
Stem Cell Therapy for Erectile Dysfunction: A Step towards a Future Treatment
 ,
,
Abstract
:1. Introduction
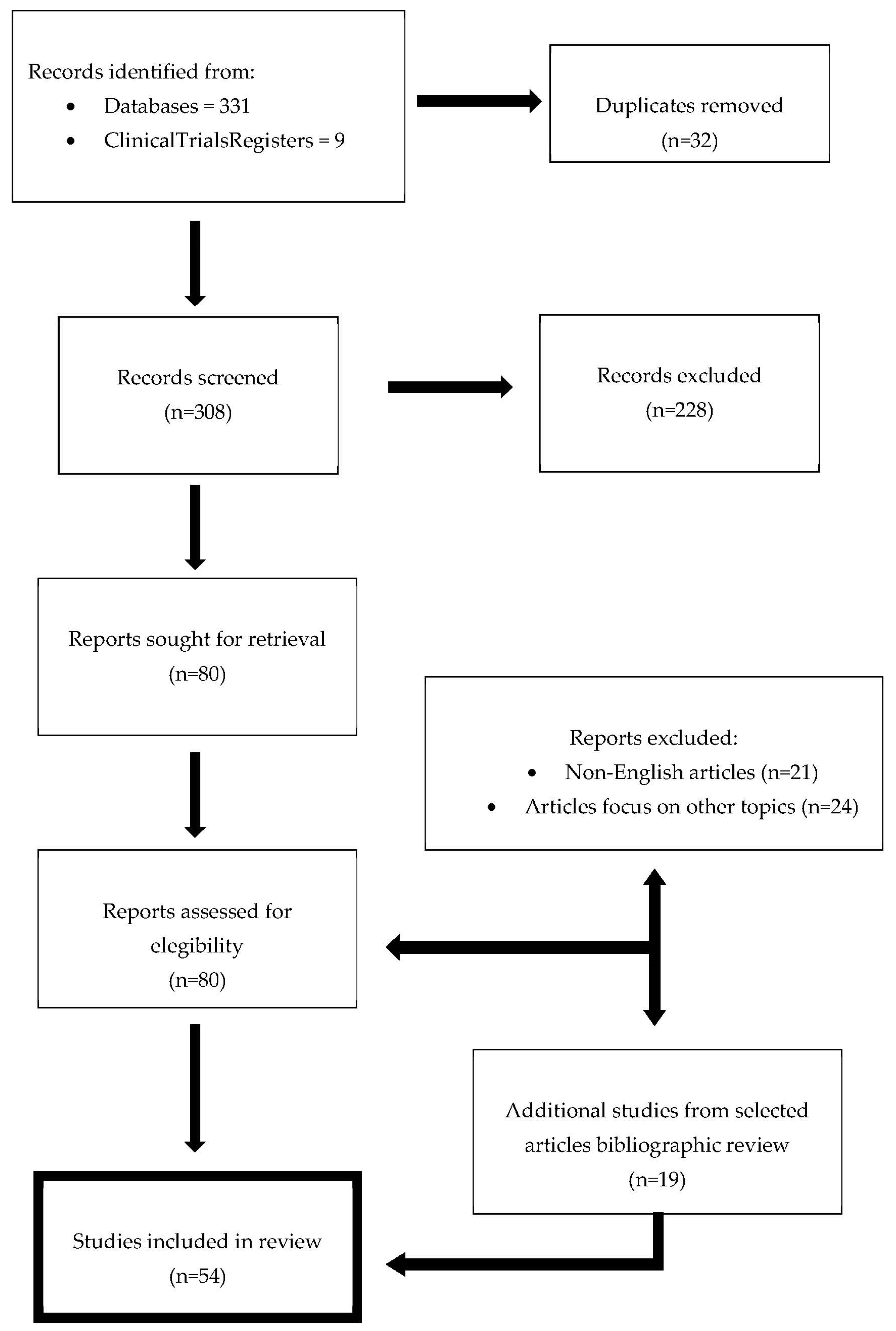
2. Materials and Methods
3. Results
3.1. Stem Cell Therapy for ED in the Preclinical Setting
3.2. Stem Cell Therapy in the Clinical Setting
3.2.1. Umbilical Cord-(UCSC) and Placenta-Derived (PSC) Stem Cells
3.2.2. Bone Marrow-Derived Stem Cells (BMSC)

{kind=link}
{kind=link}
| NCT | MI | Study Design | Design Adm./Dose Route | Comorbidity | Sample Size/Follow-Up (Months) | Latency Period until Improvement of ED | Duration Effect (Months) | SAE | Year of Publication |
|---|---|---|---|---|---|---|---|---|---|
| NR | UC-MSCs | Phase I/Pilot study. Single blinded | Single ICI/1.5 × 107 Cells | Type II DM | 10 (7)/9 | 1 | 11 | No | 2010 [43] |
| NR | BM-MNSCs | Case report | Single ICI/unquantified | COED | 1/18 | 0.75 | 18 | No | 2013 [31] |
| NR | ADSC | Pilot study | Single ICI/1.5 × 107 Cells | Type II DM | 6/12 | 2 | 12 | No | 2015 [50] |
| 02398370 | PM-MSCs | Phase I-II/Open Label | Single ICI/unquantified | COED | 8/6 | 1.5 | 6 | No | 2016 [44] |
| 01089387 | BM-MNSCs | Phase I | Single ICI/2 × 109–2 × 107 Cells | Post-RP | 12/12 | 3 | 6 | No | 2016 [46] |
| Phases II: | Single ICI/10 × 108 Cells | 18/62.1 | 3 | 6 | 2017 [45] | ||||
| 02240823 | ADSC | Phase I/Open Label | Single ICI/8.4–37.2 × 106 Cells | Post-RP | 17/6 | 6 | 6 | No | 2016 [51] |
| 21/12 | 6 | 12 | 2018 [52] | ||||||
| 02945462 | BM-MSCs | Phase I/Open Label | Two ICI/30 × 106 Cells | Type II DM | 4/12–24 | 1 | 12 | No | 2018 [48] |
| NR | AD-MSCs/PLP | Open Label/Pilot study | Single ICI/47 × 106 Cells | Type II DM, AHT, DL, Peyronie D | 8/3 | 1 | 3 | No | 2019 [53] |
| NR | Trasnsendocardial hMSC | Retrosp. Cohort | 20-20047 × 106 Cells | Cardiomyopathy-ED | 36/12 | 3 | 12 | No | 2019 [54] |
| NR | AD-MSCs/PLP | Phase I/Pilot Study. Open Label | Single ICI/47 × 106 Cells | Type II DM, AHT, DL, Peyronie D | 5/6 | 1 | 6 | No | 2020 [55] |
| NR | MSC-DE/LISWT | Prosp. Cohort | 6 ICI/5 mL | Metabolic syndrome-ED | 38/3 | 3 | No | 2020 [56] | |
| 03699943 | ABMC | Phase I/Dose escalation | Two ICI 3–6 mL 108 Cells | COED | 40/12 | 3 | 6 | No | 2020 [47] |
| 02945449 | WJ-MSCs | Phase I/Open Label | Two ICI/20 × 106 Cells | Type II DM | 22/12 | 1 | 12 | No | 2021 [49] |
| 023448499 | BM-MSCs | Phase I/Open Label | ICI Cellgram ED/30 × 106 Cells | DM/Post-RP | 10 | 1 | 12 | No | 2021 [57] |
| NR | Oral mucosa-MSCs | Rand. Single-blinded | Single ICI/50–60 × 106 Cells | DM-ED | 20/6 | 3 | 6 | No | 2021 [58] |
| NR | SHED-CM | Open Label/Pilot study | 3–8 ICI/unquantified | COED | 38/8 | ND | ND | No | 2022 [59] |
| NR | ADSC | Prosp. case series | Single ICI/unquantified | COED | 10/6 | 1 | 3 | No | 2022 [60] |
3.2.3. Adipose-Derived Stem Cells (ADSC)
3.2.4. Other Stem Cell Sources
3.3. Ethical Concerns and Limitations
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993, 270, 83–90. [CrossRef]
- Lewis, R.W.; Fugl-Meyer, K.S.; Corona, G.; Hayes, R.D.; Laumann, E.O.; Moreira, E.D.; Rellini, A.H.; Segraves, T. Definitions/Epidemiology/Risk Factors for Sexual Dysfunction. J. Sex. Med. 2010, 7, 1598–1607. [Google Scholar] [CrossRef] [PubMed]
- Jackson, G. The Importance of Risk Factor Reduction in Erectile Dysfunction. Curr. Urol. Rep. 2007, 8, 463–466. [Google Scholar] [CrossRef]
- Sattayaprasert, P.; Nassal, D.M.; Wan, X.; Deschenes, I.; Laurita, K.R. Mesenchymal Stem Cells Suppress Cardiac Alternans by Activation of PI3K Mediated Nitroso-Redox Pathway. J. Mol. Cell. Cardiol. 2016, 98, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Sun, T.; Tang, Z.; Ruan, Y.; Liu, K.; Rao, K.; Lan, R.; Wang, S.; Wang, T.; Liu, J. Exosomes Derived from Smooth Muscle Cells Ameliorate Diabetes-induced Erectile Dysfunction by Inhibiting Fibrosis and Modulating the NO/CGMP Pathway. J. Cell. Mol. Med. 2020, 24, 13289–13302. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhao, S.; Luo, L.; Wang, J.; Zhu, Z.; Xiang, Q.; Deng, Y.; Zhao, Z. Mesenchymal Stem Cell-derived Exosomes Ameliorate Erection by Reducing Oxidative Stress Damage of Corpus Cavernosum in a Rat Model of Artery Injury. J. Cell. Mol. Med. 2019, 23, 7462–7473. [Google Scholar] [CrossRef]
- Ryu, J.; Kim, D.; Song, K.M.; Yi, T.; Suh, J.; Song, S.U. Intracavernous Delivery of Clonal Mesenchymal Stem Cells Restores Erectile Function in a Mouse Model of Cavernous Nerve Injury. J. Sex. Med. 2014, 11, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Martin-Morales, A.; Sanchez-Cruz, J.J.; Saenz de Tejada, I.; Rodriguez-Vela, L.; Jimenez-Cruz, J.F.; Burgos-Rodriguez, R. Prevalence and Independent Risk Factors for Erectile Dysfunction in Spain: Results of the Epidemiologia de La Disfuncion Erectil Masculina Study. J. Urol. 2001, 166, 569–574; discussion 574–575. [Google Scholar] [CrossRef]
- Palit, V.; Eardley, I. An Update on New Oral PDE5 Inhibitors for the Treatment of Erectile Dysfunction. Nat. Rev. Urol. 2010, 7, 603–609. [Google Scholar] [CrossRef]
- Goldstein, I.; Goren, A.; Li, V.W.; Tang, W.Y.; Hassan, T.A. Epidemiology Update of Erectile Dysfunction in Eight Countries with High Burden. Sex. Med. Rev. 2020, 8, 48–58. [Google Scholar] [CrossRef]
- Magheli, A.; Burnett, A.L. Erectile Dysfunction Following Prostatectomy: Prevention and Treatment. Nat. Rev. Urol. 2009, 6, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Hellstrom, W.; Wang, G. Powers Current and Emerging Treatment Options for Peyronie’s Disease. RRU 2013, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- Decaluwé, K.; Pauwels, B.; Boydens, C.; Van de Voorde, J. Treatment of Erectile Dysfunction: New Targets and Strategies from Recent Research. Pharmacol. Biochem. Behav. 2014, 121, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Peak, T.C.; Anaissie, J.; Hellstrom, W.J.G. Current Perspectives on Stem Cell Therapy for Erectile Dysfunction. Sex. Med. Rev. 2016, 4, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.P.; Pastuszak, A.W.; Hotaling, J.M. Emerging Treatments for Erectile Dysfunction: A Review of Novel, Non-Surgical Options. Curr. Urol. Rep. 2019, 20, 44. [Google Scholar] [CrossRef]
- Soebadi, M.A.; Milenkovic, U.; Weyne, E.; Castiglione, F.; Albersen, M. Stem Cells in Male Sexual Dysfunction: Are We Getting Somewhere? Sex. Med. Rev. 2017, 5, 222–235. [Google Scholar] [CrossRef]
- Chung, E. A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction. Med. Sci. 2019, 7, 91. [Google Scholar] [CrossRef]
- Strong, T.D.; Gebska, M.A.; Champion, H.C.; Burnett, A.L.; Bivalacqua, T.J. Stem and Endothelial Progenitor Cells in Erection Biology. Int. J. Impot. Res. 2008, 20, 243–254. [Google Scholar] [CrossRef]
- Valencia Mora, M.; Antuña Antuña, S.; García Arranz, M.; Carrascal, M.T.; Barco, R. Application of Adipose Tissue-Derived Stem Cells in a Rat Rotator Cuff Repair Model. Injury 2014, 45 (Suppl. S4), S22–S27. [Google Scholar] [CrossRef]
- Albersen, M.; Lin, C.-S.; Lue, T. Stem-Cell Therapy for Erectile Dysfunction. Arab. J. Urol. 2013, 11, 237–244. [Google Scholar] [CrossRef]
- Zhang, H.; Albersen, M.; Jin, X.; Lin, G. Stem Cells: Novel Players in the Treatment of Erectile Dysfunction. Asian. J. Androl. 2012, 14, 145–155. [Google Scholar] [CrossRef]
- Lin, G.; Banie, L.; Ning, H.; Bella, A.J.; Lin, C.-S.; Lue, T.F. Potential of Adipose-Derived Stem Cells for Treatment of Erectile Dysfunction. J. Sex. Med. 2009, 6 (Suppl. S3), 320–327. [Google Scholar] [CrossRef]
- Wagers, A.J.; Weissman, I.L. Plasticity of Adult Stem Cells. Cell 2004, 116, 639–648. [Google Scholar] [CrossRef]
- Bochinski, D.; Lin, G.T.; Nunes, L.; Carrion, R.; Rahman, N.; Lin, C.S.; Lue, T.F. The Effect of Neural Embryonic Stem Cell Therapy in a Rat Model of Cavernosal Nerve Injury. BJU Int. 2004, 94, 904–909. [Google Scholar] [CrossRef]
- Wani, M.M.; Rai, B.P.; Webb, W.R.; Madaan, S. Is There a Role for Stem Cell Therapy in Erectile Dysfunction Secondary to Cavernous Nerve Injury? Network Meta-Analysis from Animal Studies and Human Trials. Ther. Adv. Urol. 2022, 14, 175628722210869. [Google Scholar] [CrossRef]
- Shan, H.; Chen, F.; Zhang, T.; He, S.; Xu, L.; Wei, A. Stem Cell Therapy for Erectile Dysfunction of Cavernous Nerve Injury Rats: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0121428. [Google Scholar] [CrossRef]
- Hou, Q.-L.; Ge, M.-Y.; Zhang, C.; Tian, D.-D.; Wang, L.-K.; Tian, H.-Z.; Wang, W.-H.; Zhang, W.-D. Adipose Tissue-Derived Stem Cell Therapy for Erectile Dysfunction in Rats: A Systematic Review and Meta-Analysis. Int. Urol. Nephrol. 2017, 49, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Jeong, H.; Park, Y.H.; Yim, H.W.; Ha, U.-S.; Hong, S.-H.; Kim, S.W.; Kim, N.J.; Lee, J.Y. Adipose Tissue-Derived Stem Cell Therapy for Cavernous Nerve Injury-Induced Erectile Dysfunction in the Rat Model: A Systematic Review and Meta-Analysis Using Methodological Quality Assessment. Int. J. Stem. Cells 2019, 12, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-Y.; Jin, X.-B.; Lue, T.F. Three Important Components in the Regeneration of the Cavernous Nerve: Brain-Derived Neurotrophic Factor, Vascular Endothelial Growth Factor and the JAK/STAT Signaling Pathway. Asian J. Androl. 2011, 13, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Albersen, M.; Kendirci, M.; Van der Aa, F.; Hellstrom, W.J.G.; Lue, T.F.; Spees, J.L. Multipotent Stromal Cell Therapy for Cavernous Nerve Injury-Induced Erectile Dysfunction. J. Sex. Med. 2012, 9, 385–403. [Google Scholar] [CrossRef]
- Ichim, T.E.; Warbington, T.; Cristea, O.; Chin, J.L.; Patel, A.N. Intracavernous Administration of Bone Marrow Mononuclear Cells: A New Method of Treating Erectile Dysfunction? J. Transl. Med. 2013, 11, 139. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-O.; Lee, H.-S.; Ahn, K.; Park, K. COMP-Angiopoietin-1 Promotes Cavernous Angiogenesis in a Type 2 Diabetic Rat Model. J. Korean Med. Sci. 2013, 28, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Nishimatsu, H.; Suzuki, E.; Kumano, S.; Nomiya, A.; Liu, M.; Kume, H.; Homma, Y. Adrenomedullin Mediates Adipose Tissue-Derived Stem Cell-Induced Restoration of Erectile Function in Diabetic Rats. J. Sex. Med. 2012, 9, 482–493. [Google Scholar] [CrossRef]
- Zhou, F.; Hui, Y.; Xu, Y.; Lei, H.; Yang, B.; Guan, R.; Gao, Z.; Xin, Z.; Hou, J. Effects of Adipose-Derived Stem Cells plus Insulin on Erectile Function in Streptozotocin-Induced Diabetic Rats. Int. Urol. Nephrol. 2016, 48, 657–669. [Google Scholar] [CrossRef]
- Yan, H.; Rong, L.; Xiao, D.; Zhang, M.; Sheikh, S.P.; Sui, X.; Lu, M. Injectable and Self-Healing Hydrogel as a Stem Cells Carrier for Treatment of Diabetic Erectile Dysfunction. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 116, 111214. [Google Scholar] [CrossRef]
- Lu, J.; Xin, Z.; Zhang, Q.; Cui, D.; Xiao, Y.; Zhuo, J.; Sun, F.; Xia, S.; Shao, Y. Beneficial Effect of PEDF-Transfected ADSCs on Erectile Dysfunction in a Streptozotocin-Diabetic Rat Model. Cell. Tissue Res. 2016, 366, 623–637. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhang, Y.; Zang, G.; Wang, T.; Yu, Z.; Wang, S.; Tang, Z.; Liu, J. Adipose-Derived Stem Cells Improve Erectile Function Partially through the Secretion of IGF-1, BFGF, and VEGF in Aged Rats. Andrology 2018, 6, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.M.; Fandel, T.M.; Lin, G.; Shindel, A.W.; Banie, L.; Lin, C.-S.; Lue, T.F. Treatment of Erectile Dysfunction in the Obese Type 2 Diabetic ZDF Rat with Adipose Tissue-Derived Stem Cells. J. Sex. Med. 2010, 7, 89–98. [Google Scholar] [CrossRef]
- Feng, H.; Liu, Q.; Deng, Z.; Li, H.; Zhang, H.; Song, J.; Liu, X.; Liu, J.; Wen, B.; Wang, T. Human Umbilical Cord Mesenchymal Stem Cells Ameliorate Erectile Dysfunction in Rats with Diabetes Mellitus through the Attenuation of Ferroptosis. Stem. Cell. Res. Ther. 2022, 13, 450. [Google Scholar] [CrossRef]
- Luo, C.; Peng, Y.; Zhou, X.; Fan, J.; Chen, W.; Zhang, H.; Wei, A. NLRP3 Downregulation Enhances Engraftment and Functionality of Adipose-Derived Stem Cells to Alleviate Erectile Dysfunction in Diabetic Rats. Front. Endocrinol. 2022, 13, 913296. [Google Scholar] [CrossRef]
- Mukti, A.; Ilyas, S.; Warli, S.; Putra, A.; Rasyid, N.; Munir, D.; Siregar, K.; Ichwan, M. Umbilical Cord-Derived Mesenchymal Stem Cells Improve TGF-β, α-SMA and Collagen on Erectile Dysfunction in Streptozotocin-Induced Diabetic Rats. Med. Arch. 2022, 76, 4. [Google Scholar] [CrossRef]
- He, L.; Yu, T.; Xiao, Y.; Huang, Y.; Guan, Y.; Zhao, F.; Ma, L. Co-Overexpression of VEGF and Smad7 Improved the Therapeutic Effects of Adipose-Derived Stem Cells on Neurogenic Erectile Dysfunction in the Rat Model. Andrologia 2022, 54, e1453. [Google Scholar] [CrossRef]
- Bahk, J.Y.; Jung, J.H.; Han, H.; Min, S.K.; Lee, Y.S. Treatment of Diabetic Impotence with Umbilical Cord Blood Stem Cell Intracavernosal Transplant: Preliminary Report of 7 Cases. Exp. Clin. Transpl. 2010, 8, 150–160. [Google Scholar]
- Levy, J.A.; Marchand, M.; Iorio, L.; Cassini, W.; Zahalsky, M.P. Determining the Feasibility of Managing Erectile Dysfunction in Humans With Placental-Derived Stem Cells. J. Am. Osteopath. Assoc. 2016, 116, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Yiou, R.; Hamidou, L.; Birebent, B.; Bitari, D.; Le Corvoisier, P.; Contremoulins, I.; Rodriguez, A.-M.; Augustin, D.; Roudot-Thoraval, F.; de la Taille, A.; et al. Intracavernous Injections of Bone Marrow Mononucleated Cells for Postradical Prostatectomy Erectile Dysfunction: Final Results of the INSTIN Clinical Trial. Eur. Urol. Focus 2017, 3, 643–645. [Google Scholar] [CrossRef]
- Yiou, R.; Hamidou, L.; Birebent, B.; Bitari, D.; Lecorvoisier, P.; Contremoulins, I.; Khodari, M.; Rodriguez, A.-M.; Augustin, D.; Roudot-Thoraval, F.; et al. Safety of Intracavernous Bone Marrow-Mononuclear Cells for Postradical Prostatectomy Erectile Dysfunction: An Open Dose-Escalation Pilot Study. Eur. Urol. 2016, 69, 988–991. [Google Scholar] [CrossRef]
- Bieri, M.; Said, E.; Antonini, G.; Dickerson, D.; Tuma, J.; Bartlett, C.E.; Patel, A.N.; Gershman, A. Phase I and Registry Study of Autologous Bone Marrow Concentrate Evaluated in PDE5 Inhibitor Refractory Erectile Dysfunction. J. Transl. Med. 2020, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Al Demour, S.; Jafar, H.; Adwan, S.; AlSharif, A.; Alhawari, H.; Alrabadi, A.; Zayed, A.; Jaradat, A.; Awidi, A. Safety and Potential Therapeutic Effect of Two Intracavernous Autologous Bone Marrow Derived Mesenchymal Stem Cells Injections in Diabetic Patients with Erectile Dysfunction: An Open Label Phase I Clinical Trial. Urol. Int. 2018, 101, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Al Demour, S.; Adwan, S.; Jafar, H.; Rahmeh, R.; Alhawari, H.; Awidi, A. Safety and Efficacy of 2 Intracavernous Injections of Allogeneic Wharton’s Jelly-Derived Mesenchymal Stem Cells in Diabetic Patients with Erectile Dysfunction: Phase 1/2 Clinical Trial. Urol. Int. 2021, 105, 935–943. [Google Scholar] [CrossRef]
- Garber, M.G.; Carlos, N.D. Intracavernous Administration of Adipose Stem Cells: A New Technique of Treating Erectile Dysfunction in Diabetic Patient, Preliminary Report of 6 Cases. MOJ Cell. Sci. Rep. 2015, 2, 00018. [Google Scholar]
- Haahr, M.K.; Jensen, C.H.; Toyserkani, N.M.; Andersen, D.C.; Damkier, P.; Sørensen, J.A.; Lund, L.; Sheikh, S.P. Safety and Potential Effect of a Single Intracavernous Injection of Autologous Adipose-Derived Regenerative Cells in Patients with Erectile Dysfunction Following Radical Prostatectomy: An Open-Label Phase I Clinical Trial. EBioMedicine 2016, 5, 204–210. [Google Scholar] [CrossRef]
- Haahr, M.K.; Harken Jensen, C.; Toyserkani, N.M.; Andersen, D.C.; Damkier, P.; Sørensen, J.A.; Sheikh, S.P.; Lund, L. A 12-Month Follow-up after a Single Intracavernous Injection of Autologous Adipose-Derived Regenerative Cells in Patients with Erectile Dysfunction Following Radical Prostatectomy: An Open-Label Phase I Clinical Trial. Urology 2018, 121, 203.e6–203.e13. [Google Scholar] [CrossRef] [Green Version]
- Protogerou, V.; Michalopoulos, E.; Mallis, P.; Gontika, I.; Dimou, Z.; Liakouras, C.; Stavropoulos-Giokas, C.; Kostakopoulos, N.; Chrisofos, M.; Deliveliotis, C. Administration of Adipose Derived Mesenchymal Stem Cells and Platelet Lysate in Erectile Dysfunction: A Single Center Pilot Study. Bioengineering 2019, 6, 21. [Google Scholar] [CrossRef]
- Ory, J.; Saltzman, R.G.; Blachman-Braun, R.; Dadoun, S.; DiFede, D.L.; Premer, C.; Hurwitz, B.; Hare, J.M.; Ramasamy, R. The Effect of Transendocardial Stem Cell Injection on Erectile Function in Men With Cardiomyopathy: Results From the TRIDENT, POSEIDON, and TAC-HFT Trials. J. Sex. Med. 2020, 17, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Protogerou, V.; Beshari, S.E.; Michalopoulos, E.; Mallis, P.; Chrysikos, D.; Samolis, A.A.; Stavropoulos-Giokas, C.; Troupis, T. The Combined Use of Stem Cells and Platelet Lysate Plasma for the Treatment of Erectile Dysfunction: A Pilot Study-6 Months Results. Medicines 2020, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Zasieda, Y. Erectile dysfunction treatment with combination of mesenchymal stem cell derived exosomes and focused low-intensive shock wave therapy. Men’s Health Gend. Psychosom. Med. 2020, 70–78. [Google Scholar] [CrossRef]
- You, D.; Jang, M.J.; Song, G.; Shin, H.C.; Suh, N.; Kim, Y.M.; Ahn, T.Y.; Kim, C.-S. Safety of Autologous Bone Marrow-Derived Mesenchymal Stem Cells in Erectile Dysfunction: An Open-Label Phase 1 Clinical Trial. Cytotherapy 2021, 23, 931–938. [Google Scholar] [CrossRef]
- Mirzaei, M.; Bagherinasabsarab, M.; Pakmanesh, H.; Mohammadi, R.; Teimourian, M.; Jahani, Y.; Farsinejad, A. The Effect of Intracavernosal Injection of Stem Cell in the Treatment of Erectile Dysfunction in Diabetic Patients: A Randomized Single-Blinded Clinical Trial. Urol. J. 2021, 18, 675–681. [Google Scholar] [CrossRef]
- Koga, S.; Horiguchi, Y. Efficacy of a Cultured Conditioned Medium of Exfoliated Deciduous Dental Pulp Stem Cells in Erectile Dysfunction Patients. J. Cell. Mol. Med. 2022, 26, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Fode, M.; Nadler, N.; Lund, L.; Azawi, N. Feasibility of Minimally Invasive, Same-Day Injection of Autologous Adipose-Derived Stem Cells in the Treatment of Erectile Dysfunction. Scand. J. Urol. 2022, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Matz, E.L.; Terlecki, R.P. Stem Cell and Gene-Based Therapy for Erectile Dysfunction: Current Status and Future Needs. Urol. Clin. N. Am. 2021, 48, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Sudi, A.; Bello, A.; Lawal, A.T.; Awaisu, M.; Maitama, H.Y. Managing the Sequelae of Urology Medical Tourism: A Single Center Experience. Niger. Postgrad. Med. J. 2018, 25, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Marketing Used by Men’s Health Clinics Is Cause for Concern. Available online: https://www.urologytimes.com/view/marketing-used-mens-health-clinics-cause-concern (accessed on 11 November 2022).
- Fernández-Santos, M.E.; Garcia-Arranz, M.; Andreu, E.J.; García-Hernández, A.M.; López-Parra, M.; Villarón, E.; Sepúlveda, P.; Fernández-Avilés, F.; García-Olmo, D.; Prosper, F.; et al. Optimization of Mesenchymal Stromal Cell (MSC) Manufacturing Processes for a Better Therapeutic Outcome. Front. Immunol. 2022, 13, 918565. [Google Scholar] [CrossRef] [PubMed]
- Georgiev-Hristov, T.; García-Arranz, M.; Trébol-López, J.; Barba-Recreo, P.; García-Olmo, D. Searching for the Optimal Donor for Allogenic Adipose-Derived Stem Cells: A Comprehensive Review. Pharmaceutics 2022, 14, 2338. [Google Scholar] [CrossRef]
- Rezaee, M.E.; Ward, C.E.; Brandes, E.R.; Munarriz, R.M.; Gross, M.S. A Review of Economic Evaluations of Erectile Dysfunction Therapies. Sex. Med. Rev. 2020, 8, 497–503. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Aizpurua, X.; Garranzo-Ibarrola, M.; Simón-Rodríguez, C.; García-Cardoso, J.V.; Chávez-Roa, C.; López-Martín, L.; Tufet i Jaumot, J.J.; Alonso-Román, J.; Maqueda-Arellano, J.; Gómez-Jordana, B.; et al. Stem Cell Therapy for Erectile Dysfunction: A Step towards a Future Treatment. Life 2023, 13, 502. https://doi.org/10.3390/life13020502
Pérez-Aizpurua X, Garranzo-Ibarrola M, Simón-Rodríguez C, García-Cardoso JV, Chávez-Roa C, López-Martín L, Tufet i Jaumot JJ, Alonso-Román J, Maqueda-Arellano J, Gómez-Jordana B, et al. Stem Cell Therapy for Erectile Dysfunction: A Step towards a Future Treatment. Life. 2023; 13(2):502. https://doi.org/10.3390/life13020502
Chicago/Turabian StylePérez-Aizpurua, Xabier, María Garranzo-Ibarrola, Carlos Simón-Rodríguez, Juan Vicente García-Cardoso, César Chávez-Roa, Leticia López-Martín, Jaime Jorge Tufet i Jaumot, Josué Alonso-Román, Jesús Maqueda-Arellano, Blanca Gómez-Jordana, and et al. 2023. "Stem Cell Therapy for Erectile Dysfunction: A Step towards a Future Treatment" Life 13, no. 2: 502. https://doi.org/10.3390/life13020502