
An Analysis of the Content of Metalloproteinases in the Intestinal Wall of Patients with Crohn’s Disease

 ,
,  , , ,
, , ,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Large Intestine Tissue Samples
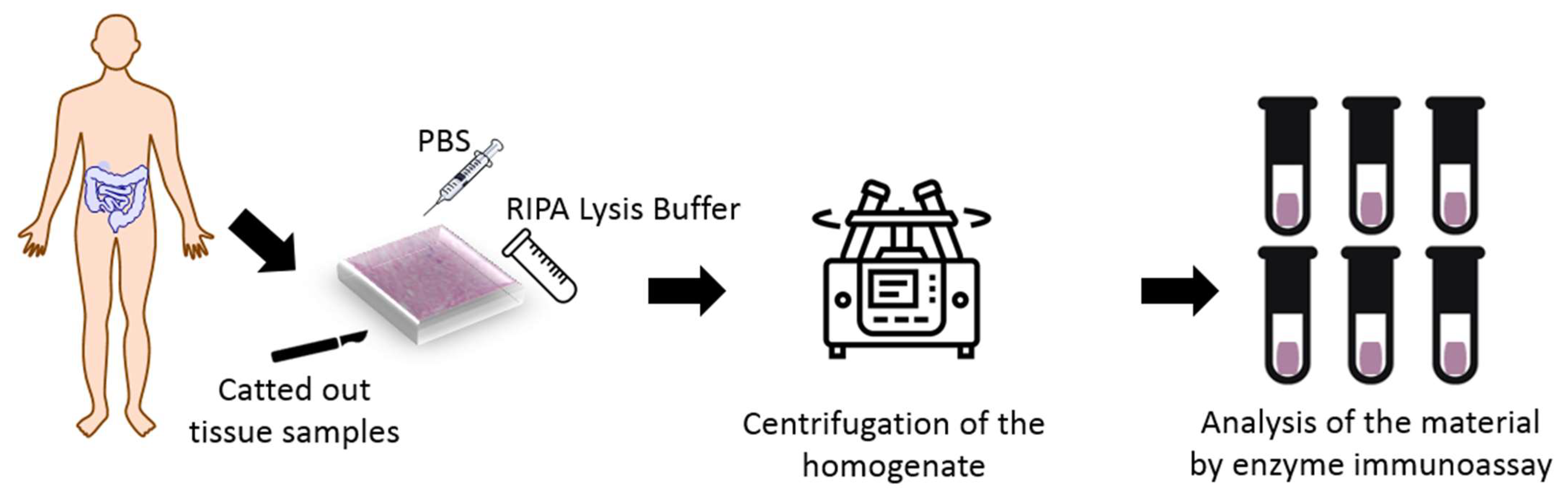
2.2. Procedure of Preparation Samples
2.3. Characteristics of Enzyme-Linked Immunosorbent Assay
2.4. Statistical Analysis
3. Results
4. Discussion
Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alfredsson, J.; Wick, M.J. Mechanism of fibrosis and stricture formation in Crohn’s disease. Scand. J. Immunol. 2020, 92, e12990. [Google Scholar] [CrossRef] [PubMed]
- Pasternak, G.; Bartusik-Aebisher, D.; Aebisher, D.; Filip, R. Crohn’s disease–A case study. Eur. J. Clin. Exp. Med. 2021, 19, 93–97. [Google Scholar] [CrossRef]
- Feuerstein, J.D.; Cheifetz, A.S. Crohn Disease: Epidemiology, Diagnosis, and Management. Mayo Clin. Proc. 2017, 92, 1088–1103. [Google Scholar] [CrossRef] [PubMed]
- Ballester Ferré, M.P.; Boscá-Watts, M.M.; Mínguez Pérez, M. Crohn’s disease. Med. Clin. 2018, 151, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Song, E.M.; Kim, N.; Lee, S.-H.; Chang, K.; Hwang, S.W.; Park, S.H.; Yang, D.-H.; Byeon, J.-S.; Myung, S.-J.; Yang, S.-K.; et al. Clinical characteristics and long-term prognosis of elderly-onset Crohn’s disease. Scand. J. Gastroenterol. 2018, 53, 417–425. [Google Scholar] [CrossRef]
- Cullen, M.; Barnes, C. Crohn’s disease in adolescence: Presentation and treatment. Nurs. Stand. 2015, 29, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Gajendran, M.; Loganathan, P.; Catinella, A.P.; Hashash, J.G. A comprehensive review and update on Crohn’s disease. Dis. Mon. 2018, 64, 20–57. [Google Scholar] [CrossRef]
- Seyedian, S.S.; Nokhostin, F.; Malamir, M.D. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef]
- Laass, M.W.; Roggenbuck, D.; Conrad, K. Diagnosis and classification of Crohn’s disease. Autoimmun. Rev. 2014, 13, 467–471. [Google Scholar] [CrossRef]
- Mazal, J. Crohn disease: Pathophysiology, diagnosis, and treatment. Radiol. Technol. 2014, 85, 297–316. [Google Scholar]
- Ueno, A.; Jijon, H.B.; Peng, R.; Sparksman, S.; Mainoli, B.; Filyk, A.; Li, Y.; Wilson, S.; Novak, K.; Panaccione, R.; et al. Association of Circulating Fibrocytes with Fibrostenotic Small Bowel Crohn’s Disease. Inflamm. Bowel Dis. 2022, 28, 246–258. [Google Scholar] [CrossRef]
- Steell, L.; Gray, S.R.; Russell, R.K.; MacDonald, J.; Seenan, J.P.; Wong, S.C.; Gaya, D.R. Pathogenesis of Musculoskeletal Deficits in Children and Adults with Inflammatory Bowel Disease. Nutrients 2021, 13, 2899. [Google Scholar] [CrossRef] [PubMed]
- Pahwa, R.; Goyal, A.; Jialal, I. Chronic Inflammation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493173/ (accessed on 31 March 2023).
- Rosen, M.J.; Dhawan, A.; Saeed, S.A. Inflammatory Bowel Disease in Children and Adolescents. JAMA Pediatr. 2015, 169, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Agency for Health Technology. Assessment and Tariff System. Available online: https://bipold.aotm.gov.pl/ (accessed on 31 March 2023).
- Gouldthorpe, O.; Catto-Smith, A.G.; Alex, G. Biologics in paediatric Crohn’s disease. Gastroenterol. Res. Pract. 2011, 2011, 287574. [Google Scholar] [CrossRef] [PubMed]
- Crohn’s and Colitis Foundation. The Facts about Inflammatory Bowel Diseases, Crohn’s & Colitis Foundation of America. Available online: https://www.crohnscolitisfoundation.org/sites/default/files/2019-02/Updated%20IBD%20Factbook.pdfdation.org/sites/default/files/2019-02/Updated%20IBD%20Factbook.pdf (accessed on 31 March 2023).
- Mills, S.C.; von Roon, A.C.; Tekkis, P.P.; Orchard, T.R. Crohn’s disease. BMJ Clin. Evid. 2011, 27, 0416. [Google Scholar]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Waschkau, B.; Faust, A.; Schäfers, M.; Bremer, C. Performance of a new fluorescence-labeled MMP inhibitor to image tumor MMP activity in vivo in comparison to an MMP-activatable probe. Contrast Media Mol. Imaging 2013, 8, 1–11. [Google Scholar] [CrossRef]
- Son, J.; Parveen, S.; MacPherson, D.; Marciano, Y.; Huang, R.H.; Ulijn, R.V. MMP-Responsive Nanomaterials. Biomater. Sci. 2023, 11, 6457–6479. [Google Scholar] [CrossRef]
- Tajhya, R.B.; Patel, R.S.; Beeton, C. Detection of Matrix Metalloproteinases by Zymography. Methods Mol. Biol. 2017, 1579, 231–244. [Google Scholar] [CrossRef]
- Bornstein, P.; Sage, E. Matricellular proteins: Extracellular modulators of cell function. Curr. Opin. Cell Biol. 2002, 14, 608–616. [Google Scholar] [CrossRef]
- Kirkegaard, T.; Hansen, A.; Bruun, E.; Brynskov, J. Expression and localisation of matrix metalloproteinases and their natural inhibitors in fistulae of patients with Crohn’s disease. Gut 2004, 53, 701–709. [Google Scholar] [CrossRef]
- Haq, M.; Shaeii, A.E.; Zervos, E.E.; Rosemurgy, A.S. In vitro and in vivo matrix metalloproteinase production by pancreatic cancer cells and by distant organs. Int. J. Surg. Investig. 2000, 1, 459–465. [Google Scholar] [PubMed]
- Egeblad, M.; Werb, Z. New functions for the matrix metalloproteinases in cancer progression. Nat. Rev. Cancer 2002, 2, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Giantin, M.; Aresu, L.; Benali, S.; Arico, A.; Morello, E.M.; Martano, M.; Vascellari, M.; Castagnaro, M.; Lopparelli, R.M.; Zancanella, V.; et al. Expression of matrix metalloproteinases, tissue inhibitors of metalloproteinases and vascular endothelial growth factor in canine mast cell tumours. J. Comp. Path. 2012, 147, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Wysocka, A.; Giziński, S.; Lechowski, R. Matrix metalloproteinases-their structure and function. Życie Weter. 2014, 89, 223–227. [Google Scholar]
- Efsen, E.; Saermark, T.; Hansen, A.; Bruun, E.; Brynskov, J. Ramiprilate inhibits functional matrix metalloproteinase activity in Crohn’s disease fistulas. Basic Clin. Pharmacol. Toxicol. 2011, 109, 208–2016. [Google Scholar] [CrossRef] [PubMed]
- Candelario-Jalil, E.; Yang, Y.; Rosenberg, G.A. Diverse roles of matrix metalloproteinases and tissue inhibitors of metalloproteinases in neuroinflammation and cerebral ischemia. Neuroscience 2009, 158, 983–994. [Google Scholar] [CrossRef]
- Pasternak, G.; Aebisher, D.; Filip, R.; Bartusik-Aebisher, D. Inflammatory bowel disease: The function of metalloproteinases. Eur. J. Clin. Exp. Med. 2018, 16, 346–349. [Google Scholar] [CrossRef]
- Kofla-Dlubacz, A.; Matusiewicz, M.; Krzystek-Korpacka, M.; Iwanczak, B. Correlation of MMP-3 and MMP-9 with Crohn’s disease activity in children. Dig. Dis. Sci. 2012, 57, 706–712. [Google Scholar] [CrossRef]
- Yablecovitch, D.; Kopylov, U.; Lahat, A.; Amitai, M.M.; Klang, E.; Ben-Ami Shor, D.; Neuman, S.; Levhar, N.; Fudim, E.; Avidan, B.; et al. Serum MMP-9: A novel biomarker for prediction of clinical relapse in patients with quiescent Crohn’s disease, a post hoc analysis. Therap. Adv. Gastroenterol. 2019, 12, 1756284819881590. [Google Scholar] [CrossRef]
- Meijer, M.J.; Mieremet-Ooms, M.A.; van der Zon, A.M.; van Duijn, W.; van Hogezand, R.A.; Sier, C.F.; Hommes, D.W.; Lamers, C.B.; Verspaget, H.W. Increased mucosal matrix metalloproteinase-1, -2, -3 and -9 activity in patients with inflammatory bowel disease and the relation with Crohn’s disease phenotype. Dig. Liver Dis. 2007, 39, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Rath, T.; Roderfeld, M.; Graf, J.; Wagner, S.; Vehr, A.K.; Dietrich, C.; Geier, A.; Roeb, E. Enhanced expression of MMP-7 and MMP-13 in inflammatory bowel disease: A precancerous potential? Inflamm. Bowel Dis. 2006, 12, 1025–1035. [Google Scholar] [CrossRef]
- Jakubowska, K.; Pryczynicz, A.; Iwanowicz, P.; Niewiński, A.; Maciorkowska, E.; Hapanowicz, J.; Jagodzińska, D.; Kemona, A.; Guzińska-Ustymowicz, K. Expressions of Matrix Metalloproteinases (MMP-2, MMP-7, and MMP-9) and Their Inhibitors (TIMP-1, TIMP-2) in Inflammatory Bowel Diseases. Gastroenterol. Res. Pract. 2016, 2016, 2456179. [Google Scholar] [CrossRef]
- Mäkitalo, L.; Rintamäki, H.; Tervahartiala, T.; Sorsa, T.; Kolho, K.L. Serum MMPs 7-9 and their inhibitors during glucocorticoid and anti-TNF-α therapy in pediatric inflammatory bowel disease. Scand. J. Gastroenterol. 2012, 47, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Mäkitalo, L.; Kolho, K.L.; Karikoski, R.; Anthoni, H.; Saarialho-Kere, U. Expression profiles of matrix metalloproteinases and their inhibitors in colonic inflammation related to pediatric inflammatory bowel disease. Scand. J. Gastroenterol. 2010, 45, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Marcello, P.W.; Schoetz, D.J.; Roberts, P.L., Jr.; Murray, J.J.; Coller, J.A.; Rusin, L.C.; Veidenheimer, M.C. Evolutionary changes in the pathologic diagnosis after the ileoanal pouch procedure. Dis. Colon Rectum 1997, 40, 263–269. [Google Scholar] [CrossRef]
- Tontini, G.E.; Vecchi, M.; Pastorelli, L.; Neurath, M.F.; Neumann, H. Differential diagnosis in inflammatory bowel disease colitis: State of the art and future perspectives. World J. Gastroenterol. 2015, 21, 21–46. [Google Scholar] [CrossRef]
- Derkacz, A.; Olczyk, P.; Olczyk, K.; Komosinska-Vassev, K. The role of extracellular matrix components in inflammatory bowel diseases. J. Clin. Med. 2021, 10, 1122. [Google Scholar] [CrossRef]
- Siegmund, B.; Feakins, R.M.; Barmias, G.; Ludvig, J.C.; Teixeira, F.V.; Rogler, G.; Scharl, M. Results of the Fifth Scientific Workshop of the ECCO (II): Pathophysiology of perianal fistulizing disease. J. Crohns Colitis 2016, 10, 377–386. [Google Scholar] [CrossRef]
- McGregor, C.G.C.; Tandon, R.; Simmons, A. Pathogenesis of Fistulating Crohn’s Disease: A Review. Cell Mol. Gastroenterol. Hepatol. 2023, 15, 1–11. [Google Scholar] [CrossRef]
- Schuppan, D.; Freitag, T. Fistulising Crohn’s disease: MMPs gone awry. Gut 2004, 53, 622–624. [Google Scholar] [CrossRef]
- Andoh, A.; Bamba, S.; Brittan, M.; Fujiyama, Y.; Wright, N.A. Role of intestinal subepithelial myofibroblasts in inflammation and regenerative response in the gut. Pharmacol. Ther. 2007, 114, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Siloşi, I.; Boldeanu, M.V.; Mogoantă, S.Ş.; Ghiluşi, M.; Cojocaru, M.; Biciuşcă, V.; Cojocaru, I.M.; Avrămescu, C.S.; Gheonea, D.I.; Siloşi, C.A.; et al. Matrix metalloproteinases (MMP-3 and MMP-9) implication in the pathogenesis of inflammatory bowel disease (IBD). Rom. J. Morphol. Embryol. 2014, 55, 1317–1324. [Google Scholar] [PubMed]
- Drygiannakis, I.; Valatas, V.; Sfakianaki, O.; Bourikas, L.; Manousou, P.; Kambas, K.; Ritis, K.; Kolios, G.; Kouroumalis, E. Proinflammatory cytokines induce crosstalk between colonic epithelial cells and subepithelial myofibroblasts: Implication in intestinal fibrosis. J. Crohn’s Colitis 2013, 7, 286–300. [Google Scholar] [CrossRef] [PubMed]
- de Bruyn, M.; Vandooren, J.; Ugarte-Berzal, E.; Arijs, I.; Vermeire, S.; Opdenakker, G. B The molecular biology of matrix metalloproteinases and tissue inhibitors of metalloproteinases in inflammatory bowel diseases. Crit. Rev. Biochem. Mol. Biol. 2016, 51, 295–358. [Google Scholar] [CrossRef]
- de Almeida, L.G.; Thode, H.; Eslambolchi, Y.; Chopra, S.; Young, D.; Gill, S.; Devel, L.; Dufour, A. Matrix Metalloproteinases: From Molecular Mechanisms to Physiology, Pathophysiology, and Pharmacology. Pharmacol. Rev. 2022, 74, 712–768. [Google Scholar] [CrossRef] [PubMed]
- Coward, S.; Clement, F.; Williamson, T.; Hazlewood, G.; Ng, S.; Heitman, S.; Seow, C.; Panaccione, R.; Ghosh, S.; Kaplan, G.G. The rising burden of inflammatory bowel disease in North America from 2015 to 2025: A predictive model. Am. J. Gastroenterol. 2015, 110, S829. [Google Scholar] [CrossRef]
- Sagi, I.; Gaffney, J.P.; Dufour, A.; Overall, C.M. Subtracting matrix out of the equation: New key roles of matrix metalloproteinases in innate immunity and disease. In Matrix Metalloproteinase Biology; Sagi, I., Gaffney, J.P., Eds.; John Wiley and Sons: Hoboken, NJ, USA, 2015; pp. 131–152. [Google Scholar]
- Marônek, M.; Marafini, I.; Gardlík, R.; Link, R.; Troncone, E.; Monteleone, G. Metalloproteinases in Inflammatory Bowel Diseases. J. Inflamm. Res. 2021, 14, 1029–1041. [Google Scholar] [CrossRef]
- Hu, J.; Van den Steen, P.E.; Sang, Q.-X.A.; Opdenakker, G. Matrix metalloproteinase inhibitors as therapy for inflammatory and vascular diseases. Nat. Rev. Drug Discov. 2007, 6, 480–498. [Google Scholar] [CrossRef]
- Yoo, J.; Perez, C.E.R.; Nie, W.; Sinnett-Smith, J.; Rozengurt, E. Protein kinase D1 mediates synergistic MMP-3 expression induced by TNF-α and bradykinin in human colonic myofibroblasts. Biochem. Biophys. Res. Commun. 2011, 413, 30–35. [Google Scholar] [CrossRef]
- Yagi, Y.; Andoh, A.; Inatomi, O.; Tsujikawa, T.; Fujiyama, Y. Inflammatory responses induced by interleukin-17 family members in human colonic subepithelial myofibroblasts. J. Gastroenterol. 2007, 42, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Rojas, M.; Ravi, A.; Bockbrader, K.; Epstein, S.; Vijay-Kumar, M.; Gewirtz, A.T.; Merlin, D.; Sitaraman, S.V. Selective ablation of matrix metalloproteinase-2 exacerbates experimental colitis: Contrasting role of gelatinases in the pathogenesis of colitis. J. Immunol. 2006, 177, 4103–4112. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.; Udi, Y.; Solomonov, I.; Sagi, I. Next generation matrix metalloproteinase inhibitors—Novel strategies bring new prospects. Biochim. Biophys. Acta Mol Cell Res. 2017, 1864, 1927–1939. [Google Scholar] [CrossRef]
- Winer, A.; Adams, S.; Mignatti, P. Matrix metalloproteinase inhibitors in cancer therapy: Turning past failures into future successes. Mol. Cancer Ther. 2018, 17, 1147–1155. [Google Scholar] [CrossRef]
- Kessenbrock, K.; Plaks, V.; Werb, Z. Matrix metalloproteinases: Regulators of the tumor microenvironment. Cell 2010, 141, 52–67. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, S.; Gilmer, J.F.; Medina, C. Matrix metalloproteinases in inflammatory bowel disease: An update. Mediat. Inflamm. 2015, 2015, 964131. [Google Scholar] [CrossRef]
- Koelink, P.J.; Overbeek, S.A.; Braber, S.; Morgan, M.E.; Henricks, P.A.J.; Roda, M.A.; Verspaget, H.W.; Wolfkamp, S.C.; Velde, A.A.T.; Jones, C.W.; et al. Collagen degradation and neutrophilic infiltration: A vicious circle in inflammatory bowel disease. Gut 2014, 63, 578–587. [Google Scholar] [CrossRef]
- Shi, J.; Aono, S.; Lu, W.; Ouellette, A.J.; Hu, X.; Ji, Y.; Wang, L.; Lenz, S.; van Ginkel, F.W.; Liles, M.; et al. A novel role for defensins in intestinal homeostasis: Regulation of IL-1beta secretion. J. Immunol. 2007, 179, 1245–1253. [Google Scholar] [CrossRef]
- Swee, M.; Wilson, C.L.; Wang, Y.; McGuire, J.K.; Parks, W.C. Matrix metalloproteinase-7 (matrilysin) controls neutrophil egress by generating chemokine gradients. J. Leukoc. Biol. 2008, 83, 1404–1412. [Google Scholar] [CrossRef]
- Deleon-Pennell, K.Y.; Altara, R.; Yabluchanskiy, A.; Modesti, A.; Lindsey, M.L. The circular relationship between matrix metalloproteinase-9 and inflammation following myocardial infarction. IUBMB Life 2015, 67, 611–618. [Google Scholar] [CrossRef]
- Vandenbroucke, R.E.; Dejonckheere, E.; Van Hauwermeiren, F.; Lodens, S.; De Rycke, R.; Van Wonterghem, E.; Staes, A.; Gevaert, K.; López-Otin, C.; Libert, C. Matrix metalloproteinase 13 modulates intestinal epithelial barrier integrity in inflammatory diseases by activating TNF. EMBO Mol. Med. 2013, 5, 1000–1016. [Google Scholar] [CrossRef]
- Kalebic, T.; Garbisa, S.; Glaser, B.; Liotta, L.A. Basement membrane collagen: Degradation by migrating endothelial cells. Science 1983, 221, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Heljasvaara, R.; Nyberg, P.; Luostarinen, J.; Parikka, M.; Heikkilä, P.; Rehn, M.; Sorsa, T.; Salo, T.; Pihlajaniemi, T. Generation of biologically active endostatin fragments from human collagen XVIII by distinct matrix metalloproteases. Exp. Cell Res. 2005, 307, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jilan, S.M.; Nikolova, G.V.; Carpizo, D.; Iruela-Arispe, M.L. Processing of VEGF-A by matrix metalloproteinases regulates bioavailability and vascular patterning in tumors. J. Cell Biol. 2005, 169, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Scaldaferri, F.; Vetrano, S.; Sans, M.; Arena, V.; Straface, G.; Stigliano, E.; Repici, A.; Sturm, A.; Malesci, A.; Panes, J.; et al. VEGF-A links angiogenesis and inflammation in inflammatory bowel disease pathogenesis. Gastroenterology 2009, 136, 585–595.e5. [Google Scholar] [CrossRef] [PubMed]
- Tolstanova, G.; Deng, X.; Khomenko, T.; Garg, P.; Paunovic, B.; Chen, L.; Sitaraman, S.V.; Shiloach, J.; Szabo, S.; Sandor, Z. Role of anti-angiogenic factor endostatin in the pathogenesis of experimental ulcerative colitis. Life Sci. 2011, 88, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Patel, N.R.; Walter, L.; Ingersoll, S.; Sitaraman, S.V.; Garg, P. Constitutive expression of MMP9 in intestinal epithelium worsens murine acute colitis and is associated with increased levels of proinflammatory cytokine Kc. Am. J. Physiol. Gastrointest. Liver Physiol. 2013, 304, G793–G803. [Google Scholar] [CrossRef]
- Pope, J.L.; Bhat, A.A.; Sharma, A.; Ahmad, R.; Krishnan, M.; Washington, M.K.; Beauchamp, R.D.; Singh, A.B.; Dhawan, P. Claudin-1 regulates intestinal epithelial homeostasis through the modulation of Notch-signalling. Gut 2014, 63, 622–634. [Google Scholar] [CrossRef]
- Garg, P.; Ravi, A.; Patel, N.R.; Roman, J.; Gewirtz, A.T.; Merlin, D.; Sitaraman, S.V. Matrix metalloproteinase-9 regulates MUC-2 expression through its effect on goblet cell differentiation. Gastroenterology 2007, 132, 1877–1889. [Google Scholar] [CrossRef]
- Hayden, D.M.; Forsyth, C.; Keshavarzian, A. The role of matrix metalloproteinases in intestinal epithelial wound healing during normal and inflammatory states. J. Surg. Res. 2011, 168, 315–324. [Google Scholar] [CrossRef]
- Medina, C.; Santos-Martinez, M.J.; Santana, A.; Paz-Cabrera, M.C.; Johnston, M.J.; Mourelle, M.; Salas, A.; Guarner, F. Transforming growth factor-beta type 1 receptor (ALK5) and Smad proteins mediate TIMP-1 and collagen synthesis in experimental intestinal fibrosis. J. Pathol. 2011, 224, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.R.; Bland, P.W.; Tarlton, J.F.; Peters, I.; Moorghen, M.; Sylvester, P.A.; Probert, C.S.; Whiting, C.V. IL-13 promotes collagen accumulation in Crohn’s disease fibrosis by down-regulation of fibroblast MMP synthesis: A role for innate lymphoid cells? PLoS ONE 2012, 7, e52332. [Google Scholar] [CrossRef] [PubMed]
- Brew, K.; Dinakarpandian, D.; Nagase, H. Tissue inhibitors of metalloproteinases: Evolution, structure and function. Biochim. Biophys. Acta 2000, 1477, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Busti, C.; Falcinelli, E.; Momi, S.; Gresele, P. Matrix metalloproteinases and peripheral arterial disease. Intern. Emerg. Med. 2010, 5, 13–25. [Google Scholar] [CrossRef]
- Lambert, E.; Dassé, E.; Haye, B.; Petitfrere, E. TIMPs as multifacial proteins. Crit. Rev. Oncol. Hematol. 2004, 49, 187–198. [Google Scholar] [CrossRef]
- Opdenakker, G.; Vermeire, S.; Abu El-Asrar, A. How to place the duality of specific MMP-9 inhibition for treatment of inflammatory bowel diseases into clinical opportunities? Front. Immunol. 2022, 9, 983964. [Google Scholar] [CrossRef]
- Pujada, A.; Walter, L.; Dhere, T.; Garg, P. Matrix metalloproteinases as potential fecal biomarkers for ulcerative colitis—A function beyond their proteolytic activity. Met. Med. 2016, 3, 19–29. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue Type | Gender Females Males | Age (Years) Range Mean | Smoker Non-Smoker | Type of Procedure Resection Colectomy | The Number of Complications | ||||
|---|---|---|---|---|---|---|---|---|---|
| Crohn’s disease patient (sick tissue) | 13 | 18 | 23–70 | 40.4 | 6 | 25 | 30 | 1 | 10 |
| Control tissue (healthy tissue) | Healthy tissues are the margin of tissue collected during the procedure without any signs of disease | ||||||||
| Patient Number | Type of Treatment | Reoperation (Year, Type) |
|---|---|---|
| 1 | Azathioprine, 5-ASA | 2011, Subtotal colectomy |
| 2 | Azathioprine, 5-ASA | 2015, Subtotal colectomy |
| 3 | Infliximab, Adalimumab, Mercaptopurine, Encorton | 2014, ileal resection and right hemicolectomy |
| 4 | Azathioprine, 5-ASA | |
| 5 | Azathioprine, 5-ASA | |
| 6 | Solu-Medrol, Encorton | |
| 7 | Ciprofloxacin, Metronidazole, Steroid therapy | |
| 8 | Immunosuppression, Asamax, Encorton, Hydrocortison, Proxacin, Metronidazole | |
| 9 | Solu-Medrol, Asamax, Cipropol, Metronidazole | |
| 10 | Azathioprine, Solu-Medrol, Cipronex, Metronidazole | |
| 11 | Azathioprine, Asamax, Proxacin, Metronidazole | 2003, sigmoid resection |
| 12 | Proxacin, Metronidazole, Corhydron | |
| 13 | Azathioprine, Encorton | |
| 14 | Azathioprine, Solu-Medrol, Tazocin, Metronidazole | |
| 15 | Azathioprine, Ciprofloxacin, Metronidazole | 2018, ileocecal resection |
| 16 | Azathioprine, Pentasa, Biotraxon, Metronidazole | 2015, left hemicolectomy 2018, rectal resection |
| 17 | Pentasa, Proxacin, Metronidazole | |
| 18 | Pentasa, Proxacin, Metronidazole | |
| 19 | Mercaptopurine, Encorton, Hydrocortisone | |
| 20 | Azathioprine, Asamax, Biotraxon, Metronidazole, Infliximab | |
| 21 | Azathioprine, Tazocin | |
| 22 | Azathioprine, Proxacin, Metronidazole | |
| 23 | Azathioprine, Asamax, Encorton, Proxacin, Metronidazole | |
| 24 | Azathioprine, Solu-Medrol, Metypred (methylprednisolone) | |
| 25 | Azathioprine, Mesalazine, Encorton, Biotraxon, Metronidazole | |
| 26 | Azathioprine, Amoksiklav, Biotraxon, Metronidazole | |
| 27 | Solu-Medrol, Proxacin, Metronidazole | |
| 28 | Infliximab, Adalimumab, Hydrocortison, Proxacin, Metronidazole | |
| 29 | Cipronex, Metronidazole, Modulen IBD | |
| 30 | Infliximab, Azathioprine | |
| 31 | Azathioprine, Amoksiklav, Biotraxon, Metronidazole |
| Assay Kit |
|---|
| Pre-coated, ready to use 96-well strip plate |
| Standard and Standard Diluent |
| Detection Reagent A and Assay Diluent A |
| Detection Reagent B and Assay Diluent B |
| TMB Substrate and Stop Solution |
| Wash Buffer (30× concentrate) |
| MMPs | Sick Tissue (n = 30) [pg per mg Tissue] | Healthy Tissue (n = 10) [pg per mg Tissue] | p-Value |
|---|---|---|---|
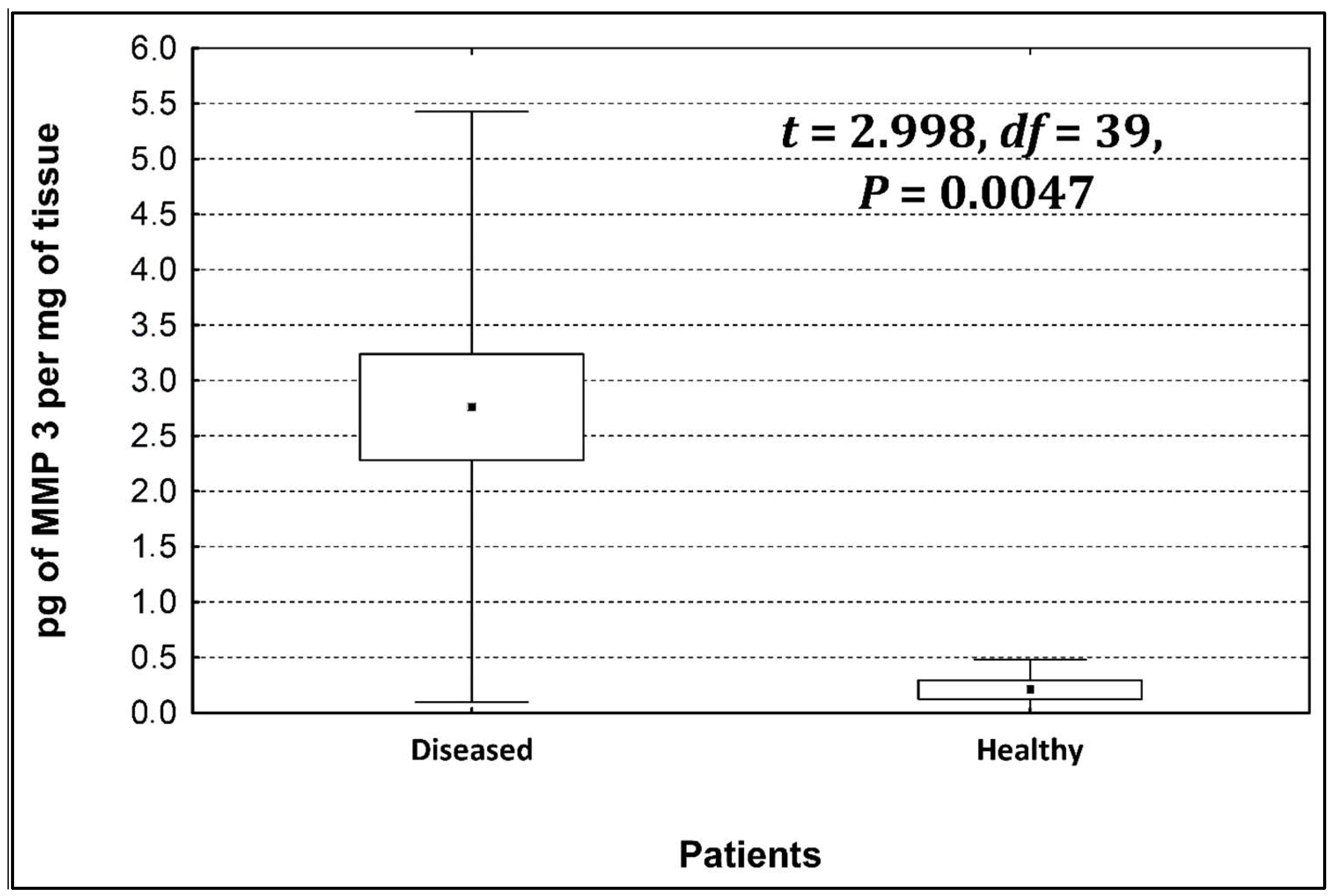
| MMP-3 | 2.8 ± 2.6 | 0.21 ± 0.25 | 0.0047 * |
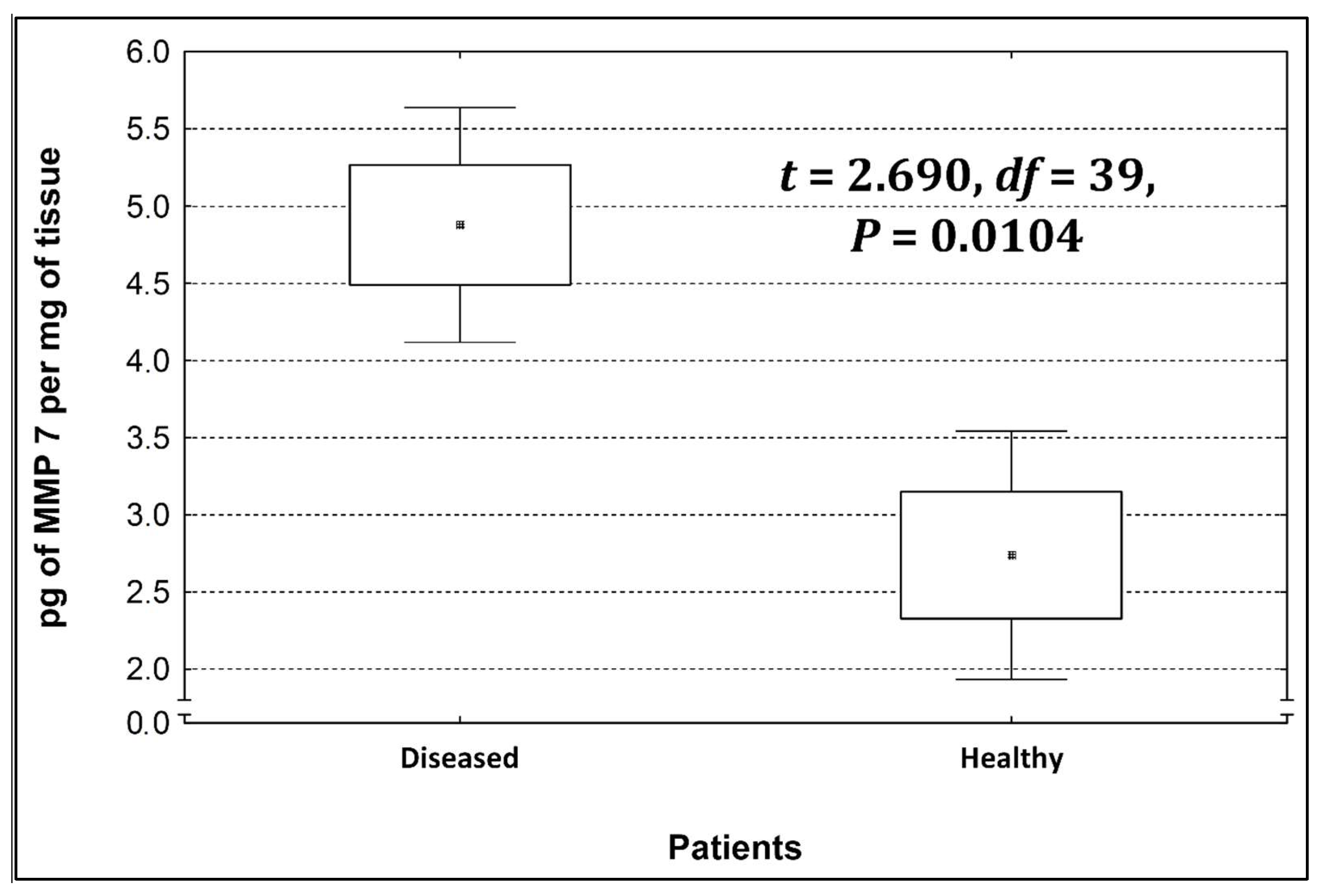
| MMP-7 | 4.9 ± 0.8 | 2.75 ± 0.85 | 0.0104 * |
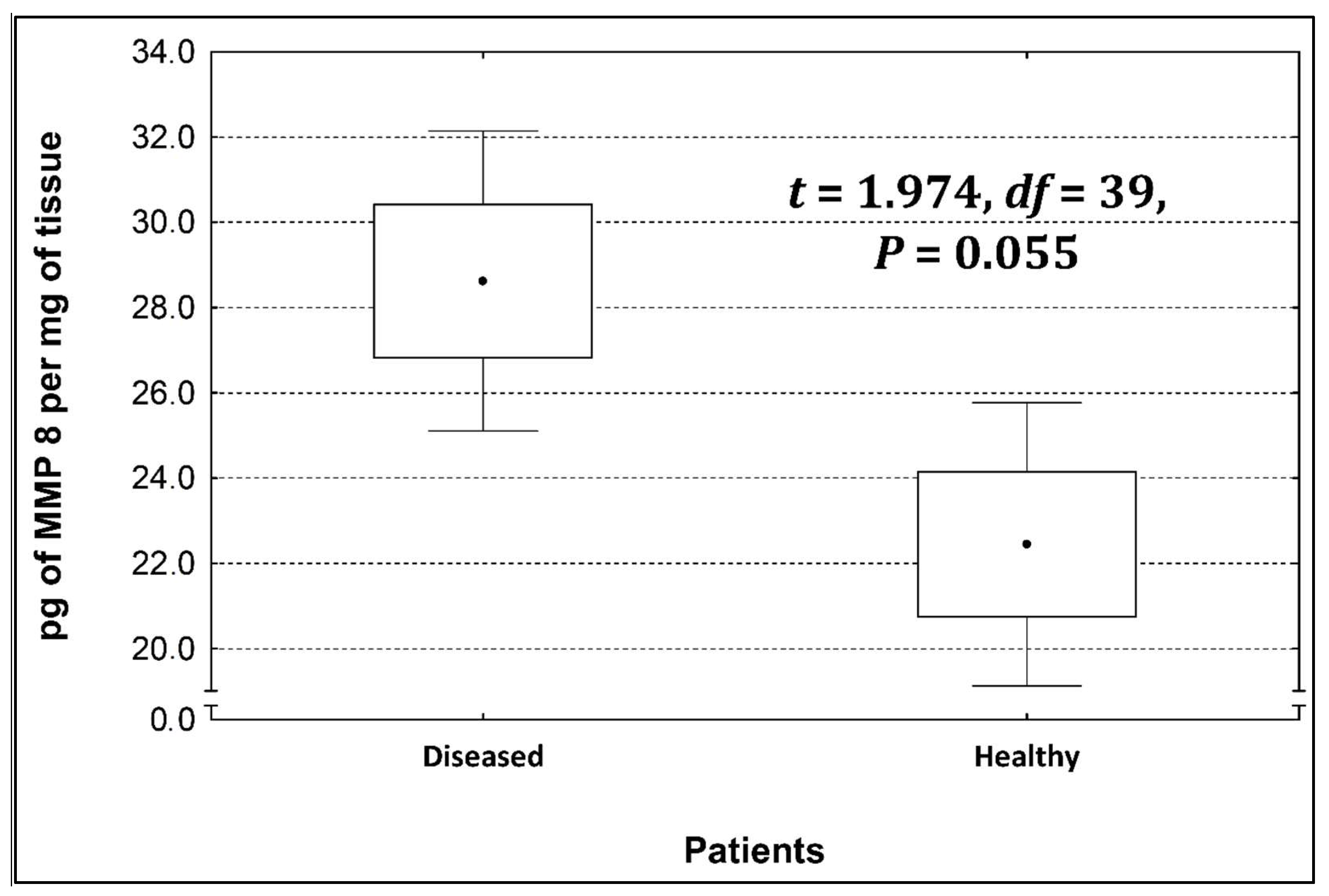
| MMP-8 | 28.3 ± 2.8 | 22.4 ± 3.5 | 0.055 |
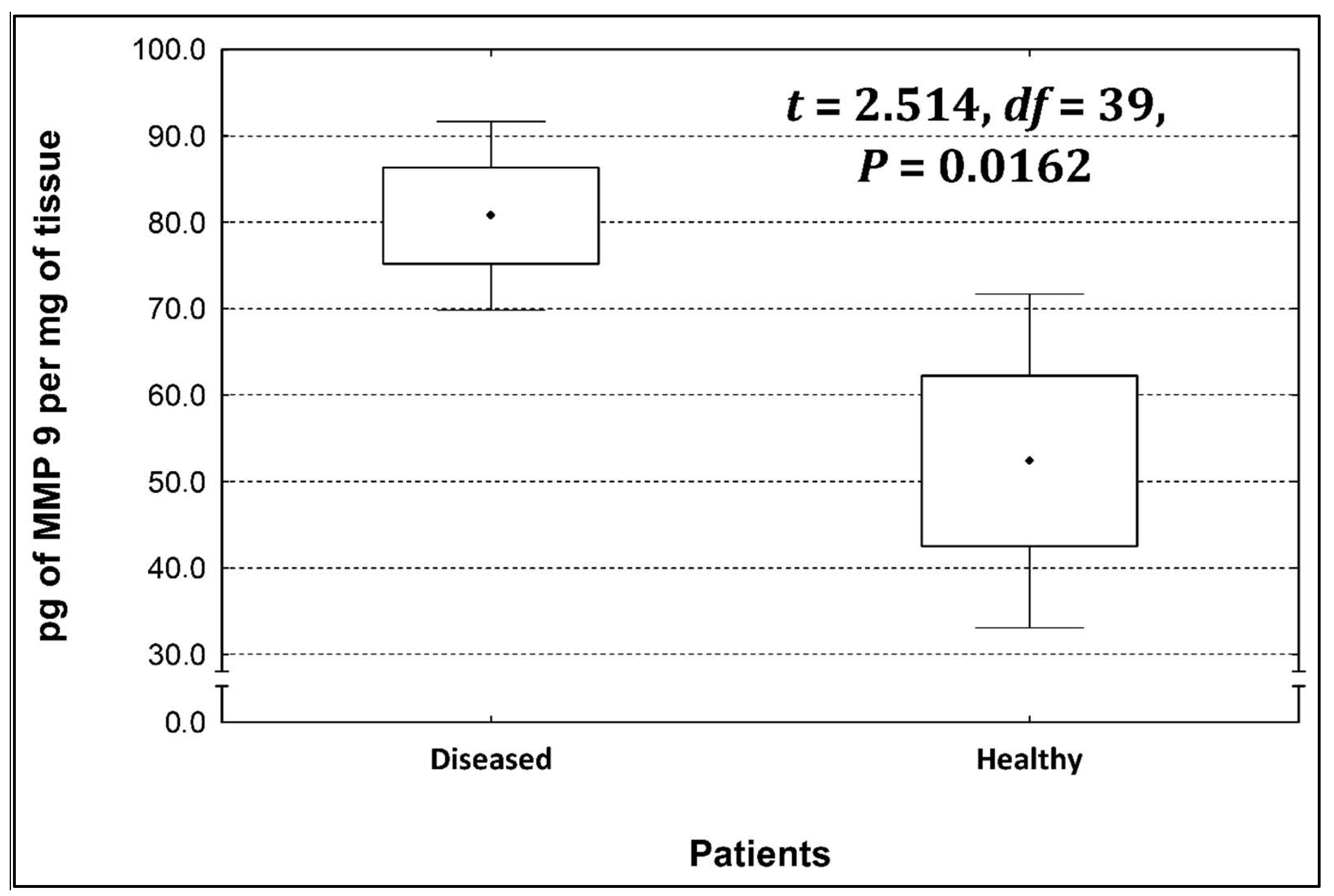
| MMP-9 | 80.8 ± 10.8 | 52.5 ± 18.5 | 0.0162 * |
| Variables | Parameter Estimate | SE | F | p |
|---|---|---|---|---|
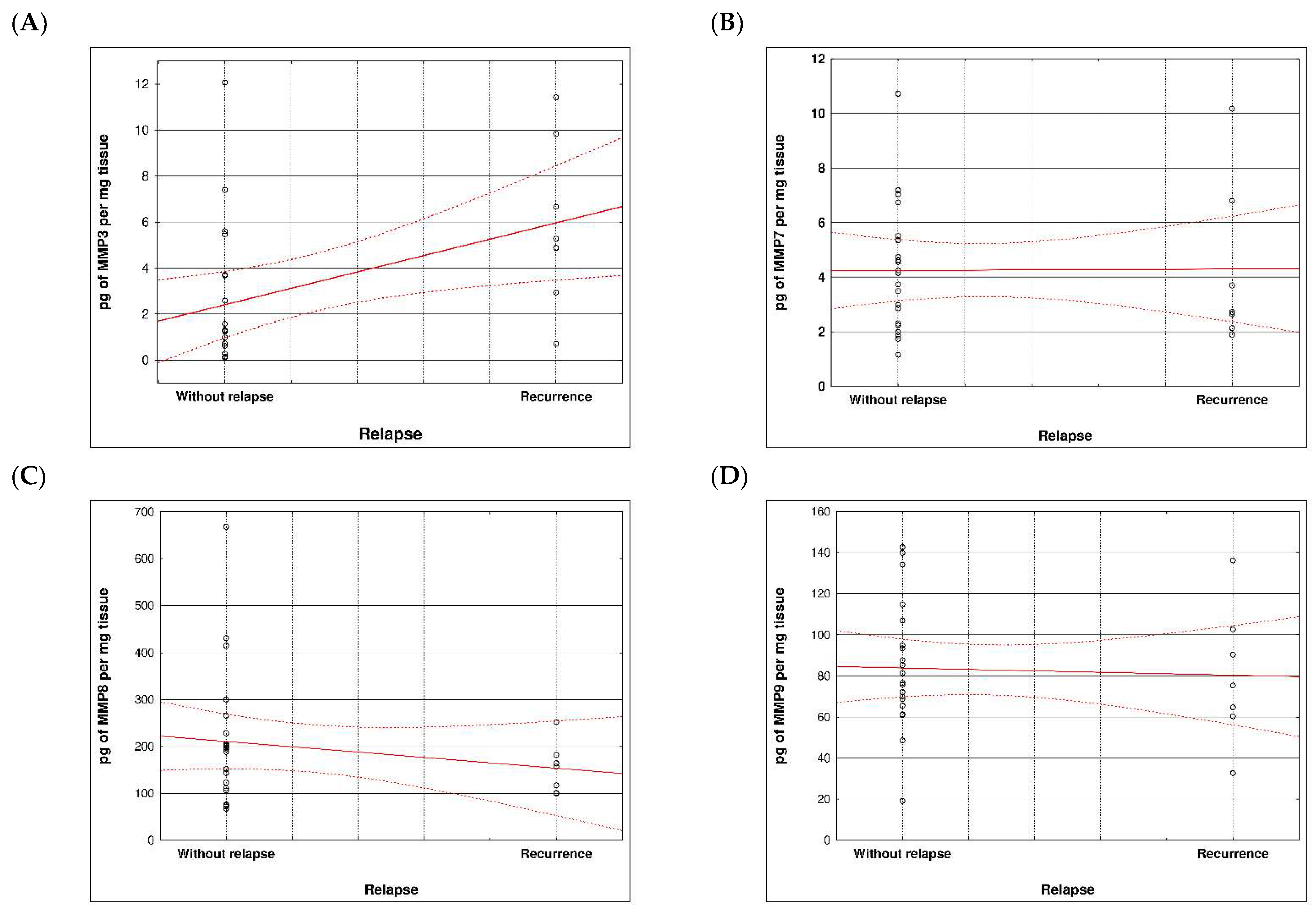
| MMP 3 | 0.087 | 0.022 | 14.58 | 0.0002 |
| MMP 7 | 0.032 | 0.032 | 1.03 | 0.309 |
| MMP 8 | −0.002 | 0.001 | 6.04 | 0.014 |
| MMP 9 | 0.001 | 0.002 | 0.108 | 0.742 |
| Variables | AIC | Δ(AIC) | wt.(AIC) | k |
|---|---|---|---|---|
| MMP3 + MMP8 | 27.48 | 0.00 | 0.374 | 3 |
| MMP3 + MMP7 + MMP8 | 28.17 | 0.69 | 0.265 | 4 |
| MMP3 + MMP8 + MMP9 | 29.35 | 1.87 | 0.147 | 4 |
| MMP3 + MMP7 + MMP8 + MMP9 | 30.10 | 2.62 | 0.101 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrzanowski, G.; Pasternak, G.; Aebisher, D.; Dynarowicz, K.; Myśliwiec, A.; Bartusik-Aebisher, D.; Sosna, B.; Cieślar, G.; Kawczyk-Krupka, A.; Filip, R. An Analysis of the Content of Metalloproteinases in the Intestinal Wall of Patients with Crohn’s Disease. Life 2023, 13, 2013. https://doi.org/10.3390/life13102013
Chrzanowski G, Pasternak G, Aebisher D, Dynarowicz K, Myśliwiec A, Bartusik-Aebisher D, Sosna B, Cieślar G, Kawczyk-Krupka A, Filip R. An Analysis of the Content of Metalloproteinases in the Intestinal Wall of Patients with Crohn’s Disease. Life. 2023; 13(10):2013. https://doi.org/10.3390/life13102013
Chicago/Turabian StyleChrzanowski, Grzegorz, Grzegorz Pasternak, David Aebisher, Klaudia Dynarowicz, Angelika Myśliwiec, Dorota Bartusik-Aebisher, Barbara Sosna, Grzegorz Cieślar, Aleksandra Kawczyk-Krupka, and Rafał Filip. 2023. "An Analysis of the Content of Metalloproteinases in the Intestinal Wall of Patients with Crohn’s Disease" Life 13, no. 10: 2013. https://doi.org/10.3390/life13102013