
The Relationship between Tricuspid Annular Longitudinal and Sphincter-like Features of Its Function in Healthy Adults: Insights from the MAGYAR-Healthy Study

Abstract
:1. Introduction
2. Materials and Methods
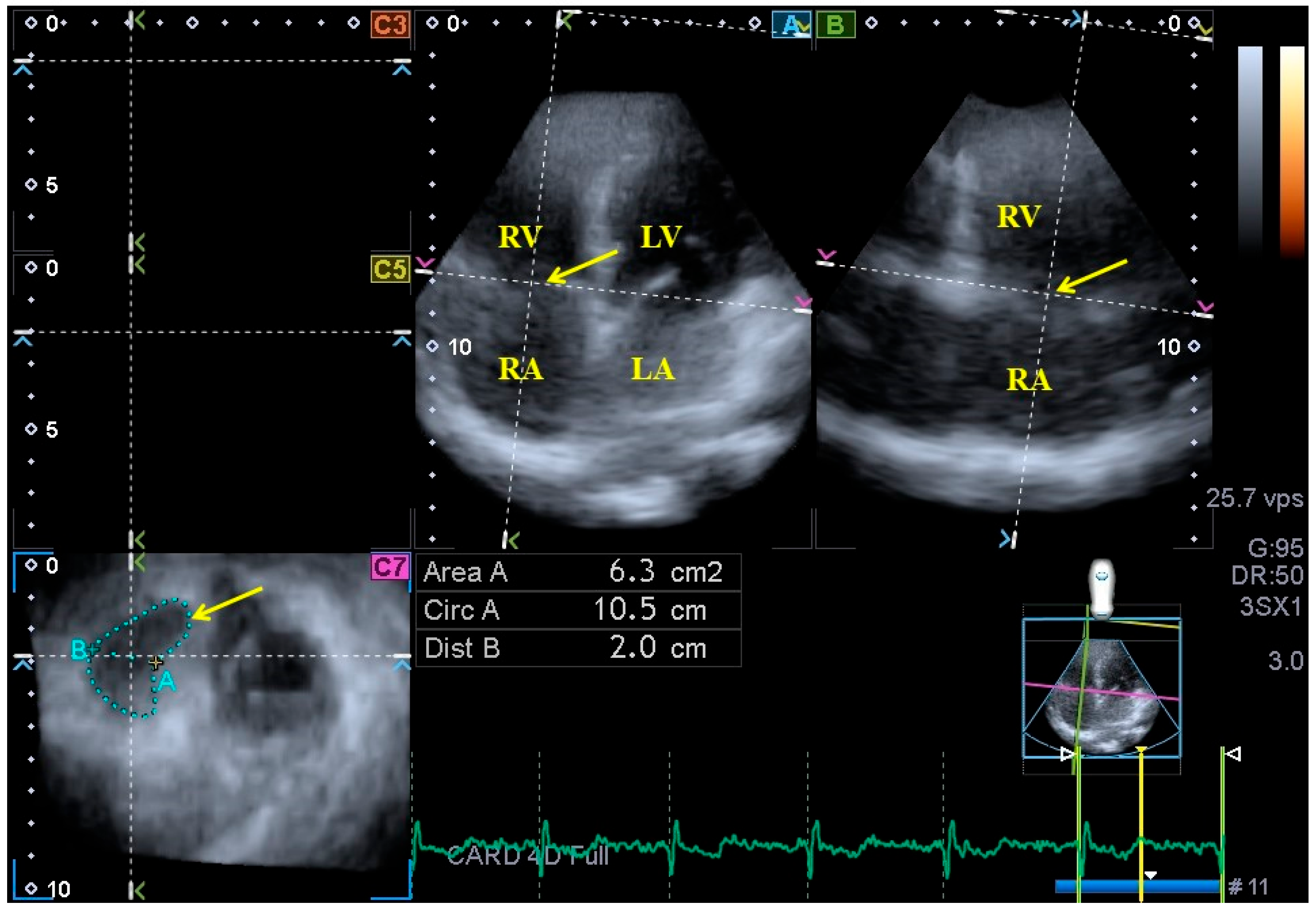
2.1. Parameters Featuring TA Morphology
- −
- TA diameter (TAD), evaluated by drawing a perpendicular line from the peak of TA curvature to the middle of the straight TA border;
- −
- TA area (TAA), evaluated via planimetry;
- −
- TA perimeter (TAP), evaluated via planimetry.
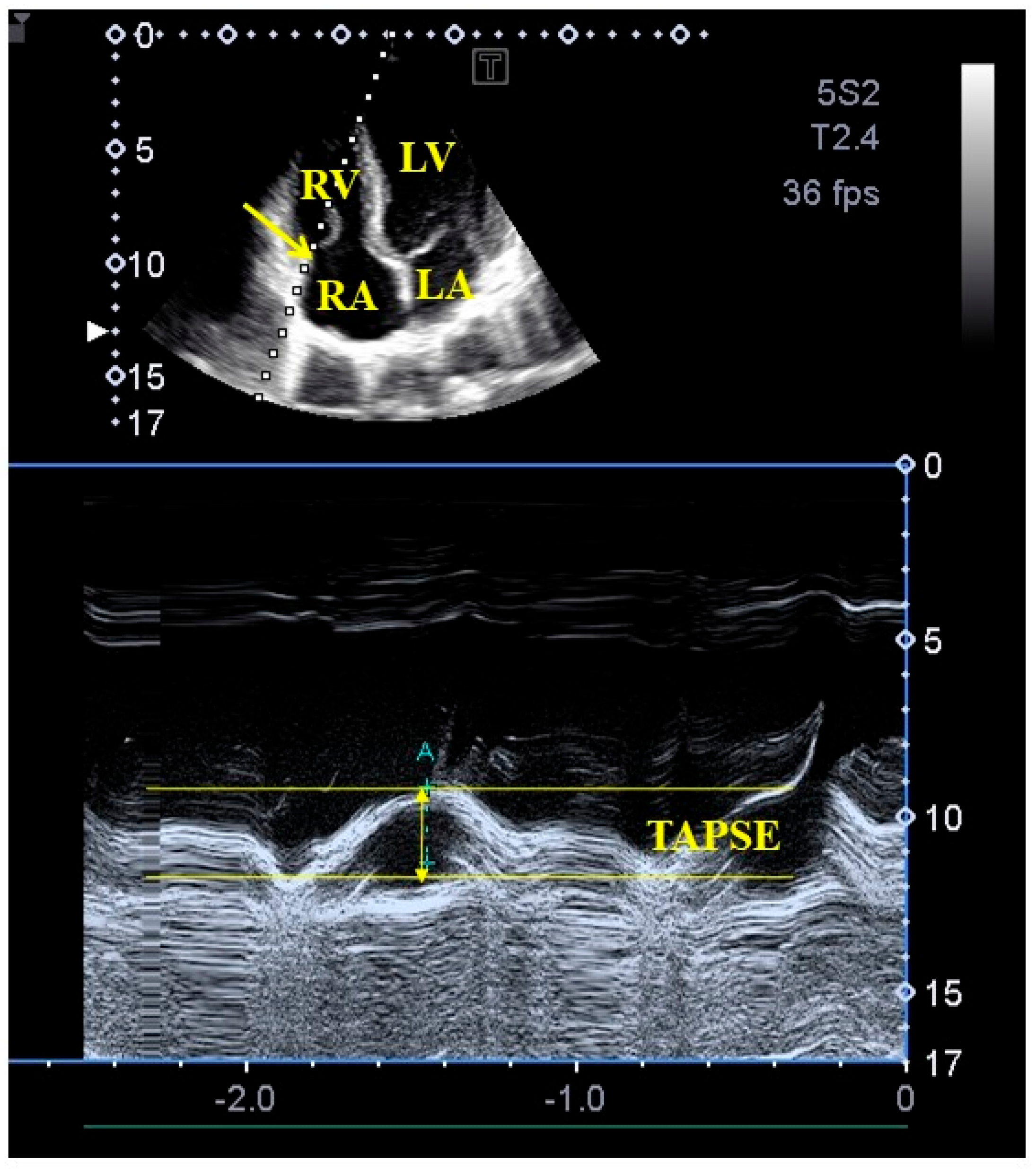
2.2. Parameters Featuring TA Function
- −
- TA fractional shortening (TAFS), defined as ([end-diastolic TAD − end-systolic TAD]/end-diastolic TAD) × 100;
- −
- TA fractional area change (TAFAC), defined as ([end-diastolic TAA − end-systolic TAA]/end-diastolic TAA) × 100.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Limitations
- The image quality of echocardiographic analysis is an important issue, still being worse in the case of 3DE than in the case of 2D echocardiography, which should be taken into account when interpreting the findings. 3DE has several technical difficulties, including lower frame rate and larger transducer size, which can significantly affect image quality. Nevertheless, considering both the advantages and disadvantages, the clinical role of 3DE is unquestionable [5,6,7].
- This study did not compare 2D echocardiography versus 3DE in the measurement of TA.
- Three-dimensional echocardiography-derived chamber quantifications of atria and ventricles were also not performed in this study.
- Validation of our 3DE results using other imaging methods could have further strengthened the significance of our scientific findings. Similar studies may be the subject of clinical trials in the future.
- STE-derived featuring of the TA function was not purposed either.
- Healthy subjects were involved in this study. However, neither special laboratory tests nor imaging testing were performed to completely exclude disorders in the early stages.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Putthapiban, P.; Amini, M.R.; Abudayyeh, I. Anatomy of the Tricuspid Valve and Pathophysiology of Tricuspid Regurgitation. Interv. Cardiol. Clin. 2022, 11, 1–9. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Morris, D.A.; Rottbauer, W. Functional tricuspid regurgitation, related right heart remodeling, and available treatment options: Good news for patients with heart failure? Heart Fail. Rev. 2022, 27, 1301–1312. [Google Scholar] [CrossRef]
- Badano, L.P.; Muraru, D.; Enriquez-Sarano, M. Assessment of functional tricuspid regurgitation. Eur. Heart J. 2013, 34, 1875–1885. [Google Scholar] [CrossRef]
- Franke, A.; Kuhl, H.P. Second-generation real-time 3D echocardiography: A revolutionary new technology. MedicaMundi 2003, 47, 34. [Google Scholar]
- Nemes, A.; Kalapos, A.; Domsik, P.; Forster, T. Three-dimensional speckle-tracking echocardiography—A further step in non-invasive three-dimensional cardiac imaging. Orv. Hetil. 2012, 153, 1570–1577. [Google Scholar] [CrossRef]
- Ammar, K.A.; Paterick, T.E.; Khanderia, B.K.; Jan, M.F.; Kramer, C.; Umland, M.M.; Tercius, A.J.; Baratta, L.; Tajik, A.J. Myocardial mechanics: Understanding and applying three-dimensional speckle tracking echocardiography in clinical practice. Echocardiography 2012, 29, 861–872. [Google Scholar] [CrossRef]
- Urbano-Moral, J.A.; Patel, A.R.; Maron, M.S.; Arias-Godinez, J.A.; Pandian, N.G. Three-dimensional speckle-tracking echocardiography: Methodological aspects and clinical potential. Echocardiography 2012, 29, 997–1010. [Google Scholar] [CrossRef]
- Nemes, A.; Kormányos, Á.; Rácz, G.; Ruzsa, Z.; Ambrus, N.; Lengyel, C. Normal reference values of tricuspid annular dimensions and functional properties in healthy adults using three-dimensional speckle-tracking echocardiography (insights from the MAGYAR-Healthy Study). Quant. Imaging Med. Surg. 2023, 13, 121–132. [Google Scholar] [CrossRef]
- Volpato, V.; Mor-Avi, V.; Veronesi, F.; Addetia, K.; Yamat, M.; Weinert, L.; Genovese, D.; Tamborini, G.; Pepi, M.; Lang, R.M. Three-dimensional echocardiography investigation of the mechanisms of tricuspid annular dilatation. Int. J. Cardiovasc. Imaging. 2020, 36, 33–43. [Google Scholar] [CrossRef]
- Bieliauskienė, G.; Kažukauskienė, I.; Kramena, R.; Zorinas, A.; Mainelis, A.; Zakarkaitė, D. Three-dimensional analysis of the tricuspid annular geometry in healthy subjects and in patients with different grades of functional tricuspid regurgitation. Cardiovasc. Ultrasound. 2023, 21, 17. [Google Scholar] [CrossRef]
- Nemes, A.; Rácz, G.; Kormányos, Á. Tricuspid Annular Abnormalities in Isolated Left Ventricular Non-compaction-Insights From the Three-dimensional Speckle-Tracking Echocardiographic MAGYAR-Path Study. Front. Cardiovasc. Med. 2022, 9, 694616. [Google Scholar] [CrossRef] [PubMed]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [PubMed]
- Nel, S.; Nihoyannopoulos, P.; Libhaber, E.; Essop, M.R.; Dos Santos, C.F.; Matioda, H.; Waterworth, C.; Grinter, S.; Meel, R.; Peters, F. Echocardiographic Indices of the Left and Right Heart in a Normal Black African Population. J. Am. Soc. Echocardiogr. 2020, 33, 358–367. [Google Scholar] [CrossRef]
- Sato, T.; Tsujino, I.; Ohira, H.; Oyama-Manabe, N.; Yamada, A.; Ito, Y.M.; Goto, C.; Watanabe, T.; Sakaue, S.; Nishimura, M. Validation study on the accuracy of echocardiographic measurements of right ventricular systolic function in pulmonary hypertension. J. Am. Soc. Echocardiogr. 2012, 25, 280–286. [Google Scholar] [CrossRef]
- Tamborini, G.; Pepi, M.; Galli, C.A.; Maltagliati, A.; Celeste, F.; Muratori, M.; Rezvanieh, S.; Veglia, F. Feasibility and accuracy of a routine echocardiographic assessment of right ventricular function. Int. J. Cardiol. 2007, 115, 86–89. [Google Scholar] [CrossRef]
- Ghio, S.; Recusani, F.; Klersy, C.; Sebastiani, R.; Laudisa, M.L.; Campana, C.; Gavazzi, A.; Tavazzi, L. Prognostic usefulness of the tricuspid annular plane systolic excursion in patients with congestive heart failure secondary to idiopathic or ischemic dilated cardiomyopathy. Am. J. Cardiol. 2000, 85, 837–884. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flasckampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Scientific Document Committee of the European Association of Cardiovascular Imaging. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef]
- Nemes, A.; Kormányos, Á.; Ruzsa, Z.; Achim, A.; Ambrus, N.; Lengyel, C. Three-Dimensional Speckle-Tracking Echocardiography-Derived Tricuspid Annular Dimensions and Right Atrial Strains in Healthy Adults-Is There a Relationship? (Insights from the MAGYAR-Healthy Study). J. Clin. Med. 2023, 12, 4240. [Google Scholar] [CrossRef]
- Gual-Capllonch, F.; Cediel, G.; Ferrer, E.; Teis, A.; Juncà, G.; Vallejo, N.; López-Ayerbe, J.; Bayes-Genis, A. Sex-Related Differences in the Mechanism of Functional Tricuspid Regurgitation. Heart Lung Circ. 2021, 30, e16–e22. [Google Scholar] [CrossRef]
- Florescu, D.R.; Muraru, D.; Volpato, V.; Gavazzoni, M.; Caravita, S.; Tomaselli, M.; Ciampi, P.; Florescu, C.; Bălșeanu, T.A.; Parati, G.; et al. Atrial Functional Tricuspid Regurgitation as a Distinct Pathophysiological and Clinical Entity: No Idiopathic Tricuspid Regurgitation Anymore. J. Clin. Med. 2022, 11, 382. [Google Scholar] [CrossRef] [PubMed]
- Muraru, D.; Addetia, K.; Guta, A.C.; Ochoa-Jimenez, R.C.; Genovese, D.; Veronesi, F.; Basso, C.; Iliceto, S.; Badano, L.P.; Lang, R.M. Right atrial volume is a major determinant of tricuspid annulus area in functional tricuspid regurgitation: A three-dimensional echocardiography study. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, G.; Mahadevan, G.; Jimenez, D.; Frenneaux, M.; Steeds, R.P. Reference values for mitral and tricuspid annular dimensions using two-dimensional echocardiography. Echo. Res. Pract. 2014, 1, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Y.; Debs, D.; Khan, M.A.; Nguyen, D.T.; Graviss, E.A.; Shah, D.J. Normal Reference Values and Reproducibility of Tricuspid Annulus Dimensions Using Cardiovascular Magnetic Resonance. Am. J. Cardiol. 2019, 124, 594–598. [Google Scholar] [CrossRef]
- Anwar, A.M.; Soliman, O.I.; Nemes, A.; van Geuns, R.J.M.; Geleijnse, M.L.; ten Cate, F.J. Value of assessment of tricuspid annulus: Real-time three-dimensional echocardiography and magnetic resonance imaging. Int. J. Cardiovasc. Imaging 2007, 23, 701–705. [Google Scholar] [CrossRef]
- Anwar, A.M.; Geleijnse, M.L.; Soliman, O.I.; McGhie, J.S.; Frowijn, R.; Nemes, A.; van den Bosch, A.E.; Galema, T.W.; ten Cate, F.J. Assessment of normal tricuspid valve anatomy in adults by real-time three-dimensional echocardiography. Int. J. Cardiovasc. Imaging 2007, 23, 717–724. [Google Scholar] [CrossRef]
- Muraru, D.; Gavazzoni, M.; Heilbron, F.; Mihalcea, D.J.; Guta, A.C.; Radu, N.; Muscogiuri, G.; Tomaselli, M.; Sironi, S.; Parati, G.; et al. Reference ranges of tricuspid annulus geometry in healthy adults using a dedicated three-dimensional echocardiography software package. Front. Cardiovasc. Med. 2022, 9, 1011931. [Google Scholar] [CrossRef]
- Addetia, K.; Muraru, D.; Veronesi, F.; Jenei, C.; Cavalli, G.; Besser, S.A.; Mor-Avi, V.; Lang, R.M.; Badano, L.P. 3-Dimensional Echocardiographic Analysis of the Tricuspid Annulus Provides New Insights Into Tricuspid Valve Geometry and Dynamics. JACC Cardiovasc. Imaging 2019, 12, 401–412. [Google Scholar] [CrossRef]
- Muraru, D.; Hahn, R.T.; Soliman, O.I.; Faletra, F.F.; Basso, C.; Badano, L.P. 3-Dimensional Echocardiography in Imaging the Tricuspid Valve. JACC Cardiovasc. Imaging 2019, 12, 500–515. [Google Scholar] [CrossRef]
- Kleijn, S.A.; Aly, M.F.A.; Terwee, C.B.; van Rossum, A.C.; Kamp, O. Reliability of left ventricular volumes and function measurements using three-dimensional speckle tracking echocardiography. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 159–168. [Google Scholar] [CrossRef]
- Wood, P.W.; Choy, J.B.; Nanda, N.C.; Becher, H. Left ventricular ejection fraction and volumes: It depends on the imaging method. Echocardiography 2014, 31, 87–100. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | Subjects (n = 119) | TAPSE 17–21 mm (n = 29) | TAPSE ≥22 mm (n = 90) |
|---|---|---|---|
| LA diameter (mm) | 36.9 ± 3.3 | 37.2 ± 3.4 | 36.8 ± 3.2 |
| LV end-diastolic diameter (mm) | 48.1 ± 3.6 | 47.8 ± 3.8 | 48.3 ± 3.6 |
| LV end-diastolic volume (mL) | 105.8 ± 24.0 | 100.4 ± 28.1 | 107.7 ± 22.2 |
| LV end-systolic diameter (mm) | 32.4 ± 3.5 | 31.9 ± 3.2 | 32.6 ± 3.6 |
| LV end-systolic volume (mL) | 38.3 ±9.6 | 36.9 ± 9.0 | 38.9 ± 9.8 |
| Interventricular septum (mm) | 9.1 ± 1.2 | 8.9 ± 1.2 | 9.2 ± 1.2 |
| LV posterior wall (mm) | 9.3 ± 1.4 | 9.4 ± 1.6 | 9.3 ± 1.4 |
| LV ejection fraction (%) | 64.5 ±4.3 | 64.9 ± 3.3 | 64.3 ± 4.6 |
| Data | Subjects (n = 119) | TAPSE 17–21 mm (n = 29) | TAPSE ≥22 mm (n = 90) |
|---|---|---|---|
| LV-EDV (mL) | 85.8 ± 20.8 | 82.4 ± 23.8 | 87.0 ± 19.7 |
| LV-ESV (mL) | 36.1 ± 10.2 | 34.4 ± 12.2 | 36.7 ± 9.4 |
| LV-EF (%) | 58.0 ± 5.7 | 58.8 ± 6.6 | 57.7 ± 5.4 |
| LV mass (g) | 164 ± 32 | 161 ± 28 | 165 ± 33 |
| Data | Subjects (n = 119) | TAPSE 17–21 mm (n = 29) | TAPSE ≥22 mm (n = 90) |
|---|---|---|---|
| Tricuspid annular dimensions | |||
| TAD-D (cm) | 2.55 ± 1.91 | 2.43 ± 0.40 | 2.10 ± 2.19 |
| TAA-D (cm2) | 7.53 ± 1.66 | 7.70 ± 1.91 | 5.70 ± 1.58 |
| TAP-D (cm) | 10.57 ± 1.18 | 10.63 ± 1.22 | 9.30 ± 1.17 |
| TAD-S (cm) | 1.84 ± 0.29 | 1.90 ± 0.40 | 1.70 ± 0.25 |
| TAA-S (cm2) | 5.41 ± 1.43 | 5.85 ± 1.90 | 3.70 ± 1.22 * |
| TAP-S (cm) | 9.11 ± 1.11 | 9.32 ± 1.30 | 7.70 ± 1.05 |
| Tricuspid annular ”sphincter-like” functional parameters | |||
| TAFAC (%) | 28.1 ± 9.2 | 24.8 ± 9.0 | 35.1 ± 9.1 * |
| TAFS (%) | 23.0 ± 10.9 | 21.8 ± 10.2 | 19.1 ± 11.1 |
| Tricuspid annular longitudinal functional parameter | |||
| TAPSE (mm) | 23.8 ± 2.9 | 20.2 ± 0.9 | 23.0 ± 2.3 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nemes, A.; Rácz, G.; Kormányos, Á.; Ruzsa, Z.; Achim, A.; Lengyel, C. The Relationship between Tricuspid Annular Longitudinal and Sphincter-like Features of Its Function in Healthy Adults: Insights from the MAGYAR-Healthy Study. Life 2023, 13, 2079. https://doi.org/10.3390/life13102079
Nemes A, Rácz G, Kormányos Á, Ruzsa Z, Achim A, Lengyel C. The Relationship between Tricuspid Annular Longitudinal and Sphincter-like Features of Its Function in Healthy Adults: Insights from the MAGYAR-Healthy Study. Life. 2023; 13(10):2079. https://doi.org/10.3390/life13102079
Chicago/Turabian StyleNemes, Attila, Gergely Rácz, Árpád Kormányos, Zoltán Ruzsa, Alexandru Achim, and Csaba Lengyel. 2023. "The Relationship between Tricuspid Annular Longitudinal and Sphincter-like Features of Its Function in Healthy Adults: Insights from the MAGYAR-Healthy Study" Life 13, no. 10: 2079. https://doi.org/10.3390/life13102079