
Association of Genetic and Allelic Variants of Von Willebrand Factor (VWF), Glutathione S-Transferase and Tumor Necrosis Factor Alpha with Ischemic Stroke Susceptibility and Progression in the Saudi Population
 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Methodology
2.1. Study Population
2.2. Inclusion and Exclusion Criteria for Stroke
2.3. Inclusion and Exclusion Criteria for Healthy Controls
2.4. Specimen and Data Collection from the Stroke Patients
2.5. Genomic DNA Extraction from Stroke Patients and Healthy Controls
2.6. Amplification Refractory Mutation System PCR of TNF-α rs1800629 G > A Genotyping
Gel Electrophoresis and PCR Product Visualization
2.7. Multiplex PCR for GSTT1 and GSTM1 (rs4025935 and rs71748309) Genotyping
Gel Electrophoresis and PCR Product Visualization
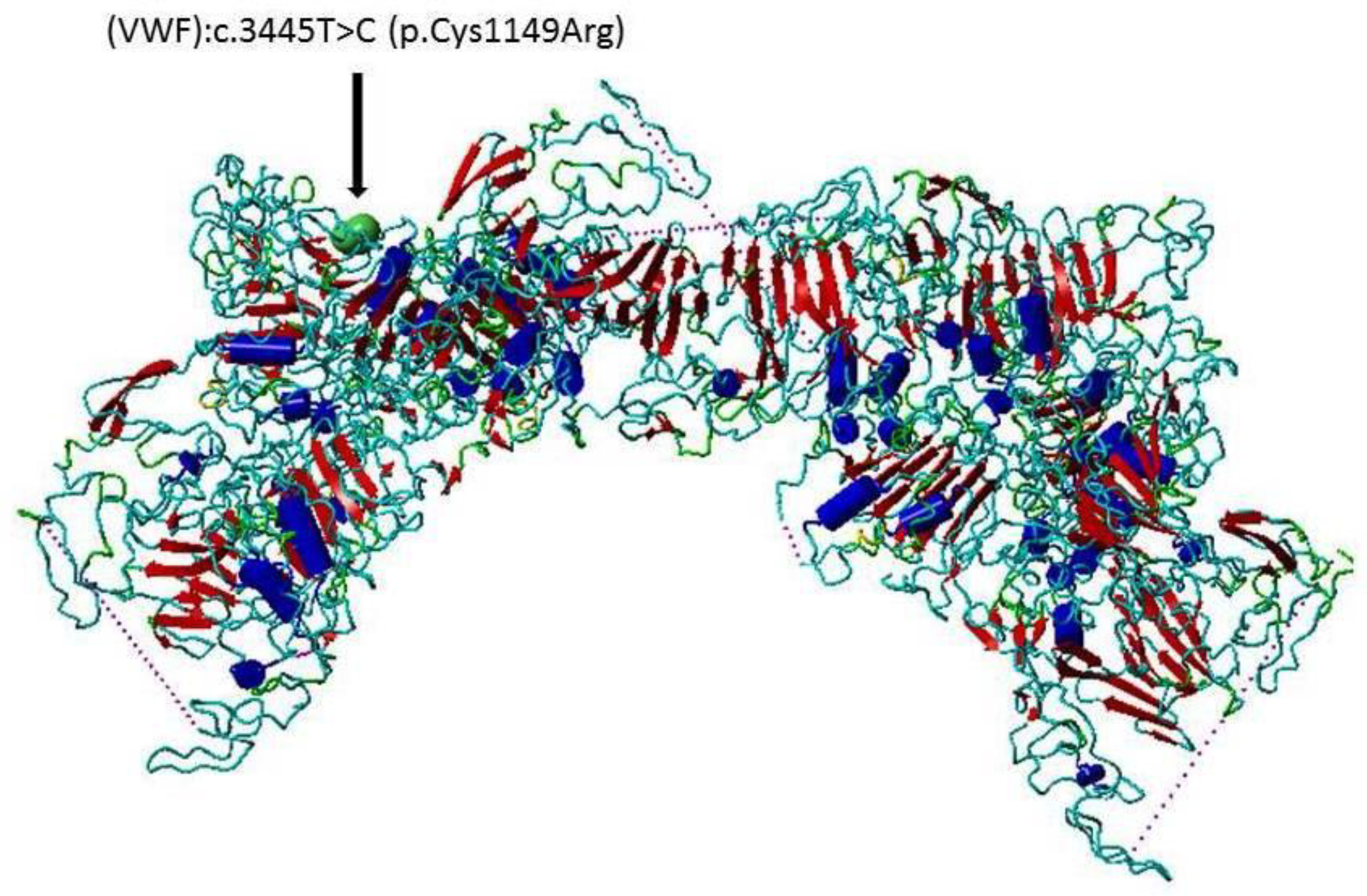
2.8. Allele-Specific PCR Primers for VWF rs 61748511T > C (VWD c.3445T > C)
2.9. Statistical Analysis
3. Results
3.1. Demographic Features of Stroke Patients
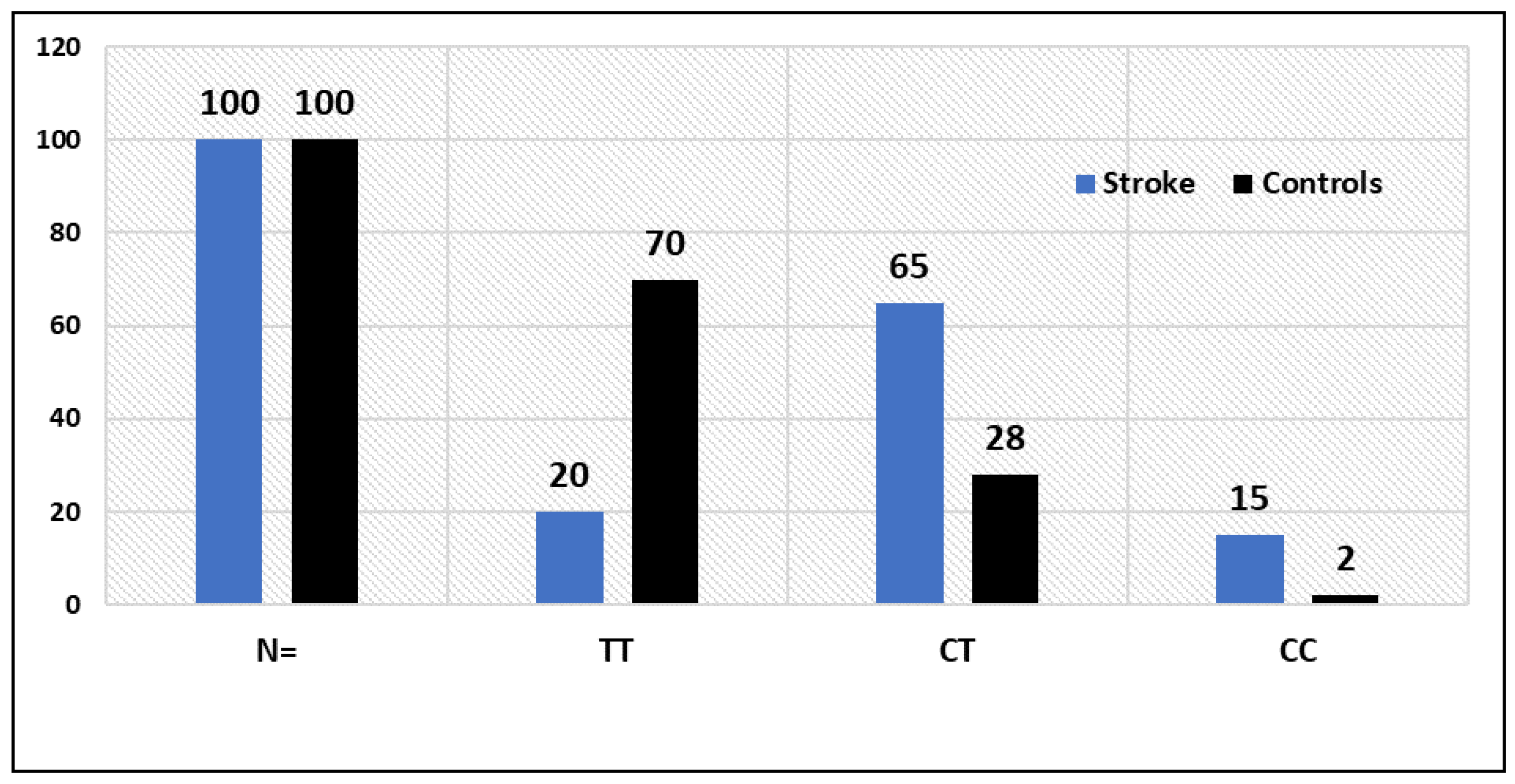
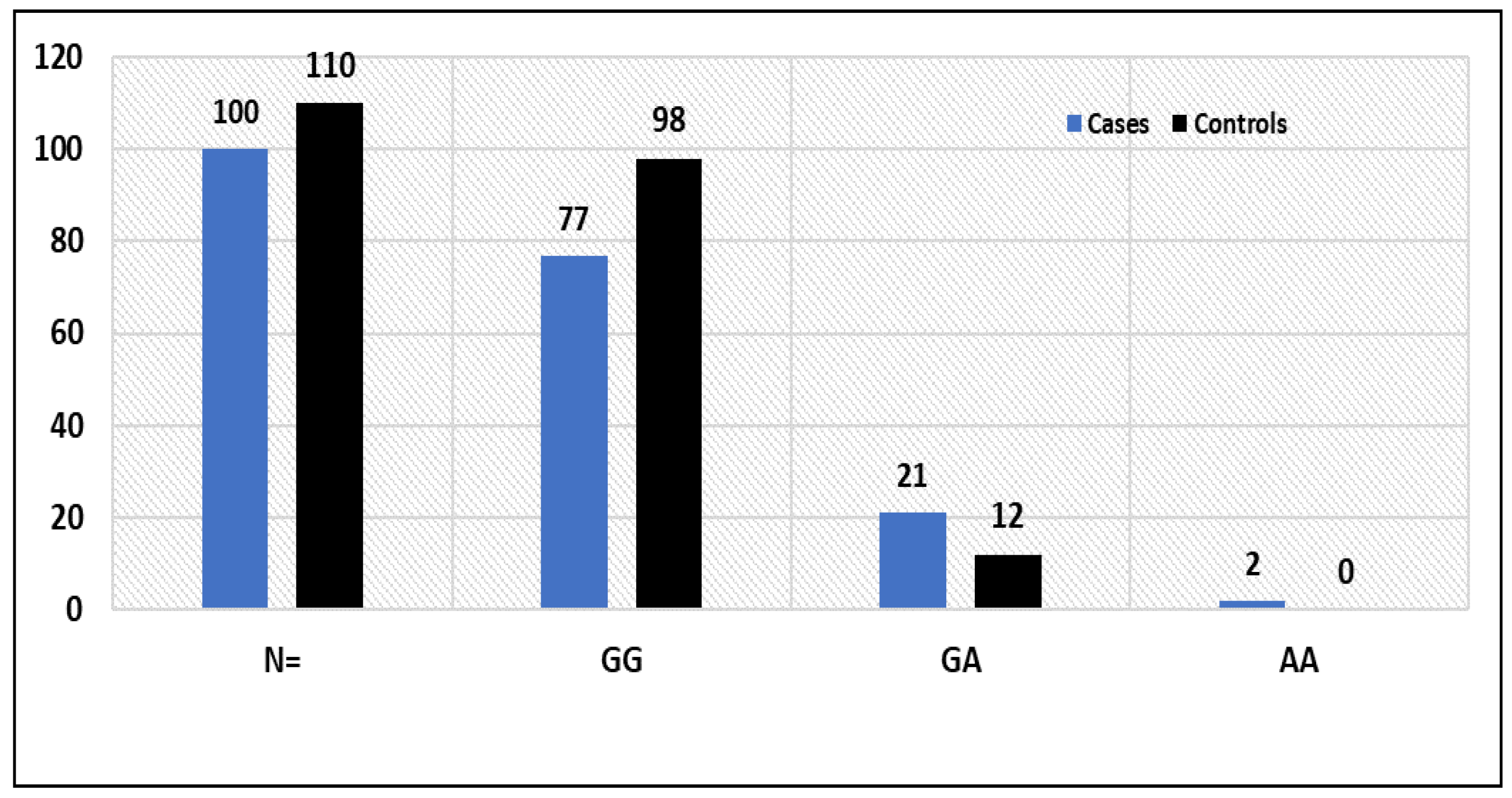
3.2. Statistical Comparisons between Stroke Patients and Controls (p-Values) for VWF rs61748511 T > C (c.3445T > C, p.Cys1149Arg): TNF-α rs1800629 G > A genotypes
3.3. Potential Association of the TNF-Alpha rs1800629 SNP G > A Genotypes with Risk to Stroke
3.4. Potential Association of GSTT1 (+) and GSTT1(−) Genotypes with the Susceptibility to Stroke
3.5. Association of VWD rs61748511 T/C Genotypes with the Clinical Features of Stroke Patients
3.6. Association of TNF-α rs1800629 G > A Genotypes with the Clinical Features of Stroke Patients
4. Discussion
4.1. Von Willebrand Factor (VWF) VWF rs61748511 in STROKE
4.2. Glutathione-S-Transferases (GSTs) in Stroke
4.3. Tumor Necrosis Factor Alpha (TNF-Alpha) rs1800629 G > A in Stroke
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An Updated Definition of Stroke for the 21st Century: A Statement for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef]
- Amarenco, P.; Bogousslavsky, J.; Caplan, L.R.; Donnan, G.A.; Hennerici, M.G. Classification of Stroke Subtypes. Cerebrovasc. Dis. 2009, 27, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.J.; Werring, D.J. Stroke: Causes and Clinical Features. Medicine 2020, 48, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Dash, D.; Bhashin, A.; Pandit, A.K.; Tripathi, M.; Bhatia, R.; Prasad, K.; Padma, M.V. Risk Factors and Etiologies of Ischemic Strokes in Young Patients: A Tertiary Hospital Study in North India. J. Stroke 2014, 16, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Ovbiagele, B.; Nguyen-Huynh, M.N. Stroke Epidemiology: Advancing Our Understanding of Disease Mechanism and Therapy. Neurotherapeutics 2011, 8, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Donkor, E.S. Stroke in the 21(St) Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar]
- Boehme, A.K.; Esenwa, C.; Elkind, A.M.S. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- Chugh, C. Acute Ischemic Stroke: Management Approach. Indian J. Crit. Care Med. 2019, 23 (Suppl. S2), S140–S146. [Google Scholar]
- Denorme, F.; Vanhoorelbeke, K.; De Meyer, S.F. Von Willebrand Factor and Platelet Glycoprotein Ib: A Thromboinflammatory Axis in Stroke. Front. Immunol. 2019, 10, 2884. [Google Scholar] [CrossRef]
- Peyvandi, F.; Garagiola, I.; Baronciani, A.L. Role of Von Willebrand Factor in the Haemostasis. Blood Transfus. 2011, 9 (Suppl. S2), S3–S8. [Google Scholar]
- Bharati, K.P.; Prashanth, U.R. Von Willebrand Disease: An Overview. Indian J. Pharm. Sci. 2011, 73, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Manderstedt, E.; Lind-Hallden, C.; Lethagen, S.; Hallden, C. Genetic Variation in the Von Willebrand Factor Gene in Swedish Von Willebrand Disease Patients. TH Open 2018, 2, E39–E48. [Google Scholar] [CrossRef] [PubMed]
- De Meyer, S.F.; Stoll, G.; Wagner, D.D.; Kleinschnitz, C. Von Willebrand Factor: An Emerging Target in Stroke Therapy. Stroke 2012, 43, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Buchtele, N.; Schwameis, M.; Gilbert, J.C.; Schorgenhofer, C.; Jilma, B. Targeting Von Willebrand Factor in Ischaemic Stroke: Focus on Clinical Evidence. Thromb. Haemost. 2018, 118, 959–978. [Google Scholar] [CrossRef]
- Harper, S.; Speicher, D.W. Purification of Proteins Fused to Glutathione S-Transferase. Methods Mol. Biol. 2011, 681, 259–280. [Google Scholar] [PubMed]
- Vona, R.; Pallotta, L.; Cappelletti, M.; Severi, C.; Matarrese, P. The Impact of Oxidative Stress in Human Pathology: Focus on Gastrointestinal Disorders. Antioxidants 2021, 10, 201. [Google Scholar] [CrossRef] [PubMed]
- Pahwa, S.; Sharma, R.; Singh, A.B. Role of Glutathione S-Transferase in Coronary Artery Disease Patients with and without Type 2 Diabetes Mellitus. J. Clin. Diagn. Res. 2017, 11, Bc05–Bc08. [Google Scholar] [PubMed]
- Hollman, A.L.; Tchounwou, P.B.; Huang, A.H.C. The Association between Gene-Environment Interactions and Diseases Involving the Human Gst Superfamily with Snp Variants. Int. J. Environ. Res. Public Health 2016, 13, 379. [Google Scholar] [CrossRef]
- Dasari, S.; Gonuguntla, S.; Ganjayi, M.S.; Bukke, S.; Sreenivasulu, B.; Meriga, B. Genetic Polymorphism of Glutathione S-Transferases: Relevance to Neurological Disorders. Pathophysiology 2018, 25, 285–292. [Google Scholar] [CrossRef]
- Popko, K.; Gorska, E.; Stelmaszczyk-Emmel, A.; Plywaczewski, R.; Stoklosa, A.; Gorecka, D.; Pyrzak, B.; Demkow, U. Proinflammatory Cytokines Il-6 and Tnf-Alpha and the Development of Inflammation in Obese Subjects. Eur. J. Med. Res. 2010, 15 (Suppl. S2), 120–122. [Google Scholar] [CrossRef]
- Xue, Y.; Zeng, X.; Tu, W.J.; Zhao, J. Tumor Necrosis Factor-Alpha: The Next Marker of Stroke. Dis. Markers 2022, 2022, 2395269. [Google Scholar] [CrossRef] [PubMed]
- Jang, D.I.; Lee, A.H.; Shin, H.Y.; Song, H.R.; Park, J.H.; Kang, T.B.; Lee, S.R.; Yang, S.H. The Role of Tumor Necrosis Factor Alpha (Tnf-Alpha) in Autoimmune Disease and Current Tnf-Alpha Inhibitors in Therapeutics. Int. J. Mol. Sci. 2021, 22, 2719. [Google Scholar] [CrossRef] [PubMed]
- Boesten, L.S.; Zadelaar, A.S.; van Nieuwkoop, A.; Gijbels, M.J.; de Winther, M.P.; Havekes, L.M.; van Vlijmen, B.J. Tumor Necrosis Factor-Alpha Promotes Atherosclerotic Lesion Progression in Apoe*3-Leiden Transgenic Mice. Cardiovasc. Res. 2005, 66, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Rolski, F.; Blyszczuk, P. Complexity of Tnf-Alpha Signaling in Heart Disease. J. Clin. Med. 2020, 9, 3267. [Google Scholar] [CrossRef]
- Matheson, M.C.; Ellis, J.A.; Raven, J.; Walters, E.H.; Abramson, M.J. Association of Il8, Cxcr2 and Tnf-Alpha Polymorphisms and Airway Disease. J. Hum. Genet. 2006, 51, 196–203. [Google Scholar] [CrossRef]
- Abu-Duhier, F.; Mir, R. Gstt1 (Rs4025935) Null Genotype Is Associated with Increased Risk of Sickle Cell Disease in the Populations of Tabuk-Northwestern Region of Saudi Arabia. Hematology 2017, 22, 172–177. [Google Scholar] [CrossRef]
- Arshad, N.; Nawaz, S.K.; Iqbal, R.; Arshad, M.; Musheer, F.; Naz, A.; Mushtaq, I.; Jaleel, S. Association between Genetic Polymorphism and Risk of Von Willebrand Disease in Pakistan. Biomed. Res. Int. 2017, 2017, 1070471. [Google Scholar] [CrossRef]
- Saini, V.; Guada, L.; Yavagal, A.D.R. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology 2021, 97 (Suppl. S2), S6–S16. [Google Scholar] [CrossRef]
- Robert, A.A.; Zamzami, M.M. Stroke in Saudi Arabia: A Review of the Recent Literature. Pan Afr. Med. J. 2014, 17, 14. [Google Scholar] [CrossRef]
- Bakraa, R.; Aldhaheri, R.; Barashid, M.; Benafeef, S.; Alzahrani, M.; Bajaba, R.; Alshehri, S.; Alshibani, M. Stroke Risk Factor Awareness among Populations in Saudi Arabia. Int. J. Gen. Med. 2021, 14, 4177–4182. [Google Scholar] [CrossRef]
- Liu, J.; Zhu, Y.; Wu, Y.; Liu, Y.; Teng, Z.; Hao, Y. Association of Carotid Atherosclerosis and Recurrent Cerebral Infarction in the Chinese Population: A Meta-Analysis. Neuropsychiatr. Dis. Treat. 2017, 13, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Elfaki, I.; Mir, R.; Mir, M.M.; AbuDuhier, F.M.; Babakr, A.T.; Barnawi, J. Potential Impact of Microrna Gene Polymorphisms in the Pathogenesis of Diabetes and Atherosclerotic Cardiovascular Disease. J. Pers. Med. 2019, 9, 51. [Google Scholar] [CrossRef] [PubMed]
- Elfaki, I.; Mir, R.; Almutairi, F.M.; Duhier, F.M.A. Cytochrome P450: Polymorphisms and Roles in Cancer, Diabetes and Atherosclerosis. Asian Pac. J. Cancer Prev. 2018, 19, 2057–2070. [Google Scholar]
- Cano-Gamez, E.; Trynka, G. From Gwas to Function: Using Functional Genomics to Identify the Mechanisms Underlying Complex Diseases. Front. Genet. 2020, 11, 424. [Google Scholar] [CrossRef] [PubMed]
- Jha, C.K.; Mir, R.; Elfaki, I.; Khullar, N.; Rehman, S.; Javid, J.; Banu, S.; Chahal, S.M.S. Potential Impact of Microrna-423 Gene Variability in Coronary Artery Disease. Endocr. Metab. Immune Disord. Drug. Targets 2019, 19, 67–74. [Google Scholar] [CrossRef]
- Doddapattar, P.; Dhanesha, N.; Chorawala, M.R.; Tinsman, C.; Jain, M.; Nayak, M.K.; Staber, J.M.; Chauhan, A.K. Endothelial Cell-Derived Von Willebrand Factor, but Not Platelet-Derived, Promotes Atherosclerosis in Apolipoprotein E-Deficient Mice. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 520–528. [Google Scholar] [CrossRef]
- Dmitrieva, N.I.; Burg, M.B. Secretion of Von Willebrand Factor by Endothelial Cells Links Sodium to Hypercoagulability and Thrombosis. Proc. Natl. Acad. Sci. USA 2014, 111, 6485–6490. [Google Scholar] [CrossRef]
- Spiel, A.O.; Gilbert, J.C.; Jilma, A.B. Von Willebrand Factor in Cardiovascular Disease: Focus on Acute Coronary Syndromes. Circulation 2008, 117, 1449–1459. [Google Scholar] [CrossRef]
- van Schie, M.C.; de Maat, M.P.; Isaacs, A.; van Duijn, C.M.; Deckers, J.W.; Dippel, D.W.; Leebeek, F.W. Variation in the Von Willebrand Factor Gene Is Associated with Von Willebrand Factor Levels and with the Risk for Cardiovascular Disease. Blood 2011, 117, 1393–1399. [Google Scholar] [CrossRef]
- Elfaki, I.; Bayer, P.; Mueller, A.J.W. A Potential Transcriptional Regulator Is Out-of-Frame Translated from the Metallothionein 2a Messenger Rna. Anal. Biochem. 2011, 409, 159–161. [Google Scholar] [CrossRef]
- Elfaki, I.; Knitsch, A.; Matena, A.; Bayer, P. Identification and Characterization of Peptides That Bind the Ppiase Domain of Parvulin17. J. Pept. Sci. Off. Publ. Eur. Pept. Soc. 2013, 19, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Reva, B.; Antipin, Y.; Sander, A.C. Predicting the Functional Impact of Protein Mutations: Application to Cancer Genomics. Nucleic Acids Res. 2011, 39, E118. [Google Scholar] [CrossRef] [PubMed]
- Vihinen, M. Functional Effects of Protein Variants. Biochimie 2021, 180, 104–120. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.R.; Reindl, K.M. Glutathione S-Transferases in Cancer. Antioxidants 2021, 10, 701. [Google Scholar] [CrossRef] [PubMed]
- Allocati, N.; Masulli, M.; Di Ilio, C.; Federici, L. Glutathione Transferases: Substrates, Inihibitors and Pro-Drugs in Cancer and Neurodegenerative Diseases. Oncogenesis 2018, 7, 8. [Google Scholar] [CrossRef] [PubMed]
- Ribas, V.; Garcia-Ruiz, C.; Fernandez-Checa, A.J.C. Glutathione and Mitochondria. Front. Pharmacol. 2014, 5, 151. [Google Scholar] [CrossRef]
- Adibhesami, G.; Shahsavari, G.R.; Amiri, A.; Emami Razavi, A.N.; Shamaei, M.; Birjandi, M. Glutathione S-Transferase M1 (Gstm1) and T1 (Gstt1) Polymorphisms and Lung Cancer Risk among a Select Group of Iranian People. Asian Pac. J. Cancer Prev. 2018, 19, 2921–2927. [Google Scholar]
- Pincinato, E.C.; Costa, E.F.D.; Lopes-Aguiar, L.; Nogueira, G.A.S.; Lima, T.R.P.; Visacri, M.B.; Costa, A.P.L.; Lourenco, G.J.; Calonga, L.; Mariano, F.V.; et al. Gstm1, Gstt1 and Gstp1 Ile105val Polymorphisms in Outcomes of Head and Neck Squamous Cell Carcinoma Patients Treated with Cisplatin Chemoradiation. Sci. Rep. 2019, 9, 9312. [Google Scholar] [CrossRef]
- Wang, R.; Wang, Y.; Wang, J.; Yang, K. Association of Glutathione S-Transferase T1 and M1 Gene Polymorphisms with Ischemic Stroke Risk in the Chinese Han Population. Neural Regen. Res. 2012, 7, 1420–1427. [Google Scholar] [PubMed]
- Bid, H.K.; Konwar, R.; Saxena, M.; Chaudhari, P.; Agrawal, C.G.; Banerjee, M. Association of Glutathione S-Transferase (Gstm1, T1 and P1) Gene Polymorphisms with Type 2 Diabetes Mellitus in North Indian Population. J. Postgrad. Med. 2010, 56, 176–181. [Google Scholar]
- Khanam, J.; Hossain, D.; Hosen, B.; Uddin, M.; Kabir, A.; Anwarul Bari, M. Association of Glutathione S-Transferase Theta 1 and Mu 1 Genes Polymorphisms with the Susceptibility of Myocardial Infarction in Bangladesh. Rep. Biochem. Mol. Biol. 2020, 9, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Mir, R.; Bhat, M.A.; Javaid, J.; Shah, N.; Kumar, P.; Sharma, E.; Jhu, C.; Basak, S.; Amle, D.; Ray, P.C.; et al. Glutathione S-Transferase M1 and T1 (Rs4025935 and Rs71748309) Null Genotypes Are Associated with Increased Susceptibility to Coronary Artery Disease in Indian Populations. Acta Cardiol. 2016, 71, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Polonikov, A.; Vialykh, E.; Vasil’eva, O.; Bulgakova, I.; Bushueva, O.; Illig, T.; Solodilova, M. Genetic Variation in Glutathione S-Transferase Genes and Risk of Nonfatal Cerebral Stroke in Patients Suffering from Essential Hypertension. J. Mol. Neurosci. 2012, 47, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Bokhari, F.A.; Shakoori, T.A.; Butt, A.; Ghafoor, F. Tnf-Alpha: A Risk Factor for Ischemic Stroke. J. Ayub Med. Coll. Abbottabad 2014, 26, 111–114. [Google Scholar]
- Bonetti, N.R.; Diaz-Canestro, C.; Liberale, L.; Crucet, M.; Akhmedov, A.; Merlini, M.; Reiner, M.F.; Gobbato, S.; Stivala, S.; Kollias, G.; et al. Tumour Necrosis Factor-Alpha Inhibition Improves Stroke Outcome in a Mouse Model of Rheumatoid Arthritis. Sci. Rep. 2019, 9, 2173. [Google Scholar] [CrossRef]
- Khan, S.; Mandal, R.K.; Jawed, A.; Dar, S.A.; Wahid, M.; Panda, A.K.; Areeshi, M.Y.; Ahmed Khan, M.E.; Haque, S. Tnf-Alpha -308 G > A (Rs1800629) Polymorphism Is Associated with Celiac Disease: A Meta-Analysis of 11 Case-Control Studies. Sci. Rep. 2016, 6, 32677. [Google Scholar] [CrossRef]
- Kamdee, K.; Panadsako, N.; Mueangson, O.; Nuinoon, M.; Janwan, P.; Poonsawat, W.; Pongpanitanont, P.; Kitkumthorn, N.; Thongsroy, J.; Chunglok, W. Promoter Polymorphism of Tnf-Alpha (Rs1800629) Is Associated with Ischemic Stroke Susceptibility in A Southern Thai Population. Biomed. Rep. 2021, 15, 78. [Google Scholar] [CrossRef]
- Marulanda-Londono, E.; Chaturvedi, S. Stroke Due to Large Vessel Atherosclerosis: Five New Things. Neurol. Clin. Pract. 2016, 6, 252–258. [Google Scholar] [CrossRef]
- Liu, Z.H.; Ding, Y.L.; Xiu, L.C.; Pan, H.Y.; Liang, Y.; Zhong, S.Q.; Liu, W.W.; Rao, S.Q.; Kong, D.L. A Meta-Analysis of the Association between Tnf-Alpha -308g>A Polymorphism and Type 2 Diabetes Mellitus in Han Chinese Population. PLoS ONE 2013, 8, e59421. [Google Scholar]
- Shi, L.X.; Zhang, L.; Zhang, D.L.; Zhou, J.P.; Jiang, X.J.; Jin, Y.L.; Chang, W.W. Association between Tnf-Alpha G-308a (Rs1800629) Polymorphism and Susceptibility to Chronic Periodontitis and Type 2 Diabetes Mellitus: A Meta-Analysis. J. Periodontal Res. 2021, 56, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Ghareeb, D.; Abdelazem, A.S.; Hussein, E.M.; Al-Karamany, A.S. Association of Tnf-Alpha-308 G > A (Rs1800629) Polymorphism with Susceptibility of Metabolic Syndrome. J. Diabetes Metab. Disord. 2021, 20, 209–215. [Google Scholar] [CrossRef]
- Plomgaard, P.; Bouzakri, K.; Krogh-Madsen, R.; Mittendorfer, B.; Zierath, J.R.; Pedersen, B.K. Tumor Necrosis Factor-Alpha Induces Skeletal Muscle Insulin Resistance in Healthy Human Subjects via Inhibition of Akt Substrate 160 Phosphorylation. Diabetes 2005, 54, 2939–2945. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G.; Ebrahim, A.S. Hdl-Cholesterol, Total Cholesterol, and the Risk of Stroke in Middle-Aged British Men. Stroke 2000, 31, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Reina, S.A.; Llabre, M.M.; Allison, M.A.; Wilkins, J.T.; Mendez, A.J.; Arnan, M.K.; Schneiderman, N.; Sacco, R.L.; Carnethon, M.; Delaney, J.A. Hdl Cholesterol and Stroke Risk: The Multi-Ethnic Study of Atherosclerosis. Atherosclerosis 2015, 243, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Carter, P.; Bruzelius, M.; Vithayathil, M.; Kar, S.; Mason, A.M.; Lin, A.; Burgess, S.; Larsson, S.C. Effects of Tumour Necrosis Factor on Cardiovascular Disease and Cancer: A Two-Sample Mendelian Randomization Study. Ebiomedicine 2020, 59, 102956. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, N.; Frick, A.; Kopp, A.J.B. Genetic Testing in Clinical Settings. Am. J. Kidney Dis. 2018, 72, 569–581. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline from the American Heart Association/American Stroke Association. Stroke 2021, 52, E364–E467. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Direction | Sequence | AT | PCR Product | Reference |
|---|---|---|---|---|
| ARMS-primers for TNF-α rs1800629 G > A genotyping | ||||
| TNF-alpha Fo | 5′-ACC CAA ACA CAG GCCTCAGGACTCAACA-3′ | 60 °C | 323 bp | [25] |
| TNF-alpha Ro | 5′-TGGA GGC AAT AGCTTTTGAGGGGCAGGA-3′ | |||
| TNF-alpha FI A | 5′-AGTTGGGGACACGCAAGCATGAAGGATA-3′ | 154 bp | ||
| TNF-alpha RIC | 5′-TAGGACCCTGGAGGCTAGACCCCGTACG-3′ | 224 bp | ||
| Multiplex PCR primers for GSTT1 and GSTM1 (rs4025935 and rs71748309) genotyping | ||||
| GSTT1 F | 5′-TTC CTT ACT GGT CCT CAC A TCTC-3′ | 60 °C | 480 bp | [26] |
| GSTT1 R | 5′-TCA CGG GAT CAT GGC CAGCA-3′ | |||
| GSTM1 F | 5′-GAA CTC CCT GAA AAGCTAAAGC-3′ | 215 bp | ||
| GSTM1 R | 5′-GTT GGG CTC AAA TAT ACG GTGG-3′ | |||
| CYP1A1F | 5′-GAA CTG CCA CTT CAG CT GTCT-3′ | 312 bp | ||
| CYP1A1R | 5′-CAG CTG CAT TTG GAA GTGCTC-3′ | |||
| Allele specific PCR primers for VWF rs 61748511T > C (VWD c.3445T > C) genotyping | ||||
| AS-PCR for T allele | [27] | |||
| F1-T | 5′-ACT TGA CAG GCAGGTGCACT-3′ | 55 °C | 213 bp | |
| C-R | 5′-ATT GGT GAC GCCCATAGTCC-3′ | |||
| AS-PCR for C allele | ||||
| F2-C | 5′-ACTT GAC AGG CAGGTGCACC-3′ | 55 °C | 213 bp | |
| C-R | 5′-ATTG GTG ACGCCCATAGTCC-3′ | |||
| Characteristic | Controls a | Patients | p b |
|---|---|---|---|
| Age | 33.50 ± 13.50 | 55.33 ± 8.12 | <0.001 |
| Blood sugar fasting | 97.70 ± 4.49 | 103.70 ± 4.50 | <0.001 |
| HbA1c | 5.50 ± 0.490 | 6.802 ± 0.390 | <0.001 |
| LDL | 116.13 ± 9.70 | 149.40 ± 32.18 | <0.001 |
| Cholesterol | 121.40 ± 7.40 | 169.32 ± 54.13 | <0.001 |
| VLDL | 26.91 ± 5.80 | 44.2 ± 12.7 | <0.001 |
| HDL | 47.31 ± 10.7 | 26.77 ± 4.22 | <0.001 |
| Triglyceride | 130.09 ± 8.50 | 175.8 ± 38.4 | <0.001 |
| Platelet count | 230.19 ± 78.7 | 252.15 ± 82.13 | 0.161 |
| Association of VWF rs61748511 T > C Genotypes between Stroke Patients and Controls | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Subjects | N= | TT | CT | CC | X2 | DF | T | C | p Value |
| Stroke | 100 | 20(20%) | 65(65%) | 15(15%) | 52.12 | 2 | 0.52 | 0.48 | 0.0001 |
| Controls | 100 | 70(70%) | 28(28%) | 2(2%) | 0.84 | 0.16 | |||
| Association of TNF-alpha rs1800629 G > A genotypes between stroke patients and controls | |||||||||
| Subjects | N= | GG | GA | AA | Df | X2 | G | A | p value |
| Cases | 100 | 77(77%) | 21(21%) | 02(2%) | 2 | 6.51 | 0.87 | 0.13 | 0.038 |
| Controls | 110 | 98(89%) | 12(10.90%) | 0(0%) | 0.95 | 0.5 | |||
| Genotypes | Healthy Controls N = 100 | Stroke Cases N = 100 | Odd Ratio OR (95% CI) | Risk Ratio RR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Codominant inheritance model | |||||
| VWF-TT | 70 | 20 | 1 (ref.) | 1 (ref.) | |
| VWF-TC | 28 | 65 | 8.12(4.1752 to 15.8113) | 2.58(1.859 to 3.588) | 0.0001 |
| VWF-CC | 02 | 15 | 26.1(5.5333 to 124.529) | 6.61(1.7900 to 24.417) | 0.0001 |
| Dominant inheritance model | |||||
| VWF-TT | 70 | 20 | 1 (ref.) | 1 (ref.) | |
| VWF-(TC + CC) | 30 | 80 | 9.3(4.8704 to 17.8857) | 2.85(2.0615 to 3.945) | 0.0001 |
| Recessive inheritance model | |||||
| VWF-(TC + TT) | 98 | 85 | 1 (ref.) | 1 (ref.) | |
| VWF-CC | 02 | 15 | 8.38(1.8626 to 37.7242) | 4.48(1.2115 to 16.612) | 0.005 |
| Allele | 1 (ref.) | 1 (ref.) | |||
| VWF-T | 168 | 105 | |||
| VWF-C | 32 | 95 | 4.7(2.9718 to 7.5922) | 2.44(1.7842 to 3.343) | 0.0001 |
| Over-dominant inheritance model | |||||
| VWF-(TT + CC) | 98 | 85 | 1 (ref.) | 1 (ref.) | |
| VWF-(TC) | 28 | 65 | 2.67(1.5757 to 4.5463) | 1.75(1.2488 to 2.460) | 0.0003 |
| Genotypes | Healthy Controls (N = 100) | Stroke Cases (N = 100) | Odd Ratio OR (95% CI) | Risk Ratio RR (95% CI) | p Value |
|---|---|---|---|---|---|
| Codominant inheritance model | |||||
| TNF-alpha-GG | 98 | 77 | 1 (ref.) | 1 (ref.) | |
| TNF-alpha-GA | 12 | 21 | 2.22(1.031 to 4.808) | 1.54(0.9624 to 2.464) | 0.041 |
| TNF-alpha-AA | 00 | 02 | 6.35(0.300 to 134.314) | 3.35(0.266 to 42.312) | 0.23 |
| Dominant inheritance model | |||||
| TNF-alpha-GG | 98 | 77 | 1 (ref.) | 1 (ref.) | |
| TNF-alpha (GA + AA) | 12 | 23 | 2.43(1.1418 to 5.2115) | 1.63(1.0136 to 2.6319) | 0.021 |
| Recessive inheritance model | |||||
| TNF-alpha -(GA + GG) | 110 | 98 | 1 (ref.) | 1(ref.) | |
| TNF-alpha-AA | 00 | 02 | 5.60(0.2660 to 118.266) | 3.17(0.2518 to 39.9659) | 0.260 |
| Allele | 1 (ref.) | 1 (ref.) | |||
| TNF-alpha-G | 208 | 175 | |||
| TNF-alpha-A | 12 | 25 | 2.47(1.2088 to 5.0724) | 1.67(1.0423 to 2.6901) | 0.013 |
| Over-dominant inheritance model | |||||
| TNF-alpha-(GG + AA) | 98 | 79 | 1 (ref.) | 1 (ref.) | |
| TNF-alpha (GA) | 12 | 21 | 2.17(1.0065 to 4.682) | 1.52(0.9513 to 2.437) | 0.048 |
| Variables | Controls (110) | Cases (100) | |||
|---|---|---|---|---|---|
| Genotype frequencies of GSTT1 in case and control groups | |||||
| GSTT1 (+) | 48(43.63%) | 10 (10%) | |||
| GSTT1 (−) | 52(47.27%) | 90 (90%) | |||
| Genotype frequencies of GSTM1 in case and control groups | |||||
| GSTM1(+) | 28(25.45%) | 33 (33%) | |||
| GSTM1(−) | 72(65.45%) | 77 (77%) | |||
| Genotype frequencies of GSTT1/GSTM1 in case and control groups | |||||
| GSTT1 (+) GSTM1 (+) | 24(21.81%) | 43(38.18%) | |||
| GSTT1 (−) GSTM1 (−) | 32(29.09%) | 33(30%) | |||
| GSTT1 (+) GSTM1 (−) | 24(21.81%) | 13(11.81%) | |||
| GSTT1 (−) GSTM1 (+) | 20(18.81%) | 11(10%) | |||
| Association of GSTM1/GSTT1 null genotypes with stroke risk | |||||
| Association of GSTT1 (+) and GSTT1 (−) genotypes with stroke risk | |||||
| Variables | 110 | 100 | OR (95% CI) | RR (95% CI) | p value |
| GSTT1 (+) | 48(48%) | 10 (10%) | Ref. 1.00 | Ref. 1.00 | |
| GSTT1 (−) | 52(52%) | 90 (90%) | 8.30(3.8772 to 17.801) | 2.25(1.7667 to 2.890) | 0.0001 |
| Association of GSTM1 (+) and GSTM1 (−) genotypes with stroke risk | |||||
| Variables | 110 | 100 | OR (95% CI) | RR (95% CI) | |
| GSTM1 (+) | 28(28%) | 33 (33%) | Ref. 1.00 | Ref. 1.00 | |
| GSTM1 (−) | 72(72%) | 77 (77%) | 0.90(0.4993 to 1.649) | 0.94(0.6904 to 1.306) | 0.74 |
| Association of GSTT1 (+) GSTM1 (+) and GSTT1 (−) GSTM1 (−) genotypes with stroke risk | |||||
| Variables | 110 | 100 | OR (95% CI) | RR (95% CI) | p value |
| GSTT1 (+) GSTM1 (+) | 24 | 43 | Ref. 1.00 | Ref. 1.00 | |
| GSTT1 (−) GSTM1 (−) | 32 | 33 | 0.57(0.2867 to 1.155) | 0.72(0.4855 to 1.090) | 0.120 |
| Association of GSTT1 (+) GSTM1 (−) and GSTT1 (−) GSTM1 (−) genotypes with stroke risk | |||||
| Variables | 110 | 100 | OR (95% CI) | RR (95% CI) | p value |
| GSTT1 (+) GSTM1 (−) | 24 | 13 | Ref. 1.00 | Ref. 1.00 | |
| GSTT1 (−) GSTM1 (+) | 20 | 11 | 1.01(0.3741 to 2.755) | 1.0(0.7066 to 1.430) | 0.97 |
| Clinical Feature | N = 100 | GG77 | GA21 | AA02 | X2 | DF | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Gender | Male | 62 | 49 | 12 | 01 | 0.42 | 2 | 0.81 |
| Female | 38 | 28 | 09 | 01 | ||||
| Age | Age < 50 | 20 | 17 | 01 | 02 | 11.26 | 2 | 0.003 |
| Age > 50 | 80 | 60 | 20 | 00 | ||||
| Fasting glucose mg/dL | <100 | 70 | 57 | 12 | 01 | 2.63 | 2 | 0.26 |
| >100 | 30 | 20 | 09 | 01 | ||||
| HbA1c % | >6 | 22 | 11 | 10 | 01 | 11.6 | 2 | 0.003 |
| <6 | 78 | 66 | 11 | 01 | ||||
| Triglycerides mg/dL | <200 | 70 | 56 | 13 | 01 | 1.31 | 2 | 0.51 |
| >200 | 30 | 28 | 08 | 01 | ||||
| Cholesterol mg/dL | <200 | 82 | 66 | 21 | 01 | 3.7 | 2 | 0.157 |
| >200 | 18 | 11 | 06 | 01 | ||||
| LDL-C mg/dL | <100 | 75 | 59 | 15 | 01 | 0.92 | 2 | 0.631 |
| >100 | 25 | 18 | 06 | 01 | ||||
| HDL-L mg/dL | <55 | 19 | 11 | 08 | 0 | 6.56 | 2 | 0.037 |
| >55 | 81 | 66 | 13 | 02 | ||||
| Association of VWD rs61748511 T/C genotypes with respected to clinical features of stroke | ||||||||
| Clinical feature | N | TT 20 | TC 65 | CC 15 | X2 | DF | p-value | |
| Gender | Male | 62 | 17 | 02 | 01 | 7.7 | 2 | 0.020 |
| Female | 38 | 60 | 20 | 00 | ||||
| Age | Age < 50 | 20 | 07 | 08 | 05 | 6.8 | 2 | 0.032 |
| Age > 50 | 80 | 13 | 57 | 10 | ||||
| Fasting glucose mg/dL | <100 | 70 | 09 | 55 | 06 | 18.9 | 2 | 0.0001 |
| >100 | 30 | 11 | 10 | 09 | ||||
| HbA1c % | >6 | 22 | 7 | 13 | 2 | 2.78 | 2 | 0.241 |
| <6 | 78 | 13 | 52 | 13 | ||||
| Triglycerides mg/dL | <200 | 69 | 14 | 45 | 10 | 0.05 | 2 | 0.97 |
| >200 | 31 | 06 | 20 | 05 | ||||
| Cholesterol mg/dL | <200 | 82 | 06 | 08 | 04 | 4.14 | 2 | 0.126 |
| >200 | 18 | 14 | 57 | 11 | ||||
| LDL-C mg/dL | <100 | 75 | 14 | 51 | 10 | 1.24 | 2 | 0.532 |
| >100 | 25 | 06 | 14 | 05 | ||||
| HDL-C mg/dL | <55 | 19 | 06 | 09 | 04 | 3.27 | 2 | 0.19 |
| >55 | 81 | 14 | 56 | 11 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jalal, M.M.; Mir, R.; Hamadi, A.; Altayar, M.A.; Elfaki, I.; Barnawi, J.; Alkayyal, A.A.; Amr, M.; Hadeel, J.; Moawadh, M.S.; et al. Association of Genetic and Allelic Variants of Von Willebrand Factor (VWF), Glutathione S-Transferase and Tumor Necrosis Factor Alpha with Ischemic Stroke Susceptibility and Progression in the Saudi Population. Life 2023, 13, 1200. https://doi.org/10.3390/life13051200
Jalal MM, Mir R, Hamadi A, Altayar MA, Elfaki I, Barnawi J, Alkayyal AA, Amr M, Hadeel J, Moawadh MS, et al. Association of Genetic and Allelic Variants of Von Willebrand Factor (VWF), Glutathione S-Transferase and Tumor Necrosis Factor Alpha with Ischemic Stroke Susceptibility and Progression in the Saudi Population. Life. 2023; 13(5):1200. https://doi.org/10.3390/life13051200
Chicago/Turabian StyleJalal, Mohammed M., Rashid Mir, Abdullah Hamadi, Malik A. Altayar, Imadeldin Elfaki, Jameel Barnawi, Almohanad A. Alkayyal, Mouminah Amr, Jabali Hadeel, Mamdoh S. Moawadh, and et al. 2023. "Association of Genetic and Allelic Variants of Von Willebrand Factor (VWF), Glutathione S-Transferase and Tumor Necrosis Factor Alpha with Ischemic Stroke Susceptibility and Progression in the Saudi Population" Life 13, no. 5: 1200. https://doi.org/10.3390/life13051200