Evaluation of Peri-Implant Bone Grafting Around Surface-Porous Dental Implants: An In Vivo Study in a Goat Model

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Model
2.2. Study Design
- Solid Dental Implants (SI, n1 = 12): Tapered Screw-Vent®, Zimmer Dental Inc., Carlsbad, CA, USA.
- Porous Dental Implants (PI, n2 = 12): Trabecular Metal®, Zimmer Dental Inc., Carlsbad, CA, USA.
- Porous Dental Implants with BCP peri-implant bone grafting (PI + BCP, n3 = 12): Trabecular Metal® Implant placement was combined with peri-implant bone grafting using biphasic calcium phosphate (BCP) granulates (Maxresorb®, Biotiss Biomaterials, Zossen, Germany). Maxresorb® granules, composed of 60% hydroxyapatite (HA) and 40% beta-tricalcium phosphate (β-TCP).
2.3. Sample Size Calculation
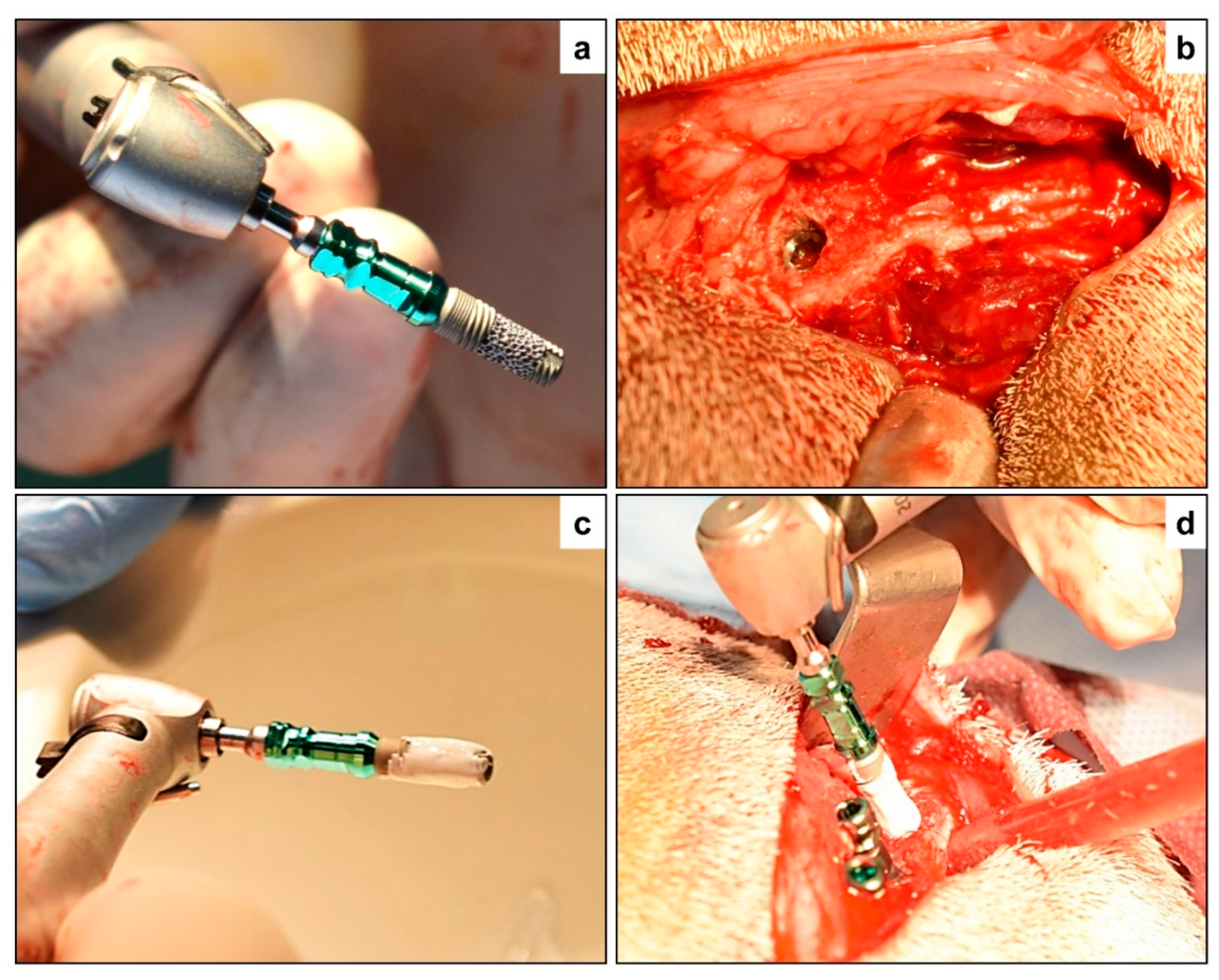
2.4. Surgical Protocol
2.5. Study Endpoint and Specimen Collection
3. Analytical Protocols
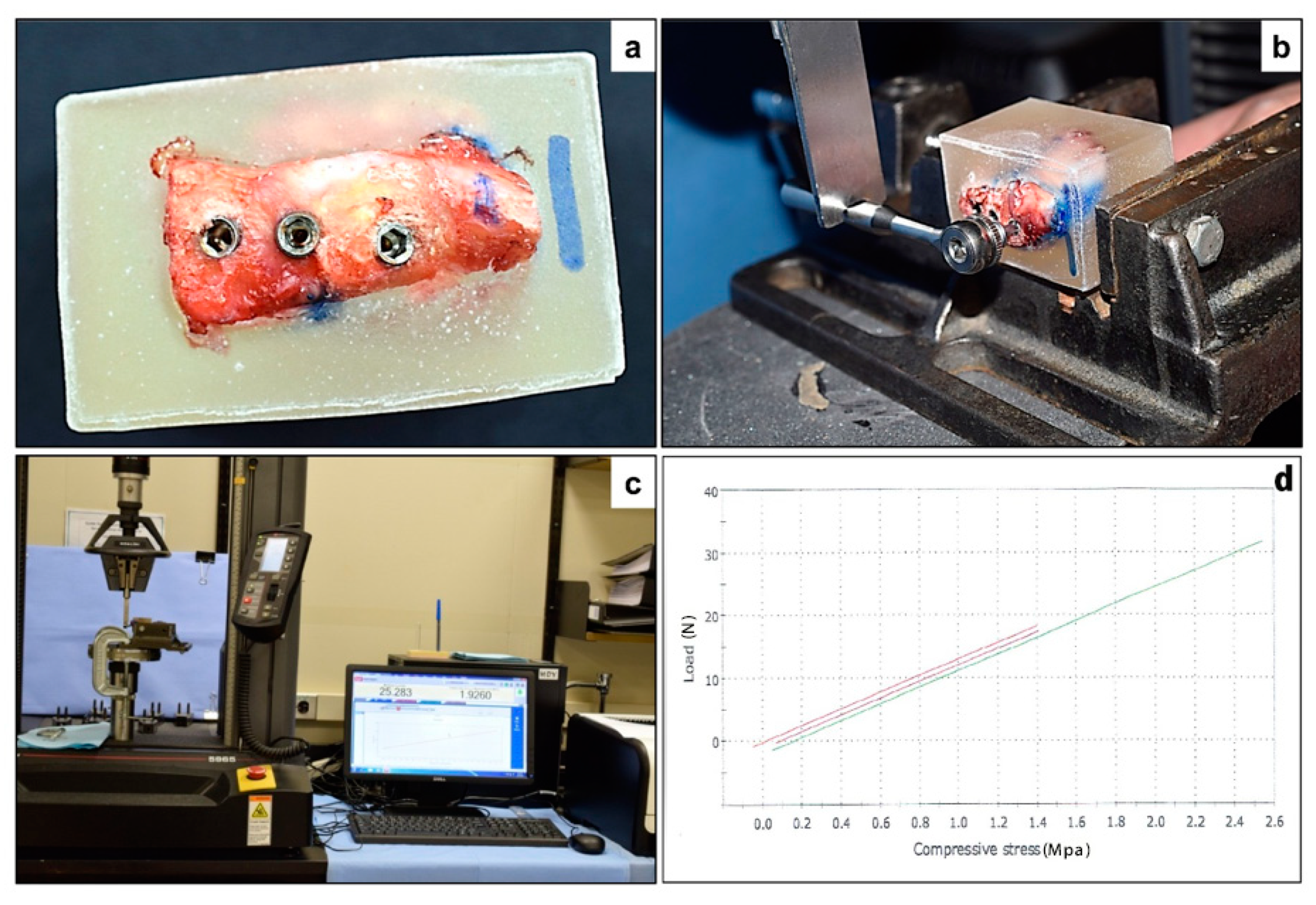
3.1. Biomechanical Testing
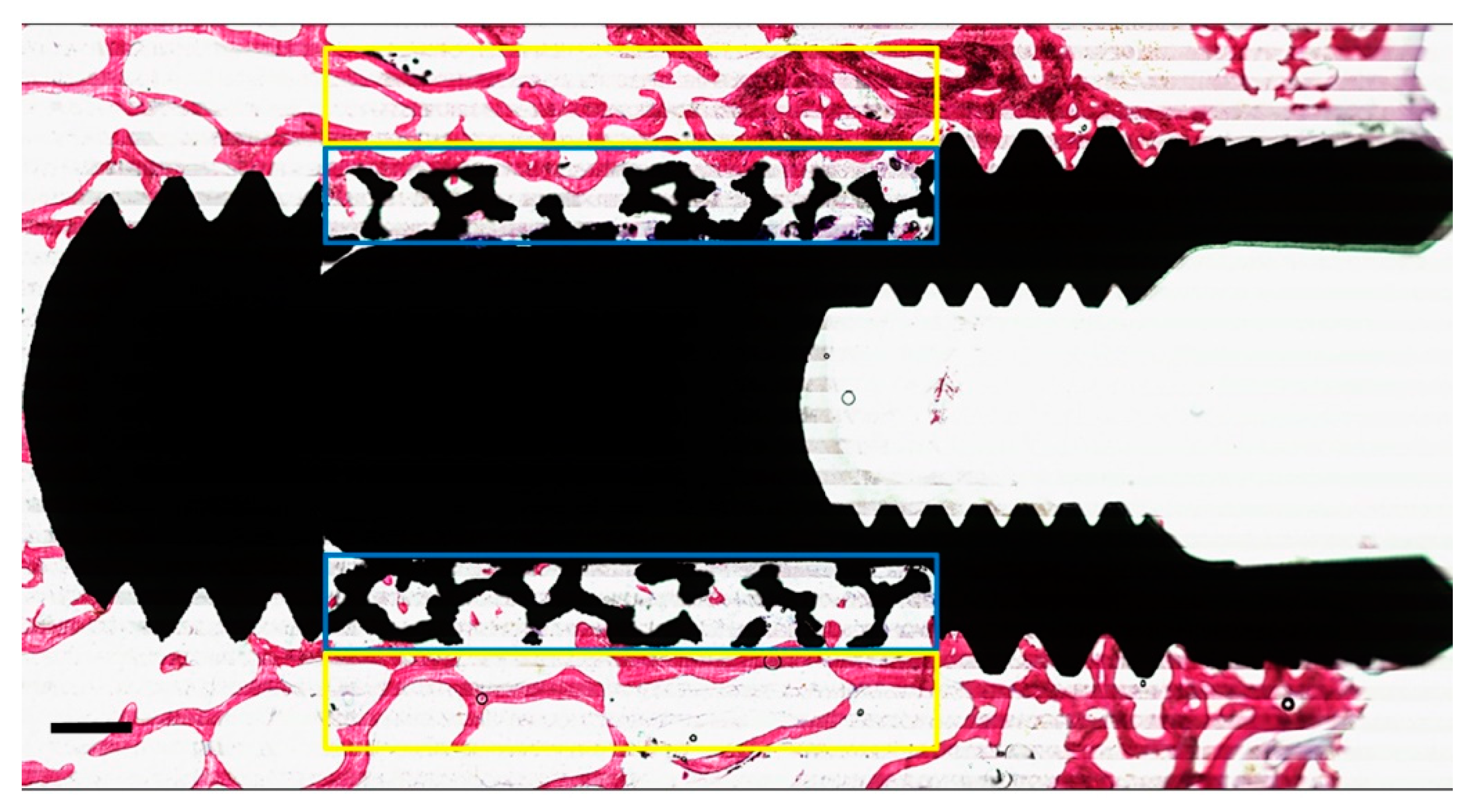
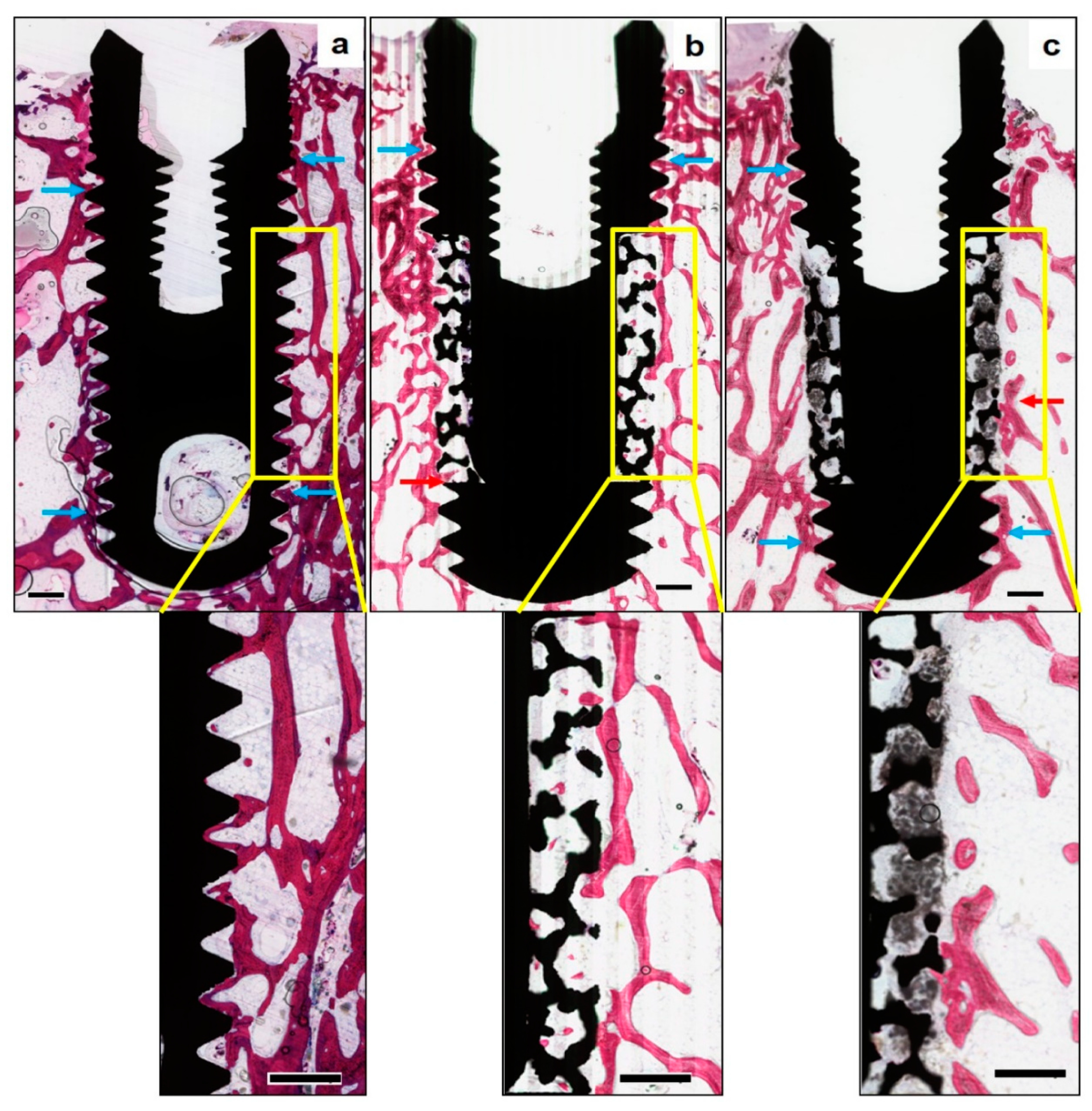
3.2. Histological and Histomorphometrical Evaluation
3.3. Statistical Analysis
4. Results
4.1. Post-Operative Observations
4.2. Biomechanical Testing (n = 6 Implants Per Group)
4.3. Histologic and Histomorphometrical Analysis (n = 6 Implants Per Group)
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sykaras, N.; Iacopino, A.M.; Marker, V.A.; Triplett, R.G.; Woody, R.D. Implant materials, designs, and surface topographies: Their effect on osseointegration. A literature review. Int. J. Oral Maxillofac. Implants 1999, 15, 675–690. [Google Scholar]
- Gaviria, L.; Salcido, J.P.; Guda, T.; Ong, J.L. Current trends in dental implants. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Emami, E.; de Souza, R.F.; Kabawat, M.; Feine, J.S. The impact of edentulism on oral and general health. Int. J. Dent. 2013, 2013, 498305. [Google Scholar] [CrossRef] [PubMed]
- Steigenga, J.T.; Al-Shammari, K.F.; Nociti, F.H.; Misch, C.E.; Wang, H.L. Dental implant design and its relationship to long-term implant success. Implants Dent. 2003, 12, 306–317. [Google Scholar] [CrossRef]
- Bencharit, S.; Byrd, W.C.; Altarawneh, S.; Hosseini, B.; Leong, A.; Reside, G.; Morelli, T.; Offenbacher, S. Development and Applications of Porous Tantalum Trabecular Metal-Enhanced Titanium Dental Implants. Clin. Implants Dent. Relat. Res. 2014, 16, 817–826. [Google Scholar] [CrossRef]
- Schlee, M.; Schoor, W.P.; Schoor, A.R. Immediate Loading of Trabecular Metal-Enhanced Titanium Dental Implants: Interim Results from an International Proof-of-Principle Study. Clin. Implant Dent. Relat. Res. 2015, 17, e308–e320. [Google Scholar] [CrossRef]
- Kim, D.-G.; Huja, S.S.; Tee, B.C.; Larsen, P.E.; Kennedy, K.S.; Chien, H.H.; Lee, J.W.; Wen, H.B. Bone ingrowth and initial stability of titanium and porous tantalum dental implants: A pilot canine study. Implants Dent. 2013, 22, 399–405. [Google Scholar] [CrossRef]
- Tabassum, A.; Meijer, G.J.; Wolke, J.G.; Jansen, J.A. Influence of the surgical technique and surface roughness on the primary stability of an implant in artificial bone with a density equivalent to maxillary bone: A laboratory study. Clin. Oral Implants Res. 2009, 20, 327–332. [Google Scholar] [CrossRef]
- Lekholm, U. Patient selection and preparation. In Tissue-Integrated Prostheses Osseointegration in Clinical Dentistry; Quintessence: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Martinez, H.; Davarpanah, M.; Missika, P.; Celletti, R.; Lazzara, R. Optimal implant stabilization in low density bone. Clin. Oral Implants Res. 2001, 12, 423–432. [Google Scholar] [CrossRef]
- Jaffin, R.A.; Berman, C.L. The Excessive Loss of Branemark Fixtures in Type IV Bone: A 5-Year Analysis. J. Periodontol. 1991, 62, 2–4. [Google Scholar] [CrossRef]
- Alsaadi, G.; Quirynen, M.; Komárek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of oral implant failures, up to abutment connection. J. Clin. Periodontol. 2007, 34, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Biemond, J.E.; Aquarius, R.; Verdonschot, N.; Buma, P. Frictional and bone ingrowth properties of engineered surface topographies produced by electron beam technology. Arch. Orthop. Trauma Surg. 2011, 131, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Vandamme, K.; Naert, I.; Vander Sloten, J.; Puers, R.; Duyck, J. Effect of implant surface roughness and loading on peri-implant bone formation. J. Periodontol. 2008, 79, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Brentel, A.S.; de Vasconcellos, L.M.R.; Oliveira, M.V.; Graça, M.L.; de Vasconcellos, L.G.; Cairo, C.A.; Carvalho, Y.R. Histomorphometric analysis of pure titanium implants with porous surface versus rough surface. J. Appl. Oral Sci. 2006, 14, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Kujala, S.; Ryhänen, J.; Danilov, A.; Tuukkanen, J. Effect of porosity on the osteointegration and bone ingrowth of a weight-bearing nickel–titanium bone graft substitute. Biomaterials 2003, 24, 4691–4697. [Google Scholar] [CrossRef]
- Coelho, P.G.; Granjeiro, J.M.; Romanos, G.E.; Suzuki, M.; Silva, N.R.; Cardaropoli, G.; Thompson, V.P.; Lemons, J.E. Basic research methods and current trends of dental implant surfaces. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 88, 579–596. [Google Scholar] [CrossRef]
- Mittal, Y.; Jindal, G.; Garg, S. Bone manipulation procedures in dental implants. Indian J. Dent. 2016, 7, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Jamjoom, A.; Cohen, R.E. Grafts for Ridge Preservation. J. Funct. Biomater. 2015, 6, 833–848. [Google Scholar] [CrossRef]
- Wähnert, D.; Lange, J.; Schulze, M.; Lenschow, S.; Stange, R.; Raschke, M.J. The potential of implant augmentation in the treatment of osteoporotic distal femur fractures: A biomechanical study. Injury 2013, 44, 808–812. [Google Scholar] [CrossRef]
- Charnley, J. The bonding of prostheses to bone by cement. J. Bone Jt. Surg. Br. 1964, 46, 518–529. [Google Scholar] [CrossRef]
- Haas, S.; Brauer, G.; Dickson, G. A characterization of polymethylmethacrylate bone cement. J. Bone Jt. Surg. 1975, 57, 380–391. [Google Scholar] [CrossRef]
- Yi, X.; Wang, Y.; Lu, H.; Li, C.; Zhu, T. Augmentation of pedicle screw fixation strength using an injectable calcium sulfate cement: An in vivo study. Spine 2008, 33, 2503–2509. [Google Scholar] [CrossRef] [PubMed]
- Schreurs, B.W.; Arts, J.J.; Verdonschot, N. Femoral component revision with use of impaction bone-grafting and a cemented polished stem. Surgical technique. JBJS 2006, 88 (Suppl. 1), 259–274. [Google Scholar] [CrossRef]
- Sehlke, B.M.; Wilson, T.G.; Jones, A.A.; Yamashita, M.; Cochran, D.L. The use of a magnesium-based bone cement to secure immediate dental implants. Int. J. Oral Maxillofac. Implants 2012, 28, e357–e367. [Google Scholar] [CrossRef] [PubMed]
- Sharan, A.; Madjar, D. Maxillary sinus pneumatization following extractions: A radiographic study. Int. J. Oral Maxillofac. Implants 2008, 23, 48–56. [Google Scholar]
- Bohner, M. Calcium orthophosphates in medicine: From ceramics to calcium phosphate cements. Injury 2000, 31, D37–D47. [Google Scholar] [CrossRef]
- Ginebra, M.-P.; Traykova, T.; Planell, J. Calcium phosphate cements as bone drug delivery systems: A review. J. Control. Release 2006, 113, 102–110. [Google Scholar] [CrossRef]
- Takagi, S.; Chow, L.; Ishikawa, K. Formation of hydroxyapatite in new calcium phosphate cements. Biomaterials 1998, 19, 1593–1599. [Google Scholar] [CrossRef]
- Lobo, S.E.; Arinzeh, T.L. Biphasic Calcium Phosphate Ceramics for Bone Regeneration and Tissue Engineering Applications. Materials 2010, 3, 815–826. [Google Scholar] [CrossRef] [Green Version]
- van der Lubbe, H.B.M.; Klein, C.P.A.T.; de Groot, K. A Simple Method for Preparing Thin (10 μm) Histological Sections of Undecalcified Plastic Embedded Bone with Implants. Stain Technol. 1988, 63, 171–176. [Google Scholar] [CrossRef]
- Schouten, C.; Meijer, G.J.; van den Beucken, J.J.; Spauwen, P.H.; Jansen, J.A. A novel implantation model for the evaluation of the bone healing response to dental implants: The goat iliac crest. Clin. Oral Implants Res. 2010, 21, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Pattanayak, D.K.; Fukuda, A.; Matsushita, T.; Takemoto, M.; Fujibayashi, S.; Sasaki, K.; Nishida, N.; Nakamura, T.; Kokubo, T. Bioactive Ti metal analogous to human cancellous bone: Fabrication by selective laser melting and chemical treatments. Acta Biomater. 2011, 7, 1398–1406. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Fiorillo, L.; Herford, A.S.; Crimi, S.; Bianchi, A.; D'Amico, C.; Laino, L.; Cervino, G. Bioactive Titanium Surfaces: Interactions of Eukaryotic and Prokaryotic Cells of Nano Devices Applied to Dental Practice. Biomedicines 2019, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Baldini, N.; Martinolli, M.; Xhanari, E.; Kim, Y.J.; Cervino, G.; Meloni, S.M. Do the New Hydrophilic Surface Have Any Influence on Early Success Rate and Implant Stability during Osseointegration Period? Four-Month Preliminary Results from a Split-Mouth, Randomized Controlled Trial. Eur. J. Dent. 2019, 13, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Vasconcellos, L.M.R.; Leite, D.O.; Oliveira, F.N.; Carvalho, Y.R.; Cairo, C.A. Evaluation of bone ingrowth into porous titanium implant: Histomorphometric analysis in rabbits. Braz. Oral Res. 2010, 24, 399–405. [Google Scholar] [CrossRef]
- Taniguchi, N.; Fujibayashi, S.; Takemoto, M.; Sasaki, K.; Otsuki, B.; Nakamura, T.; Matsushita, T.; Kokubo, T.; Matsuda, S. Effect of pore size on bone ingrowth into porous titanium implants fabricated by additive manufacturing: An in vivo experiment. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 59, 690–701. [Google Scholar] [CrossRef]
- Lembert, E.; Galante, J.; Rosiokir, W. Fixation of skeletal replacement by fiber metal composites. Clin. Orthop. Relat. Res. 1972, 87, 303–310. [Google Scholar] [CrossRef]
- Clemow, A.; Weinstein, A.; Klawitter, J.; Koeneman, J.; Anderson, J. Interface mechanics of porous titanium implants. J. Biomed. Mater. Res. Part A 1981, 15, 73–82. [Google Scholar] [CrossRef]
- Bobyn, J.D.; Pilliar, R.M.; Cameron, H.U.; Weatherly, G.C. The optimum pore size for the fixation of porous-surfaced metal implants by the ingrowth of bone. Clin. Orthop. Relat. Res. 1980, 150, 263–270. [Google Scholar] [CrossRef]
- Robertson, D.M.; St Pierre, L.; Chahal, R. Preliminary observations of bone ingrowth into porous materials. J. Biomed. Mater. Res. Part A 1976, 10, 335–344. [Google Scholar] [CrossRef]
- Hara, D.; Nakashima, Y.; Sato, T.; Hirata, M.; Kanazawa, M.; Kohno, Y.; Yoshimoto, K.; Yoshihara, Y.; Nakamura, A.; Nakao, Y.; et al. Bone bonding strength of diamond-structured porous titanium-alloy implants manufactured using the electron beam-melting technique. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 59, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Bobyn, J.; Stackpool, G.; Hacking, S.; Tanzer, M.; Krygier, J.J. Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial. J. Bone Jt. Surg. Br. 1999, 81, 907–914. [Google Scholar] [CrossRef]
- Bobyn, J.; Wilson, G.; MacGregor, D.; Pilliar, R.M.; Weatherly, G.C. Effect of pore size on the peel strength of attachment of fibrous tissue to porous-surfaced implants. J. Biomed. Mater. Res. 1982, 16, 571–584. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.D.; Walsh, K.A.; Haddad, J.R. Interface mechanics and bone growth into porous Co-Cr-Mo alloy implants. Clin. Orthop. Relat. Res. 1985, 193, 271–280. [Google Scholar] [CrossRef]
- Itälä, A.I.; Ylänen, H.O.; Ekholm, C.; Karlsson, K.H.; Aro, H.T. Pore diameter of more than 100 μm is not requisite for bone ingrowth in rabbits. J. Biomed. Mater. Res. 2001, 58, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Kent, J.N. Placement of endosseous implants into tooth extraction sites. J. Oral Maxillofac. Surg. 1991, 49, 1269–1276. [Google Scholar] [CrossRef]
- Buser, D.; Chen, S.T.; Weber, H.P.; Belser, U.C. Early implant placement following single-tooth extraction in the esthetic zone: Biologic rationale and surgical procedures. Int. J. Periodont. Restor. Dent. 2008, 28, 441–451. [Google Scholar]
- Paré, P.E.; Chappuis, J.L.; Rampersaud, R.; Agarwala, A.O.; Perra, J.H.; Erkan, S.; Wu, C. Biomechanical evaluation of a novel fenestrated pedicle screw augmented with bone cement in osteoporotic spines. Spine 2011, 36, E1210–E1214. [Google Scholar] [CrossRef]
- Rohmiller, M.T.; Schwalm, D.; Glattes, R.C.; Elalayli, T.G.; Spengler, D.M. Evaluation of calcium sulfate paste for augmentation of lumbar pedicle screw pullout strength. Spine J. 2002, 2, 255–260. [Google Scholar] [CrossRef]
- Tan, J.-S.; Kwon, B.K.; Dvorak, M.F.; Fisher, C.G.; Oxland, T.R. Pedicle screw motion in the osteoporotic spine after augmentation with laminar hooks, sublaminar wires, or calcium phosphate cement: A comparative analysis. Spine 2004, 29, 1723–1730. [Google Scholar] [CrossRef]
- Castilho, M.; Moseke, C.; Ewald, A.; Gbureck, U.; Groll, J.; Pires, I.; Teßmar, J.; Vorndran, E. Direct 3D powder printing of biphasic calcium phosphate scaffolds for substitution of complex bone defects. Biofabrication 2014, 6, 015006. [Google Scholar] [CrossRef] [PubMed]
- Barrère, F.; van Blitterswijk, C.A.; de Groot, K. Bone regeneration: Molecular and cellular interactions with calcium phosphate ceramics. Int. J. Nanomed. 2006, 1, 317. [Google Scholar]
- Daculsi, G.; Uzel, A.; Weiss, P.; Goyenvalle, E.; Aguado, E. Developments in injectable multiphasic biomaterials. The performance of microporous biphasic calcium phosphate granules and hydrogels. J. Mater. Sci. Mater. Med. 2010, 21, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Fellah, B.H.; Weiss, P.; Gauthier, O.; Rouillon, T.; Pilet, P.; Daculsi, G.; Layrolle, P. Bone repair using a new injectable self-crosslinkable bone substitute. J. Orthop. Res. 2006, 24, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, O.; Goyenvalle, E.; Bouler, J.-M.; Guicheux, J.; Pilet, P.; Weiss, P.; Daculsi, G. Macroporous biphasic calcium phosphate ceramics versus injectable bone substitute: A comparative study 3 and 8 weeks after implantation in rabbit bone. J. Mater. Sci. Mater. Med. 2001, 12, 385–390. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Biphasic, triphasic and multiphasic calcium orthophosphates. Acta Biomater. 2012, 8, 963–977. [Google Scholar] [CrossRef]
- Yin, B.; Ma, P.; Chen, J.; Wang, H.; Wu, G.; Li, B.; Li, Q.; Huang, Z.; Qiu, G.; Wu, Z. Hybrid Macro-Porous Titanium Ornamented by Degradable 3D Gel/nHA Micro-Scaffolds for Bone Tissue Regeneration. Int. J. Mol. Sci. 2016, 17, 575. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Quantitative Variables | STI Implants | PTI Implants | PTI + BCP Implants | - | |||
|---|---|---|---|---|---|---|---|
| N | Mean ± SD | N | Mean ± SD | N | Mean ± SD | ||
| Maximum load (N) | 6 | 19.05 ± 10.19 | 6 | 25.69 ± 4.31 | 6 | 18.57 ± 7.57 | p > 0.05 * |
| Peri-implant Bone Area (PIBA%) | 6 | 8.63 ± 3.93 | 6 | 9.89 ± 3.69 | 6 | 9.28 ± 2.61 | p > 0.05 * |
| Bone growth Area (BGA%) | - | 10.67 ± 4.61 | 6.50 ± 6.53 | p < 0.05 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshehri, F.; Alshehri, M.; Sumague, T.; Niazy, A.; Jansen, J.; van den Beucken, J.; Alghamdi, H. Evaluation of Peri-Implant Bone Grafting Around Surface-Porous Dental Implants: An In Vivo Study in a Goat Model. Materials 2019, 12, 3606. https://doi.org/10.3390/ma12213606
Alshehri F, Alshehri M, Sumague T, Niazy A, Jansen J, van den Beucken J, Alghamdi H. Evaluation of Peri-Implant Bone Grafting Around Surface-Porous Dental Implants: An In Vivo Study in a Goat Model. Materials. 2019; 12(21):3606. https://doi.org/10.3390/ma12213606
Chicago/Turabian StyleAlshehri, Fahad, Mohammed Alshehri, Terrence Sumague, Abdurahman Niazy, John Jansen, Jeroen van den Beucken, and Hamdan Alghamdi. 2019. "Evaluation of Peri-Implant Bone Grafting Around Surface-Porous Dental Implants: An In Vivo Study in a Goat Model" Materials 12, no. 21: 3606. https://doi.org/10.3390/ma12213606