

SENOSI Confocal Microscopy: A New and Innovating Way to Detect Positive Margins in Non-Palpable Breast Cancer?
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Study Design
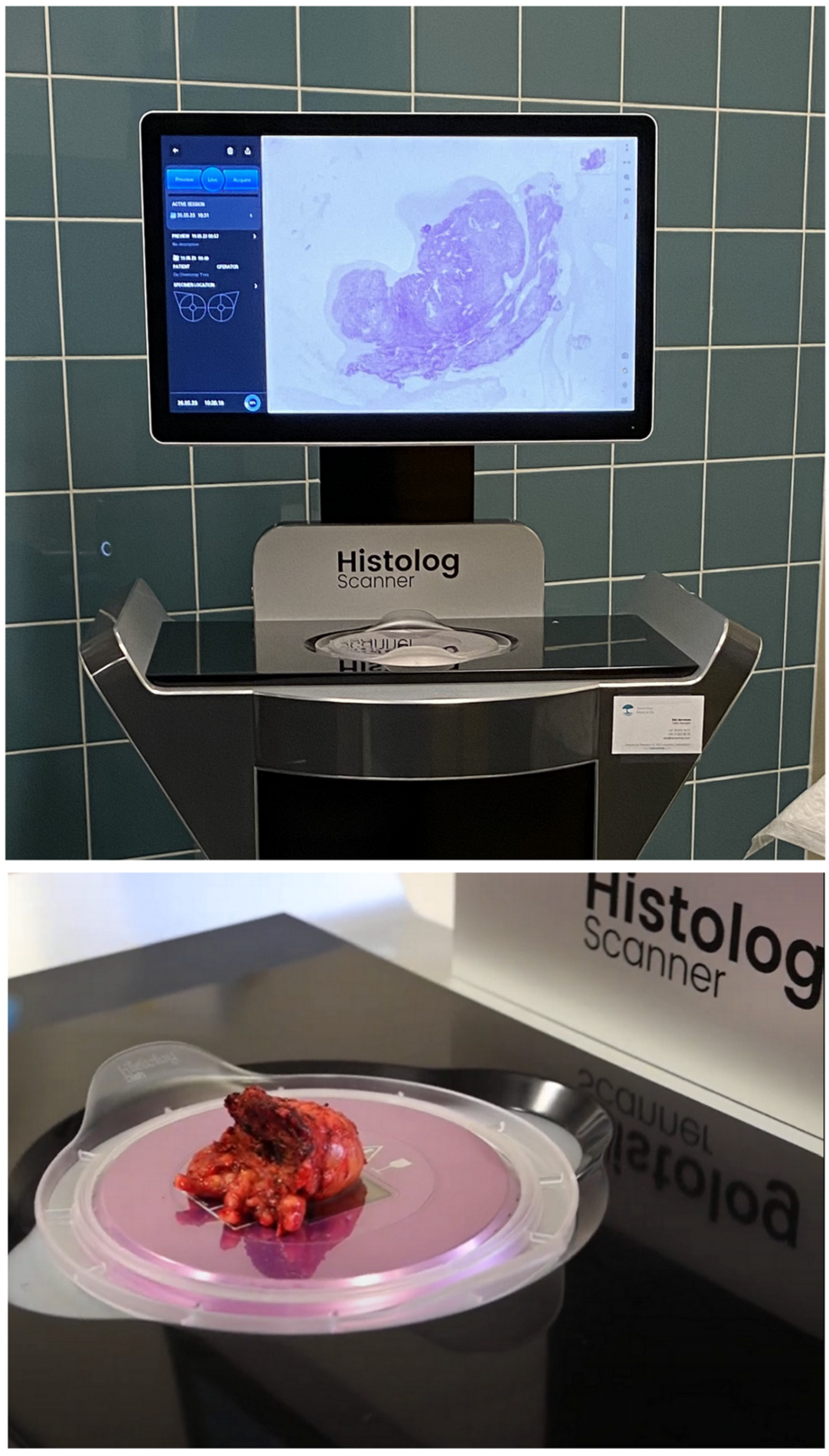
2.2. Materials
2.3. Objectives
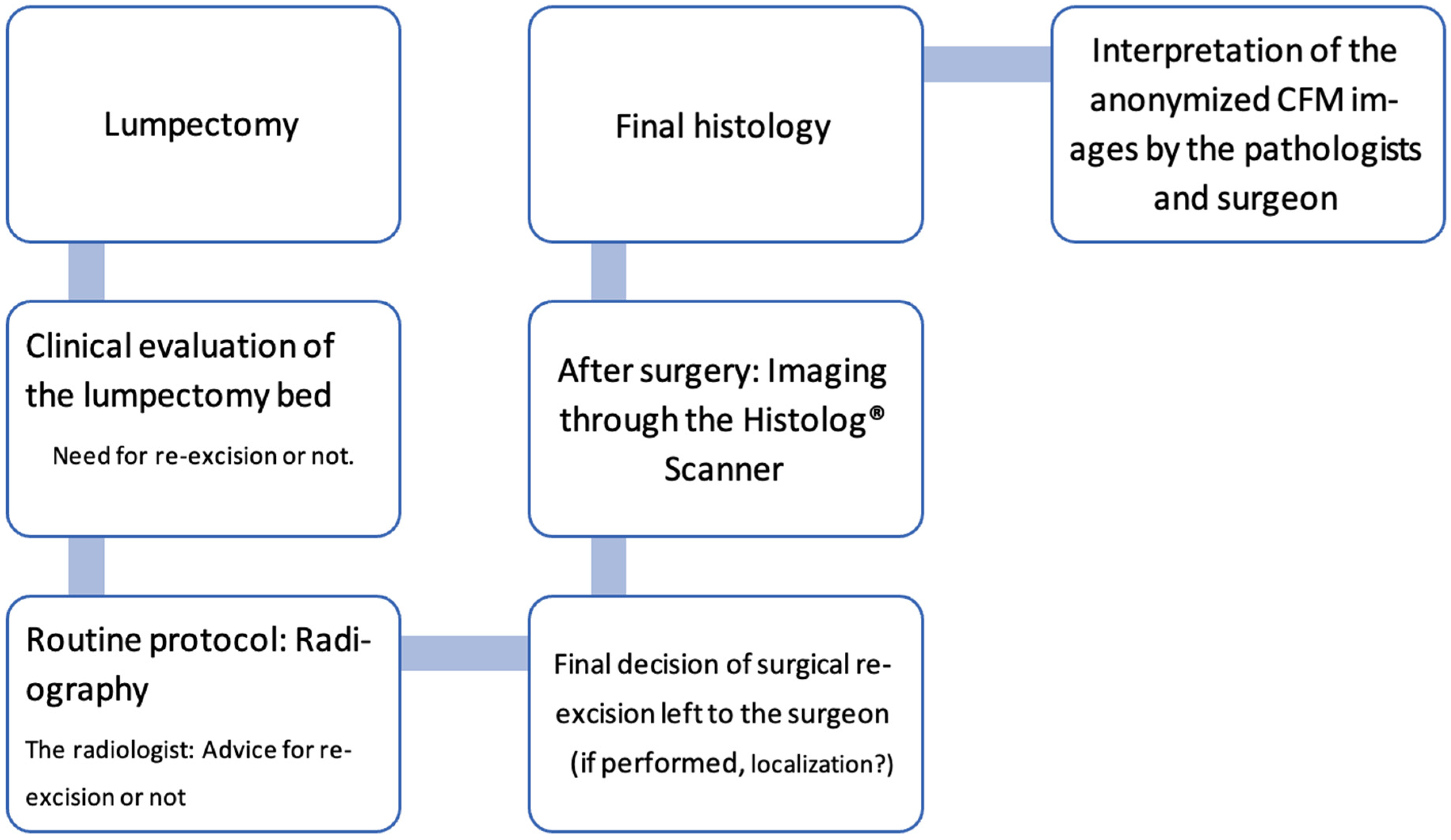
2.4. Methods
2.4.1. Training in Histolog Images
2.4.2. Standard of Care (SoC)
2.4.3. Histolog Imaging
2.4.4. Data Collection
2.5. Statistics
3. Results
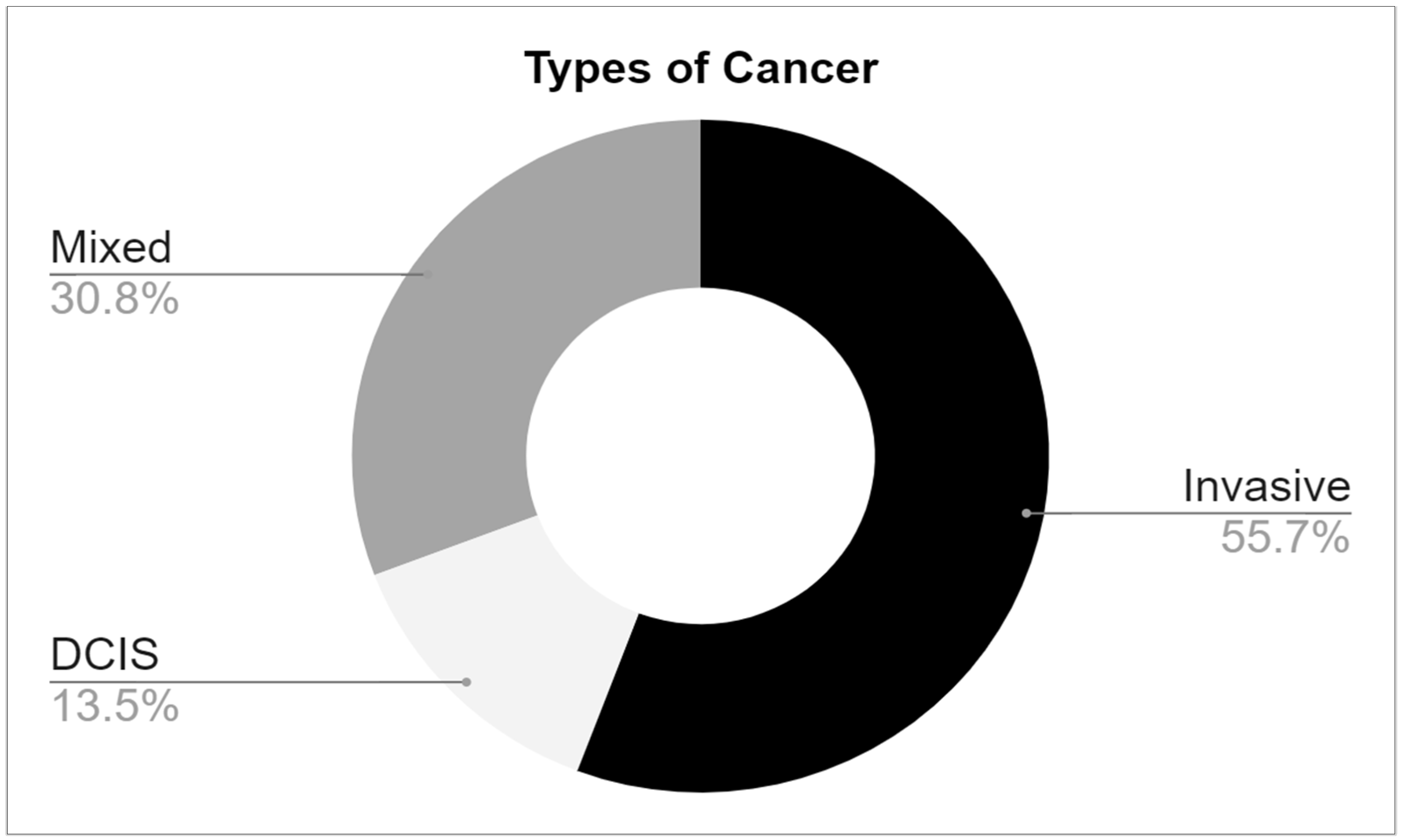
3.1. Cancer Patient Characteristics
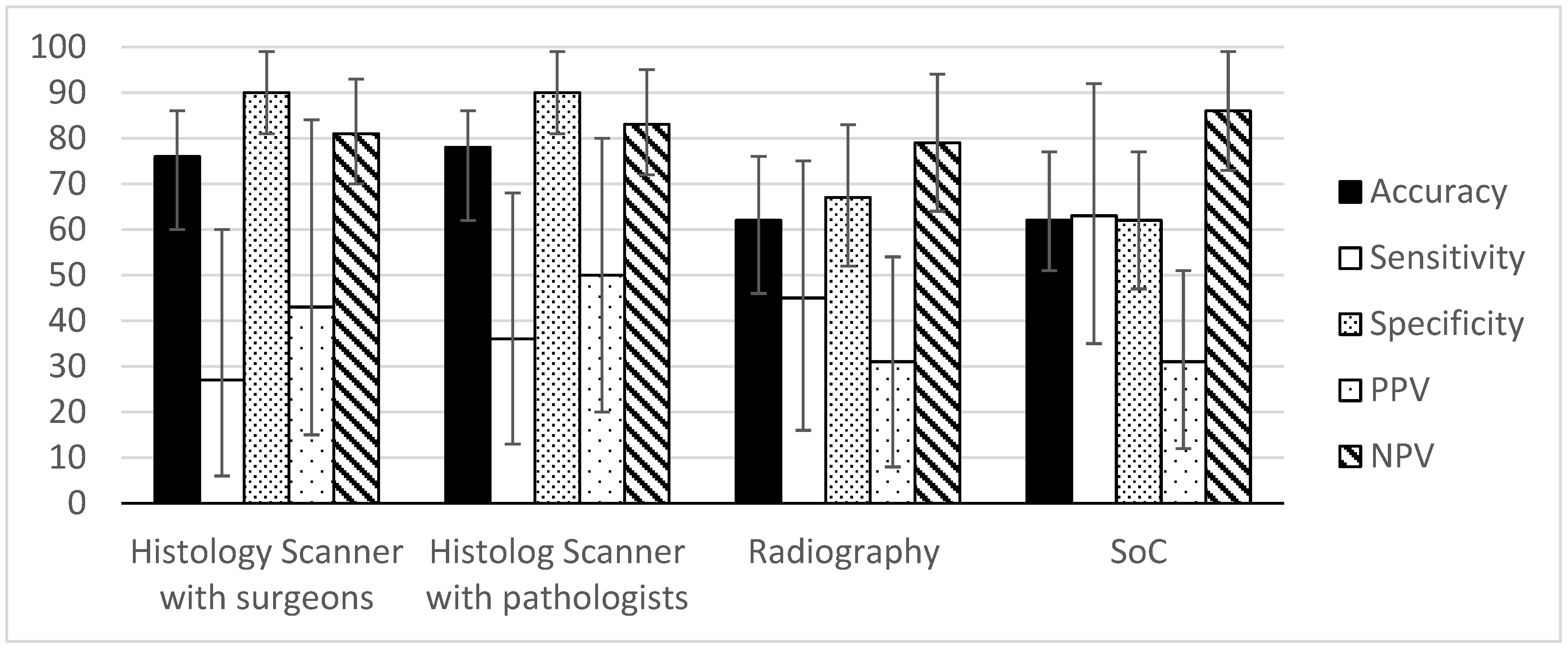
Performance Analysis
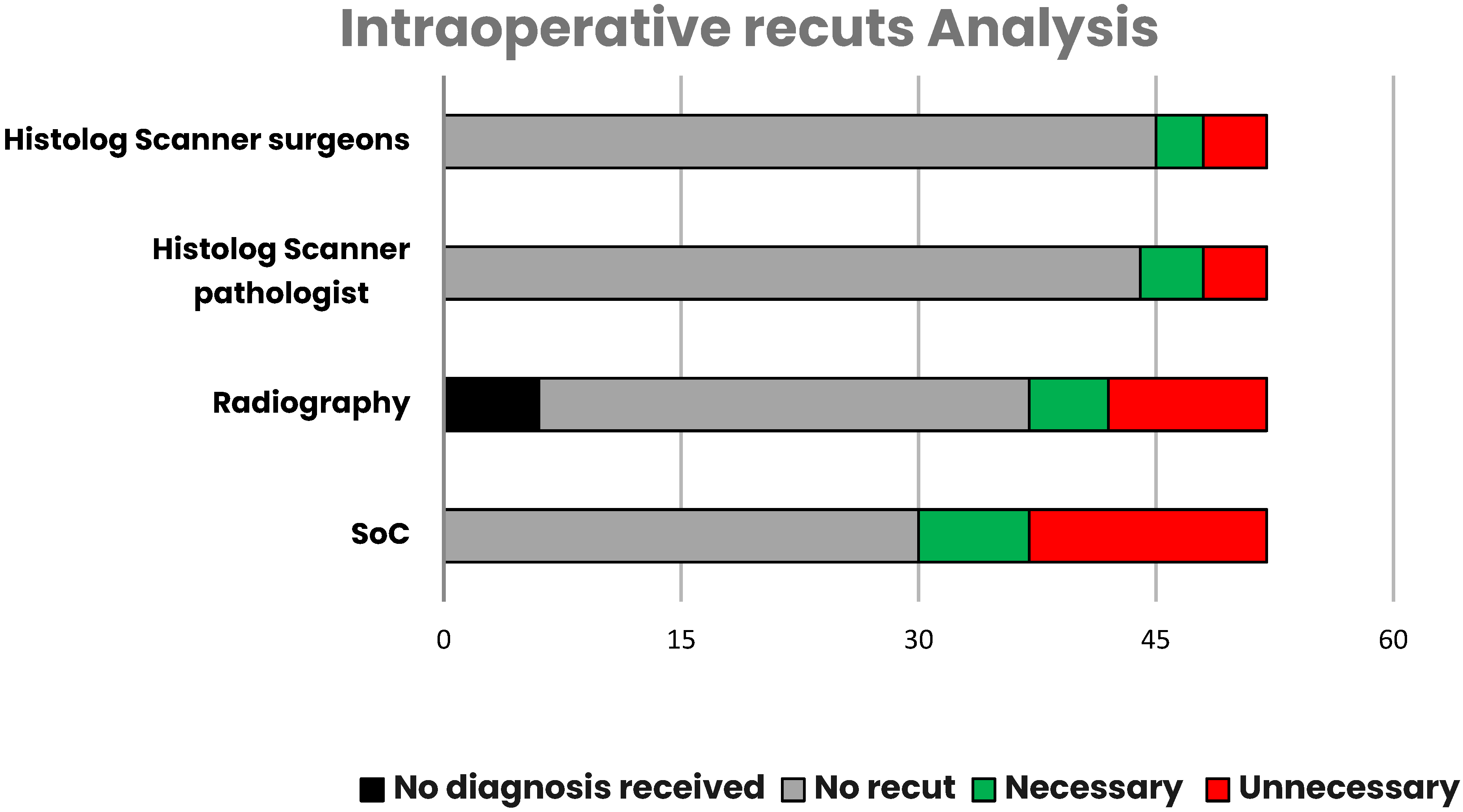
3.2. Intraoperative Recuts
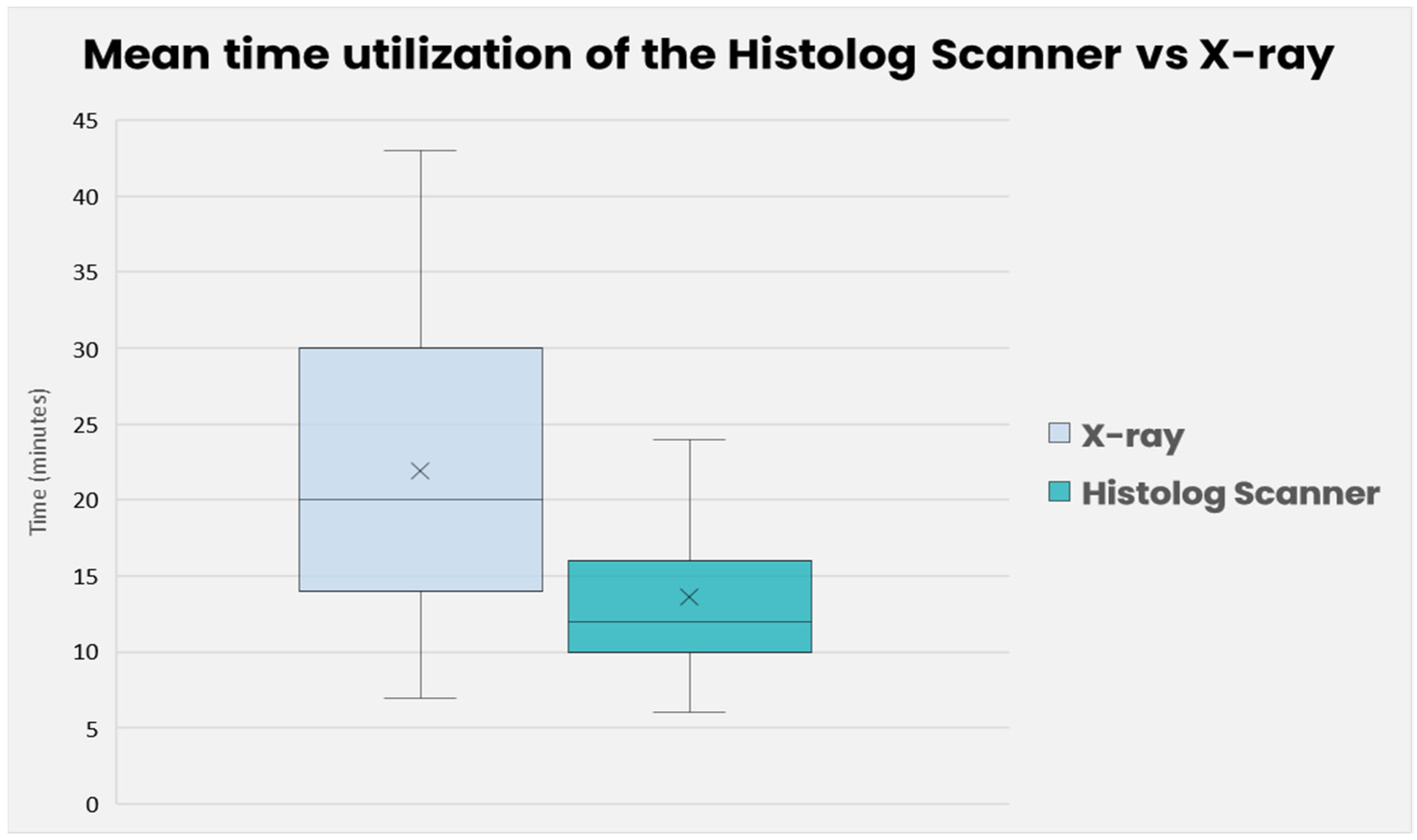
3.3. Timing Analysis
4. Discussion
4.1. Performance Review
4.2. Time and User Analysis
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization: Regional Office for Europe. World Cancer Report: Cancer Research for Cancer Development; IARC: Lyon, France, 2020; ISBN 978-92-832-0447-3. [Google Scholar]
- Ligue Suisse Contre le Cancer Le Cancer en Suisse: Les Chiffres Période Déterminante: 2015–2019 (Moyenne Annuelle) 2022. Available online: https://www.bfs.admin.ch/bfs/fr/home/actualites/quoi-de-neuf.assetdetail.23566716.html (accessed on 27 November 2023).
- Agarwal, S.; Pappas, L.; Neumayer, L.; Kokeny, K.; Agarwal, J. Effect of Breast Conservation Therapy vs. Mastectomy on Disease-Specific Survival for Early-Stage Breast Cancer. JAMA Surg. 2014, 149, 267. [Google Scholar] [CrossRef]
- Yoon, G.Y.; Cha, J.H.; Kim, H.H.; Shin, H.J.; Chae, E.Y.; Choi, W.J. Recurrent and Second Breast Cancer Detected on Follow-Up Mammography and Breast Ultrasound after Breast-Conserving Surgery: Imaging Findings and Clinicopathologic Factors. J. Korean Soc. Radiol. 2016, 74, 15. [Google Scholar] [CrossRef]
- Atkins, J.; Mushawah, F.A.; Appleton, C.M.; Cyr, A.E.; Gillanders, W.E.; Aft, R.L.; Eberlein, T.J.; Gao, F.; Margenthaler, J.A. Positive margin rates following breast-conserving surgery for stage I–III breast cancer: Palpable versus nonpalpable tumors. J. Surg. Res. 2012, 177, 109–115. [Google Scholar] [CrossRef]
- Pilewskie, M.; Morrow, M. Margins in breast cancer: How much is enough? Cancer 2018, 124, 1335–1341. [Google Scholar] [CrossRef]
- Tran-Harding, K.; Shi, Q.; Gibbs, R.; Szabunio, M.; Wang, X. Evaluation of Margin Status of a Breast Lumpectomy Specimen: What the Radiologist Should Know. Curr. Probl. Diagn. Radiol. 2019, 48, 599–604. [Google Scholar] [CrossRef]
- Moran, M.S.; Schnitt, S.J.; Giuliano, A.E.; Harris, J.R.; Khan, S.A.; Horton, J.; Klimberg, S.; Chavez-MacGregor, M.; Freedman, G.; Houssami, N.; et al. Society of Surgical Oncology–American Society for Radiation Oncology Consensus Guideline on Margins for Breast-Conserving Surgery With Whole-Breast Irradiation in Stages I and II Invasive Breast Cancer. Ann. Surg. Oncol. 2014, 21, 704–716. [Google Scholar] [CrossRef]
- Kreike, B.; Hart, A.A.M.; van de Velde, T.; Borger, J.; Peterse, H.; Rutgers, E.; Bartelink, H.; van de Vijver, M.J. Continuing Risk of Ipsilateral Breast Relapse After Breast-Conserving Therapy at Long-Term Follow-up. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Singh, G.; Hogan, K.T.; Atkins, K.A.; Schroen, A.T. The effect of intraoperative specimen inking on lumpectomy re-excision rates. World J. Surg. Onc. 2010, 8, 4. [Google Scholar] [CrossRef] [PubMed]
- Havel, L.; Naik, H.; Ramirez, L.; Morrow, M.; Landercasper, J. Impact of the SSO-ASTRO Margin Guideline on Rates of Re-excision After Lumpectomy for Breast Cancer: A Meta-analysis. Ann. Surg. Oncol. 2019, 26, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- McCahill, L.E.; Single, R.M.; Aiello Bowles, E.J.; Feigelson, H.S.; James, T.A.; Barney, T.; Engel, J.M.; Onitilo, A.A. Variability in Reexcision Following Breast Conservation Surgery. JAMA 2012, 307, 467. [Google Scholar] [CrossRef]
- Namdar, Z.M.; Omidifar, N.; Arasteh, P.; Akrami, M.; Tahmasebi, S.; Nobandegani, A.S.; Sedighi, S.; Zangouri, V.; Talei, A. How accurate is frozen section pathology compared to permanent pathology in detecting involved margins and lymph nodes in breast cancer? World J. Surg. Onc. 2021, 19, 261. [Google Scholar] [CrossRef]
- Nunez, A.; Jones, V.; Schulz-Costello, K.; Schmolze, D. Accuracy of gross intraoperative margin assessment for breast cancer: Experience since the SSO-ASTRO margin consensus guidelines. Sci. Rep. 2020, 10, 17344. [Google Scholar] [CrossRef]
- He, X.-F.; Ye, F.; Wen, J.-H.; Li, S.-J.; Huang, X.-J.; Xiao, X.-S.; Xie, X.-M. High Residual Tumor Rate for Early Breast Cancer Patients Receiving Vacuum-assisted Breast Biopsy. J. Cancer 2017, 8, 490–496. [Google Scholar] [CrossRef]
- Rua, C.; Lebas, P.; Michenet, P.; Ouldamer, L. Evaluation of lumpectomy surgical specimen radiographs in subclinical, in situ and invasive breast cancer, and factors predicting positive margins. Diagn. Interv. Imaging 2012, 93, 871–877. [Google Scholar] [CrossRef]
- Ragazzi, M.; Piana, S.; Longo, C.; Castagnetti, F.; Foroni, M.; Ferrari, G.; Gardini, G.; Pellacani, G. Fluorescence confocal microscopy for pathologists. Mod. Pathol. 2014, 27, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Ragazzi, M.; Longo, C.; Piana, S. Ex Vivo (Fluorescence) Confocal Microscopy in Surgical Pathology: State of the Art. Adv. Anat. Pathol. 2016, 23, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, J.L.; Ding, H.; Benveniste, A.P.; Kuerer, H.M.; Krishnamurthy, S.; Yang, W.; Richards-Kortum, R. Feasibility of confocal fluorescence microscopy for real-time evaluation of neoplasia in fresh human breast tissue. J. Biomed. Opt. 2013, 18, 106016. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.P.; Leff, D.R.; Shousha, S.; Hadjiminas, D.J.; Ramakrishnan, R.; Hughes, M.R.; Yang, G.-Z.; Darzi, A. Imaging breast cancer morphology using probe-based confocal laser endomicroscopy: Towards a real-time intraoperative imaging tool for cavity scanning. Breast Cancer Res. Treat. 2015, 153, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Sandor, M.-F.; Schwalbach, B.; Hofmann, V.; Istrate, S.-E.; Schuller, Z.; Ionescu, E.; Heimann, S.; Ragazzi, M.; Lux, M.P. Imaging of lumpectomy surface with large field-of-view confocal laser scanning microscope for intraoperative margin assessment—POLARHIS study. Breast 2022, 66, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Elfgen, C.; Papassotiropoulos, B.; Varga, Z.; Moskovszky, L.; Nap, M.; Güth, U.; Baege, A.; Amann, E.; Chiesa, F.; Tausch, C. Comparative analysis of confocal microscopy on fresh breast core needle biopsies and conventional histology. Diagn. Pathol. 2019, 14, 58. [Google Scholar] [CrossRef] [PubMed]
- Peters, N.; Schubert, M.; Metzler, G.; Geppert, J.-P.; Moehrle, M. Diagnostic accuracy of a new ex vivo confocal laser scanning microscope compared to H&E-stained paraffin slides for micrographic surgery of basal cell carcinoma. Acad. Dermatol. Venereol. 2019, 33, 298–304. [Google Scholar] [CrossRef]
- Grizzetti, L.; Kuonen, F. Ex vivo confocal microscopy for surgical margin assessment: A histology-compared study on 109 specimens. Ski. Health Dis. 2022, 2, e91. [Google Scholar] [CrossRef] [PubMed]
- Togawa, R.; Hederer, J.; Ragazzi, M.; Bruckner, T.; Fastner, S.; Gomez, C.; Hennigs, A.; Nees, J.; Pfob, A.; Riedel, F.; et al. Imaging of lumpectomy surface with large field-of-view confocal laser scanning microscopy ‘Histolog® scanner’ for breast margin assessment in comparison with conventional specimen radiography. Breast 2023, 68, 194–200. [Google Scholar] [CrossRef]
- Conversano, A.; Abbaci, M.; Van Diest, P.; Roulot, A.; Falco, G.; Ferchiou, M.; Coiro, S.; Richir, M.; Genolet, P.-M.; Clement, C.; et al. Breast carcinoma detection in ex vivo fresh human breast surgical specimens using a fast slide-free confocal microscopy scanner: HIBISCUSS project. BJS Open 2023, 7, zrad046. [Google Scholar] [CrossRef]
- Olsha, O.; Shemesh, D.; Carmon, M.; Sibirsky, O.; Abu Dalo, R.; Rivkin, L.; Ashkenazi, I. Resection Margins in Ultrasound-Guided Breast-Conserving Surgery. Ann. Surg. Oncol. 2011, 18, 447–452. [Google Scholar] [CrossRef]
- Allweis, T.M.; Kaufman, Z.; Lelcuk, S.; Pappo, I.; Karni, T.; Schneebaum, S.; Spector, R.; Schindel, A.; Hershko, D.; Zilberman, M.; et al. A prospective, randomized, controlled, multicenter study of a real-time, intraoperative probe for positive margin detection in breast-conserving surgery. Am. J. Surg. 2008, 196, 483–489. [Google Scholar] [CrossRef]
- Keller, M.D.; Majumder, S.K.; Kelley, M.C.; Meszoely, I.M.; Boulos, F.I.; Olivares, G.M.; Mahadevan-Jansen, A. Autofluorescence and diffuse reflectance spectroscopy and spectral imaging for breast surgical margin analysis. Lasers Surg. Med. 2010, 42, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, M.; Ragazzi, M.; Van Diest, P.; Ferchiou, M.; Casiraghi, O.; Labaied, N.; Conversano, A.; Abbaci, M. Atlas of ex vivo breast tissue and carcinomas images by ultra-fast large feld-of-view fuorescence confocal microscopy of lumpectomy. Virchows Arch. 2023, 483 (Suppl. S1), S63. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medical Procedure | Accuracy | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| Histolog Scanner with surgeons | 76.47% | 27.27% | 90.00% | 42.86% | 81.82% |
| Histolog Scanner with pathologists | 78.43% | 36.36% | 90.00% | 50.00% | 83.72% |
| Radiography | 62.22% | 45.45% | 67.65% | 31.25% | 79.31% |
| SoC | 62.75% | 63.64% | 62.50% | 31.82% | 86.21% |
| No Recut | Recut | Total Recut | ||
|---|---|---|---|---|
| Necessary | Unnecessary | |||
| Histolog Scanner Surgeon | 45 | 3 | 4 | 7 |
| Histolog Scanner Pathologist | 44 | 4 | 4 | 8 |
| Specimen Radiography * | 37 | 5 | 10 | 15 |
| SoC | 30 | 7 | 15 | 22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wernly, D.; Beniere, C.; Besse, V.; Seidler, S.; Lachat, R.; Letovanec, I.; Huber, D.; Simonson, C. SENOSI Confocal Microscopy: A New and Innovating Way to Detect Positive Margins in Non-Palpable Breast Cancer? Life 2024, 14, 204. https://doi.org/10.3390/life14020204
Wernly D, Beniere C, Besse V, Seidler S, Lachat R, Letovanec I, Huber D, Simonson C. SENOSI Confocal Microscopy: A New and Innovating Way to Detect Positive Margins in Non-Palpable Breast Cancer? Life. 2024; 14(2):204. https://doi.org/10.3390/life14020204
Chicago/Turabian StyleWernly, Deborah, Charles Beniere, Valerie Besse, Stephanie Seidler, Regine Lachat, Igor Letovanec, Daniela Huber, and Colin Simonson. 2024. "SENOSI Confocal Microscopy: A New and Innovating Way to Detect Positive Margins in Non-Palpable Breast Cancer?" Life 14, no. 2: 204. https://doi.org/10.3390/life14020204