
Gender Differences in the Impact of Recommendations on Diagnostic Imaging Tests: A Retrospective Study 2007–2021
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Imaging Test Frequency
2.5. Effective Dose Estimate
2.6. Socioeconomical Status
2.7. Calendar Time
2.8. Statistical Analysis
3. Results
3.1. Population Included in the Study
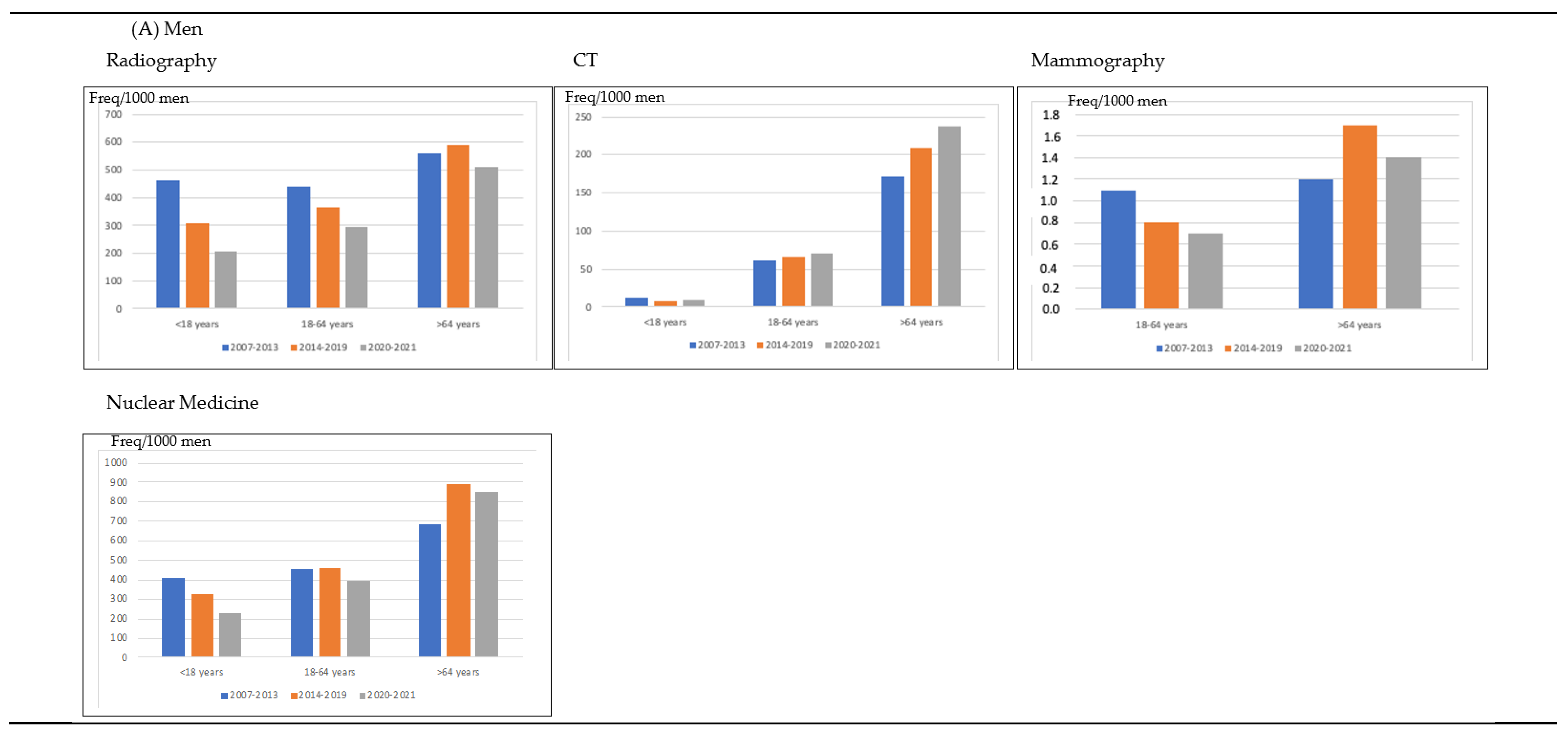
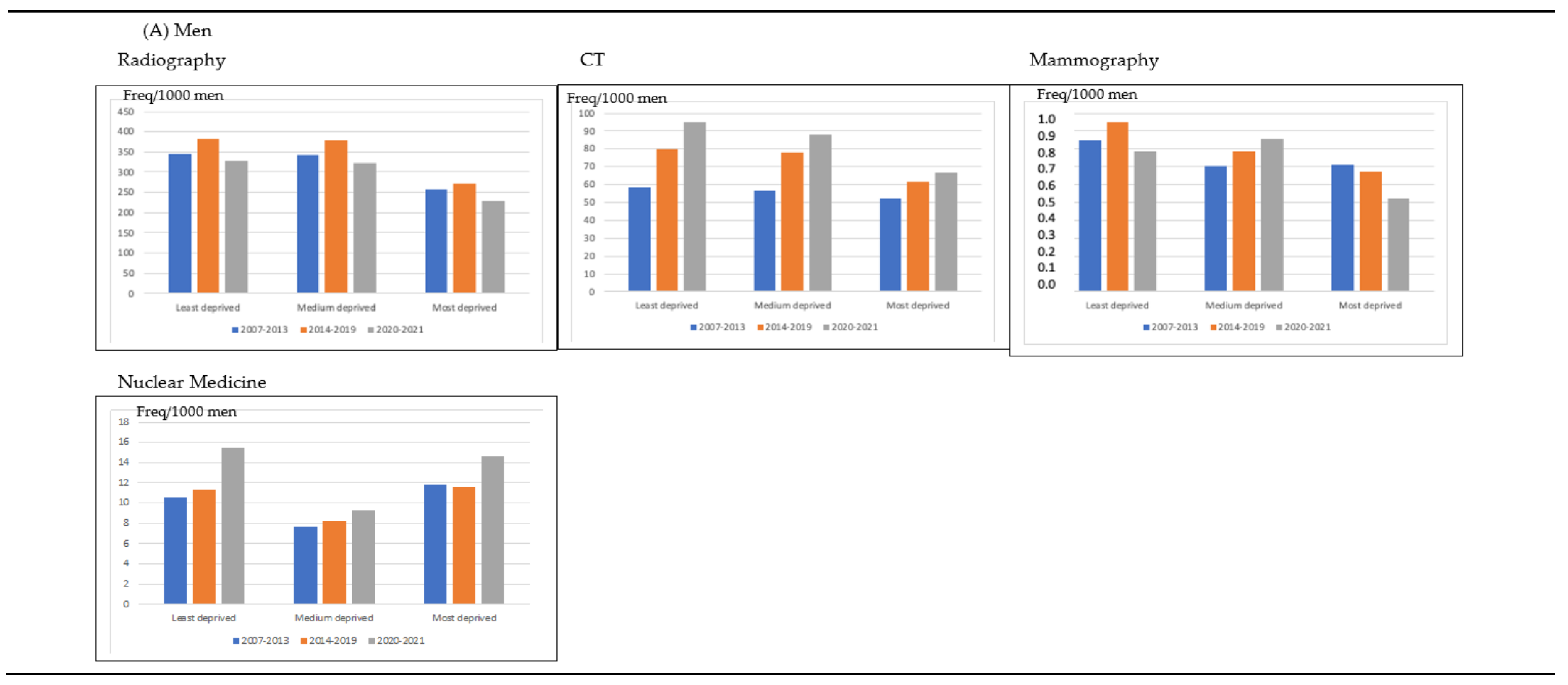
3.2. Impact of Calendar Time in the Frequency of Imaging Tests According to Type of Imaging Test, Patients’ Age and Deprivation Index for Men and Women (Table 1)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency per 1000 Persons | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| 2007–2013 | 2014–2019 | 2020–2021 | p Value | 2007–2013 | 2014–2019 | 2020–2021 | p Value | |
| Imaging test | <0.001 | <0.001 | ||||||
| Mamography | 0.9 | 0.9 | 0.8 | 26.3 | 32.5 | 28.7 | ||
| Radiography | 400.5 | 407.6 | 330.4 | 460.4 | 486.7 | 376.3 | ||
| CT | 67.1 | 88.8 | 98.7 | 53.0 | 71.7 | 76.9 | ||
| Nuclear medicine | 29.9 | 38.4 | 41.2 | 35.6 | 43.4 | 37.7 | ||
| Age (years) | <0.001 | <0.001 | ||||||
| <18 | 409.4 | 327.3 | 223.4 | 310.5 | 255.6 | 168.1 | ||
| 18–64 | 452.2 | 458.4 | 393.9 | 519.4 | 532.6 | 431 | ||
| >64 | 686.2 | 892.3 | 855.8 | 916.6 | 1180 | 1010.3 | ||
| Deprivation index | <0.001 | <0.001 | ||||||
| Least deprived | 414.5 | 474.4 | 440.1 | 492.1 | 587.1 | 500.9 | ||
| Medium deprived | 407.6 | 466.1 | 422.1 | 452.3 | 537.0 | 456.6 | ||
| Most deprived | 323.1 | 346.1 | 310.4 | 400.1 | 448.5 | 376.2 | ||
| Total | 498.5 | 535.6 | 471.0 | <0.001 | 575.3 | 634.3 | 519.6 | <0.001 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mettler, F.A., Jr.; Bhargavan, M.; Faulkner, K.; Gilley, D.B.; Gray, J.E.; Ibbott, G.S.; Lipoti, J.A.; Mahesh, M.; McCrohan, J.L.; Stabin, M.G.; et al. Radiologic and nuclear medicine studies in the United States and worldwide: Frequency, radiation dose, and comparison with other radiation sources—1950–2007. Radiology 2009, 253, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Skrk, D.; Zontar, D. Estimated collective effective dose to the population from nuclear medicine examinations in Slovenia. Radiol. Oncol. 2013, 47, 304–310. [Google Scholar]
- Huppmann, M.V.; Johnson, W.B.; Javitt, M.C. Radiation risks from exposure to chest computed tomography. Semin. Ultrasound CT MR 2010, 31, 14–28. [Google Scholar] [CrossRef]
- Sodickson, A.; Baeyens, P.F.; Andriole, K.P.; Prevedello, L.M.; Nawfel, R.D.; Hanson, R.; Khorasani, R.; Recurrent, C.T. Cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology 2009, 251, 175–184. [Google Scholar] [CrossRef]
- Lumbreras, B.; González-Alvarez, I.; Gómez-Sáez, N.; Lorente, M.F.; Hernández-Aguado, I. Management of patients with incidental findings in imaging tests: A large prospective single-center study. Clin. Imaging 2014, 38, 249–254. [Google Scholar] [CrossRef] [PubMed]
- IAEA Smart Card/SmartRadTrack Project. Available online: https://rpop.iaea.org/RPOP/RPoP/Content/News/smart-card-project.htm (accessed on 30 October 2022).
- Council Directive 97/43/Euratom of 30 June 1997 on Health Protection against Dangers Arising from Ionising Radiation in Medical Exposures. Available online: https://www.eumonitor.eu/9353000/1/j9vvik7m1c3gyxp/vitgbgi170zi (accessed on 30 October 2022).
- Medical Radiation Protection Education and Training (Medrapet Project). Available online: http://www.medrapet.eu/ (accessed on 30 October 2022).
- European Medical ALARA Network (EMAN). Available online: http://www.eman-network.eu/ (accessed on 30 October 2022).
- European Commission Project: Guidelines on Medical Physics Expert. Available online: http://ec.europa.eu/energy/nuclear/events/2011_05_09_mpe_workshop_en.htm.2012;366:780-1 (accessed on 30 October 2022).
- Council Directive 2013/59/Euratom: A revised Basic Safety Standards Directive Was Adopted by the European Union. Available online: https://eur-lex.europa.eu/legal-content/ES/TXT/PDF/?uri=CELEX:32013L0059&from=EN (accessed on 30 October 2022).
- Real Decreto 601/2019, De 18 De Octubre, Sobre Justificación y Optimización Del Uso De Las Radiaciones Ionizantes Para La Protección Radiológica De Las Personas Con Ocasión De Exposiciones Médicas. Available online: https://www.boe.es/diario_boe/txt.php?id=BOE-A-2019-15604 (accessed on 30 October 2022).
- Winder, M.; Owczarek, A.J.; Chudek, J.; Pilch-Kowalczyk, J.; Baron, J. Are We Overdoing It? Changes in Diagnostic Imaging Workload during the Years 2010–2020 including the Impact of the SARS-CoV-2 Pandemic. Healthcare 2021, 16, 1557. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Sendino, A.; Guallar-Castillón, P.; Banegas, J.R.; Rodríguez-Artalejo, F. Gender differences in the utilization of health-care services among the older adult population of Spain. BMC Public Health 2006, 6, 155. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Cantero, M.T.; Blasco-Blasco, M.; Chilet-Rosell, E.; Peiró, A.M. Sesgos de género en el esfuerzo terapéutico: De la investigación a la atención sanitaria. Farm. Hosp. 2020, 44, 109–113. [Google Scholar]
- Vilar-Palop, J.; Hernandez-Aguado, I.; Pastor-Valero, M.; Vilar, J.; González-Alvarez, I.; Lumbreras, B. Appropriate use of medical imaging in two Spanish public hospitals: A cross-sectional analysis. BMJ Open 2018, 8, e019535. [Google Scholar] [CrossRef]
- Gupta, A.; Tsiaras, S.V.; Dunsiger, S.I.; Tilkemeier, P.L. Gender disparity and the appropriateness of myocardial perfusion imaging. J. Nucl. Cardiol. 2011, 18, 588–594. [Google Scholar] [CrossRef]
- Berrington de Gonzalez, A.; Darby, S. Risk of cancer from diagnostic X-rays: Estimates for the UK and 14 other countries. Lancet 2004, 363, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Berrington de González, A.; Mahesh, M.; Kim, K.P.; Bhargavan, M.; Lewis, R.; Mettler, F.; Land, C. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch. Intern. Med. 2009, 169, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Smith-Bindman, R.; Lipson, J.; Marcus, R.; Kim, K.P.; Mahesh, M.; Gould, R.; Berrington de González, A.; Miglioretti, D.L. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch. Intern. Med. 2009, 169, 2078–2086. [Google Scholar] [CrossRef]
- Fazel, R.; Krumholz, H.M.; Wang, Y.; Ross, J.S.; Chen, J.; Ting, H.H.; Shah, N.D.; Nasir, K.; Einstein, A.J.; Nallamothu, B.K. Exposure to low-dose ionizing radiation from medical imaging procedures. N. Engl. J. Med. 2009, 361, 849–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith-Bindman, R. Environmental causes of breast cancer and radiation from medical imaging: Findings from the Institute of Medicine report. Arch. Intern. Med. 2012, 172, 1023–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Research Council of the National Academies. BEIR VII Phase 2. In Health Risks from Exposure to Low Levels of Ionizing Radiation; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Einstein, A.J.; Pascual, T.N.; Mercuri, M.; Karthikeyan, G.; Vitola, J.V.; Mahmarian, J.J.; Better, N.; Bouyoucef, S.E.; Hee-Seung Bom, H.; Lele, V.; et al. Current worldwide nuclear cardiology practices and radiation exposure: Results from the 65 country IAEA Nuclear Cardiology Protocols Cross- Sectional Study (INCAPS). Eur. Heart J. 2015, 36, 1689–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Droomers, M.; Westert, G.P. Do lower socioeconomic groups use more health services, because they suffer from more illnesses? Eur. J. Pub. Health 2004, 14, 311–313. [Google Scholar] [CrossRef] [Green Version]
- Agborsangaya, C.B.; Lau, D.; Lahtinen, M.; Cooke, T.; Johnson, J.A. Multimorbidity prevalence and patterns across socioeconomic determinants: A cross- sectional survey. BMC Public Health 2012, 12, 201. [Google Scholar] [CrossRef] [Green Version]
- Tadiri, C.P.; Gisinger, T.; Kautzky-Willer, A.; Kublickiene, K.; Herrero, M.T.; Norris, C.M.; Raparelli, V.; Pilote, L.; GOING-FWD Consortium. Determinants of perceived health and unmet healthcare needs in universal healthcare systems with high gender equality. BMC Public Health 2021, 31, 1488. [Google Scholar] [CrossRef]
- Jahnen, A.; Järvinen, H.; Olerud, H.; Vassilieva, J.; Vogiatzi, S.; Shannoun, F.; Bly, R. Analysis of factors correlating with medical radiological examination frequencies. Radiat. Prot. Dosim. 2015, 165, 133–136. [Google Scholar] [CrossRef]
- Lumbreras, B.; Salinas, J.M.; Gonzalez-Alvarez, I. Cumulative exposure to ionising radiation from diagnostic imaging tests: A 12-year follow-up population-based analysis in Spain. BMJ Open 2019, 18, e030905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marant-Micallef, C.; Shield, K.D.; Vignat, J.; Cléro, E.; Kesminiene, A.; Hill, C.; Rogel, A.; Vacquier, B.; Bray, F.; Laurier, D.; et al. The risk of cancer attributable to diagnostic medical radiation: Estimation for France in 2015. Int. J. Cancer 2019, 144, 2954–2963. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Palop, J.; Vilar, J.; Hernández-Aguado, I.; González-Álvarez, I.; Lumbreras, B. Updated effective doses in radiology. J. Radiol. Prot. 2016, 36, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Shrimpton, P.C.; Hillier, M.C.; Lewis, M.A.; Dunn, M. National survey of doses from CT in the UK: 2003. Br. J. Radiol. 2006, 79, 968–980. [Google Scholar] [CrossRef]
- Mettler, F.A., Jr.; Huda, W.; Yoshizumi, T.T.; Mahesh, M. Effective doses in radiology and diagnostic nuclear medicine: A catalog. Radiology 2008, 248, 254–263. [Google Scholar] [CrossRef]
- Cohnen, M.; Poll, L.J.; Puettmann, C.; Ewen, K.; Saleh, A.; Mödder, U. Effective doses in standard protocols for multi-slice CT scanning. Eur. Radiol. 2003, 13, 1148–1153. [Google Scholar] [CrossRef]
- Duque, I.; Domínguez-Berjón, M.F.; Cebrecos, A.; Prieto-Salceda, M.D.; Esnaola, S.; Calvo Sánchez, M.; Marí-Dell’Olmo, M. en nombre del Grupo de Determinantes Sociales de la Salud, iniciativa contexto de la Sociedad Española de Epidemiología. Índice de privación en España por sección censal en 2011 [Deprivation index by enumeration district in Spain, 2011]. Gac. Sanit. 2021, 35, 113–122. [Google Scholar] [CrossRef]
- Lumbreras, B.; Vilar, J.; González-Álvarez, I.; Guilabert, M.; Parker, L.A.; Pastor-Valero, M.; Domingo, M.L.; Fernández-Lorente, M.F.; Hernández-Aguado, I. Evaluation of clinicians’ knowledge and practices regarding medical radiological exposure: Findings from a mixed-methods investigation (survey and qualitative study). BMJ Open 2016, 6, e012361. [Google Scholar] [CrossRef] [Green Version]
- Kralik, I.; Štefanić, M.; Brkić, H.; Šarić, G.; Težak, S.; Grbac Ivanković, S.; Griotto, N.; Štimac, D.; Rubin, O.; Salha, T.; et al. Estimated collective effective dose to the population from nuclear medicine diagnostic procedures in Croatia: A comparison of 2010 and 2015. PLoS ONE 2017, 12, e0180057. [Google Scholar] [CrossRef]
- Brenner, D.J.; Hall, E.J. Computed tomography—An increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Stein, E.G.; Haramati, L.B.; Bellin, E.; Ashton, L.; Mitsopoulos, G.; Schoenfeld, A.; Amis, E.S., Jr. Radiation exposure from medical imaging in patients with chronic and recurrent conditions. J. Am. Coll. Radiol. 2010, 7, 351–359. [Google Scholar] [CrossRef]
- Smith-Bindman, R.; Miglioretti, D.L.; Johnson, E.; Lee, C.; Feigelson, H.S.; Flynn, M.; Greenlee, R.T.; Kruger, R.L.; Hornbrook, M.C.; Roblin, D.; et al. Use of diagnostic imaging studies and associated radiation exposure for patients enrolled in large integrated health care systems, 1996–2010. JAMA 2012, 307, 2400–2409. [Google Scholar] [CrossRef]
- Lee, D.W.; Levy, F. The sharp slowdown in growth of medical imaging: An early analysis suggests combination of policies was the cause. Health Aff. 2012, 31, 1876–1884. [Google Scholar] [CrossRef] [PubMed]
- Herts, B.R.; Perl J 2nd Seney, C.; Lieber, M.L.; Davros, W.J.; Baker, M.E. Comparison of examination times between CT scanners: Are the newer scanners faster? AJR Am. J. Roentgenol. 1998, 170, 13–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehani, M.M.; Yang, K.; Melick, E.R.; Heil, J.; Šalát, D.; Sensakovic, W.F.; Liu, B. Patients undergoing recurrent CT scans: Assessing the magnitude. Eur. Radiol. 2020, 30, 1828–1836. [Google Scholar] [CrossRef] [PubMed]
- Chilet-Rosell, E.; Parker, L.A.; Hernández-Aguado, I.; Pastor-Valero, M.; Vilar, J.; González-Álvarez, I.; Salinas-Serrano, J.M.; Lorente-Fernández, F.; Domingo, M.L.; Lumbreras, B. Differences in the clinical management of women and men after detection of a solitary pulmonary nodule in clinical practice. Eur. Radiol. 2020, 30, 4390–4397. [Google Scholar] [CrossRef] [PubMed]
- Tannenbaum, C.; Clow, B.; Haworth-Brockman, M.; Voss, P. Sex and gender considerations in Canadian clinical practice guidelines: A systematic review. CMAJ Open 2017, 5, E66–E73. [Google Scholar] [CrossRef] [Green Version]
- Brix, G.; Nagel, H.D.; Stamm, G.; Veit, R.; Lechel, U.; Griebel, J.; Galanski, M. Radiation exposure in multi-slice versus single-slice spiral CT: Results of a nationwide survey. Eur. Radiol. 2003, 8, 1979–1991. [Google Scholar] [CrossRef]




| Mean Dose (mSv) | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| 2007–2013 | 2014–2019 | 2020–2021 | p Value | 2007–2013 | 2014–2019 | 2020–2021 | p Value | |
| Imaging test | <0.001 | <0.001 | ||||||
| Mamography | 0 | 0 | 0 | 0.01 | 0.01 | 0.01 | ||
| Radiography | 0.14 | 0.20 | 0.17 | 0.17 | 0.24 | 0.20 | ||
| CT | 0.57 | 0.71 | 0.80 | 0.44 | 0.56 | 0.63 | ||
| Nuclear medicine | 0.32 | 0.36 | 0.30 | 0.37 | 0.43 | 0.32 | ||
| Age | <0.001 | <0.001 | ||||||
| <18 | 0.31 | 0.16 | 0.22 | 0.25 | 0.21 | 0.15 | ||
| 18–64 | 0.80 | 1.00 | 1.05 | 0.83 | 1.04 | 1.05 | ||
| >64 | 2.20 | 3.18 | 5.59 | 1.98 | 2.80 | 2.88 | ||
| Deprivation index | <0.001 | <0.001 | ||||||
| Least deprived | 0.77 | 1.02 | 1.23 | 0.70 | 0.97 | 1.02 | ||
| Medium deprived | 0.71 | 0.96 | 1.07 | 0.63 | 0.85 | 0.91 | ||
| Most deprived | 0.69 | 0.82 | 0.90 | 0.64 | 0.78 | 0.82 | ||
| Total | 1.04 | 1.27 | 1.27 | <0.001 | 0.99 | 1.24 | 1.16 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parker, L.A.; Moreno-Garijo, A.; Chilet-Rosell, E.; Lorente, F.; Lumbreras, B. Gender Differences in the Impact of Recommendations on Diagnostic Imaging Tests: A Retrospective Study 2007–2021. Life 2023, 13, 289. https://doi.org/10.3390/life13020289
Parker LA, Moreno-Garijo A, Chilet-Rosell E, Lorente F, Lumbreras B. Gender Differences in the Impact of Recommendations on Diagnostic Imaging Tests: A Retrospective Study 2007–2021. Life. 2023; 13(2):289. https://doi.org/10.3390/life13020289
Chicago/Turabian StyleParker, Lucy A., Andrea Moreno-Garijo, Elisa Chilet-Rosell, Fermina Lorente, and Blanca Lumbreras. 2023. "Gender Differences in the Impact of Recommendations on Diagnostic Imaging Tests: A Retrospective Study 2007–2021" Life 13, no. 2: 289. https://doi.org/10.3390/life13020289