Nanoporous 3D-Printed Scaffolds for Local Doxorubicin Delivery in Bone Metastases Secondary to Prostate Cancer


Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Lines and Patient-Derived Cells
2.2. Metabolic Activity and Proliferation Assays
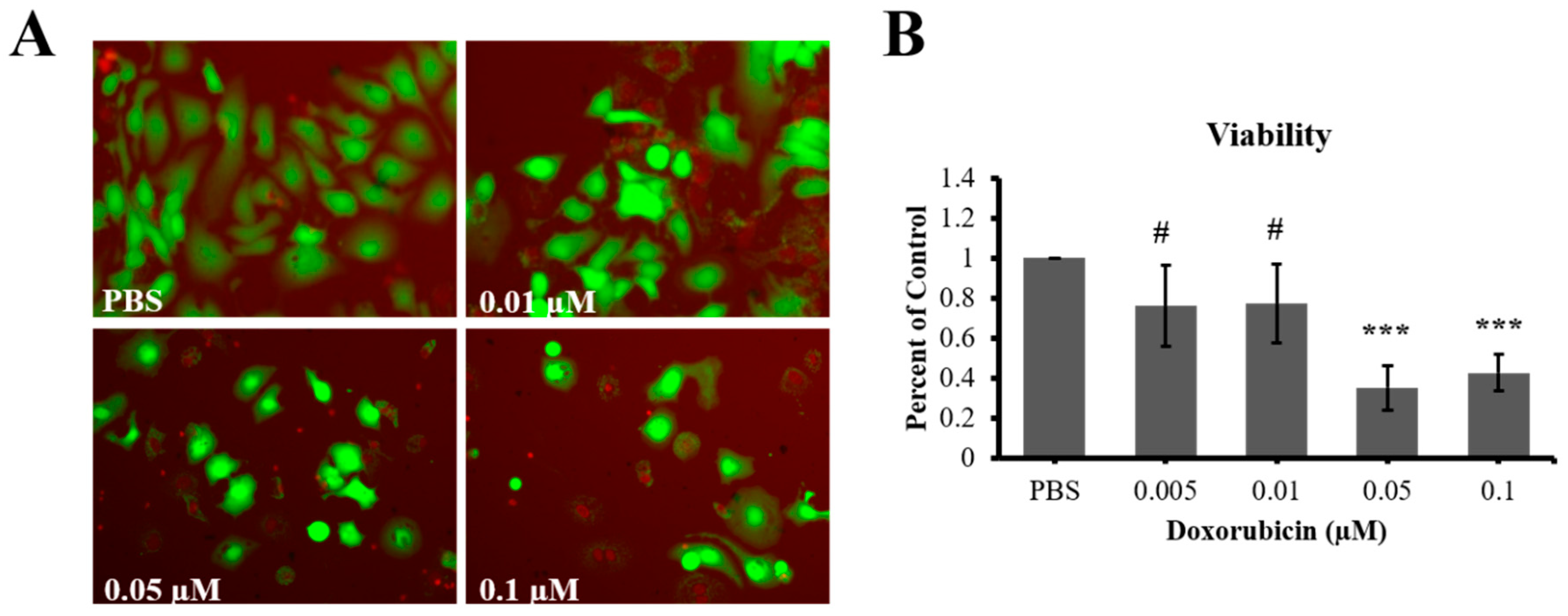
2.3. Live/Dead Viability Assay
2.4. Boyden Chamber Migration Assay
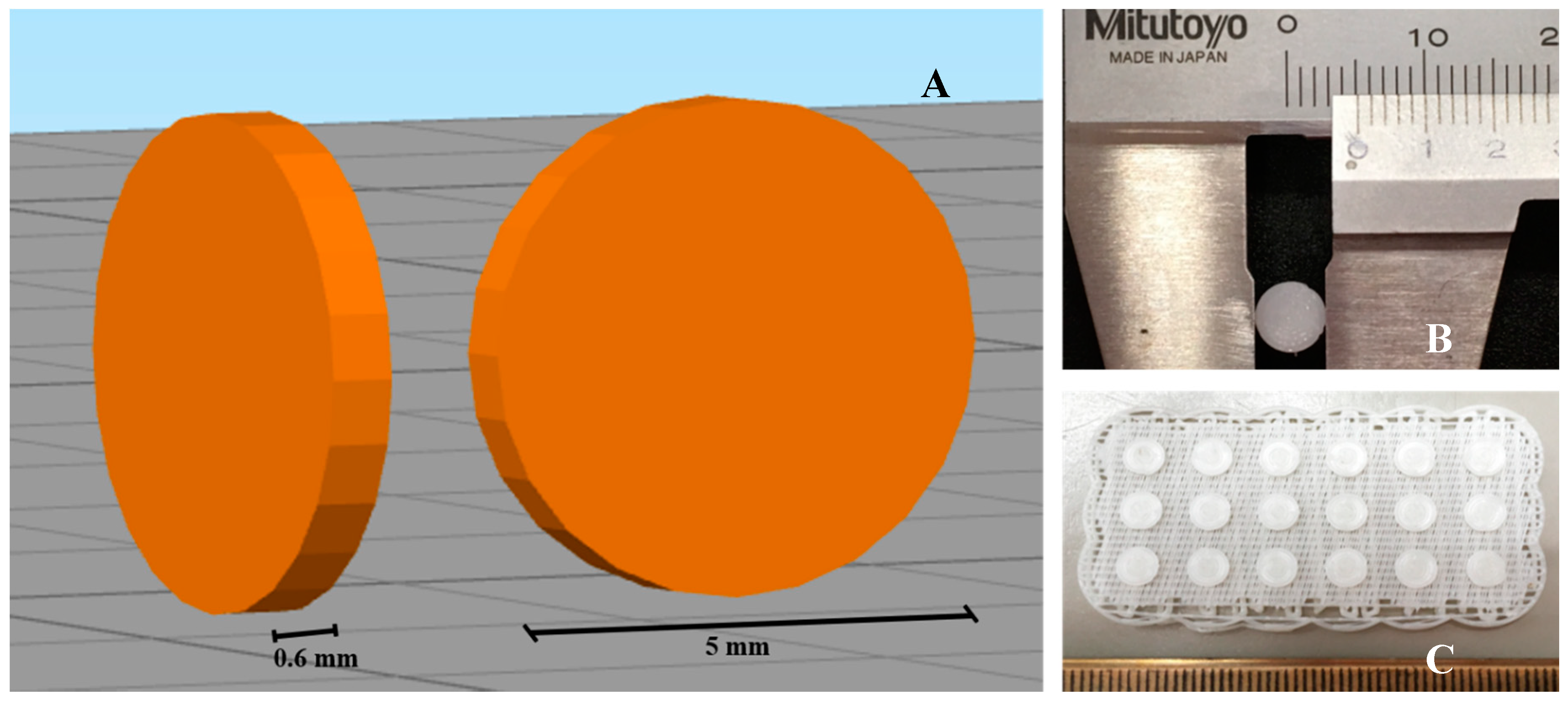
2.5. 3D Printing of Scaffolds
2.6. Assessment of Doxorubicin Release from Scaffolds
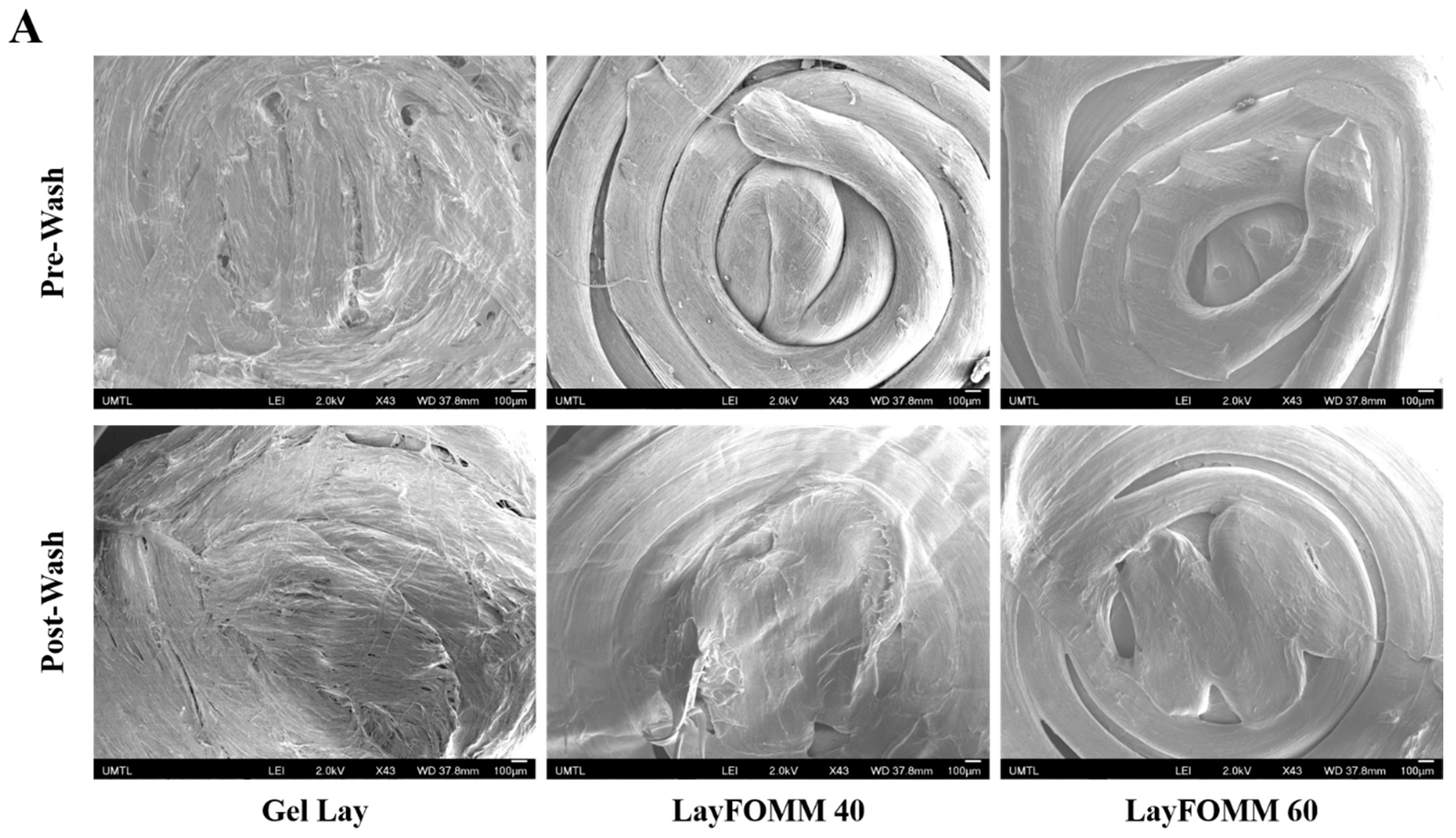
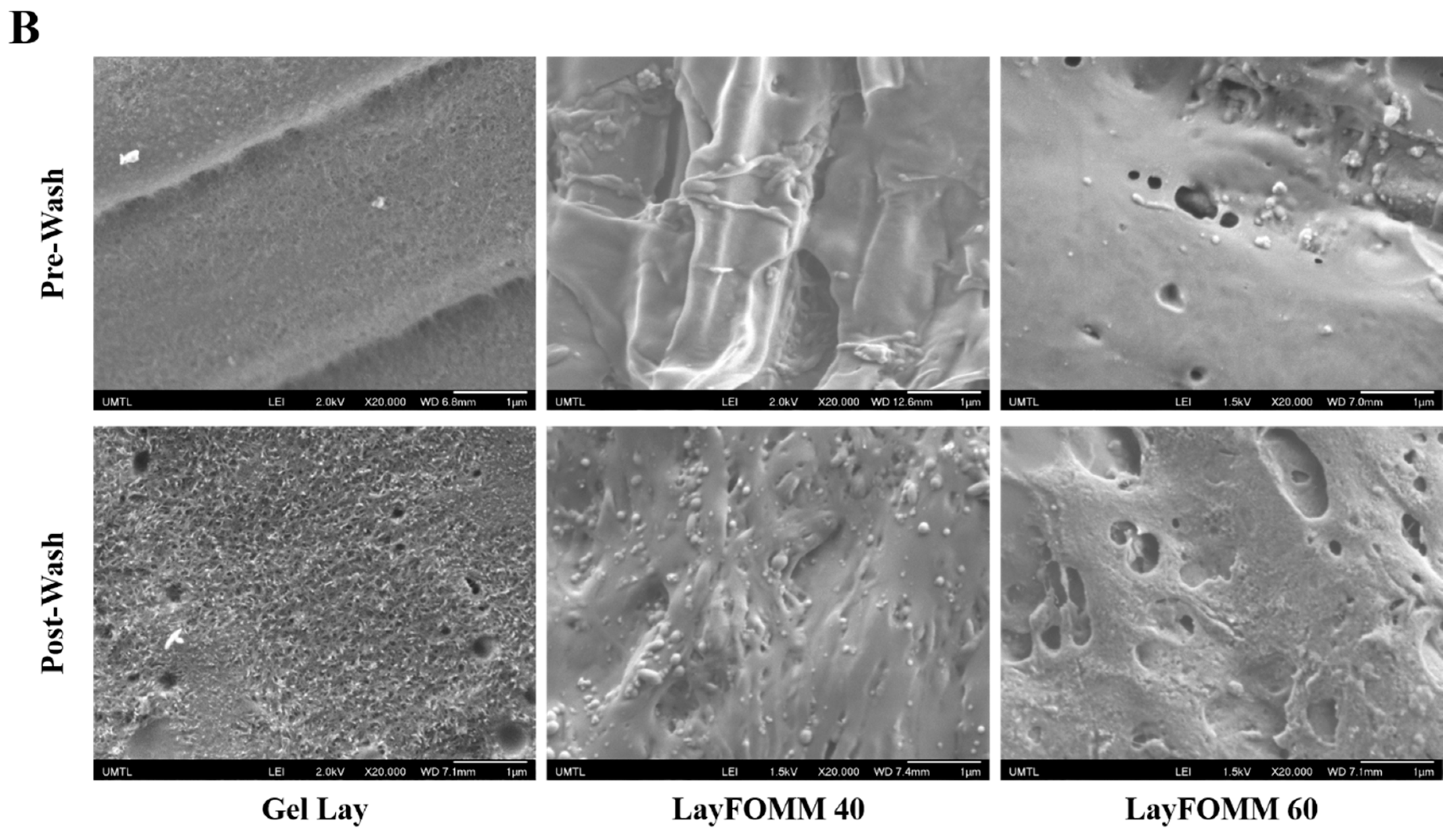
2.7. Scanning Electron Microscopy
2.8. Statistical Analysis
3. Results
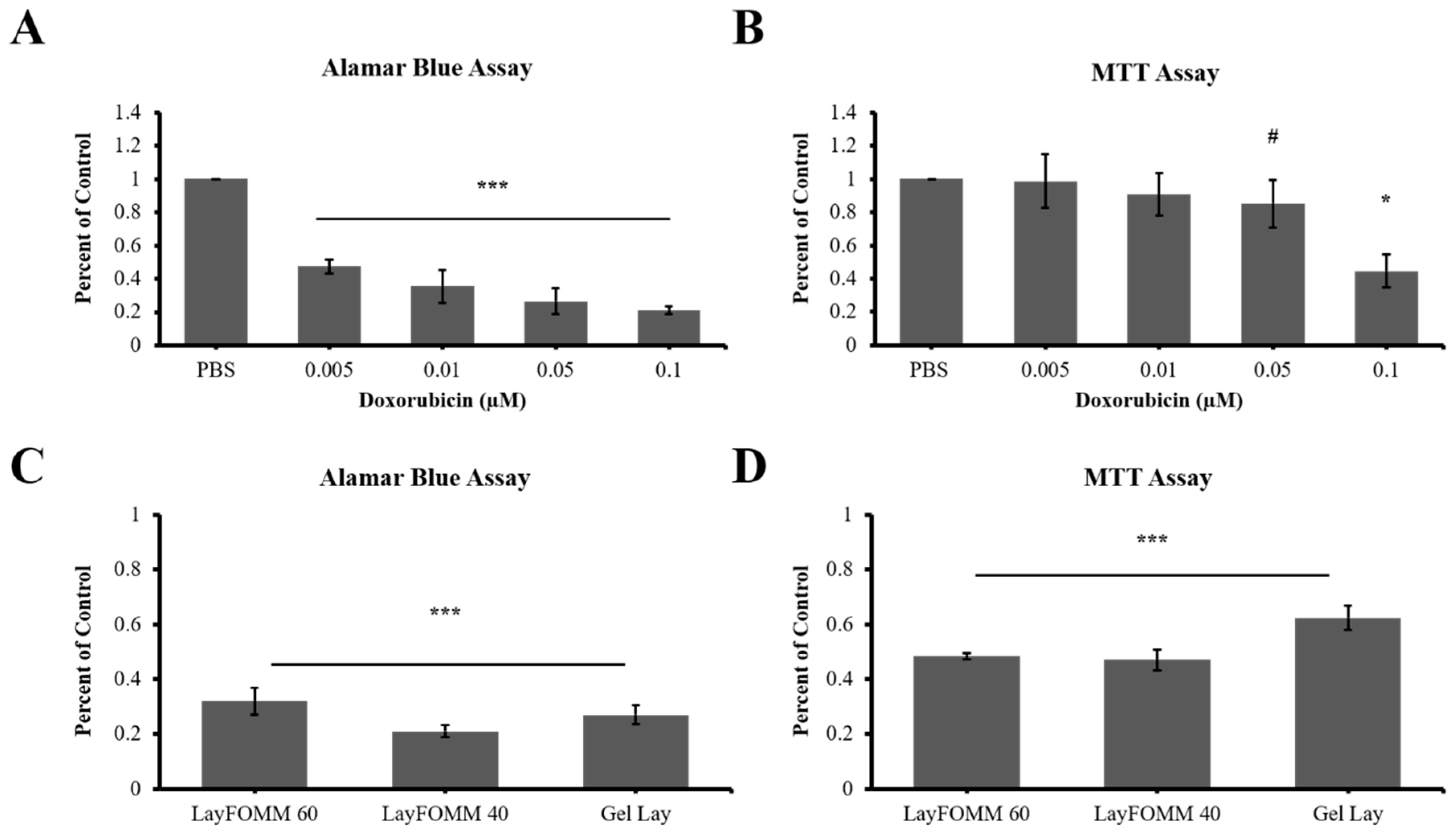
3.1. Evaluation of Effective Doxorubicin Dosage for LAPC4 Cells
3.2. 3D Scaffold Structure
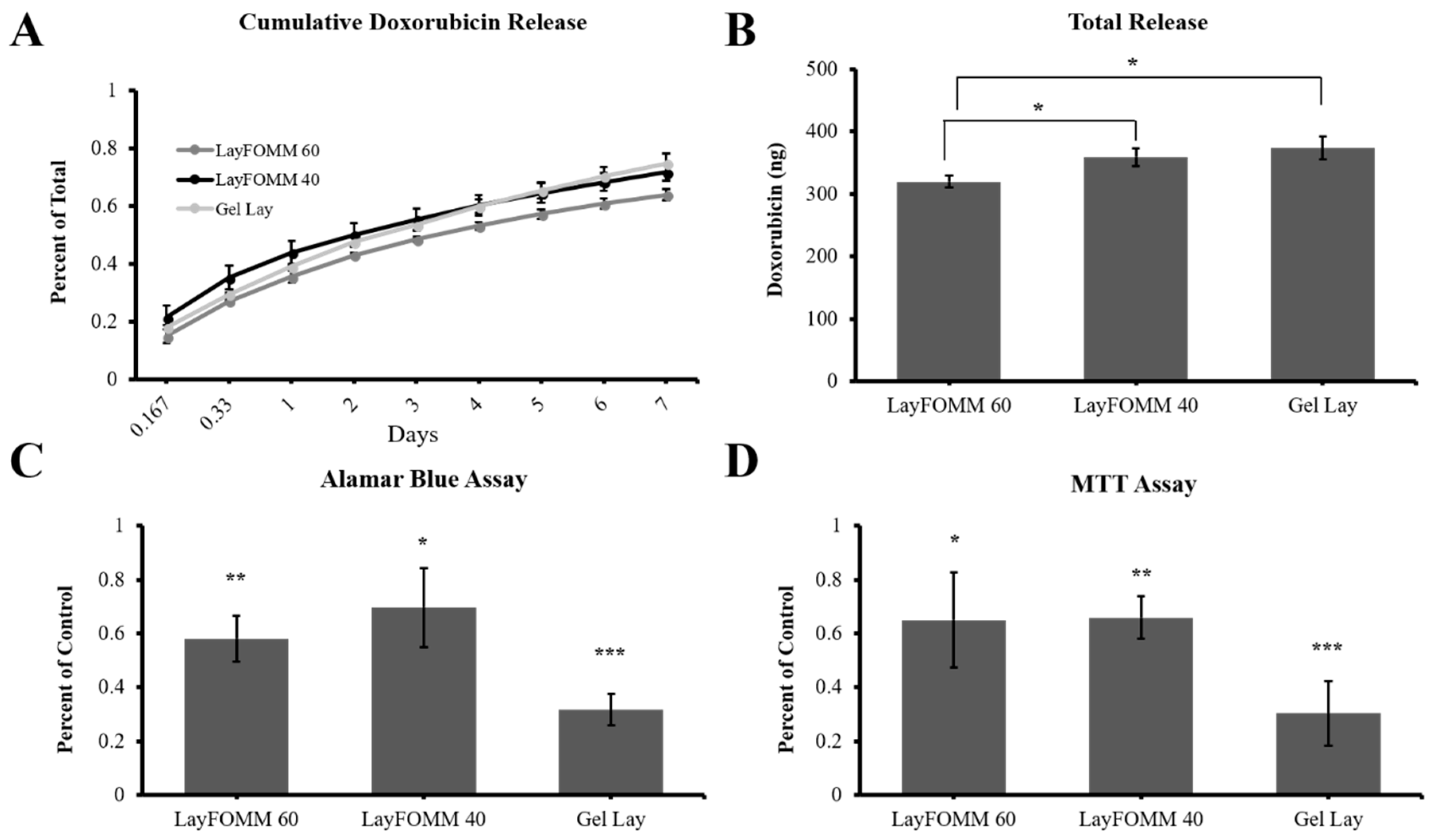
3.3. 3D Printed Scaffold DOX Release
3.4. 3D Scaffold Drug Delivery to LAPC4 Cells
3.5. Direct Treatment and Scaffold Drug Delivery to Patient Derived Cancer Cells
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Aaron, A.D. The management of cancer metastatic to bone. JAMA 1994, 272, 1206–1209. [Google Scholar] [CrossRef] [PubMed]
- Altaf, F.; Weber, M.; Dea, N.; Boriani, S.; Ames, C.; Williams, R.; Verlaan, J.J.; Laufer, I.; Fisher, C.G. Evidence-Based review and survey of expert opinion of reconstruction of metastatic spine tumors. Spine (Phila Pa 1976) 2016, 41, S254–S261. [Google Scholar] [CrossRef] [PubMed]
- Sciubba, D.M.; Goodwin, C.R.; Yurter, A.; Ju, D.; Gokaslan, Z.L.; Fisher, C.; Rhines, L.D.; Fehlings, M.G.; Fourney, D.R.; Mendel, E.; et al. A systematic review of clinical outcomes and prognostic factors for patients undergoing surgery for spinal metastases secondary to breast cancer. Glob. Spine J. 2016, 6, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.J.; Molina, C.A.; Fourney, D.R.; Fisher, C.G.; Gokaslan, Z.L.; Schmidt, M.H.; Rhines, L.D.; Fehlings, M.G.; Laufer, I.; Patel, S.R.; et al. Systematic review of the outcomes of surgical treatment of prostate metastases to the spine. Glob. Spine J. 2017, 7, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Batista, N.; Tee, J.; Sciubba, D.; Sahgal, A.; Laufer, I.; Weber, M.; Gokaslan, Z.; Rhines, L.; Fehlings, M.; Patel, S.; et al. Emerging and established clinical, histopathological and molecular parametric prognostic factors for metastatic spine disease secondary to lung cancer: Helping surgeons make decisions. J. Clin. Neurosci. 2016, 34, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Aebi, M. Spinal metastasis in the elderly. European spine journal: Official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. Eur. Spine J. 2003, 12, S202–S213. [Google Scholar] [CrossRef] [PubMed]
- Falicov, A.; Fisher, C.G.; Sparkes, J.; Boyd, M.C.; Wing, P.C.; Dvorak, M.F. Impact of surgical intervention on quality of life in patients with spinal metastases. Spine 2006, 31, 2849–2856. [Google Scholar] [CrossRef] [PubMed]
- Wai, E.K.; Finkelstein, J.A.; Tangente, R.P.; Holden, L.; Chow, E.; Ford, M.; Yee, A. Quality of life in surgical treatment of metastatic spine disease. Spine 2003, 28, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Rose, P.S.; Clarke, M.J.; Dekutoski, M.B. Minimally invasive treatment of spinal metastases: Techniques. Int. J. Surg. Oncol. 2011, 2011, 494381. [Google Scholar] [CrossRef] [PubMed]
- Boatright, K.; Boden, S. Biology of spine fusion. In Bone Regeneration and Repair: Biology and Clinical Applications; Humana Press: Totowa, NJ, USA, 2005. [Google Scholar]
- Makatsoris, T.; Kalofonos, H.P. The role of chemotherapy in the treatment of bone metastases. Cancer Metast. Biol. 2009, 12, 287–297. [Google Scholar]
- Volkova, M.; Russell, R. Anthracycline cardiotoxicity: Prevalence, pathogenesis and treatment. Curr. Cardiol. Rev. 2011, 7, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Hanigan, M.H.; Devarajan, P. Cisplatin nephrotoxicity: Molecular mechanisms. Cancer Ther. 2003, 1, 47–61. [Google Scholar] [PubMed]
- Velasco, R.; Bruna, J. Taxane-induced peripheral neurotoxicity. Toxics 2015, 3, 152–169. [Google Scholar] [CrossRef] [PubMed]
- Nooh, A.; Zhang, Y.L.; Sato, D.; Rosenzweig, D.H.; Tabaries, S.; Siegel, P.; Barralet, J.E.; Weber, M.H. Intra-tumor delivery of zoledronate mitigates metastasis-induced osteolysis superior to systemic administration. J. Bone Oncol. 2017, 6, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Wolinsky, J.B.; Colson, Y.L.; Grinstaff, M.W. Local drug delivery strategies for cancer treatment: Gels, nanoparticles, polymeric films, rods, and wafers. J. Control. Release 2012, 159, 14–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.W.; Andersen, M.O.; Dillschneider, P.; Chang, C.C.; Gao, S.; Le, D.Q.S.; Yang, C.X.; Hein, S.; Bunger, C.; Kjems, J. Co-delivery of sirna and doxorubicin to cancer cells from additively manufactured implants. RSC Adv. 2015, 5, 101718–101725. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.H.; Kathuria, H.; Tan, J.J.Y.; Kang, L. 3D printed drug delivery and testing systems—A passing fad or the future? Adv. Drug Deliv. Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, D.H.; Carelli, E.; Steffen, T.; Jarzem, P.; Haglund, L. 3D-printed abs and pla scaffolds for cartilage and nucleus pulposus tissue regeneration. Int. J. Mol. Sci. 2015, 16, 15118–15135. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, F.; Torres, J.; Gbureck, U.; Lopez-Cabarcos, E.; Bassett, D.C.; Alkhraisat, M.H.; Barralet, J.E. Craniofacial vertical bone augmentation: A comparison between 3D printed monolithic monetite blocks and autologous onlay grafts in the rabbit. Biomaterials 2009, 30, 6318–6326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichert, J.C.; Cipitria, A.; Epari, D.R.; Saifzadeh, S.; Krishnakanth, P.; Berner, A.; Woodruff, M.A.; Schell, H.; Mehta, M.; Schuetz, M.A.; et al. A tissue engineering solution for segmental defect regeneration in load-bearing long bones. Sci. Transl. Med. 2012, 4, 141ra193. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, L.; Sun, R.; Jia, Y.; Chen, X.; Liu, Y.; Oyang, H.; Feng, L. A new 3D printed titanium metal trabecular bone reconstruction system for early osteonecrosis of the femoral head. Medicine (Baltimore) 2018, 97, e11088. [Google Scholar] [CrossRef] [PubMed]
- You, J.; Preen, R.J.; Bull, L.; Greenman, J.; Ieropoulos, I. 3D printed components of microbial fuel cells: Towards monolithic microbial fuel cell fabrication using additive layer manufacturing. Sustain. Energy Technol. Assess. 2017, 19, 94–101. [Google Scholar] [CrossRef]
- Belka, M.; Ulenberg, S.; Baczek, T. Fused deposition modeling enables the low-cost fabrication of porous, customized-shape sorbents for small-molecule extraction. Anal. Chem. 2017, 89, 4373–4376. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.J.; Dixon, S.; Hale, L.R.; Darbyshire, A.; Martin, D.; de Mel, A. Biomimetic heterogenous elastic tissue development. NPJ Regen. Med. 2017, 2, 16. [Google Scholar] [CrossRef] [PubMed]
- Gawri, R.; Rosenzweig, D.H.; Krock, E.; Ouellet, J.A.; Stone, L.S.; Quinn, T.M.; Haglund, L. High mechanical strain of primary intervertebral disc cells promotes secretion of inflammatory factors associated with disc degeneration and pain. Arthrit. Res. Ther. 2014, 16, R21. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, D.H.; Djap, M.J.; Ou, S.J.; Quinn, T.M. Mechanical injury of bovine cartilage explants induces depth-dependent, transient changes in map kinase activity associated with apoptosis. Osteoarthr. Cartil. 2012, 20, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Hamid, R.; Rotshteyn, Y.; Rabadi, L.; Parikh, R.; Bullock, P. Comparison of alamar blue and mtt assays for high through-put screening. Toxicol. In Vitro 2004, 18, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Gardner, D.E.; Mitchell, D.F.; McDonald, R.E. Treatment of pulps of monkeys with vancomycin and calcium hydroxide. J. Dent. Res. 1971, 50, 1273–1277. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Thiery, J.P.; Benoit, J.; Voisin, M.C.; Leroux, P.; Hagege, G.; Delepine, G.; Goutallier, D. Methotrexate diffusion from acrylic cement. Local chemotherapy for bone tumours. J. Bone Jt. Surg. Br. 1989, 71, 804–811. [Google Scholar] [CrossRef]
- Anagnostakos, K. Therapeutic use of antibiotic-loaded bone cement in the treatment of hip and knee joint infections. J. Bone Jt. Infect. 2017, 2, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, M.O.; Kavan, P.; Miller, W.H., Jr.; Panasci, L.; Assouline, S.; Johnson, N.; Cohen, V.; Patenaude, F.; Pollak, M.; Jagoe, R.T.; et al. Systemic cancer therapy: Achievements and challenges that lie ahead. Front. Pharmacol. 2013, 4, 57. [Google Scholar] [CrossRef] [PubMed]
- Anselmo, A.C.; Mitragotri, S. Nanoparticles in the clinic. Bioeng. Transl. Med. 2016, 1, 10–29. [Google Scholar] [CrossRef] [PubMed]
- Rudnick-Glick, S.; Corem-Salkmon, E.; Grinberg, I.; Margel, S. Targeted drug delivery of near ir fluorescent doxorubicin-conjugated poly(ethylene glycol) bisphosphonate nanoparticles for diagnosis and therapy of primary and metastatic bone cancer in a mouse model. J. Nanobiotechnol. 2016, 14, 80. [Google Scholar] [CrossRef] [PubMed]
- Gross, B.C.; Erkal, J.L.; Lockwood, S.Y.; Chen, C.P.; Spence, D.M. Evaluation of 3d printing and its potential impact on biotechnology and the chemical sciences. Anal. Chem. 2014, 86, 3240–3253. [Google Scholar] [CrossRef] [PubMed]
- Serra, T.; Mateos-Timoneda, M.A.; Planell, J.A.; Navarro, M. 3D printed pla-based scaffolds: A versatile tool in regenerative medicine. Organogenesis 2013, 9, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Serra, T.; Planell, J.A.; Navarro, M. High-resolution pla-based composite scaffolds via 3-D printing technology. Acta Biomater. 2013, 9, 5521–5530. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.T.; Lin, C.C.; Chen, Y.W.; Yeh, C.H.; Fang, H.Y.; Shie, M.Y. Poly(dopamine) coating of 3D printed poly(lactic acid) scaffolds for bone tissue engineering. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 56, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Barbeck, M.; Serra, T.; Booms, P.; Stojanovic, S.; Najman, S.; Engel, E.; Sader, R.; Kirkpatrick, C.J.; Navarro, M.; Ghanaati, S. Analysis of the in vitro degradation and the in vivo tissue response to bi-layered 3D-printed scaffolds combining pla and biphasic pla/bioglass components—Guidance of the inflammatory response as basis for osteochondral regeneration. Bioact. Mater. 2017, 2, 208–223. [Google Scholar] [CrossRef] [PubMed]
- Hutmacher, D.W.; Schantz, T.; Zein, I.; Ng, K.W.; Teoh, S.H.; Tan, K.C. Mechanical properties and cell cultural response of polycaprolactone scaffolds designed and fabricated via fused deposition modeling. J. Biomed. Mater. Res. 2001, 55, 203–216. [Google Scholar] [CrossRef]
- Cipitria, A.; Reichert, J.C.; Epari, D.R.; Saifzadeh, S.; Berner, A.; Schell, H.; Mehta, M.; Schuetz, M.A.; Duda, G.N.; Hutmacher, D.W. Polycaprolactone scaffold and reduced rhbmp-7 dose for the regeneration of critical-sized defects in sheep tibiae. Biomaterials 2013, 34, 9960–9968. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.C.; Lee, J.J.; Shim, J.H.; Park, K.H.; Lee, J.S.; Bae, E.B.; Choi, J.W.; Huh, J.B. Development and assessment of a 3D-printed scaffold with rhbmp-2 for an implant surgical guide stent and bone graft material: A pilot animal study. Materials 2017, 10, 1434. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, E.D.; Besunder, R.; Pappas, D.; Allen, F.; Guceri, S.; Sun, W. Accelerated differentiation of osteoblast cells on polycaprolactone scaffolds driven by a combined effect of protein coating and plasma modification. Biofabrication 2010, 2, 014109. [Google Scholar] [CrossRef] [PubMed]
- Rai, B.; Ho, K.H.; Lei, Y.; Si-Hoe, K.M.; Jeremy Teo, C.M.; Yacob, K.B.; Chen, F.; Ng, F.C.; Teoh, S.H. Polycaprolactone-20% tricalcium phosphate scaffolds in combination with platelet-rich plasma for the treatment of critical-sized defects of the mandible: A pilot study. J Oral Maxillofac. Surg. 2007, 65, 2195–2205. [Google Scholar] [CrossRef] [PubMed]
- Devulapally, R.; Paulmurugan, R. Polymer nanoparticles for drug and small silencing rna delivery to treat cancers of different phenotypes. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2014, 6, 40–60. [Google Scholar] [CrossRef] [PubMed]
- Tani, T.; Okada, K.; Takahashi, S.; Suzuki, N.; Shimada, Y.; Itoi, E. Doxorubicin-loaded calcium phosphate cement in the management of bone and soft tissue tumors. In Vivo 2006, 20, 55–60. [Google Scholar] [PubMed]
- Chen, M.; Le, D.Q.; Hein, S.; Li, P.; Nygaard, J.V.; Kassem, M.; Kjems, J.; Besenbacher, F.; Bunger, C. Fabrication and characterization of a rapid prototyped tissue engineering scaffold with embedded multicomponent matrix for controlled drug release. Int. J. Nanomed. 2012, 7, 4285–4297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, M.; Wang, M.; Chen, M.; Dagnaes-Hansen, F.; Le, D.Q.; Baatrup, A.; Horsman, M.R.; Kjems, J.; Bunger, C.E. A tissue-engineered therapeutic device inhibits tumor growth in vitro and in vivo. Acta Biomater. 2015, 18, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Jalani, G.; Naccache, R.; Rosenzweig, D.H.; Haglund, L.; Vetrone, F.; Cerruti, M. Photocleavable hydrogel-coated upconverting nanoparticles: A multifunctional theranostic platform for nir imaging and on-demand macromolecular delivery. J. Am. Chem. Soc. 2016, 138, 1078–1083. [Google Scholar] [CrossRef] [PubMed]
- Jalani, G.; Naccache, R.; Rosenzweig, D.H.; Lerouge, S.; Haglund, L.; Vetrone, F.; Cerruti, M. Real-time, non-invasive monitoring of hydrogel degradation using LiYF4:Yb(3+)/tm(3+) nir-to-nir upconverting nanoparticles. Nanoscale 2015, 7, 11255–11262. [Google Scholar] [CrossRef] [PubMed]
- DeMerlis, C.C.; Schoneker, D.R. Review of the oral toxicity of polyvinyl alcohol (PVA). Food Chem. Toxicol. 2003, 41, 319–326. [Google Scholar] [CrossRef]
- Hung, K.C.; Tseng, C.S.; Hsu, S.H. Synthesis and 3d printing of biodegradable polyurethane elastomer by a water-based process for cartilage tissue engineering applications. Adv. Healthc. Mater. 2014, 3, 1578–1587. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.J.; Ren, J.A.; Wang, G.F.; Li, Z.A.; Wu, X.W.; Ren, H.J.; Liu, S. 3D-printed “fistula stent” designed for management of enterocutaneous fistula: An advanced strategy. World J. Gastroenterol. 2017, 23, 7489–7494. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Mangadlao, J.D.; Wallat, J.; De Leon, A.; Pokorski, J.K.; Advincula, R.C. 3D printing biocompatible polyurethane/poly(lactic acid)/graphene oxide nanocomposites: Anisotropic properties. ACS Appl. Mater. Interfaces 2017, 9, 4015–4023. [Google Scholar] [CrossRef] [PubMed]
- Castel, N.; Soon-Sutton, T.; Deptula, P.; Flaherty, A.; Parsa, F.D. Polyurethane-coated breast implants revisited: A 30-year follow-up. Arch. Plast. Surg. 2015, 42, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Feula, A.; Tang, X.; Giannakopoulos, I.; Chippindale, A.M.; Hamley, I.W.; Greco, F.; Paul Buckley, C.; Siviour, C.R.; Hayes, W. An adhesive elastomeric supramolecular polyurethane healable at body temperature. Chem. Sci. 2016, 7, 4291–4300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janik, H.; Marzec, M. A review: Fabrication of porous polyurethane scaffolds. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 48, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Tomankova, K.; Polakova, K.; Pizova, K.; Binder, S.; Havrdova, M.; Kolarova, M.; Kriegova, E.; Zapletalova, J.; Malina, L.; Horakova, J.; et al. In vitro cytotoxicity analysis of doxorubicin-loaded/superparamagnetic iron oxide colloidal nanoassemblies on mcf7 and nih3t3 cell lines. Int. J. Nanomed. 2015, 10, 949–961. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Type | Alamar Blue | MTT | ||||
|---|---|---|---|---|---|---|
| Ratio to Control * | SD | p Value | Ratio to Control * | SD | p Value | |
| LAPC4 | 0.57 | 0.12 | 0.0025 | 0.96 | 0.14 | 0.29 |
| Patient Cells | 0.35 | 0.098 | 0.0002 | 0.91 | 0.13 | 0.14 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahangar, P.; Akoury, E.; Ramirez Garcia Luna, A.S.; Nour, A.; Weber, M.H.; Rosenzweig, D.H. Nanoporous 3D-Printed Scaffolds for Local Doxorubicin Delivery in Bone Metastases Secondary to Prostate Cancer. Materials 2018, 11, 1485. https://doi.org/10.3390/ma11091485
Ahangar P, Akoury E, Ramirez Garcia Luna AS, Nour A, Weber MH, Rosenzweig DH. Nanoporous 3D-Printed Scaffolds for Local Doxorubicin Delivery in Bone Metastases Secondary to Prostate Cancer. Materials. 2018; 11(9):1485. https://doi.org/10.3390/ma11091485
Chicago/Turabian StyleAhangar, Pouyan, Elie Akoury, Ana Sofia Ramirez Garcia Luna, Antone Nour, Michael H. Weber, and Derek H. Rosenzweig. 2018. "Nanoporous 3D-Printed Scaffolds for Local Doxorubicin Delivery in Bone Metastases Secondary to Prostate Cancer" Materials 11, no. 9: 1485. https://doi.org/10.3390/ma11091485