Evaluation of the Use of an Inorganic Bone Matrix in the Repair of Bone Defects in Rats Submitted to Experimental Alcoholism

 , , ,
, , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Biomaterial—Bone Graft Substitutes
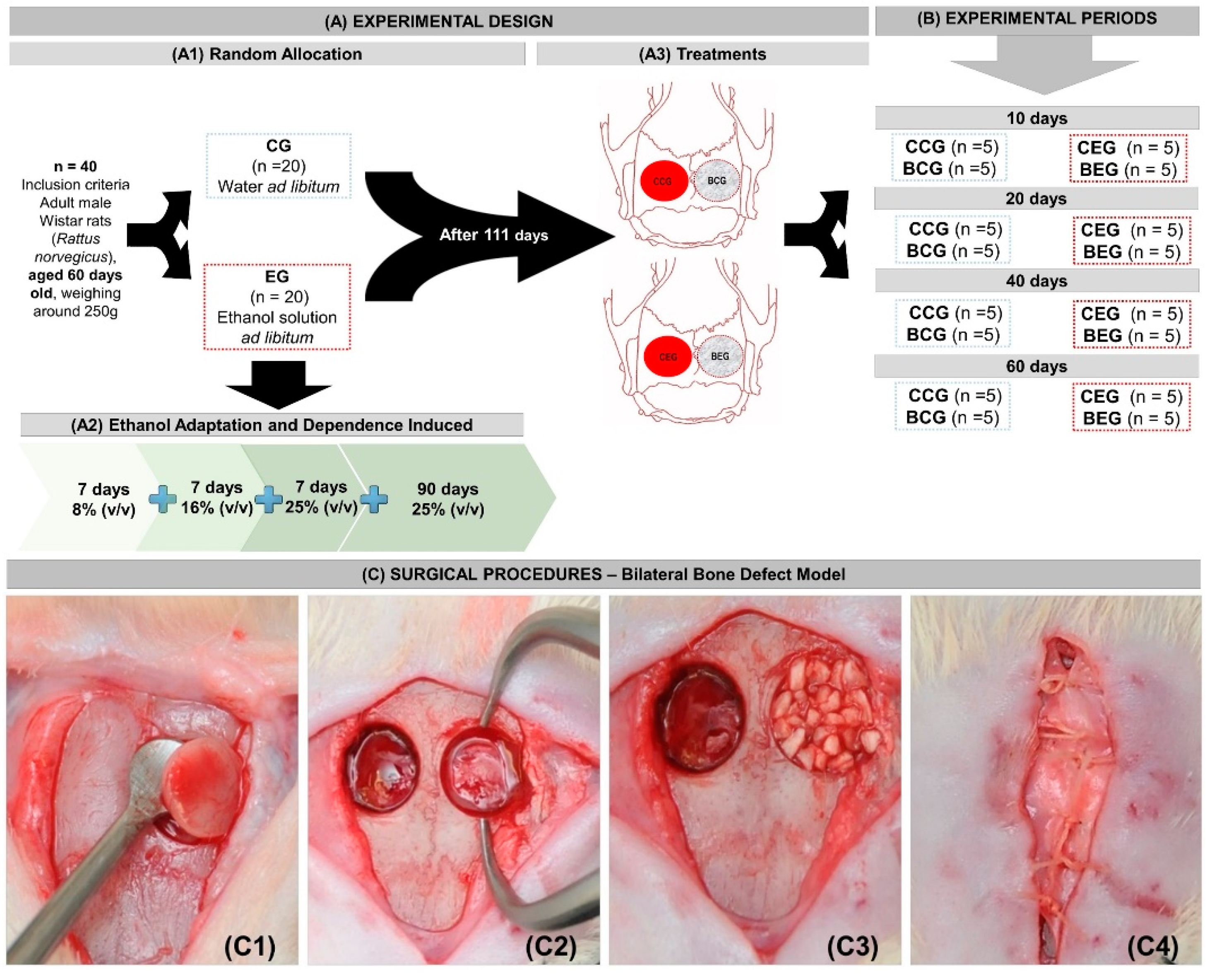
2.2. Experimental Design
2.3. Ethanol Adaptation and Induced Dependence—Semi-Voluntary Ethanol Administration—Alcohol-Liquid Diet
2.4. Surgical Procedures
2.5. Collection of Specimens and Histological Procedures
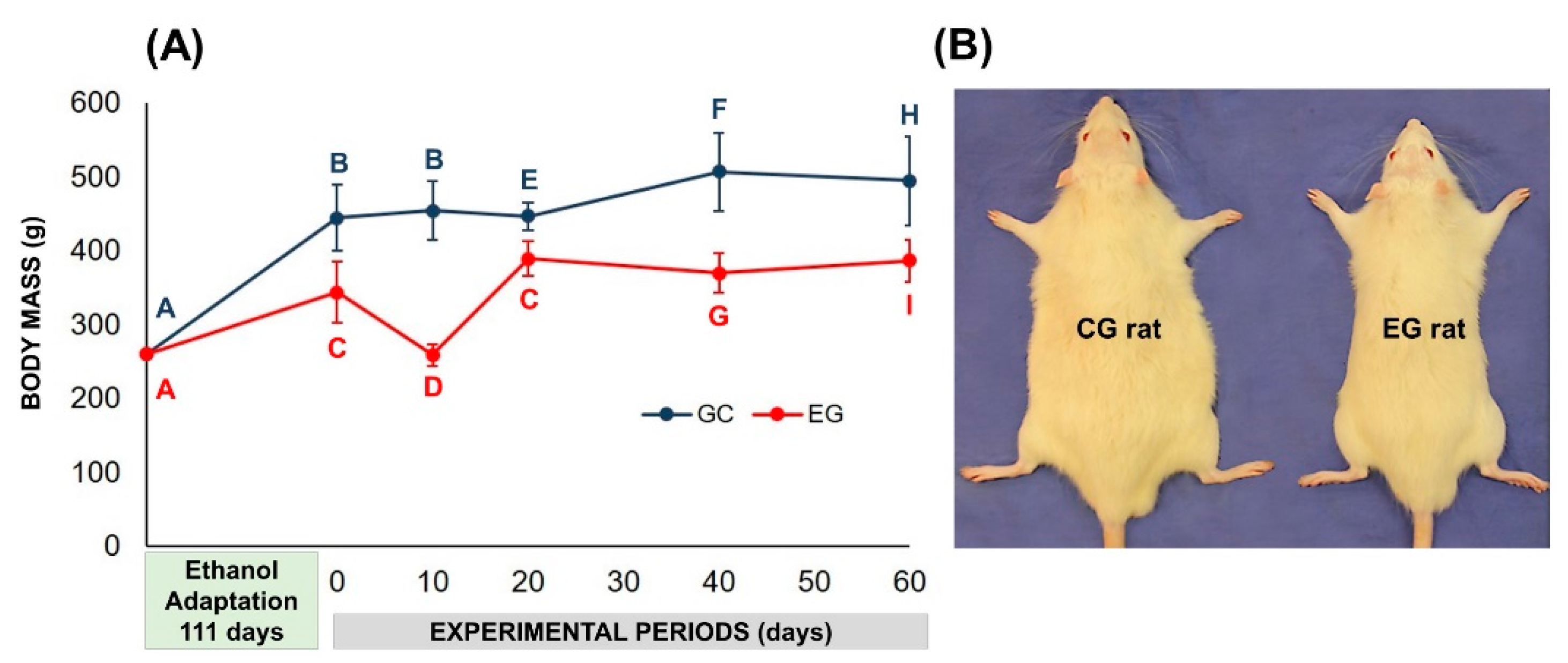
2.6. Body Mass Analysis
2.7. Histomorphological and Histomorphometric Evaluation
2.8. Statistical Evaluation of Data
3. Results
3.1. Effects of Ethanol Administration on Behavioral and Clinical Profiles of Rats
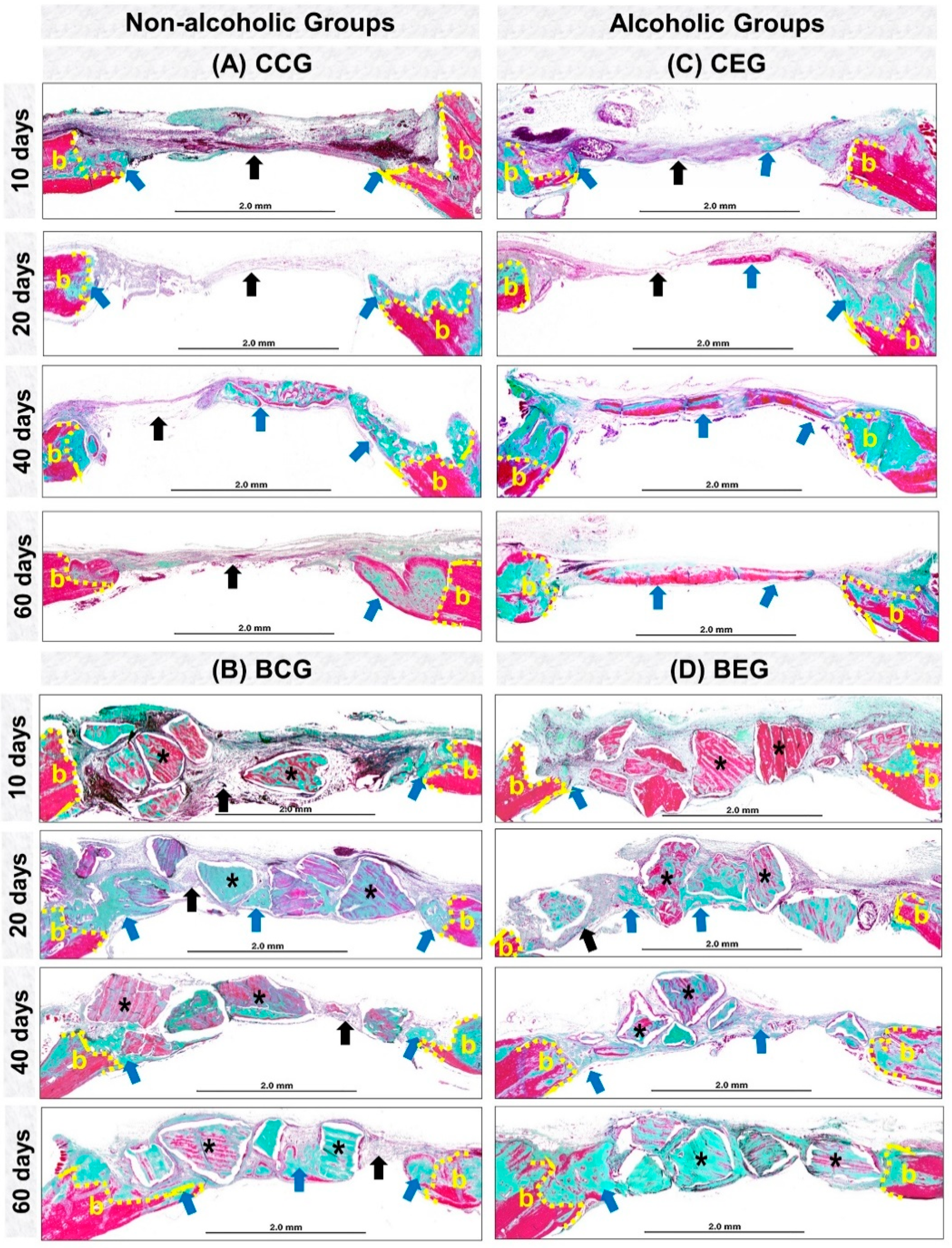
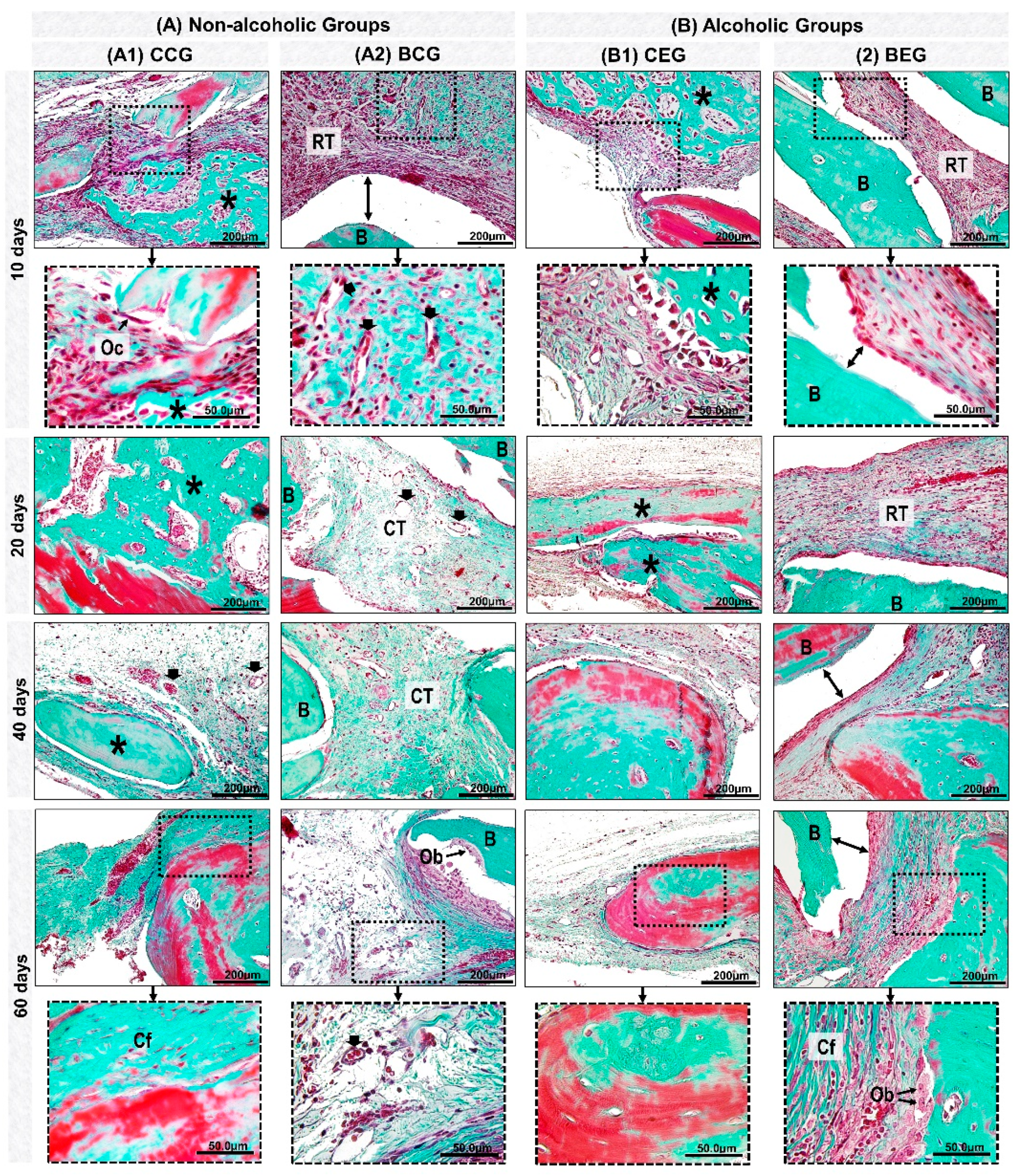
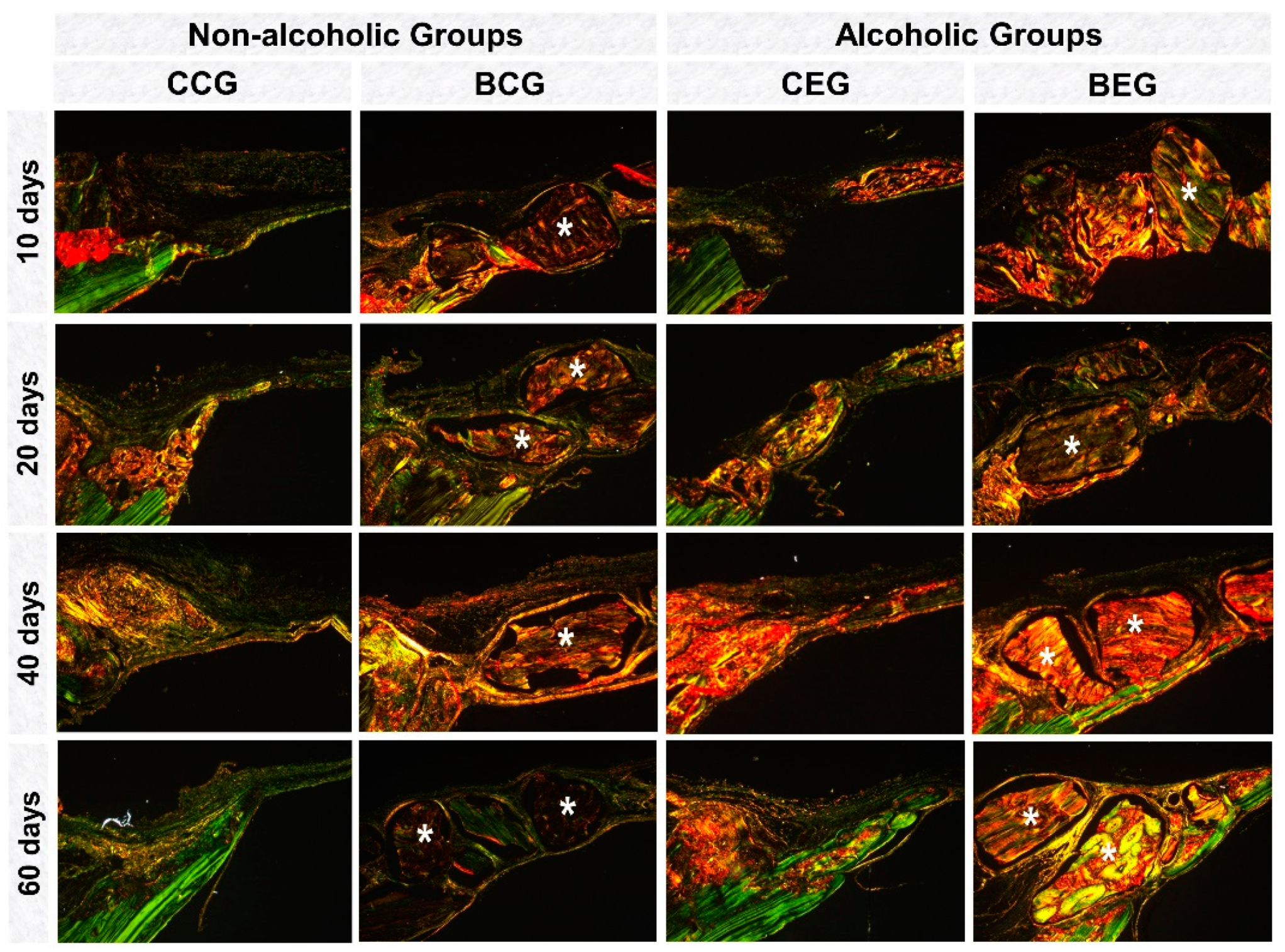
3.2. Histological Evaluation
3.3. Histomorphometric Evaluation
3.4. Influence of Clinical Condition (Alcoholic Versus non-Alcoholic) and/or Type of Treatment (Clot vs. Biomaterial) on Collagen Content During the Bone Repair Process
4. Discussion
5. Limitations
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- González-Reimers, E.; Santolaria-Fernández, F.; Martín-González, M.; Fernández-Rodríguez, C.; Quintero-Platt, G. Alcoholism: A systemic proinflammatory condition. World J. Gastroenterol. 2014, 20, 14660–14671. [Google Scholar] [CrossRef] [PubMed]
- Ronis, M.; Mercer, K.; Chen, J. Effects of Nutrition and Alcohol Consumption on Bone Loss. Bone 2008, 23, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Maurel, D.B.; Boisseau, N.; Benhamou, C.L.; Jaffre, C. Alcohol and bone: Review of dose effects and mechanisms. Osteoporos. Int. 2012, 23, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Maaurel, D.B.; Jaffre, C.; Rochefort, G.Y.; Aveline, P.C.; Boisseau, N.; Uzbekov, R.; Gosset, D.; Pichon, C.; Fazzalari, N.L.; Pallu, S.; et al. Low bone accrual is associated with osteocyte apoptosis in alcohol-induced osteopenia. Bone 2011, 49, 543–552. [Google Scholar] [CrossRef]
- Shetty, S.; Kapoor, N.; Bondu, J.; Thomas, N.; Paul, T. Bone turnover markers: Emerging tool in the management of osteoporosis. Indian J. Endocrinol. Metab. 2016, 20, 846. [Google Scholar]
- Johnson, T.L.; Gaddini, G.; Branscum, A.J.; Olson, D.A.; Caroline-Westerlind, K.; Turner, R.T.; Iwaniec, U.T. Effects of chronic heavy alcohol consumption and endurance exercise on cancellous and cortical bone microarchitecture in adult male rats. Alcohol. Clin. Exp. Res. 2014, 38, 1365–1372. [Google Scholar] [CrossRef] [Green Version]
- Mikosch, P. Alcohol and bone. Wien. Med. Wochenschr. 2014, 164, 15–24. [Google Scholar] [CrossRef]
- Chakkalakal, D.A. Alcohol-induced bone loss and deficient bone repair. Alcohol. Clin. Exp. Res. 2005, 29, 2077–2090. [Google Scholar] [CrossRef]
- Ventura, A.S.; Winter, M.R.; Heeren, T.C.; Sullivan, M.M.; Walley, A.Y.; Holick, M.F.; Patts, G.J.; Meli, S.M.; Samet, J.H.; Saitz, R. Lifetime and recent alcohol use and bone mineral density in adults with HIV infection and substance dependence. Medicine (United States) 2017, 96, e6759. [Google Scholar] [CrossRef]
- Rosso, M.P.D.O.; Buchaim, D.V.; Pomini, K.T.; Botteon, B.D.C.; Reis, C.H.B.; Pilon, J.P.G.; Duarte Júnior, G.; Buchaim, R.L. Photobiomodulation Therapy (PBMT) Applied in Bone Reconstructive Surgery Using Bovine Bone Grafts: A Systematic Review. Materials (Basel) 2019, 12, 4051. [Google Scholar] [CrossRef] [Green Version]
- Flintoff, K. Oh rats! A guide to rat anaesthesia for veterinary nurses and technicians. N. Z. Vet. Nurse 2014, 20, 22–27. [Google Scholar]
- Weibel, E.R. Stereological Principles for Morphometry in Electron Microscopic Cytology. Int. Rev. Cytol. 1969, 26, 235–302. [Google Scholar] [PubMed]
- Lauing, K.; Roper, P.; Nauer, R.; Callaci, J. Acute alcohol exposure impairs fracture healing and deregulates β-catenin signaling in the fracture callus. Alcohol. Clin. Exp. Res. 2012, 36, 2095–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dguzeh, U.; Haddad, N.C.; Smith, K.T.S.; Johnson, J.O.; Doye, A.A.; Gwathmey, J.K.; Haddad, G.E. Alcoholism: A multi-systemic cellular insult to organs. Int. J. Environ. Res. Public Health 2018, 15, 1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vajgel, A.; Mardas, N.; Farias, B.C.; Petrie, A.; Cimões, R.; Donos, N. A systematic review on the critical size defect model. Clin. Oral Implant Res. 2014, 25, 879–893. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Wood, A.M.; Kaptoge, S.; Butterworth, A.; Willeit, P.; Warnakula, S.; Bolton, T.; Paige, E.; Paul, D.S.; Sweeting, M.; Burgess, S.; et al. Risk thresholds for alcohol consumption: Combined analysis of individual-participant data for 599912 current drinkers in 83 prospective studies. Lancet 2018, 391, 1513–1523. [Google Scholar] [CrossRef] [Green Version]
- De Souza, D.M.; Ricardo, L.H.; Prado, M.D.A.; Prado, F.D.A.; Da Rocha, R.F. The effect of alcohol consumption on periodontal bone support in experimental periodontitis in rats. J. Appl. Oral. Sci. 2006, 14, 443–447. [Google Scholar] [CrossRef] [Green Version]
- Buchaim, R.L.; Buchaim, D.V.; Andreo, J.C.; Roque, D.D.; Roque, J.S.; de Castro Rodrigues, A. Effects of three alcoholic diets on the bone repair in the tibia of rats. Cienc. Odontol. Bras. 2009, 12, 17–23. [Google Scholar]
- Pomini, K.; Cestari, M.; German, I.; Rosso, M.; Gonçalves, J.; Buchaim, D.; Pereira, M.; Andreo, J.C.; Rosa Júnior, G.M.; Della Coletta, B.; et al. Influence of experimental alcoholism on the repair process of bone defects filled with beta-tricalcium phosphate. Drug Alcohol Depend. 2019, 197, 315–325. [Google Scholar] [CrossRef]
- Liberman, D.N.; Pilau, R.M.; Gaio, E.J.; Orlandini, L.F.; Rösing, C.K. Low concentration alcohol intake may inhibit spontaneous alveolar bone loss in Wistar rats. Arch. Oral. Biol. 2011, 56, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Lieber, C.S. Relationships between nutrition, alcohol use and liver disease. Alcohol Res. Health 2003, 27, 220–231. [Google Scholar] [PubMed]
- Feinman, L.; Lieber, C.S. Nutrition and diet in alcoholism. In Modern Nutrition in Health and Disease, 9th ed.; Shils, M.E., Olson, J.A., Shike, M., Ross, A.C., Eds.; Williams & Wilkins: Baltimore, MD, USA, 1998; pp. 1523–1542. [Google Scholar]
- Velvizhi, S.; Nagalashmi, I.; Essa, M.M.; Dakshayani, K.B.; Subramanian, P. Effects of α-ketoglutarate on lipid peroxidation and antioxidant status during chronic ethanol administration in Wistar rats. Pol. J. Pharmacol. 2002, 54, 231–236. [Google Scholar] [PubMed]
- Thomson, A.D.; Pratt, O.E. Interaction of nutrients and alcohol: Absorption, transport, utilization and metabolism. In Nutrition and Alcohol; Watson, R.R., Watzl, B., Eds.; CRC Press: Boca Raton, FL, USA, 1992; pp. 75–99. [Google Scholar]
- Aruna, K.; Rukkumani, P.; Varma, S.P.; Menon, V.P. Therapeutic role of Cuminum on ethanol and thermally oxidized sunflower oil induced toxicity. Phytother. Res. 2005, 19, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Kovács, G.L.; Toldy, E. Basal and isoproterenol-stimulated cyclic-adenosine monophosphate levels in mouse hippocampus and lymphocytes during alcohol tolerance and withdrawal. Alcohol Alcohol. 2003, 38, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimbrough, A.; de Guglielmo, G.; Kononoff, J.; Kallupi, M.; Zorrilla, E.; George, O. CRF1 receptor-dependent increases in irritability-like behavior during abstinence from chronic intermittent ethanol vapor exposure. Alcohol. Clin. Exp. Res. 2017, 41, 1886–1895. [Google Scholar] [CrossRef]
- Neagu, T.P.; Ţigliş, M.; Cocoloş, I.; Jecan, C.R. The relationship between periosteum and fracture healing. Rom. J. Morphol. Embryol. 2016, 57, 1215–1220. [Google Scholar]
- Spicer, P.; Kretlow, J.; Young, S.; Jansen, J.; Kasper, F.; Mikos, A. Evaluation of Bone Regeneration Using the Rat Critical Size Calvarial Defect. Nat Protoc. 2012, 7, 1918–1929. [Google Scholar] [CrossRef] [Green Version]
- Gosain, A.; Song, L.; Yu, P.; Mehrara, B.; Maeda, C.; Gold, L.; Longaker, M. Osteogenesis in cranial defects: Reassessment of the concept of critical size and the expression of TGF-beta isoforms. Plast. Reconstr. Surg. 2000, 106, 360–371. [Google Scholar] [CrossRef]
- Browne, S.; Pandit, A. Biomaterial-Mediated Modification of the Local Inflammatory Environment. Front. Bioeng. Biotechnol. 2015, 3, 67. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Klein, T.; Murray, R.Z.; Crawford, R.; Chang, J.; Wu, C.; Xiao, Y. Osteoimmunomodulation for the development of advanced bone biomaterials. Mater. Today 2016, 19, 304–321. [Google Scholar] [CrossRef] [Green Version]
- Rocha, C.A.; Cestari, T.M.; Vidotti, H.A.; De Assis, G.F.; Garlet, G.P.; Taga, R. Sintered anorganic bone graft increases autocrine expression of VEGF, MMP-2 and MMP-9 during repair of critical-size bone defects. J. Mol. Histol. 2014, 45, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Liu, W.; Hill, P.; Bratlie, K.; Siegwart, D.; Chin, J.; Park, M.; Guerreiro, J.; Anderson, D.G. Development of Cationic Polymer Coatings to Regulate Foreign Body Responses. PLoS ONE 2017, 32, 736–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaikof, E.L.; Matthew, H.; Kohn, J.; Mikos, A.G.; Prestwich, G.D.; Yip, C.M. Biomaterials and scaffolds in reparative medicine. Ann. N. Y. Acad. Sci. 2002, 961, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Wubneh, A.; Tsekoura, E.K.; Ayranci, C.; Uludağ, H. Current state of fabrication technologies and materials for bone tissue engineering. Acta Biomater. 2018, 80, 1–30. [Google Scholar] [CrossRef]
- Zhang, N.; Ma, L.; Liu, X.; Jiang, X.; Yu, Z.; Zhao, D.; Zhang, L.; Zhang, C.; Huang, F. In vitro and in vivo evaluation of xenogeneic bone putty with the carrier of hydrogel derived from demineralized bone matrix. Cell Tissue Bank. 2018, 19, 591–601. [Google Scholar] [CrossRef]
- Winkler, T.; Sass, F.A.; Duda, G.N.; Schmidt-Bleek, K. A review of biomaterials in bone defect healing, remaining shortcomings and future opportunities for bone tissue engineering. Bone Jt. Res. 2018, 7, 232–243. [Google Scholar] [CrossRef]
- Hanak, C.; Benoit, J.; Fabry, L.; Hein, M.; Verbanck, P.; de Witte, P.; Walter, H.; Dexter, D.T.; Ward, R.J. Changes in pro-inflammatory markers in detoxifying chronic alcohol abusers, divided by lesch typology, reflect cognitive dysfunction. Alcohol Alcohol. 2017, 52, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Shiu, H.; Goss, B.; Lutton, C.; Crawford, R.; Xiao, Y. Formation of Blood Clot on Biomaterial Implants Influences Bone Healing. Tissue Eng. Part B Rev. 2014, 20, 697–712. [Google Scholar] [CrossRef]
- Wang, X.; Luo, Y.; Yang, Y.; Zheng, B.; Yan, F.; Wei, F.; Friis, T.E.; Crawford, R.W.; Xiao, Y. Alteration of clot architecture using bone substitute biomaterials (beta-tricalcium phosphate) significantly delays the early bone healing process. J. Mater. Chem. B 2018, 6, 8204–8213. [Google Scholar] [CrossRef]
- De Paula do Desterro, F.; Sader, M.S.; de Almeida Soares, G.; Vidigal, G.M.; Vidigal, G.M. Can inorganic bovine bone grafts present distinct properties? Braz. Dent. J. 2014, 25, 282–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamidabadi, H.; Shafaroudi, M.; Seifi, M.; Bojnordi, M.; Behruzi, M.; Gholipourmalekabadi, M.; Shafaroudi, A.; Rezaei, N. Repair of Critical-Sized Rat Calvarial Defects With Three-Dimensional Hydroxyapatite-Gelatin Scaffolds and Bone Marrow Stromal Stem Cells. Med. Arch. 2018, 72, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biguetti, C.; Cavalla, F.; Tim, C.; Saraiva, P.; Orcini, W.; de Andrade Holgado, L.; Rennó, A.; Matsumoto, M. Bioactive glass-ceramic bone repair associated or not with autogenous bone: A study of organic bone matrix organization in a rabbit critical-sized calvarial model. Clin. Oral Investig. 2019, 23, 413–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomini, K.T.; Buchaim, D.V.; Andreo, J.C.; de Oliveira Rosso, M.P.; Della Coletta, B.B.; German, Í.J.S.; Biguetti, A.C.C.; Shinohara, A.L.; Rosa Júnior, G.M.; Cosin Shindo, J.V.T.; et al. Fibrin Sealant Derived from Human Plasma as a Scaffold for Bone Grafts Associated with Photobiomodulation Therapy. Int. J. Mol. Sci. 2019, 20, 1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Oliveira Gonçalves, J.; Buchaim, D.; de Souza Bueno, C.; Pomini, K.; Barraviera, B.; Júnior, R.; Andreo, J.; de Castro Rodrigues, A.; Cestari, T.; Buchaim, R.L. Effects of low-level laser therapy on autogenous bone graft stabilized with a new heterologous fibrin sealant. J. Photochem. Photobiol. B 2016, 162, 663–668. [Google Scholar] [CrossRef] [Green Version]
- Pomini, K.T.; Andreo, J.C.; De Rodrigues, A.C.; De Gonçalves, J.B.O.; Daré, L.R.; German, I.J.S.; Rosa, G.M.; Buchaim, R.L. Effect of low-intensity pulsed ultrasound on bone regeneration biochemical and radiologic analyses. J. Ultrasound Med. 2014, 33, 713–717. [Google Scholar] [CrossRef] [Green Version]
- Escudero, J.S.B.; Perez, M.G.B.; de Oliveira Rosso, M.P.; Buchaim, D.V.; Pomini, K.T.; Campos, L.M.G.; Audi, M.; Buchaim, R.L. Photobiomodulation therapy (PBMT) in bone repair: A systematic review. Injury 2019, 50, 1853–1867. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Chow * |
|---|---|
| Humidity (%) | 2.30 |
| Brute protein (%) | 21.96 |
| Ether (fatty) extract (%) | 4.61 |
| Mineral residue (%) | 8.36 |
| Brute fiber (%) | 4.04 |
| Nitrogen-free extract (%) | 48.73 |
| Calcium (%) | 1.32 |
| Phosphorus (%) | 0.82 |
| Brute energy (Kcal/kg) | 3913 |
| Group | 10 Days | 20 Days | 40 Days | 60 Days | One-Way ANOVA (p) |
|---|---|---|---|---|---|
| BCG | 32.69 ± 11.71 a | 21.60 ± 5.16 a | 28.03 ± 10.64 a | 18.43 ± 11.86 a | 0.160 |
| BEG | 28.24 ± 11.60 a | 22.93 ± 11.46 a | 25.58 ± 4.00 a | 19.54 ± 11.06 a | 0.601 |
| Unpaired t-test (p) | 0.5875 | 0.8190 | 0.6426 | 0.8829 |
| Period (Days) | Volume Density of New Bone Formation (%) | |||||
|---|---|---|---|---|---|---|
| Non-Alcoholic Rat (n = 5/Period) | Alcoholic Rat (n = 5/Period) | |||||
| CCG | BCG | Paired t-Test (p) | CEG | BEG | Paired t-Test (p) | |
| 10 | 5.30 ± 3.08 a | 7.54 ± 6.56 a | 0.326 | 6.67 ± 3,09 a | 6.98 ± 5,97 a | 0.852 |
| 20 | 8.41 ± 5.17 a | 13.79 ± 11.14 a | 0.370 | 12.33 ± 1,89 a,b | 7.96 ± 4,40 a | 0.156 |
| 40 | 15.50 ± 7.14 a | 12.97 ± 7.07 a | 0.610 | 17.42 ± 2,78 b | 9.59 ± 4,59 a | 0.018 |
| 60 | 14.51 ± 7.69 a | 13.34 ± 12.45 a | 0.865 | 18.29 ± 7,89 b,* | 12.85 ± 7,94 a,* | 0.122 |
| One way ANOVA (p) | 0.05 | 0.618 | 0.007 | 0.466 | ||
| Period (Days) | Volume Density of New Bone Formation (%) | |||||
|---|---|---|---|---|---|---|
| Clot | Biomaterial | |||||
| CCG (n = 5/Period) | CEG (n = 5/Period) | Unpaired t-Test (p) | BCG (n = 5/Period) | BEG (n = 5/Period) | Unpaired t-Test (p) | |
| 10 | 5.30 ± 3.08 a | 6.67 ± 3.09 a | 0.528 | 7.54 ± 6.56 a | 6.98 ± 5.97 a | 0.899 |
| 20 | 8.41 ± 5.17 a | 12.33 ± 1.89 a | 0.151 | 13.79 ± 11.14 a | 7.96 ± 4.40 a | 0.307 |
| 40 | 15.50 ± 7.14 a | 17.42 ± 2.78 a | 0.591 | 12.97 ± 7.07 a | 9.59 ± 4.59 a | 0.678 |
| 60 | 14.51 ± 7.69 a | 18.29 ± 7.89 a | 0.464 | 13.34 ± 12.45 a | 12.85 ± 7.94 a | 0.942 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos German, I.J.; Pomini, K.T.; Bighetti, A.C.C.; Andreo, J.C.; Reis, C.H.B.; Shinohara, A.L.; Rosa Júnior, G.M.; Teixeira, D.d.B.; Rosso, M.P.d.O.; Buchaim, D.V.; et al. Evaluation of the Use of an Inorganic Bone Matrix in the Repair of Bone Defects in Rats Submitted to Experimental Alcoholism. Materials 2020, 13, 695. https://doi.org/10.3390/ma13030695
Santos German IJ, Pomini KT, Bighetti ACC, Andreo JC, Reis CHB, Shinohara AL, Rosa Júnior GM, Teixeira DdB, Rosso MPdO, Buchaim DV, et al. Evaluation of the Use of an Inorganic Bone Matrix in the Repair of Bone Defects in Rats Submitted to Experimental Alcoholism. Materials. 2020; 13(3):695. https://doi.org/10.3390/ma13030695
Chicago/Turabian StyleSantos German, Iris Jasmin, Karina Torres Pomini, Ana Carolina Cestari Bighetti, Jesus Carlos Andreo, Carlos Henrique Bertoni Reis, André Luis Shinohara, Geraldo Marco Rosa Júnior, Daniel de Bortoli Teixeira, Marcelie Priscila de Oliveira Rosso, Daniela Vieira Buchaim, and et al. 2020. "Evaluation of the Use of an Inorganic Bone Matrix in the Repair of Bone Defects in Rats Submitted to Experimental Alcoholism" Materials 13, no. 3: 695. https://doi.org/10.3390/ma13030695