Three-Dimensional Evaluation of Maxillary Sinus Changes in Growing Subjects: A Retrospective Cross-Sectional Study

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection and Inclusion Criteria
- Growing patients,
- Caucasian patients.
- pathological conditions affecting the maxillary sinuses (fracture, inflammation, residual root fragments, extrusion of endodontic filling materials),
- missing teeth in maxillary posterior regions,
- history of orthodontic treatment,
- metabolic diseases affecting bone tissue,
- skeletal asymmetry,
- congenital disorders,
- craniofacial syndromes.
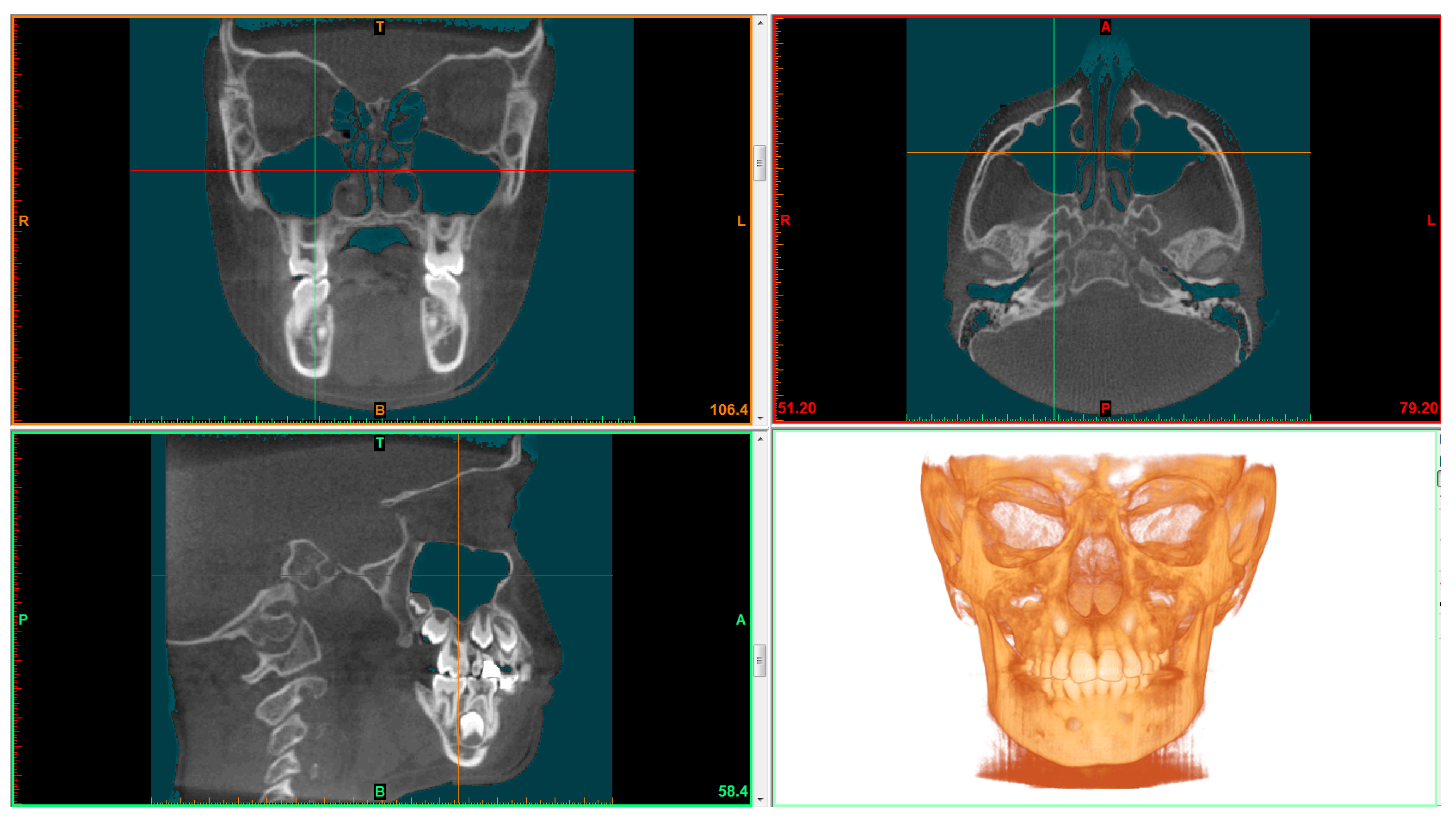
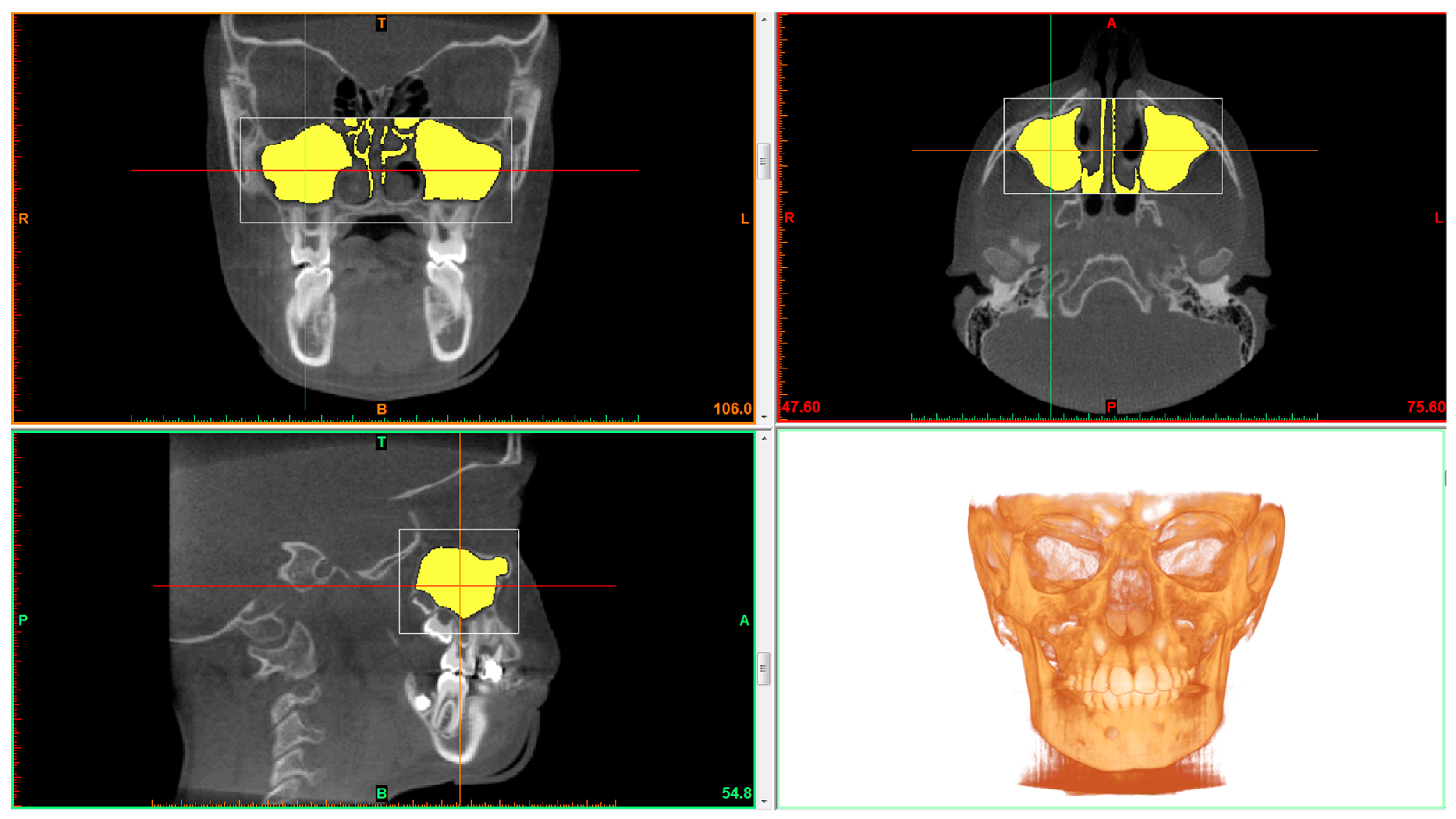
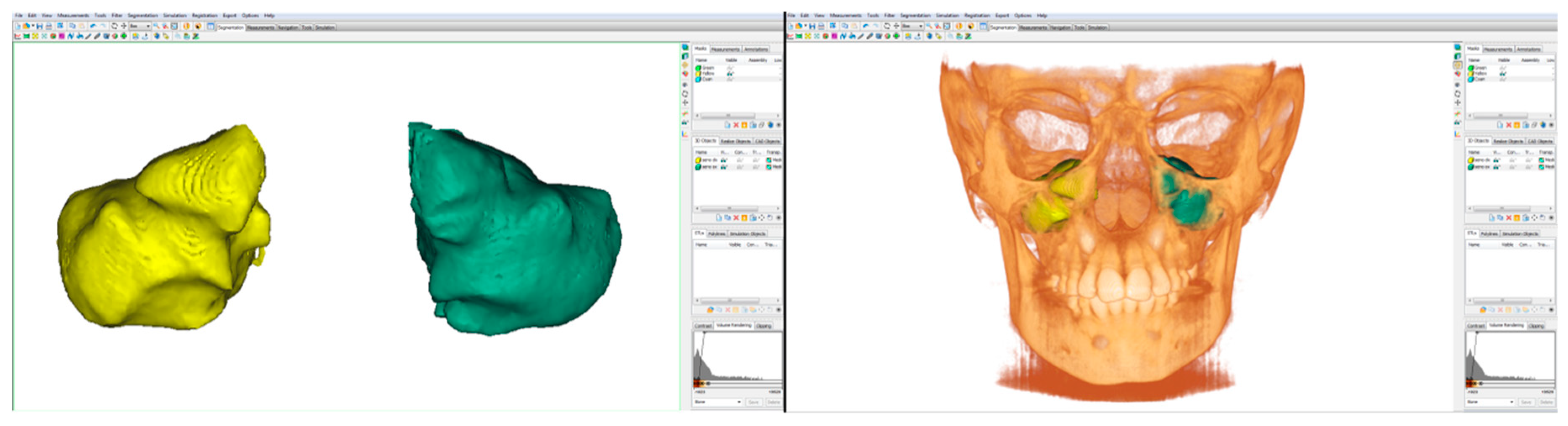
2.2. CBCT Examination and Data Processing
2.3. Statistical Analysis
2.4. Method Error
3. Results
3.1. Comparisons Whithin Groups between Genders
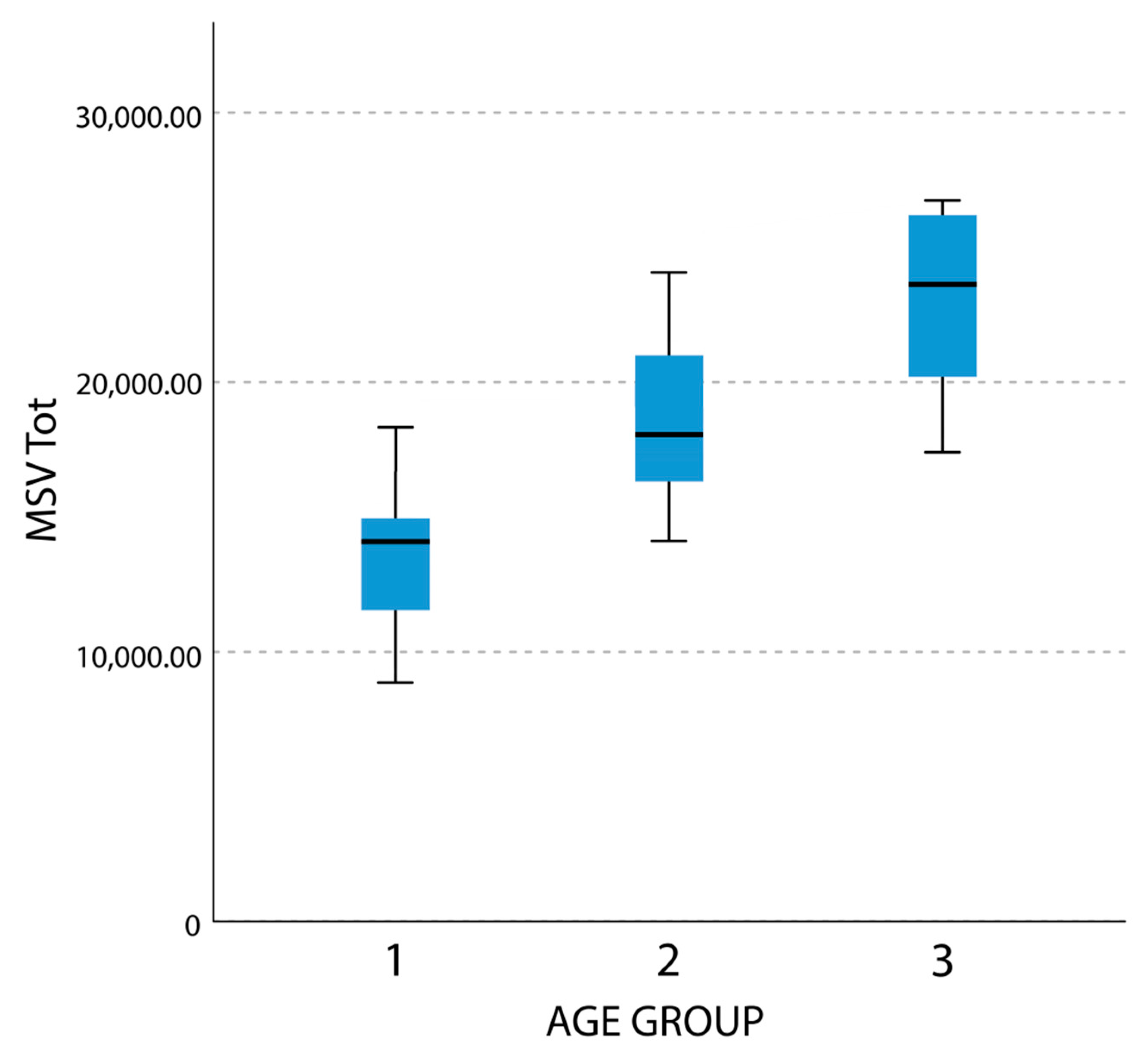
3.1.1. Maxillary Sinus Volume (MSV)
3.1.2. Maxillary Sinus Surface (MSS)
3.1.3. Linear Maximum Width (LMW)
3.1.4. Linear Maximum Depth (LMD)
3.1.5. Linear Maximum Height (LMH)
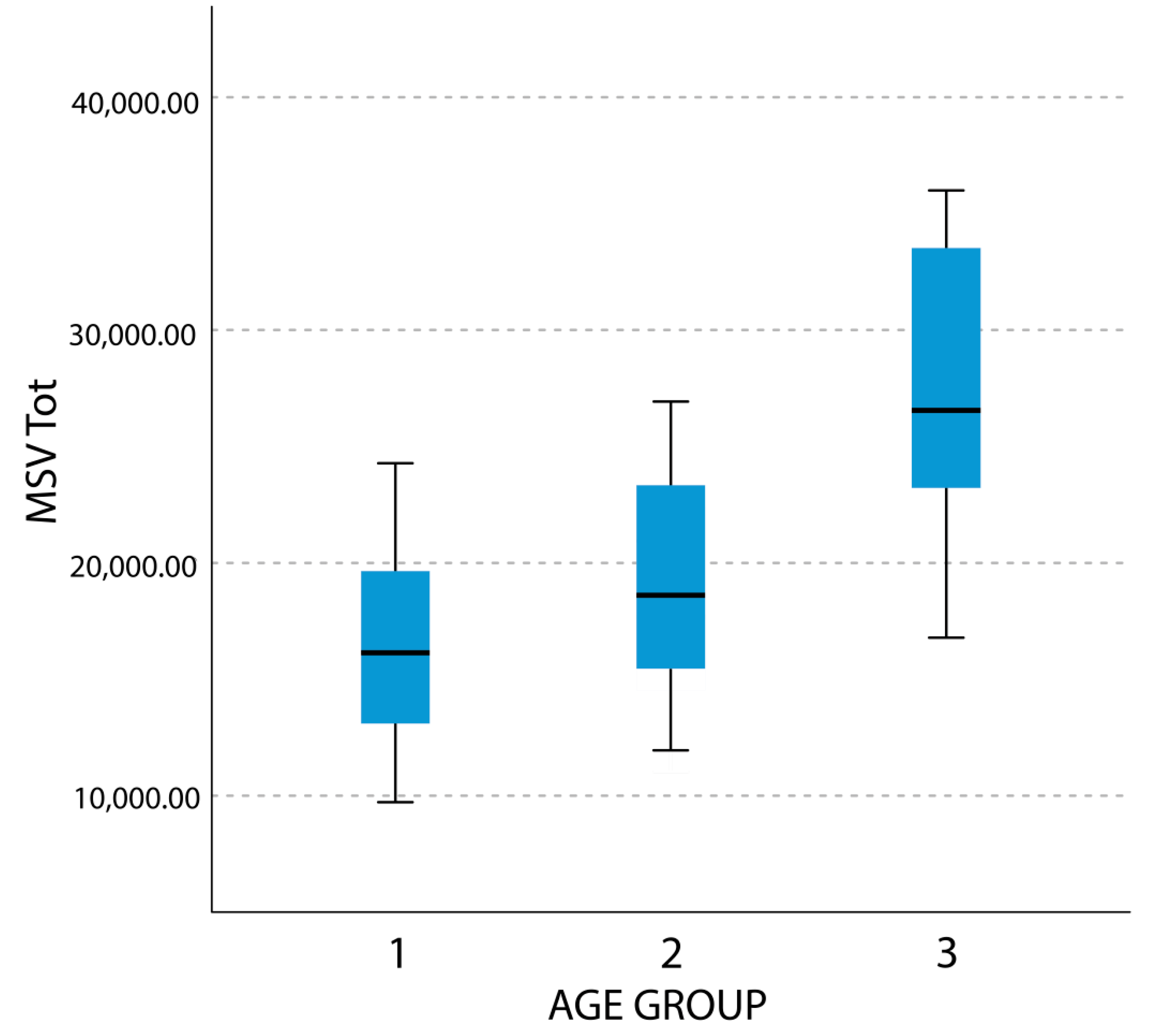
3.2. Comparisons whithin Gender between Age Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Emirzeoglu, M.; Sahin, B.; Bilgic, S.; Çelebi, M.; Uzun, A. Volumetric evaluation of the paranasal sinuses in normal subjects using computer tomography images: A stereological study. Auris Nasus Larynx 2007, 34, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Oktay, H. The study of the maxillary sinus areas in different orthodontic malocclusions. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 143–145. [Google Scholar] [CrossRef]
- Scuderi, A.J.; Harnsberger, H.R.; Boyer, R.S. Pneumatization of the paranasal sinuses: Normal features of importance to the accurate interpretation of CT scans and MR images. Am. J. Roentgenol. 1993, 160, 1101–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endo, T.; Abe, R.; Kuroki, H.; Kojima, K.; Oka, K.; Shimooka, S. Cephalometric evaluation of maxillary sinus sizes in different malocclusion classes. Odontology 2010, 98, 65–72. [Google Scholar] [CrossRef]
- Livas, C.; Halazonetis, D.J.; Booij, J.W.; Pandis, N.; Tu, Y.-K.; Katsaros, C. Maxillary sinus floor extension and posterior tooth inclination in adolescent patients with Class II Division 1 malocclusion treated with maxillary first molar extractions. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 479–485. [Google Scholar] [CrossRef]
- Tikku, T.; Khanna, R.; Sachan, K.; Srivastava, K.; Munjal, N. Dimensional changes in maxillary sinus of mouth breathers. J. Oral Boil. Craniofacial Res. 2012, 3, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Maresh, M. Paranasal Sinuses from Birth to Late Adolescence. I. Size of the Paranasal Sinuses as Observed in Routine Posteroanterior Roentograms. Am. J. Dis. Child. 1940, 60, 55–78. [Google Scholar] [CrossRef]
- Koymen, R.; Karacayli, U.; Ortakoglu, K.; Özen, T.; Yazici, A.C.; Gocmen-Mas, N. Anatomic evaluation of maxillary sinus septa: Surgery and radiology. Clin. Anat. 2009, 22, 563–570. [Google Scholar] [CrossRef]
- Fernández, J.A.A.J.M.S. Morphometric Study of the Paranasal Sinuses in Normal and Pathological Conditions. Acta Oto-Laryngologica 2000, 120, 273–278. [Google Scholar] [CrossRef]
- Uchida, Y.; Goto, M.; Katsuki, T.; Akiyoshi, T. A cadaveric study of maxillary sinus size as an aid in bone grafting of the maxillary sinus floor. J. Oral Maxillofac. Surg. 1998, 56, 1158–1163. [Google Scholar] [CrossRef]
- Kanthem, R.K.; Guttikonda, V.R.; Yeluri, S.; Kumari, G. Sex determination using maxillary sinus. J. Forensic Dent. Sci. 2015, 7, 163–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farronato, M.; Cavagnetto, D.; Abate, A.; Cressoni, P.; Fama, A.; Maspero, C. Assessment of condylar volume and ramus height in JIA patients with unilateral and bilateral TMJ involvement: Retrospective case-control study. Clin. Oral Investig. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, H.A.R.; Andrade, M.E.A.; Ramos-Perez, F.; Freitas, D.Q.; Frazão, M.A.G.; Nascimento, E. Dosimetry in CBCT with Different Protocols: Emphasis on Small FOVs Including Exams for TMJ. Braz. Dent. J. 2017, 28, 511–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauwels, R. Cone beam CT for dental and maxillofacial imaging: Dose matters: Table 1. Radiat. Prot. Dosim. 2015, 165, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Szabó, B.T.; Aksoy, S.; Répassy, G.; Csomo, K.; Dobo-Nagy, C.; Orhan, K. Comparison of Hand and Semiautomatic Tracing Methods for Creating Maxillofacial Artificial Organs using Sequences of Computed Tomography (CT) and Cone Beam Computed Tomography (CBCT) Images. Int. J. Artif. Organs 2017, 40, 307–312. [Google Scholar] [CrossRef]
- Panou, E.; Motro, M.; Ateş, M.; Acar, A.; Erverdi, N. Dimensional changes of maxillary sinuses and pharyngeal airway in Class III patients undergoing bimaxillary orthognathic surgery. Angle Orthod. 2013, 83, 824–831. [Google Scholar] [CrossRef]
- Sahlstrand-Johnson, P.; Jannert, M.; Strömbeck, A.; Abul-Kasim, K. Computed tomography measurements of different dimensions of maxillary and frontal sinuses. BMC Med. Imaging 2011, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Favato, M.N.; Vidigal, B.C.; Cosso, M.G.; Manzi, F.R.; Shibli, J.A.; Zenóbio, E.G. Impact of human maxillary sinus volume on grafts dimensional changes used in maxillary sinus augmentation: A multislice tomographic study. Clin. Oral Implant. Res. 2014, 26, 1450–1455. [Google Scholar] [CrossRef] [PubMed]
- Belgin, C.A.; Colak, M.; Adiguzel, O.; Akkus, Z.; Orhan, K. Three-dimensional evaluation of maxillary sinus volume in different age and sex groups using CBCT. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 1493–1499. [Google Scholar] [CrossRef]
- Motro, M. Three-Dimensional Examination of Changes in the Maxillary Sinuses Following Rapid Maxillary Expansion and after One-Year Retention Period. Ph.D. Thesis, Marmara University, İstanbul, Turkey, July 2011. [Google Scholar]
- Orhan, I.; Ormeci, T.; Aydin, S.; Altin, G.; Urger, E.; Soylu, E.; Yilmaz, F.; Aydın, S.; Altın, G. Morphometric analysis of the maxillary sinus in patients with nasal septum deviation. Eur. Arch. Oto-Rhino-Laryngol. 2013, 271, 727–732. [Google Scholar] [CrossRef]
- Möhlhenrich, S.; Heussen, N.; Peters, F.; Steiner, T.; Hölzle, F.; Modabber, A. Is the Maxillary Sinus Really Suitable in Sex Determination? A Three-Dimensional Analysis of Maxillary Sinus Volume and Surface Depending on Sex and Dentition. J. Craniofacial Surg. 2015, 26, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.H.; Kim, T.H.; Kim, K.R.; Lee, J.-M.; Lee, D.-K.; Kim, J.-H.; Im, J.-J.; Park, C.-J.; Hwang, K.-G. Factors for Maxillary Sinus Volume and Craniofacial Anatomical Features in Adults with Chronic Rhinosinusitis. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koppe, T.; Weigel, C.; Bärenklau, M.; Kaduk, W.; Bayerlein, T.; Gedrange, T. Maxillary sinus pneumatization of an adult skull with an untreated bilateral cleft palate. J. Cranio-Maxillofacial Surg. 2006, 34, 91–95. [Google Scholar] [CrossRef]
- Barbosa, G.D.R.; Pimenta, L.; Gribel, B.F.; Golden, B.A.; Roberts, J.; Drake, A.F. Difference in maxillary sinus volumes of patients with cleft lip and palate. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 2234–2236. [Google Scholar] [CrossRef] [PubMed]
- Erdur, O.; Uçar, F.I.; Sekerci, A.E.; Celikoglu, M.; Buyuk, S.K. Maxillary sinus volumes of patients with unilateral cleft lip and palate. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1741–1744. [Google Scholar] [CrossRef]
- Ariji, Y.; Kuroki, T.; Moriguchi, S.; Ariji, E.; Kanda, S. Age changes in the volume of the human maxillary sinus: A study using computed tomography. Dentomaxillofacial Radiol. 1994, 23, 163–168. [Google Scholar] [CrossRef]
- Kurita, S.; Sato, K.; Fukazawa, H.; Mitani, H. [Morphological relationship between maxillary sinus and skeletal facial type]. Nihon Kyosei Shika Gakkai zasshi = J. Jpn. Orthod. Soc. 1988, 47, 689–696. [Google Scholar]
- Jun, B.-C.; Song, S.-W.; Park, C.-S.; Lee, N.-H.; Cho, K.-J.; Cho, J.-H. The analysis of maxillary sinus aeration according to aging process; volume assessment by 3-dimensional reconstruction by high-resolutional CT scanning. Otolaryngol. Neck Surg. 2005, 132, 429–434. [Google Scholar] [CrossRef]
- Graney, D.O.; Anatomy Rice, D. Otolaryngology: Head and Neck Surgery, 2nd ed.; Cummings, C., Fredrickson, J.M., Harker, L.A., Krause, C.J., Schuller, D., Eds.; Mosby Year Book: St. Louis, MO, USA, 1992; pp. 901–906. [Google Scholar]
- Oh, H.; Herchold, K.; Hannon, S.; Heetland, K.; Ashraf, G.; Nguyen, V.; Cho, H.J. Orthodontic tooth movement through the maxillary sinus in an adult with multiple missing teeth. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 493–505. [Google Scholar] [CrossRef]
- Maspero, C.; Fama, A.; Cavagnetto, D.; Abate, A.; Farronato, M. Treatment of dental dilacerations. J. Biol. Regul. Homeost. Agents 2019, 33, 1623–1628. [Google Scholar]
- Oz, A.Z.; Oz, A.A.; Palomo, J.M.; El, H. Maxillary sinus volume in patients with impacted canines. Angle Orthod. 2017, 87, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maspero, C.; Abate, A.; Cavagnetto, D.; Fama, A.; Stabilini, A.; Farronato, G.; Farronato, M. Operculectomy and spontaneous eruption of impacted second molars: A retrospective study. J. Biol. Regul. Homeost. Agents. 2019, 33, 1909–1912. [Google Scholar]
- Li, J.; Wang, H.-L. Common Implant-Related Advanced Bone Grafting Complications: Classification, Etiology, and Management. Implant. Dent. 2008, 17, 389–401. [Google Scholar] [CrossRef] [Green Version]
- Hauman, C.H.J.; Chandler, N.P.; Tong, D.C. Endodontic implications of the maxillary sinus: A review. Int. Endod. J. 2002, 35, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Testori, T.; Weinstein, T.; Taschieri, S.; Wallace, S.S. Risk factors in lateral window sinus elevation surgery. Periodontology 2000 2019, 81, 91–123. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.; Choi, S.-H.; Cha, J.-Y.; Lee, K.-J.; Hwang, C.-J. Retrospective study of maxillary sinus dimensions and pneumatization in adult patients with an anterior open bite. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 796–801. [Google Scholar] [CrossRef]
- Park, J.H.; Tai, K.; Kanao, A.; Takagi, M. Space closure in the maxillary posterior area through the maxillary sinus. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 95–102. [Google Scholar] [CrossRef]
- Verna, C.; Melsen, B.; Melsen, F. Differences in static cortical bone remodeling parameters in human mandible and iliac crest. Bone 1999, 25, 577–583. [Google Scholar] [CrossRef]
- Birte, M. Adult Orthodontics, 1st ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2012. [Google Scholar]
- Farronato, G.; Giannini, L.; Galbiati, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Maspero, C. Oral tissues and orthodontic treatment: Common side effects. Minerva Stomatol. 2013, 62, 431–446. [Google Scholar]
- Sun, W.; Xia, K.; Huang, X.-Q.; Cen, X.; Liu, Q.; Liu, J. Knowledge of orthodontic tooth movement through the maxillary sinus: A systematic review. BMC Oral Health 2018, 18, 91. [Google Scholar] [CrossRef]
- Juerchott, A.; Freudlsperger, C.; Zingler, S.; Saleem, M.A.; Jende, J.M.E.; Lux, C.J.; Bendszus, M.; Heiland, S.; Hilgenfeld, T. In vivo reliability of 3D cephalometric landmark determination on magnetic resonance imaging: A feasibility study. Clin. Oral Investig. 2019, 1–11. [Google Scholar] [CrossRef]
- Maspero, C.; Abate, A.; Bellincioni, F.; Cavagnetto, D.; Lanteri, V.; Costa, A.; Farronato, M. Comparison of a tridimensional cephalometric analysis performed on 3T-MRI compared with CBCT: A pilot study in adults. Prog. Orthod. 2019, 20, 40. [Google Scholar] [CrossRef] [PubMed]
- Juerchott, A.; Freudlsperger, C.; Weber, D.; Jende, J.M.E.; Saleem, M.A.; Zingler, S.; Lux, C.J.; Bendszus, M.; Heiland, S.; Hilgenfeld, T. In Vivo Comparison of MRI- and CBCT-Based 3D Cephalometric Analysis: Beginning of a Non-Ionizing Diagnostic Era in Craniomaxillofacial Imaging? Eur. Radiol. 2020, 30, 1488–1497. [Google Scholar] [CrossRef] [PubMed]
- Juerchott, A.; Saleem, M.A.; Hilgenfeld, T.; Freudlsperger, C.; Zingler, S.; Lux, C.J.; Bendszus, M.; Heiland, S. 3D cephalometric analysis using Magnetic Resonance Imaging: Validation of accuracy and reproducibility. Sci. Rep. 2018, 8, 13029. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurements | Male | Female | Comparison Male vs. Female | |||||
|---|---|---|---|---|---|---|---|---|
| Mean; ± SD | Median; (1–3 quartile) | R vs. L p Value | Mean ± SD | Median; (1–3 quartile) | R vs. L p Value | p Value | ||
| MSV-R | 1 | 8493.15 ± 2475.17 | 8054.94 (6758.08; 9987.84) | 0.921 | 7165.59 ± 1852.45 | 6872.39 (6266.72; 7861.48) | 0.341 | 0.027 * |
| MSV-L | 1 | 8462.65 ± 2782.68 | 8043.21 (6232.69; 9055.70) | 6907.22 ± 2051.71 | 7008.02 (6199.91; 8345.58) | 0.041 * | ||
| MSV-Tot a | 1 | 16955.79 ± 5013.80 | 16131.32 (12765.36; 19647.39) | / | 13998.74 ± 3687.55 | 14474.08 (11783.02; 15378.44) | / | 0.035 * |
| MSV-R | 2 | 9192.22 ± 2657.30 | 8912.55 (6971.69; 12251.59) | 0.982 | 8616.21 ± 2211.75 | 8291.05 (7246.57; 9792.60) | 0.614 | 0.525 |
| MSV-L | 2 | 9187.38 ± 2359.84 | 8781.82 (7234.86; 10888.86) | 8739.56 ± 2104.15 | 8842.62 (7265.33; 10333.56) | 0.683 | ||
| MSV-Tot a | 2 | 18379.59 ± 4924.78 | 17666.02 (14194.21; 22615.68) | / | 17033.04 ± 3704.71 | 16233.36 (14853.99; 19878.85) | / | 0.414 |
| MSV R | 3 | 13760.25 ± 2987.21 | 13271.63 (11189.04; 16610.20) | 0.914 | 12072.57 ± 1456.78 | 11802.14(11263.35; 13552.32) | 0.600 | 0.025 * |
| MSV-L | 3 | 13716.68 ± 2915.70 | 13672.61 (10852.76; 16749.64) | 11935.12 ± 2211.45 | 12913.72 (10024.76; 13737.23) | 0.02 * | ||
| MSV-Tot a | 3 | 27476.93 ± 5613.75 | 26543.26(23051.89; 33593.30) | / | 23923.68 ± 3642.16 | 24715.86 (21288.11; 27289.55) | / | 0.023 * |
| MSS-R | 1 | 2627.54 ± 472.44 | 2625.82 (2240.99; 2853.09) | 0.163 | 2427.69 ± 859.05 | 2419.11 (2253.69; 2800.98) | 0.190 | 0.095 |
| MSS-L | 1 | 2550.62 ± 509.45 | 2592.87 (2166.05; 2686.81) | 2318.82 ± 411.52 | 2266.80 (2128.95; 2609.66) | 0.245 | ||
| MSS-Tot a | 1 | 5178.16 ± 940.73 | 5198.35 (4359.62; 5754.33) | / | 4746.51 ± 1079.35 | 4814.97 (4324.41; 5346.92) | / | 0.173 |
| MSS-R | 2 | 2922.01 ± 704.82 | 2848.49 (2310.30; 3338.45) | 0.513 | 2796.29 ± 601.49 | 2653.18 (2372.07; 3326.60) | 0.727 | 0.768 |
| MSS-L | 2 | 2879.33 ± 689.13 | 2875.83 (2337.30; 3369.11) | 2826.91 ± 529.21 | 2862.92 (2519.62; 3250.57) | 0.932 | ||
| MSS-Tot a | 2 | 5801.34 ± 1159.55 | 5809.96 (4649.24; 6454.23) | / | 5623.2 ± 1021.78 | 5477.35 (4966.67; 6496.63) | / | 0.862 |
| MSS-R | 3 | 4119.71±1077.28 | 3835.41 (3272.23; 5404.33) | 0.464 | 3571.66 ± 635.21 | 3756.41 (3658.72; 4342.12) | 0.117 | 0.049 * |
| MSS-L | 3 | 4184.08 ±1036.80 | 4053.72 (3197.29; 4714.99) | 3615.59 ± 492.46 | 3929.09 (3193.67; 4046.57) | 0.041 * | ||
| MSS-Tot a | 3 | 8303.79 ± 1785.91 | 7369.94 (6623.68; 9866.96) | / | 7367.25 ± 1057.09 | 7708.17 (6870.08; 8273.06) | / | 0.043 * |
| LMW-R | 1 | 27.13 ± 4.64 | 27.64 (24.12; 30.02) | 0.783 | 26.51 ± 2.88 | 27.08 (24.10; 29.03) | 0.142 | 0.567 |
| LMW-L | 1 | 27.28 ± 4.93 | 27.08 (24.00; 31.58) | 25.91 ± 2.94 | 26.74 (25.09; 27.42) | 0.289 | ||
| LMW-R | 2 | 27.89 ± 4.63 | 28.21 (24.56; 30.56) | 0.544 | 26.82 ± 3.24 | 26.69 (23.32; 28.43) | 0.093 | 0.107 |
| LMW-L | 2 | 27.51 ± 2.67 | 28.17 (24.92; 29.49) | 26.98 ± 3.21 | 27.97 (24.13; 29.91) | 0.650 | ||
| LMW-R | 3 | 31.31 ± 3.53 | 32.30 (28.60; 34.25) | 0.807 | 28.04 ± 2.71 | 29.32 (28.18; 30.56) | 0.174 | 0.002 * |
| LMW-L | 3 | 31.19 ± 3.08 | 31.27 (29.24; 36.96) | 27.93 ± 2.49 | 27.60 (28.29; 30.21) | < 0.001 * | ||
| LMD-R | 1 | 34.36 ± 2.90 | 34.08 (31.59; 36.95) | 0.40 | 32.61 ± 3.74 | 33.45 (31.05; 35.29) | 0.191 | 0.099 |
| LMD-L | 1 | 33.65 ± 3.39 | 33.93 (32.22; 36.39) | 34.13 ± 6.60 | 34.09 (31.46; 35.34) | 0.987 | ||
| LMD-R | 2 | 35.67 ± 3.47 | 35.28 (32.73; 38.57) | 0.271 | 34.68 ± 2.22 | 34.48 (33.38; 34.63) | 0.038 | 0.097 |
| LMD-L | 2 | 35.32 ± 3.14 | 34.95 (33.99; 38.26) | 33.90 ± 2.77 | 33.66 (33.59; 35.64) | 0.481 | ||
| LMD-R | 3 | 37.99 ± 4.26 | 39.19 (35.54; 41.53) | 0.037 | 35.90 ± 2.32 | 36.12 (35.20; 38.17) | 0.672 | 0.013 * |
| LMD-L | 3 | 39.48 ± 2.60 | 40.52 (38.12; 41.92) | 36.13 ± 1.92 | 35.26 (34.16; 38.59) | < 0.001 * | ||
| LMH-R | 1 | 28.09 ± 4.32 | 28.80 (24.01; 30.81) | 0.233 | 26.52 ± 2.59 | 26.81 (26.00; 28.11) | 0.817 | 0.095 |
| LMH-L | 1 | 27.68 ± 5.25 | 27.81 (24.00; 31.21) | 26.42 ± 2.45 | 26.82 (24.02; 27.60) | 0.232 | ||
| LMH-R | 2 | 30.15 ± 4.02 | 29.61 (27.22; 32.41) | 0.921 | 29.45 ± 3.40 | 29.21 (26.83; 32.23) | 0.277 | 0.609 |
| LMH-L | 2 | 30.11 ± 3.84 | 30.01 (27.20; 32.40) | 29.78 ± 3.51 | 30.02 (27.82; 32.50) | 0.874 | ||
| LMH-R | 3 | 36.36 ± 3.92 | 36.40 (33.03; 38.81) | 0.900 | 35.46 ± 3.43 | 35.21 (34.01; 38.81) | 0.103 | 0.617 |
| LMH-L | 3 | 36.29 ± 4.71 | 37.72 (32.65; 39.61) | 35.98 ± 3.32 | 36.41 (35.77; 38.02) | 0.956 | ||
| Measurements | Mean Ranks | Kruskal–Wallis Test | Pairwise Comparisons (Bonferroni Correction) | ||||
|---|---|---|---|---|---|---|---|
| Group 1 6–8 years | Group 2 9–11 years | Group 3 12–14 years | p Value | p Value Group 1 vs. 2 | p Value Group 2 vs. 3 | p Value Group 1 vs. 3 | |
| MSV R | 21.30 | 32.91 | 59.04 | <0.001 * | 0.060 | <0.001 * | <0.001 * |
| MSV L | 20.78 | 34.91 | 57.84 | <0.001 * | 0.066 | <0.001 * | <0.001 * |
| MSV Tot a | 20.67 | 33.73 | 59.00 | <0.001 * | 0.034 * | <0.001 * | <0.001 * |
| MSS R | 23.44 | 32.36 | 57.20 | <0.001 * | 0.148 | <0.001 * | <0.001 * |
| MSS L | 24.37 | 33.34 | 58.10 | <0.001 * | 0.075 | 0.002 * | <0.001 * |
| MSS Tot a | 21.89 | 34.27 | 57.20 | <0.001 * | 0.045 * | <0.001 * | <0.001 * |
| LMW-R | 31.44 | 38.05 | 46.60 | 0.001 * | 0.821 | 0.121 | 0.001 * |
| LMW-L | 30.85 | 37.36 | 44.80 | 0.045 * | 1.00 | 0.210 | 0.011 * |
| LMD-R | 28.63 | 34.45 | 46.40 | <0.001 * | 0.647 | 0.091 | 0.001 * |
| LMD-L | 29.89 | 35.82 | 47.20 | 0.013 * | 0.337 | 0.070 | 0.004 * |
| LMH-R | 19.96 | 34.14 | 59.40 | <0.001 * | 0.022 * | <0.001 * | <0.001 * |
| LMH-L | 18.91 | 35.66 | 59.20 | <0.001 * | 0.020 * | <0.001 * | <0.001 * |
| Measurements | Mean Ranks | Kruskal–Wallis Test | Pairwise Comparisons (Bonferroni Correction) | ||||
|---|---|---|---|---|---|---|---|
| Group 1 6–8 years | Group 2 9–11 years | Group 3 12–14 years | p Value | p Value Group 1 vs. 2 | p Value Group 2 vs. 3 | p Value Group 1 vs. 3 | |
| MSV R | 26.11 | 30.65 | 56.76 | <0.001 * | 1.000 | <0.001 * | <0.001 * |
| MSV L | 25.64 | 31.35 | 56.62 | <0.001 * | 0.998 | <0.001 * | <0.001 * |
| MSV Tot a | 25.79 | 30.74 | 57.10 | <0.001 * | 1.000 | <0.001 * | <0.001 * |
| MSS R | 24.96 | 33.43 | 55.24 | <0.001 * | 0.451 | 0.002 * | <0.001 * |
| MSS L | 23.36 | 34.30 | 56.43 | <0.001 * | 0.189 | 0.001 * | <0.001 * |
| MSS Tot a | 23.64 | 33.78 | 56.62 | <0.001 * | 0.255 | 0.001 * | <0.001 * |
| LMW-R | 29.18 | 33.07 | 50.02 | 0.002 * | 1.000 | 0.022 * | 0.002 * |
| LMW-L | 28.43 | 34.74 | 49.19 | 0.002 * | 0.284 | 0.025 * | 0.001 * |
| LMD-R | 24.75 | 31.96 | 57.14 | <0.001 * | 0.221 | <0.001 * | <0.001 * |
| LMD-L | 30.57 | 30.24 | 51.26 | 0.001 * | 1.000 | 0.002 * | 0.003 * |
| LMH-R | 24.71 | 32.74 | 56.33 | <0.001 * | 0.519 | 0.001 * | <0.001 * |
| LMH-L | 24.93 | 33.52 | 55.19 | <0.001 * | 0.433 | 0.002 * | <0.001 * |
| Measurements | ICC (Intra-Operator) | ICC (Inter-Operator) |
|---|---|---|
| MSV R | 0.981 | 0.974 |
| MSV L | 0.974 | 0.971 |
| MSV Tot a | 0.971 | 0.982 |
| MSS R | 0.982 | 0.974 |
| MSS L | 0.984 | 0.978 |
| MSS Tot a | 0.978 | 0.983 |
| LMW-R | 0.983 | 0.951 |
| LMW-L | 0.967 | 0.972 |
| LMD-R | 0.972 | 0.965 |
| LMD-L | 0.985 | 0.979 |
| LMH-R | 0.989 | 0.958 |
| LMH-L | 0.978 | 0.944 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maspero, C.; Farronato, M.; Bellincioni, F.; Annibale, A.; Machetti, J.; Abate, A.; Cavagnetto, D. Three-Dimensional Evaluation of Maxillary Sinus Changes in Growing Subjects: A Retrospective Cross-Sectional Study. Materials 2020, 13, 1007. https://doi.org/10.3390/ma13041007
Maspero C, Farronato M, Bellincioni F, Annibale A, Machetti J, Abate A, Cavagnetto D. Three-Dimensional Evaluation of Maxillary Sinus Changes in Growing Subjects: A Retrospective Cross-Sectional Study. Materials. 2020; 13(4):1007. https://doi.org/10.3390/ma13041007
Chicago/Turabian StyleMaspero, Cinzia, Marco Farronato, Francesca Bellincioni, Alessandro Annibale, Jacopo Machetti, Andrea Abate, and Davide Cavagnetto. 2020. "Three-Dimensional Evaluation of Maxillary Sinus Changes in Growing Subjects: A Retrospective Cross-Sectional Study" Materials 13, no. 4: 1007. https://doi.org/10.3390/ma13041007