In Vitro Evaluation of Substantivity, Staining Potential, and Biofilm Reduction of Guava Leaf Extract Mouth Rinse in Combination with its Anti-Inflammatory Effect on Human Gingival Epithelial Keratinocytes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Plant Materials
2.2. Preparation of the Guava Mouth Rinse
2.3. Assessment of Substantivity
2.4. Biofilm Development
2.5. Assessment of the Anti-Biofilm Effect
2.6. Staining Potential
2.7. Assessment of Stains on Specimens
2.8. Cell Viability Assay
2.9. Cell Culture and LPS-Induction
2.10. Real-Time Quantitative Polymerase Chain Reaction Analysis (RT-PCR)
2.11. Scratch Wound Healing Assay (Cell Migration)
2.12. Statistical Analysis
3. Results
3.1. Substantivity Property
3.2. Anti-Biofilm Effects
3.3. Staining Potential
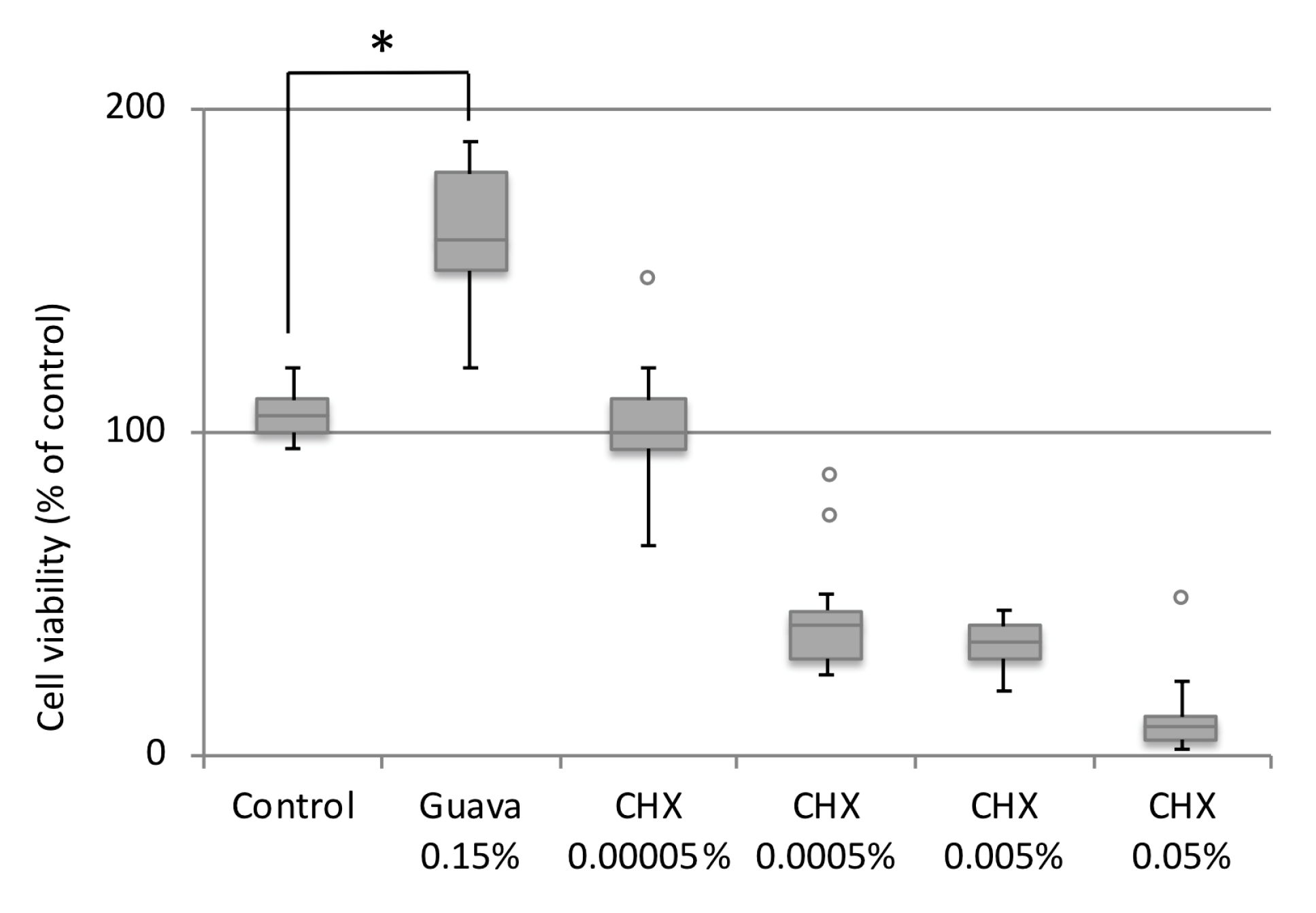
3.4. Effect of Guava Mouth rinse on HGEK-16 Cell Viability
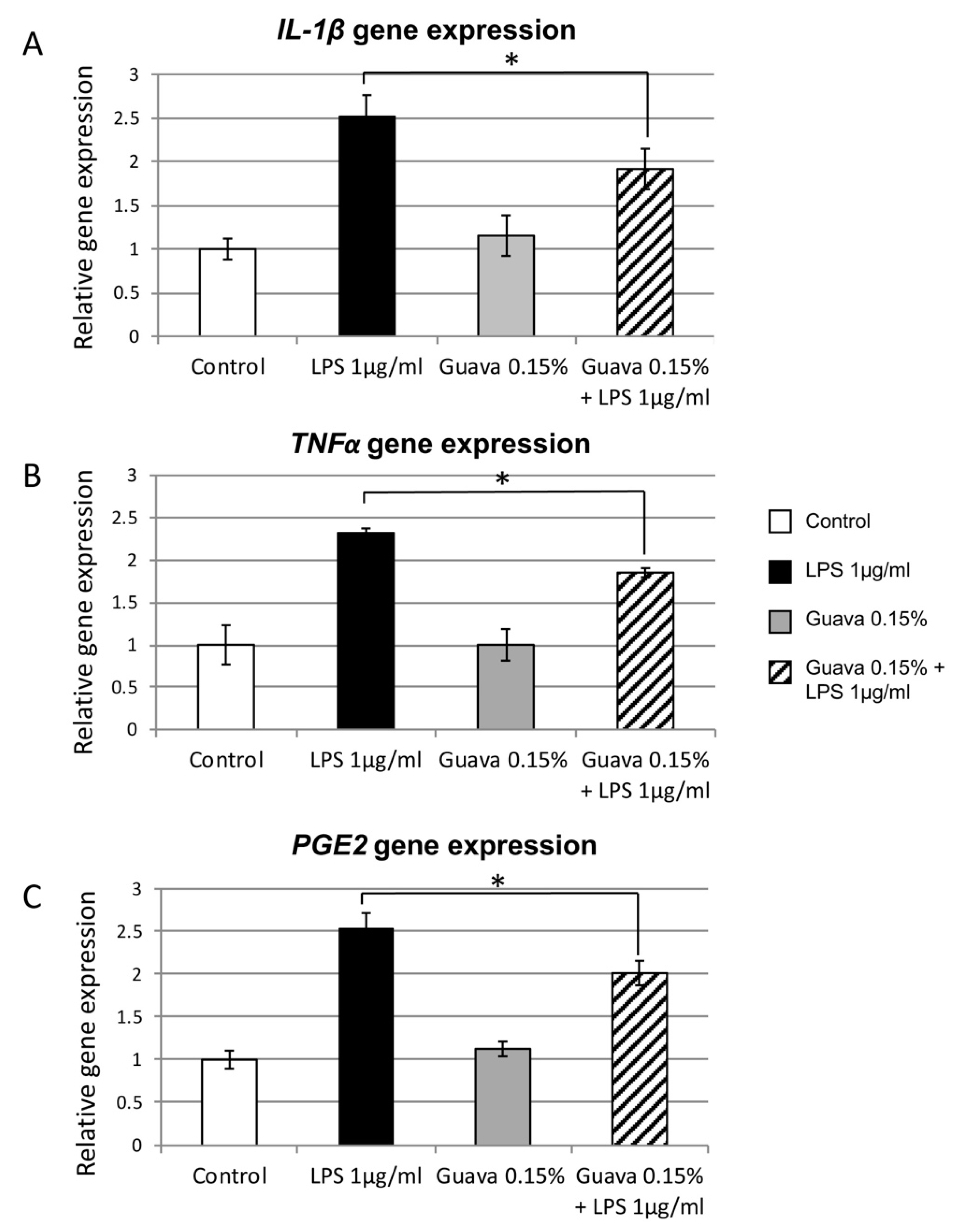
3.5. Anti-Inflammatory Potential of Guava Mouth rinse
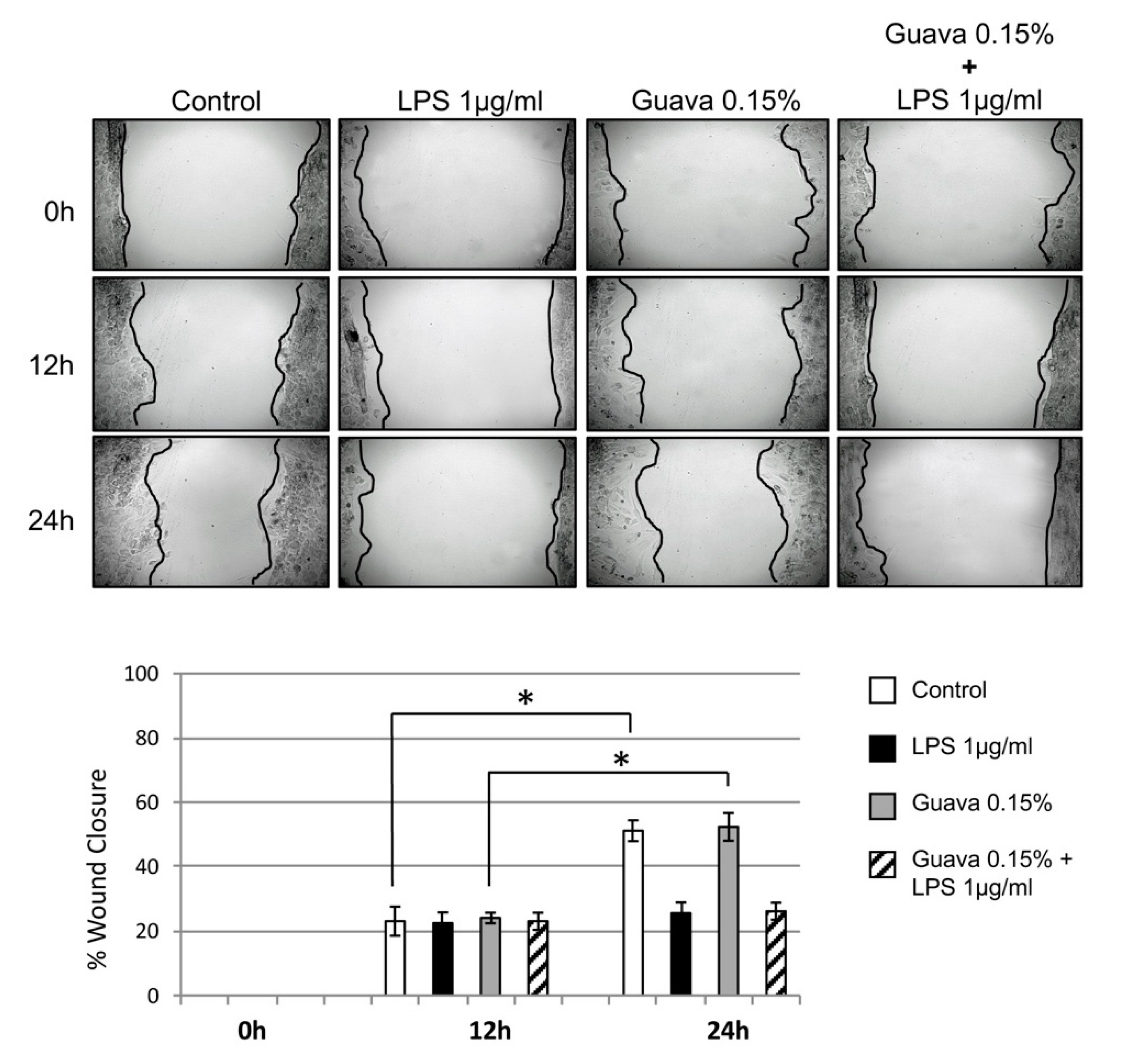
3.6. Scratch Wound Healing Assay (Cell Migration)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Listgarten, M.A. Structure of the microbial flora associated with periodontal health and disease in man. A light and electron microscopic study. J. Periodontol. 1976, 47, 1–18. [Google Scholar] [CrossRef]
- Bidra, A.S.; Daubert, D.M.; Garcia, L.T.; Kosinski, T.F.; Nenn, C.A.; Olsen, J.A.; Platt, J.A.; Wingrove, S.S.; Chandler, N.D.; Curtis, D.A. Clinical practice guidelines for recall and maintenance of patients with tooth-borne and implant-borne dental restorations. J. Am. Dent. Assoc. 2016, 147, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Addy, M.; Moran, J.M. Clinical indications for the use of chemical adjuncts—To plaque control: Chlorhexidine formulations. Periodontology 2000 1997, 15, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Flotra, L.; Gjermo, P.; Rolla, G.; Waerhaug, J. Side effects of chlorhexidine mouth washes. Scand. J. Dent. Res. 1971, 79, 119–125. [Google Scholar] [CrossRef]
- Wyganowska-Swiatkowska, M.; Kotwicka, M.; Urbaniak, P.; Nowak, A.; Skrzypczak-Jankun, E.; Jankun, J. Clinical implications of the growth-suppressive effects of chlorhexidine at low and high concentrations on human gingival fibroblasts and changes in morphology. Int. J. Mol. Med. 2016, 37, 1594–1600. [Google Scholar] [CrossRef]
- Chang, Y.C.; Huang, F.M.; Tai, K.W.; Chou, M.Y. The effect of sodium hypochlorite and chlorhexidine on cultured human periodontal ligament cells. Oral Surg Oral Med. Oral Pathol. Oral. Radiol. 2001, 92, 446–450. [Google Scholar] [CrossRef]
- Lee, T.H.; Hu, C.C.; Lee, S.S.; Chou, M.Y.; Chang, Y.C. Cytotoxicity of chlorhexidine on human osteoblastic cells is related to intracellular glutathione levels. Int. End. J. 2010, 43, 430–435. [Google Scholar] [CrossRef]
- Braga, A.; Pires, J.; Magalhães, A.C. Commercial antimicrobials mouth rinses on caries and periodontitis-related biofilm control: A review of literature. Braz Dent. Sci. 2017, 20, 13–23. [Google Scholar]
- Rolla, G.; Loe, H.N.; Schiott, R.C. Retention of Chlorhexidine in the human oral cavity. Arch. Oral. Biol. 1971, 16, 1109–1116. [Google Scholar] [CrossRef]
- Cousido, M.C.; Carmona, I.T.; García-Caballero, L.; Limeres, J.; Álvarez, M.; Diz, P. In vivo substantivity of 0.12% and 0.2% chlorhexidine mouth rinses on salivary bacteria. Clin. Oral Investig. 2010, 14, 397–402. [Google Scholar] [CrossRef]
- Cieplik, F.; Jakubovics, N.S.; Buchalla, W.; Maisch, T.; Hellwig, E.; Al-Ahmad, A. Resistance toward chlorhexidine in oral bacteria–Is There Cause for Concern? Front. Microbiol. 2019, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Singla, S.; Malhotra, R.; Saxena, S. Antibacterial Efficacy of Mouthwash Prepared from Pomegranate, Grape Seed and Guava Extracts against Oral Streptococci: An in vivo study. J. Clin. Pediatric Dent. 2018, 42, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, A.R.; Suke, D.K.; Martande, S.S.; Singh, S.P.; Nagpal, K.; Naik, S.B. Triphala—A new herbal mouthwash in gingivitis: A randomized controlled clinical trial. J. Periodontol. 2016, 87, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.; Gopalakrishnan, D.; Mehta, V.; Rizwan, S.A.; Shetiya, S.H.; Bagwe, S. Efficacy of green tea-based mouthwashes on dental plaque and gingival inflammation: A systematic review and meta-analysis. Indian J. Dent. Res. 2018, 29, 225–232. [Google Scholar] [PubMed]
- Gutiérrez, R.M.; Mitchell, S.; Solis, R.V. Psidium guajava: A review of its traditional uses, phytochemistry and pharmacology. J. Ethnopharmacol. 2008, 117, 1–27. [Google Scholar] [CrossRef]
- Joseph, B.; Priya, R.M. Review on nutritional, medicinal and pharmacological properties of guava (Psidium guajava linn). Int. J. Pharm. Biol. Sci. 2011, 2, 53–69. [Google Scholar]
- Mittal, P.; Gupta, V.; Kaur, G.; Garg, A.K.; Singh, A. Phytochemistry and pharmacological activities of Psidium guajava: A review. Int. J. Pharm. Sci. Res. 2010, 1, 9–19. [Google Scholar]
- Ravi, K.; Divyashree, P. Psidium guajava: A review on its potential as an adjunct in treating periodontal disease. Pharmacogn. Rev. 2014, 8, 96–100. [Google Scholar]
- Choi, S.Y.; Hwang, J.H.; Park, S.Y.; Jin, Y.J.; Ko, H.C.; Moon, S.W.; Kim, S.J. Fermented guava leaf extract inhibits LPS-induced COX-2 and iNOS expression in mouse macrophage cells by inhibition of transcription factor NF-kappa B. Phytother. Res. 2008, 22, 1030–1034. [Google Scholar] [CrossRef]
- Freitas, C.S.; Diniz, H.F.O.; Gomes, J.B.; Sinisterra, R.D.; Cortés, M.E. Evaluation of the substantivity of chlorhexidine in association with sodium fluoride in vitro. Braz. Oral. Res. 2003, 17, 78–81. [Google Scholar] [CrossRef]
- Guggenheim, B.; Giertsen, E.; Schüpbach, P.; Shapiro, S. Validation of an in vitro Biofilm Model of Supragingival Plaque. J. Dent. Res. 2001, 80, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Addy, M.; Moran, J.; Newcombe, R.; Warren, P. The comparative tea staining potential of phenolic, chlorhexidine and anti-adhesive mouth rinses. J. Clin. Periodontol. 1995, 22, 923–928. [Google Scholar] [CrossRef] [PubMed]
- García-Caballero, L.; Quintas, V.; Prada-López, I.; Seoane, J.; Donos, N.; Tomás, I. Chlorhexidine substantivity on salivary flora and plaque-like biofilm: An in situ model. PLoS ONE 2013, 8, e83522. [Google Scholar] [CrossRef] [PubMed]
- Gomashe, A.V.; Sharma, A.A.; Kasulkar, A. Investigation of biofilm inhibition activity and antibacterial activity of Psidium guajava plant extracts against Streptococcus mutans causing dental plaque. Int. J. Curr. Microbiol. App. Sci. 2014, 3, 335–345. [Google Scholar]
- John, N.R.; Gala, V.C.; Sawant, C.S. Inhibitory effects of plant extracts on multispecies dental biofilm formation invitro. Int. J. Pharm. Bio. Sci. 2013, 4, 487–495. [Google Scholar]
- Stober, T.; Gilde, H.; Lenz, P. Color stability of highly filled composite resin materials for facings. Dent. Mater. 2001, 17, 87–94. [Google Scholar] [CrossRef]
- Miotti, L.L.; Nicoloso, G.F.; Durand, L.B.; Susin, A.H.; Rocha, R.O. Color stability of a resin composite: Effect of the immersion method and surface treatments. Indian J. Dent. Res. 2016, 27, 195–199. [Google Scholar]
- Graziani, F.; Gabriele, M.; D’Aiuto, F.; Suvan, J.; Tonelli, M.; Cei, S. Dental Plaque, Gingival Inflammation and Tooth Discolouration with Different Commercial Formulations of 0.2% Chlorhexidine Rinse: A Double-blind Randomised Controlled Clinical Trial. Oral Health Prev. Dent. 2015, 13, 101–111. [Google Scholar]
- Lee, Y.K.; Powers, J.M. Discoloration of dental resin composites after immersion in a series of organic and chemical solutions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2005, 73, 361–367. [Google Scholar] [CrossRef]
- Bagis, B.; Baltacioglu, E.; Özcan, M.; Ustaomer, S. Evaluation of chlorhexidine gluconate mouth rinse-induced staining using a digital colorimeter: An in vivo study. Quintess Int. 2011, 42, 213–223. [Google Scholar]
- Addy, M.; Sharif, N.; Moran, J. A non-staining chlorhexidine mouthwash? Probably not: A study in vitro. Int. J. Dent. Hyg. 2005, 3, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Hofer, D.; Meier, A.; Sener, B.; Guggenheim, B.; Attin, T.; Schmidlin, P.R. Biofilm reduction and staining potential of a 0.05% chlorhexidine rinse containing essential oils. Int. J. Dent. Hyg. 2011, 9, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, G.H.; Pramanik, R.; Proctor, G.B. An in vitro model of chlorhexidine-induced tooth staining. J. Periodont. Res. 2005, 40, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.C.; Hsieh, C.L.; Huang, K.D.; Ker, Y.B.; Chyau, C.C.; Peng, R.Y. Anticancer activity of rhamnoallosan against DU-145 cells is kinetically complementary to coexisting polyphenolics in Psidium guajava budding leaves. J. Agric. Food Chem. 2009, 57, 6114–6122. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Wu, P.H.; Lo, D.; Pan, Y.C.; Wu, M.C. Hepatoprotective effect of guava (Psidium guajava L.) Leaf extracts on ethanol-induced injury on clone 9 rat liver cells. Food Nut. Sci. 2011, 2, 983–988. [Google Scholar] [CrossRef]
- Wang, X.; Ye, K.; Lv, Y.; Wei, S.; Li, X.; Ma, J.; Zhang, X.; Ye, C. Ameliorative effect and underlying mechanisms of total triterpenoids from Psidium guajava Linn (myrtaceae) leaf on high-fat streptozotocin-induced diabetic peripheral neuropathy in rats. Trop. J. Pharm. Res. 2016, 15, 327–333. [Google Scholar] [CrossRef]
- Kaileh, M.; Vanden, B.W.; Boone, E.; Essawi, T.; Haegeman, G. Screening of indigenous Palestinian medicinal plants for potential anti-inflammatory and cytotoxic activity. J. Ethnopharm 2007, 113, 510–516. [Google Scholar] [CrossRef]
- Jang, M.; Jeong, S.W.; Cho, S.K.; Ahn, K.S.; Kim, B.K.; Kim, J.C. Anti-inflammatory effects of 4 medicinal plant extracts in lipopolysaccharide-induced RAW 264.7 cells. Food Sci. Biotechnol. 2013, 22, 213–220. [Google Scholar] [CrossRef]
- Sen, S.S.; Sukumaran, V.; Giri, S.S.; Park, S.C. Flavonoid fraction of guava leaf extract attenuates lipopolysaccharide-induced inflammatory response via blocking of NF-κB signalling pathway in Labeo rohita macrophages. Fish. Shellfish Immun. 2015, 47, 85–92. [Google Scholar] [CrossRef]
- Jang, M.; Jeong, S.W.; Cho, S.K.; Ahn, K.S.; Lee, J.H.; Yang, D.C.; Kim, J.C. Anti-Inflammatory Effects of an Ethanolic Extract of Guava (Psidium guajava L.) Leaves In vitro and In vivo. J. Med. Food 2014, 17, 678–685. [Google Scholar] [CrossRef]
- Laily, N.; Kusumaningtyas, R.W.; Sukarti, I.; Rini, M.R.D.K. The potency of guava Psidium guajava (L.) leaves as a functional immune-stimulatory ingredient. Procedia Chem. 2015, 14, 301–307. [Google Scholar] [CrossRef] [Green Version]
- Vieira, B.T.; Gonçalves, R.D.; Soncin, R.C.; Gontijo Evangelista, F.C.; Tinoco, L.; de Pilla, V.; Carvalho, M.D.G.; de Paula Sabino, A. Antioxidant, antibacterial and antitumor activity of ethanolic extract of the Psidium guajava leaves. Am. J. Plant Sci. 2014, 5, 3492–3500. [Google Scholar]
- Baroroh, H.N.; Utami, E.D. Harwoko Inhibitory effect of ethanol extract of Psidium guajava leaves in rat active cutaneus anaphylaxis reaction. Int. J. Pharm. Clin. Res. 2016, 8, 1–5. [Google Scholar]
- Addy, M.; Mahadavi, S.A.; Loyn, T. Dietary staining in vitro by mouth rinses as a comparative measure of antiseptic activity and predictor of staining in vivo. J. Dent. 1995, 23, 95–99. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group 1—0.15 % Guava Mouth Rinse | Group 2—0.2% CHX Mouth Rinse | |||||
|---|---|---|---|---|---|---|
| Time (min) | 5 | 30 | 360 | 5 | 30 | 360 |
| Mean ± SD in µg/mL | 8.14 ± 2.41 | 7.010 ± 3.11 | 5.87 ± 4.41 | 177.24 ± 62.07 | 137.62 ± 54.89 | 124.82 ± 39.15 |
| % Release | 29.5% | 16.11% | 19.4% | 57% | 22.5% | 10.25% |
| Group 1 0.15% Guava Mouth Rinse (CFU/mL) | Group 2 0.2% CHX Mouth Rinse (CFU/mL) | Group 3 Distilled Water (CFU/mL) | |
|---|---|---|---|
| Baseline | 1 × 105 | 1 × 105 | 1 × 105 |
| 24 h | 2.03 × 102 ± 0.81 × 102 | 2.8 × 101 ± 0.14 × 101 | 9.05 × 108 ± 2.48 × 1010 |
| 72 h | 1.5 × 101 ± 0.15 × 101 | 0.5 × 101 ± 0.1 × 101 | 1.23 × 109 ± 2.24 × 1011 |
| - | Guava | Chlorhexidine | Distilled Water | |
|---|---|---|---|---|
| Enamel | ΔL | −10.43 ± 2.17 | −18.55 ± 6.52 | −8.85 ± 4.16 |
| Δa | 4.36 ± 0.23 B | 9.82 ± 4.57 C | 2.30 ± 0.33 B,C | |
| Δb | 12.02 ± 0.98 B | 18.82 ± 8.75 C | 4.39 ± 4.70 B,C | |
| ΔE | 13.50 ± 1.64 | 24.27 ± 9.55 | 9.11 ± 4.21 | |
| Dentin | ΔL | −10.04 ± 1.12 A | −31.42 ± 5.38 A,C | −11.69 ± 3.07 C |
| Δa | 7.11 ± 1.02 A,B | 18.03 ± 2.28 A,C | 2.03 ± 0.24 B,C | |
| Δb | 15.91 ± 1.91 A,B | 26.92 ± 2.60 A,C | 4.86 ± 0.73 B,C | |
| ΔE | 16.07 ± 1.56 A | 43.15 ± 6.79 A,C | 12.58 ± 3.12 C | |
| Composite | ΔL | 2.06 ± 2.22 | −3.66 ± 4.78 C | 6.42 ± 3.26 C |
| Δa | 3.80 ± 1.96 A,B | 6.64 ± 0.65 A,C | 1.04 ± 0.35 B,C | |
| Δb | 7.40 ± 2.99 | 10.32 ± 1.14 C | 3.70 ± 0.49 C | |
| ΔE | −1.088 ± 1.46 | 5.21 ± 4.8 C | −6.21 ± 3.19 C |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varghese, J.; Ramenzoni, L.L.; Shenoy, P.; Nayak, U.Y.; Nayak, N.; Attin, T.; Schmidlin, P.R. In Vitro Evaluation of Substantivity, Staining Potential, and Biofilm Reduction of Guava Leaf Extract Mouth Rinse in Combination with its Anti-Inflammatory Effect on Human Gingival Epithelial Keratinocytes. Materials 2019, 12, 3903. https://doi.org/10.3390/ma12233903
Varghese J, Ramenzoni LL, Shenoy P, Nayak UY, Nayak N, Attin T, Schmidlin PR. In Vitro Evaluation of Substantivity, Staining Potential, and Biofilm Reduction of Guava Leaf Extract Mouth Rinse in Combination with its Anti-Inflammatory Effect on Human Gingival Epithelial Keratinocytes. Materials. 2019; 12(23):3903. https://doi.org/10.3390/ma12233903
Chicago/Turabian StyleVarghese, J., L. L. Ramenzoni, P. Shenoy, U. Y. Nayak, N. Nayak, T. Attin, and P. R. Schmidlin. 2019. "In Vitro Evaluation of Substantivity, Staining Potential, and Biofilm Reduction of Guava Leaf Extract Mouth Rinse in Combination with its Anti-Inflammatory Effect on Human Gingival Epithelial Keratinocytes" Materials 12, no. 23: 3903. https://doi.org/10.3390/ma12233903