graziano, A.; Trovato, L.; Melandri, D.; Ghetti, M.; Marchesini, A.; De Angelis, M.G.C.; Benedetti, L.; Ceccarelli, G.; et al. Tissue Characterization after a New Disaggregation Method for Skin Micro-Grafts Generation. J. Vis. Exp. 2016, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monti, M.; Graziano, A.; Rizzo, S.; Perotti, C.; Del Fante, C.; D’Aquino, R.; Redi, C.A.; Baena, R.R.Y. In Vitro and In Vivo Differentiation of Progenitor Stem Cells Obtained After Mechanical Digestion of Human Dental Pulp. J. Cell. Physiol. 2016, 232, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Melo, L.G.N.; Nagata, M.J.H.; Bosco, A.F.; Ribeiro, L.L.G.; Leite, C. Bone healing in surgically created defects treated with either bioactive glass particles, a calcium sulfate barrier, or a combination of both materials. Clin. Oral Implant. Res. 2005, 16, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Messora, M.R.; Nagata, M.J.H.; Mariano, R.C.; Dornelles, R.C.M.; Bomfim, S.R.M.; Fucini, S.E.; Garcia, V.G.; Bosco, A.F. Bone healing in critical-size defects treated with platelet-rich plasma: a histologic and histometric study in rat calvaria. J. Periodontal Res. 2008, 43, 217–223. [Google Scholar] [CrossRef]
- D’Aquino, R.; De Rosa, A.; Laino, G.; Caruso, F.; Guida, L.; Rullo, R.; Checchi, V.; Laino, L.; Tirino, V.; Papaccio, G. Human dental pulp stem cells: from biology to clinical applications. J. Exp. Zool. Part B Mol. Dev. Evol. 2009, 312, 408–415. [Google Scholar] [CrossRef]
- Jimi, S.; Kimura, M.; De Francesco, F.; Riccio, M.; Hara, S.; Ohjimi, H. Acceleration Mechanisms of Skin Wound Healing by Autologous Micrograft in Mice. Int. J. Mol. Sci. 2017, 18, 1675. [Google Scholar] [CrossRef]
- Marcarelli, M.; Trovato, L.; Novarese, E.; Riccio, M.; Graziano, A. Rigenera protocol in the treatment of surgical wound dehiscence. Int. Wound J. 2016, 14, 277–281. [Google Scholar] [CrossRef]
- Baglioni, E.; Trovato, L.; Marcarelli, M.; Frenello, A.; Bocchiotti, M.A. Treatment of Oncological Post-surgical Wound Dehiscence with Autologous Skin Micrografts. Anticancer. Res. 2016, 36, 975–980. [Google Scholar]
- Giaccone, M.; Trovato, L.; Graziano, A. A new medical device, based on rigenera protocol, in the management of complex wounds. J. Stem Cells Res. 2014, 1, 1013. [Google Scholar]
- Riccio, M.; Marchesini, A.; Zingaretti, N.; Carella, S.; Senesi, L.; Onesti, M.G.; Parodi, P.C.; Ribuffo, D.; Vaienti, L.; De Francesco, F. A Multicentre Study: The Use of Micrografts in the Reconstruction of Full-Thickness Posttraumatic Skin Defects of the Limbs—A Whole Innovative Concept in Regenerative Surgery. Stem Cells Int. 2019, 2019, 1–10. [Google Scholar] [CrossRef]
- De Francesco, F.; Graziano, A.; Trovato, L.; Ceccarelli, G.; Romano, M.; Marcarelli, M.; De Angelis, G.M.C.; Cillo, U.; Riccio, M.; Ferraro, G.A. A Regenerative Approach with Dermal Micrografts in the Treatment of Chronic Ulcers. Stem Cell Rev. Rep. 2017, 13, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Andreone, A.; Hollander, D.D. A Retrospective Study on the Use of Dermis Micrografts in Platelet-Rich Fibrin for the Resurfacing of Massive and Chronic Full-Thickness Burns. Stem Cells Int. 2019, 2019, 8636079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svolacchia, F.; De Francesco, F.; Trovato, L.; Graziano, A.; Ferraro, G.A. An innovative regenerative treatment of scars with dermal micrografts. J. Cosmet. Dermatol. 2016, 15, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, R.G.; Rosell, J.M.C.; Ceccarelli, G.; De Sio, C.; De Angelis, G.C.; Pinto, H.; Astarita, C.; Graziano, A. Progenitor-cell-enriched micrografts as a novel option for the management of androgenetic alopecia. J. Cell. Physiol. 2019, 235, 4587–4593. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, X.; Valenzuela, M.; Tuffet, J. Clinical and Histological Evaluation of the Regenera® Method for the Treatment of Androgenetic Alopecia. Int. Educ. Appl. Sci. Res. J. 2018, 3, 2456–5040. [Google Scholar]
- Viganò, M.; Tessaro, I.; Trovato, L.; Colombini, A.; Scala, M.; Magi, A.; Toto, A.; Peretti, G.M.; De Girolamo, L. Rationale and pre-clinical evidences for the use of autologous cartilage micrografts in cartilage repair. J. Orthop. Surg. Res. 2018, 13, 279. [Google Scholar] [CrossRef] [Green Version]
- Fernández, A.D. Biostimulation of Knee Cartilage Using Autologous Micro-Grafts: A Preliminary Study of the Rigenera Protocol in Osteochondral Lesions of the Knee. Rehabilitation Sci. 2018, 3, 8. [Google Scholar] [CrossRef]
- Marcarelli, M.; Fiammengo, M.; Trovato, L.; Lancione, V.; Novarese, E.; Indelli, P.F.; Risitano, S. Autologous grafts in the treatment of avascular osteonecrosis of the femoral head. Acta Biomed. Atenei Parm. 2020, 91, 342–349. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | NVMT 15 Days | VMT 15 Days | NMT 15 Days | NVMT 30 Days | VMT 30 Days | NMT 30 Days |
|---|---|---|---|---|---|---|
| G1 | 0.00 ± 0.00 | 26.80 ± 07.66 | 73.20 ± 7.66 | 0.00 ± 0.00 | 33.20 ± 16.19 | 66.80 ± 16.19 |
| G2 | 0.00 ± 0.00 | 54.50 ± 14.32 | 45.50 ± 14.32 | 0.00 ± 0.00 | 49.60 ± 14.86 | 50.40 ± 14.86 |
| G3 | 20.40 ± 4.72 | 25.60 ± 19.96 | 53.80 ± 21.91 | 24.80 ± 5.07 | 27.20 ± 12.05 | 48.20 ± 11.10 |
| G4 | 21.60 ± 2.70 | 25.20 ± 7.33 | 53.80 ± 9.04 | 26.20 ± 8.20 | 49.60 ± 5.18 | 24.20 ± 6.72 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araùjo, C.R.G.; Astarita, C.; D'Aquino, R.; Pelegrine, A.A. Evaluation of Bone Regeneration in Rat Calvaria Using Bone Autologous Micrografts and Xenografts: Histological and Histomorphometric Analysis. Materials 2020, 13, 4284. https://doi.org/10.3390/ma13194284
Araùjo CRG, Astarita C, D'Aquino R, Pelegrine AA. Evaluation of Bone Regeneration in Rat Calvaria Using Bone Autologous Micrografts and Xenografts: Histological and Histomorphometric Analysis. Materials. 2020; 13(19):4284. https://doi.org/10.3390/ma13194284
Chicago/Turabian StyleAraùjo, Carlos R. G., Carlo Astarita, Riccardo D'Aquino, and André A. Pelegrine. 2020. "Evaluation of Bone Regeneration in Rat Calvaria Using Bone Autologous Micrografts and Xenografts: Histological and Histomorphometric Analysis" Materials 13, no. 19: 4284. https://doi.org/10.3390/ma13194284