


Assessment of Visual Quality Improvement as a Result of Spectacle Personalization
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Design
2.3. Study Devices
2.4. Personalized (3D Tailored) Spectacles
2.5. Control Standard Spectacles
2.6. Outcomes
2.7. Statistical Analysis
3. Results
3.1. Evaluation of Visual Functions and Reading Speed
3.2. First Impression Questionnaire
3.3. Subject Satisfaction Questionnaire
3.4. Final Comparison Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | 1. Age: - Single vision design (SV group): 18–44 years - Progressive addition lens design (PAL group): 45–65 years 2. The subjects should be experienced wearers wearing SV/PAL designs during the last six months. 3. Visual Acuity: distance and near monocular ≥ 1.0 (≤0.0 logMAR) 4. Normal binocular vision 5. Ametropia: - Spherical power: −6.00–+6.00 D - Cylindrical power: ≤ 2.50 D - Difference in power (spherical equivalent) between TE eyes: ≤ 2.00 D |
| Exclusion Criteria | 1. First prescription for progressive addition lenses 2. The prescription varies from the previous prescription by more than 0.75 D in the spherical equivalent or in the cylinder axis by more than 15° in any eye 3. Double vision or prismatic power in current glasses 4. Known ocular disease including strabismus, any pathology, and any eye surgeries that may affect visual acuity 5. The use of systemic or ocular medication that is likely to affect vision 6. Balance problems/vertigo problems 7. Concurrent participation in any other vision-related studies 8. Pregnancy 9. Inadequate fitting of control frames |
| Question |
|---|
| How comfortable are the new spectacles in general? (1–10) |
| How comfortable are the new spectacles on your nose? (1–10) |
| How do you find the spectacles’ bridge on your nose? |
| 1: There is a space between the bridge and my nose |
| 2: It presses on my nose |
| 3: It fits perfectly on my nose |
| How are the temples? (1–10) |
| How do you find the temples according to your head? |
| 1: They are too loose on my head |
| 2: They press on my head |
| 3: They fit perfectly according to my head |
| How is the length of the temples? |
| 1: Too long |
| 2: Too short |
| 3: The temple’s length is exactly what I need |
| How is your vision in general with the new spectacles? (1–10) |
| How do you find the field of view with the new spectacles in general? (1–10) |
| Do you notice any distortion of images or blurring? |
| 1: No, not at all |
| 2: Slightly |
| Do you experience any swaying feelings? |
| 1: No, not at all |
| 2: Slightly |
| OVERALL SCORE |
| Question |
|---|
| How comfortable is this pair of spectacles in general? (1–5) |
| How easily and quickly could you adapt to this pair of spectacles? (1–5) |
| Spectacles slide down from the nose (1–5) |
| Lenses steam up while wearing them (1–5) |
| How comfortable was this pair on your nose during the two weeks of wearing them? (1–5) |
| How comfortable were the temples during the two weeks of wearing this pair? (1–5) |
| How satisfied are you with your vision/visual acuity using this pair looking: |
| At far distances (>4–6 m: TV…)? (1–5) |
| At intermediate distances (≈60 cm–1 m: computer work) (1–5) |
| Doing your near work (≈30–50 cm: reading...) (1–5) |
| How satisfied are you with the visual field using this pair: |
| At far distances (>4–6 m: TV…)? (1–5) |
| At intermediate distances (≈60 cm -1 m: computer work) (1–5) |
| Doing your near work (≈30–50 cm: reading...) (1–5) |
| Did you experience any swaying feeling using this pair? (1–5) |
| How satisfied are you with this eyewear in general? (1–5) |
| OVERALL SCORE |
| Question |
|---|
| How comfortable are the spectacles in general? (1–5) |
| How easily and quickly could you adapt to them? (1–5) |
| How comfortable are the spectacles on your nose? (1–5) |
| How comfortable are the temples? (1–5) |
| How satisfied are you with your vision in general? (1–5) |
| How satisfied are you with the visual field? (1–5) |
| Did you experience a swaying feeling when wearing the glasses? (1–5) |
| Please rank the spectacles (1–5) |
| Which pair of spectacles would you like to keep? |
| OVERALL SCORE |
| SV Group (n = 30) | PAL Group (n = 30) | All spectacles (n = 60) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Question | Personalized | Control | p | Personalized | Control | p | Personalized | Control | p |
| How comfortable are new spectacles in general? (1–10) | 8.70 ± 1.23 | 7.46 ± 2.55 | 0.03 | 8.40 ± 1.59 | 8.43 ± 1.53 | 0.54 | 8.55 ± 1.42 | 7.95 ± 2.26 | 0.19 |
| How comfortable are the new spectacles on your nose? (1–10) | 8.23 ± 1.92 | 7.30 ± 2.84 | 0.20 | 8.50 ± 1.19 | 8.87 ± 1.04 | 0.14 | 8.37 ± 1.59 | 8.08 ± 2.26 | 0.94 |
| How do you find the spectacles’ bridge on your nose | |||||||||
| 1: There is a space between the bridge and my nose | 2 | 8 | 0.65 | 5 | 3 | 0.31 | 7 | 11 | 0.54 |
| 2: It presses on my nose | 5 | 3 | 1 | 4 | 6 | 7 | |||
| 3: It fits perfectly on my nose | 23 | 19 | 24 | 23 | 47 | 42 | |||
| How are the temples? (1–10) | 8.53 ± 1.66 | 8. 20 ± 2.19 | 0.58 | 8.83 ± 1.08 | 8.53 ± 1.33 | .27 | 8.68 ± 1.40 | 8.37 ± 1.80 | .31 |
| How do you find the temples according to your head? | |||||||||
| 1: They are too loose on my head | 8 | 9 | 0.96 | 6 | 9 | 0.33 | 14 | 18 | 0.38 |
| 2: They press on my head | 1 | 0 | 0 | 3 | 1 | 3 | |||
| 3: They fit perfectly according to my head | 21 | 21 | 24 | 18 | 45 | 39 | |||
| How is the length of the temples? | |||||||||
| 1: Too long | 7 | 11 | 0.52 | 4 | 6 | 0.69 | 11 | 17 | 0.29 |
| 2: Too short | 1 | 0 | 2 | 1 | 3 | 1 | |||
| 3: The temple’s length is exactly what I need | 22 | 19 | 24 | 23 | 46 | 42 | |||
| How is your vision in general with the new spectacles? (1–10) | 9.77 ± 0.43 | 9.37 ± 1.03 | 0.05 | 8.47 ± 1.33 | 7.90 ± 2.41 | 0.51 | 9.12 ± 1.18 | 8.63 ± 1.98 | 0.19 |
| How do you find the field of view with the new spectacles in general? (1–10) | 8. 40 ± 1.96 | 8.30 ± 1.66 | 0.59 | 8.70 ± 1.34 | 8.40 ± 1.92 | 0.52 | 8.55 ± 1.67 | 8.35 ± 1.78 | 0.34 |
| Do you notice any distortion of images or blurring? | |||||||||
| 1: No, not at all | 27 | 24 | 0.28 | 23 | 20 | 0.39 | 50 | 44 | 0.18 |
| 2: Slightly | 3 | 6 | 7 | 10 | 10 | 16 | |||
| Do you experience any swaying feelings? | |||||||||
| 1: No, not at all | 24 | 22 | 0.54 | 17 | 19 | 0.59 | 41 | 41 | 0.99 |
| 2: Slightly | 6 | 8 | 13 | 11 | 19 | 19 | |||
| OVERALL SCORE | 43.63 ± 4.73 | 40.63 ± 8.32 | 0.20 | 42.90 ± 4.37 | 42.13 ± 5.30 | 0.95 | 43.27 ± 4.52 | 41.38 ± 6.96 | 0.30 |
| SV Group (n = 30) | PAL Group (n = 30) | All spectacles (n = 60) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Question | Personalized | Control | p | Personalized | Control | p | Personalized | Control | p |
| How comfortable is this pair of spectacles in general? (1–5) | 4.13 ± 1.01 | 3.73 ± 1.26 | 0.17 | 4.13 ± 0.94 | 3.90 ± 1.06 | 0.32 | 4.13 ± 0.96 | 3.82 ± 1.16 | 0.09 |
| How easily and quickly could you adapt to this pair of spectacles? (1–5) | 4.13 ± 1.01 | 4.0 ± 1.44 | 0.76 | 3.80 ± 1.16 | 3.63 ± 1.43 | 0.59 | 3.97 ± 1.09 | 3.82 ± 1.43 | 0.55 |
| Spectacles slide down from the nose (1–5) | 3.57 ± 1.22 | 3.33 ± 1.40 | 0.51 | 3.80 ± 1.27 | 3.93 ± 1.23 | 0.56 | 3.68 ± 1.24 | 3.63 ± 1.34 | 0.89 |
| Lenses steam up while wearing them (1–5) | 4.33 ± 1.03 | 4.20 ± 1.09 | 0.58 | 4.23 ± 0.90 | 4.53 ± 0.63 | 0.06 | 4.28 ± 0.96 | 4.37 ± 0.90 | 0.51 |
| How comfortable was this pair on your nose during the two weeks of wearing them? (1–5) | 3.70 ± 1.26 | 3.53 ± 1.55 | 0.61 | 4.23 ± 0.77 | 4.07 ± 1.05 | 0.33 | 3.97 ± 1.07 | 3.80 ± 1.34 | 0.34 |
| How comfortable were the temples during the two weeks of wearing this pair? (1–5) | 4.30 ± 1.02 | 3.77 ± 1.48 | 0.19 | 3.99 ± 0.99 | 4.17 ± 0.95 | 0.38 | 4.13 ± 1.02 | 3.97 ± 1.25 | 0.46 |
| How satisfied are you with your vision/visual acuity using this pair looking: | |||||||||
| At far distances (>4–6 m: TV…)? (1–5) | 4. 87 ± 0.34 | 4.70 ± 0.70 | 0.29 | 4.43 ± 0.86 | 3.80 ± 1.21 | 0.02 | 4.65 ± 0.68 | 4.25 ± 1.08 | 0.01 |
| At intermediate distances (≈60 cm–1 m: computer work) (1–5) | 4.83 ± 0.38 | 4.73 ± 0.58 | 0.40 | 4.03 ± 1.22 | 3.97 ± 1.25 | 0.96 | 4.43 ± 0.98 | 4.35 ± 1.04 | 0.77 |
| Doing your near work (≈30–50 cm: reading...) (1–5) | 4.77 ± 0.73 | 4.67 ± 0.61 | 0.35 | 4.20 ± 1.21 | 3.60 ± 1.35 | 0.02 | 4.48 ± 0.95 | 4.13 ± 1.17 | 0.01 |
| How satisfied are you with the visual field using this pair: | |||||||||
| At far distances (>4–6 m: TV…)? (1–5) | 4.03 ± 1.07 | 4.27 ± 1.17 | 0.16 | 4.37 ± 0.99 | 4.00 ± 1.20 | 0.10 | 4.20 ± 1.04 | 4.13 ± 1.17 | 0.94 |
| At intermediate distances (≈60 cm–1 m: computer work) (1–5) | 4.27 ± 0.91 | 4.47 ± 0.97 | 0.19 | 4.20 ± 1.06 | 4.07 ± 1.20 | 0.38 | 4.23 ± 0.98 | 4.27 ± 1.10 | 0.75 |
| Doing your near work (≈30–50 cm: reading...) (1–5) | 4.57 ± 0.73 | 4.57 ± 0.94 | 0.72 | 4.27 ± 0.94 | 4.00 ± 1.26 | 0.19 | 4.42 ± 0.85 | 4.28 ± 1.14 | 0.41 |
| Did you experience any swaying feeling when using this pair? (1–5) | 4. 50 ± 0.73 | 4.20 ± 1.18 | 0.19 | 4.30 ± 1.09 | 3.80 ± 1.15 | 0.03 | 4.40 ± 0.92 | 4.00 ± 1.18 | 0.02 |
| How satisfied are you with this eyewear in general? (1–5) | 4.10 ± 0.96 | 3.77 ± 1.22 | 0.25 | 4.17 ± 0.87 | 3.70 ± 1.09 | 0.04 | 4.13 ± 0.91 | 3.73 ± 1.15 | 0.03 |
| OVERALL SCORE | 60.10 ± 7.30 | 57.93 ± 10.50 | 0.48 | 58.13 ± 9.25 | 55.17 ± 11.18 | 0.21 | 59.12 ± 8.32 | 56.55 ± 10.87 | 0.18 |
References
- Sheppard, A.L.; Wolffsohn, J.S. Digital eye strain: Prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018, 3, e000146. [Google Scholar] [CrossRef] [Green Version]
- Wolffsohn, J.S.; Davies, L.N. Presbyopia: Effectiveness of correction strategies. Prog. Retin. Eye Res. 2019, 68, 124–143. [Google Scholar] [CrossRef] [Green Version]
- Jaschinski, W.; König, M.; Mekontso, T.M.; Ohlendorf, A.; Welscher, M. Comparison of progressive addition lenses for general purpose and for computer vision: An office field study. Clin. Exp. Optom. 2015, 98, 234–243. [Google Scholar] [CrossRef] [PubMed]
- De Lestrange-Anginieur, E.; Kee, C.S. Optical performance of progressive addition lenses (PALs) with astigmatic prescription. Sci. Rep. 2021, 11, 2984. [Google Scholar] [CrossRef] [PubMed]
- Kee, C.-S.; Leung, T.W.; Kan, K.-H.B.; Lam, C.H.-I.B. Effects of Progressive Addition Lens Wear on Digital Work in Pre-presbyopes. Optom. Vis. Sci. 2018, 95, 457–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meister, D.J.; Fisher, S.W. Progress in the spectacle correction of presbyopia. Part 1: Design and development of progressive lenses. Clin. Exp. Optom. 2008, 91, 240–250. [Google Scholar] [CrossRef]
- Meister, D.J.; Fisher, S.W. Progress in the spectacle correction of presbyopia. Part 2: Modern progressive lens technologies. Clin. Exp. Optom. 2008, 91, 251–264. [Google Scholar] [CrossRef]
- Sheedy, J.E. Progressive addition lenses—Matching the specific lens to patient needs. Optom. J. Am. Optom. Assoc. 2004, 75, 83–102. [Google Scholar] [CrossRef]
- Han, Y.; Ciuffreda, K.J.; Selenow, A.; Ali, S.R. Dynamic interactions of eye and head movements when reading with single-vision and progressive lenses in a simulated computer-based environment. Investig. Opthalmology Vis. Sci. 2003, 44, 1534–1545. [Google Scholar] [CrossRef] [Green Version]
- Legras, R.; Vincent, M.; Marin, G. Does visual acuity predict visual preference in progressive addition lenses? J. Optom. 2023, 16, 91–99. [Google Scholar] [CrossRef]
- Sullivan, C.M.; Fowler, C.W. Investigation of progressive addition lens patient tolerance to dispensing anomalies. Ophthalmic Physiol. Opt. 1990, 10, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Sheedy, J.; Hardy, R.F.; Hayes, J.R. Progressive addition lenses—Measurements and ratings. Optom. J. Am. Optom. Assoc. 2006, 77, 23–39. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Raasch, T.W.; Yi, A.Y.; Bullimore, M.A. Comparison of Progressive Addition Lenses by Direct Measurement of Surface Shape. Optom. Vis. Sci. 2013, 90, 565–575. [Google Scholar] [CrossRef]
- Barbero, S.; Portilla, J. The relationship between dioptric power and magnification in progressive addition lenses. Ophthalmic Physiol. Opt. 2016, 36, 421–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rifai, K.; Wahl, S. Specific eye–head coordination enhances vision in progressive lens wearers. J. Vis. 2006, 16, 5. [Google Scholar] [CrossRef] [Green Version]
- Hutchings, N.; Irving, E.L.; Jung, N.; Dowling, L.M.; Wells, K.A. Eye and head movement alterations in naïve progressive addition lens wearers. Ophthalmic Physiol. Opt. 2007, 27, 142–153. [Google Scholar] [CrossRef]
- Alvarez, T.L.; Kim, E.H.; Granger-Donetti, B. Adaptation to Progressive Additive Lenses: Potential Factors to Consider. Sci. Rep. 2017, 7, 2529. [Google Scholar] [CrossRef] [Green Version]
- Pascual, E.; Gómez-Pedrero, J.A.; Alonso, J. Theoretical performance of progressive addition lenses with poorly measured individual parameters. Ophthalmic Physiol. Opt. 2023, 43, 244–253. [Google Scholar] [CrossRef]
- Han, S.C.; Graham, A.D.; Lin, M.C. Clinical Assessment of a Customized Free-Form Progressive Add Lens Spectacle. Optom. Vis. Sci. 2011, 88, 234–243. [Google Scholar] [CrossRef] [Green Version]
- Hoya Corporation. White Paper Hoyalux iD MyStyle V+ 2014, 01. Available online: https://www.hoyavision.com/contentassets/cd44fd98c9fb469497d6621fe1db16d9/id-mystyle2-whitepaper_full-version_10_21_20.pdf/ (accessed on 5 August 2023).
- Radner, W.; Obermayer, W.; Richter-Mueksch, S.; Willinger, U.; Velikay-Parel, M.; Eisenwort, B. The validity and reliability of short German sentences for measuring reading speed. Graefe’s Arch. Clin. Exp. Ophthalmol. 2002, 240, 461–467. [Google Scholar] [CrossRef]
- Stifter, E.; König, F.; Lang, T.; Bauer, P.; Richter-Müksch, S.; Velikay-Parel, M.; Radner, W. Reliability of a standardized reading chart system: Variance component analysis, test-retest and inter-chart reliability. Graefe’s Arch. Clin. Exp. Ophthalmol. 2004, 242, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Selenow, A.; Bauer, E.A.; Ali, S.R.; Spencer, L.W.; Ciuffreda, K.J. Assessing Visual Performance with Progressive Addition Lenses. Optom. Vis. Sci. 2002, 79, 502–505. [Google Scholar] [CrossRef]
- Sánchez-Brau, M.; Domenech-Amigot, B.; Brocal-Fernández, F.; Quesada-Rico, J.A.; Seguí-Crespo, M. Prevalence of Computer Vision Syndrome and Its Relationship with Ergonomic and Individual Factors in Presbyopic VDT Workers Using Progressive Addition Lenses. Int. J. Environ. Res. Public Health 2020, 17, 1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Espinilla, O.; Gallegos-Cocho, I.; Sanchez, I.; Cañadas, P.; Martin, R. Comparison of physiognomy and frame angle parameters using different devices to prescribe progressive addition lenses. Clin. Exp. Optom. 2022, 105, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Espinilla, O.; Gallegos-Cocho, I.; Sanchez, I.; Cañadas, P.; Martin, R. Interdevice agreement in the measurement of physiognomy parameters and frame angles to prescribe progressive addition lenses. Clin. Exp. Optom. 2023, 106, 69–74. [Google Scholar] [CrossRef]
- Fontaine, N.O.; Hanssens, J.-M.O.; Nguyen, M.; Bérubé, O. Ordering Eyeglasses Using 3D Head Scan Technology versus Established Online and Storefront Clinic Methods. Optom. Vis. Sci. 2023, 100, 319–327. [Google Scholar] [CrossRef]
- Alionte, C.G.; Ungureanu, L.M.; Alexandru, T.M. Innovation Process for Optical Face Scanner Used to Customize 3D Printed Spectacles. Materials 2022, 15, 3496. [Google Scholar] [CrossRef]
- Campomanes, A.G.d.A.; Meer, E.; Clarke, M.; Brodie, F.L. Using a Smartphone 3-Dimensional Surface Imaging Technique to Manufacture Custom 3-Dimensional–Printed Eyeglasses. JAMA Ophthalmol 2022, 140, 966–973. [Google Scholar] [CrossRef]
- Lee, L.; Burnett, A.M.; Panos, J.G.; Paudel, P.; Keys, D.; Ansari, H.M.; Yu, M. 3-D printed spectacles: Potential, challenges and the future. Clin. Exp. Optom. 2020, 103, 590–596. [Google Scholar] [CrossRef]





| Criteria | Personalized Spectacles | Control Spectacles |
|---|---|---|
| Manufacturing | Personalized frame, produced on demand for each subject | Pre-produced frame based on standard parameters in one fixed size |
| Measurement and adjustment to the subject’s face topography | Face scan and 3D rendering of the subject’s face Calculation of the ideal lens parameter/position based on prescription, functional requirements, and facial data | Manual adjustment of the frame to the subject’s face The video-centration system visuReal portable is used to measure all frame-related wearing parameters |
| Definition of frame size and position | The parametric frame model is adjusted to the calculated lens position and face topography | Selection of a frame that fits as best as possible |
| Lens design | Ideal lens-related parameters are considered | Individual frame-wearing parameters are converted into lens-related parameters |
| Lens Designs | |||||||
|---|---|---|---|---|---|---|---|
| PAL | SV | ||||||
| Personalized | Control | Standard | Personalized | Control | Standard | ||
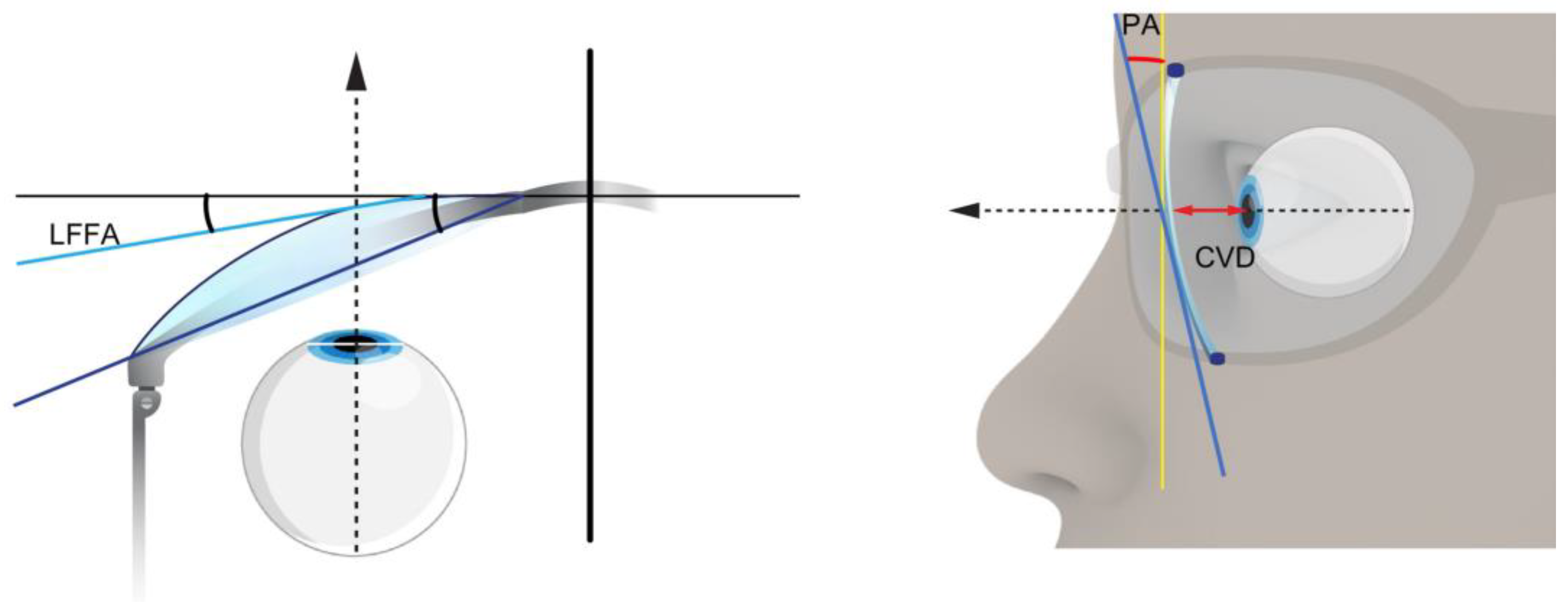
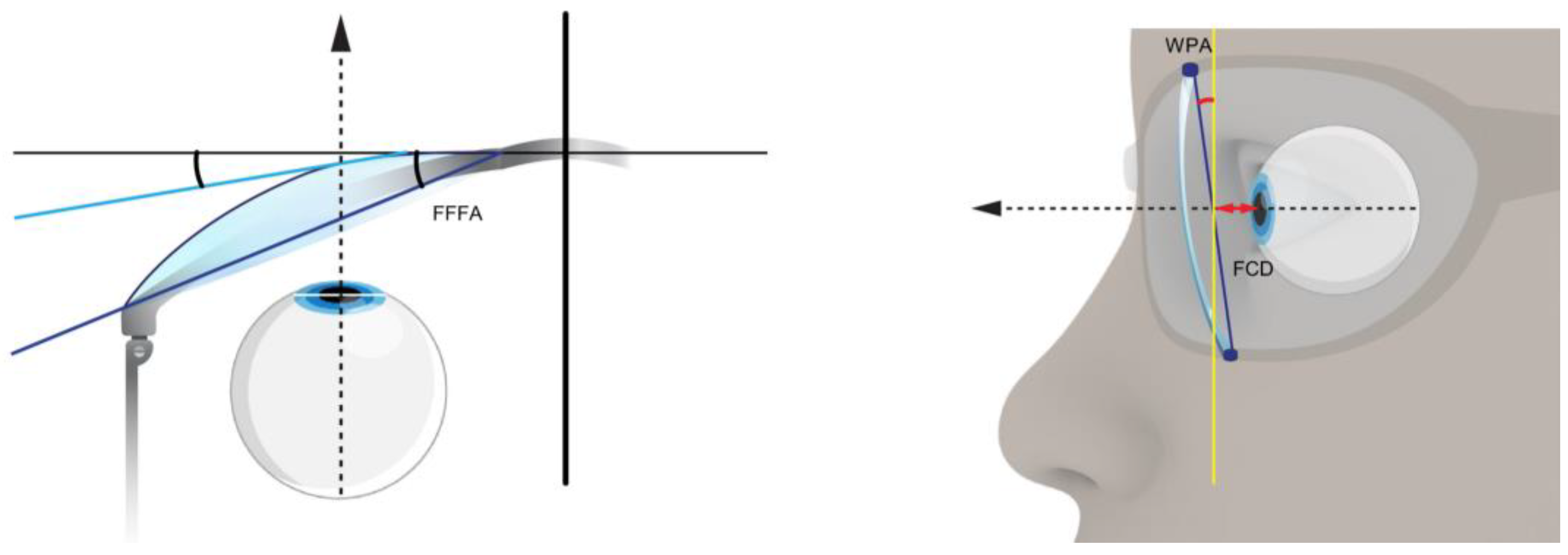
| Vertex Distance [mm] | CVD | 13.82 ± 2.51 | 13.76 ± 3.11 | ||||
| FCD | 16.25 ± 3.77 | 12.30 | 14.91 ± 3.07 | 12.30 | |||
| Pantoscopic Angle [°] | PA | 8.75 ± 2.38 | 4.04 ± 2.78 | ||||
| WPA | 8.62 ± 4.27 | 8.30 | 8.83 ± 2.87 | 8.30 | |||
| Face Form Angle [°] | LFFA | 1.14 ± 0.45 | 1.24 ± 0.24 | ||||
| FFFA | 1.75 ± 1.40 | 4.40 | 1.31 ± 0.71 | 4.40 | |||
| Question | SV Group (n = 30) | PAL Group (n = 30) | All spectacles (n = 60) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Personalized | Control | p | Personalized | Control | p | Personalized | Control | p | |
| How comfortable are the spectacles in general? (1–5) | 4.03 ± 0.93 | 3.67 ± 1.37 | 0.30 | 4.30 ± 0.92 | 4.03 ± 0.81 | 0.11 | 4.17 ± 0.92 | 3.85 ± 1.13 | 0.13 |
| How easily and quickly could you adapt to them? (1–5) | 3.87 ± 1.14 | 3.97 ± 1.40 | 0.71 | 4.07 ± 1.01 | 3.80 ± 1.21 | 0.33 | 3.97 ± 1.07 | 3.88 ± 1.30 | 0.86 |
| How comfortable are the spectacles on your nose? (1–5) | 3.77 ± 1.25 | 3.47 ± 1.43 | 0.44 | 4.17 ± 1.05 | 4.10 ± 0.96 | 0.34 | 3.97 ± 1.16 | 3.78 ± 1.25 | 0.37 |
| How comfortable are the temples? (1–5) | 4.30 ± 1.09 | 3.73 ± 1.44 | 0.11 | 4.27 ± 0.79 | 4.17 ± 0.79 | 0.35 | 4.28 ± 0.94 | 3.95 ± 1.17 | 0.10 |
| How satisfied are you with your vision in general? (1–5) | 4.77 ± 0.50 | 4.50 ± 0.97 | 0.19 | 4.37 ± 0.89 | 4.17 ± 1.18 | 0.36 | 4.57 ± 0.74 | 4.33 ± 1.08 | 0.15 |
| How satisfied are you with the visual field? (1–5) | 4.47 ± 0.68 | 4.33 ± 1.06 | 0.59 | 4.30 ± 0.99 | 4.13 ± 1.04 | 0.37 | 4.38 ± 0.85 | 4.23 ± 1.05 | 0.28 |
| Did you experience a swaying feeling when wearing the glasses? (1–5) | 4.40 ± 0.93 | 4.23 ± 1.17 | 0.46 | 4.27 ± 1.01 | 3.87 ± 1.20 | 0.38 | 4.33 ± 0.97 | 4.05 ± 1.18 | 0.06 |
| Please rank the spectacles (1–5) | 8.00 ± 1.76 | 7.27 ± 2.72 | 0.44 | 7.97 ± 1.81 | 7.40 ± 2.46 | 0.39 | 7.98 ± 1.80 | 7.33 ± 2.57 | 0.18 |
| Which pair of spectacles would you like to keep? | 17 | 13 | 0.29 | 20 | 10 | 0.40 | 37 | 23 | 0.04 |
| OVERALL SCORE | 37.6 ± 6.17 | 35.17 ± 9.79 | 0.52 | 37.73 ± 6.09 | 35.57 ± 7.55 | 0.41 | 37.67 ± 6.08 | 35.37 ± 8.67 | 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benyó, F.; István, L.; Kiss, H.; Gyenes, A.; Erdei, G.; Juhász, É.; Vlasak, N.; Unger, C.; Andorfi, T.; Réz, K.; et al. Assessment of Visual Quality Improvement as a Result of Spectacle Personalization. Life 2023, 13, 1707. https://doi.org/10.3390/life13081707
Benyó F, István L, Kiss H, Gyenes A, Erdei G, Juhász É, Vlasak N, Unger C, Andorfi T, Réz K, et al. Assessment of Visual Quality Improvement as a Result of Spectacle Personalization. Life. 2023; 13(8):1707. https://doi.org/10.3390/life13081707
Chicago/Turabian StyleBenyó, Fruzsina, Lilla István, Huba Kiss, Andrea Gyenes, Gábor Erdei, Éva Juhász, Natalia Vlasak, Claudia Unger, Tamás Andorfi, Kata Réz, and et al. 2023. "Assessment of Visual Quality Improvement as a Result of Spectacle Personalization" Life 13, no. 8: 1707. https://doi.org/10.3390/life13081707