
Healing Time of Skin Ulcers in Homecare Residents in the Province of Reggio Emilia, Northern Italy

 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lazarus, G.S.; Cooper, D.M.; Knighton, D.R.; Margolis, D.J.; Pecoraro, R.E.; Rodeheaver, G.; Robson, M.C. Definitions and guidelines for assessment of wounds and evaluation of healing. Arch. Derm. 1994, 130, 489–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frykberg, R.G.; Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 2015, 4, 560–582. [Google Scholar] [CrossRef] [Green Version]
- Sen, C.K.; Gordillo, G.M.; Roy, S.; Kirsner, R.; Lambert, L.; Hunt, T.K.; Gottrup, F.; Gurtner, G.C.; Longaker, M.T. Human skin wounds: A major and snowballing threat to public health and the economy. Wound Repair Regen. 2009, 17, 763–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyaw, B.M.; Järbrink, K.; Martinengo, L.; Car, J.; Harding, K.; Schmidtchen, A. Need for improved definition of “chronic wounds” in clinical studies. Acta Derm. Venereol. 2018, 98, 157–158. [Google Scholar] [CrossRef] [Green Version]
- Dubhashi, S.P.; Sindwani, R.D. A comparative study of honey and phenytoin dressings for chronic wounds. Indian J. Surg. 2015, 77, 1209–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, C.J.; Humphreys, I.; Fletcher, J.; Harding, K.; Chamberlain, G.; Macey, S. Estimating the costs associated with the management of patients with chronic wounds using linked routine data. Int. Wound J. 2016, 13, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Martinengo, L.; Olsson, M.; Bajpai, R.; Soljak, M.; Upton, Z.; Schmidtchen, A.; Car, J.; Järbrink, K. Prevalence of chronic wounds in the general population: Systematic review and meta-analysis of observational studies. Ann. Epidemiol. 2019, 29, 8–15. [Google Scholar] [CrossRef]
- Lindholm, C.; Searle, R. Wound management for the 21st century: Combining effectiveness and efficiency. Int. Wound J. 2016, 13 (Suppl. 2), 5–15. [Google Scholar] [CrossRef] [Green Version]
- Guest, J.F.; Ayoub, N.; McIlwraith, T.; Uchegbu, I.; Gerrish, A.; Weidlich, D.; Vowden, K.; Vowden, P. Health economic burden that different wound types impose on the UK’s National Health Service. Int. Wound J. 2017, 14, 322–330. [Google Scholar] [CrossRef]
- Graves, N.; Zheng, H. The prevalence and incidence of chronic wounds: A literature review. Wound Pract. Res. J. Aust. Wound Manag. Assoc. 2014, 22, 4–19. [Google Scholar]
- Nunan, R.; Harding, K.G.; Martin, P. Clinical challenges of chronic wounds: Searching for an optimal animal model to recapitulate their complexity. Dis. Model. Mech. 2014, 7, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- European Pressure Ulcer Advisory Panel; National Pressure Injury Advisory Panel; Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide; Haesler, E., Ed.; EPUAP/NPIAP/PPPIA, 2019; Available online: https://www.internationalguideline.com/static/pdfs/Quick_Reference_Guide-10Mar2019.pdf (accessed on 10 November 2022).
- Dissemond, J.; Protz, K.; Erfurt-Berge, C.; Kröger, K.; Kottner, J. Wundbehandlung ohne kurative Zielsetzung: Ein Positionspapier der Initiative Chronische Wunden (ICW) e. V. Dermatologie 2022, 73, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Ayello, E.A.; Levine, J.M.; Langemo, D.; Kennedy-Evans, K.L.; Brennan, M.R.; Gary Sibbald, R. Reexamining the literature on terminal ulcers, SCALE, skin failure, and unavoidable pressure injuries. Adv. Skin Wound Care 2019, 32, 109–121. [Google Scholar] [CrossRef]
- Boersema, G.C.; Smart, H.; Giaquinto-Cilliers, M.G.C.; Mulder, M.; Weir, G.R.; Bruwer, F.A.; Idensohn, P.J.; Sander, J.E.; Stavast, A.; Swart, M.; et al. Management of nonhealable and maintenance wounds: A systematic integrative review and referral pathway. Adv Skin Wound Care 2021, 34, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Edsberg, L.E.; Langemo, D.; Baharestani, M.M.; Posthauer, M.E.; Goldberg, M. Unavoidable pressure injury: State of the science and consensus outcomes. J. Wound Ostomy Cont. Nurs. 2014, 41, 313–334. [Google Scholar] [CrossRef]
- Posnett, J.; Gottrup, F.; Lundgren, H.; Saal, G. The resource impact of wounds on health-care providers in Europe. J. Wound Care 2009, 18, 154–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, M.; Järbrink, K.; Divakar, U.; Bajpai, R.; Upton, Z.; Schmidtchen, A.; Car, J. The humanistic and economic burden of chronic wounds: A systematic review. Wound Repair Regen. 2019, 27, 114–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Probst, S.; Seppänen, S.; Gerber, V.; Hopkins, A.; Rimdeika, R.; Gethin, G. EWMA Document: Home Care-Wound Care. J. Wound Care 2014, 23, S1–S44. [Google Scholar] [CrossRef]
- Gottrup, F. A specialized wound-healing center concept: Importance of a multidisciplinary department structure and surgical treatment facilities in the treatment of chronic wounds. Am. J. Surg. 2004, 187, S38–S43. [Google Scholar] [CrossRef] [PubMed]
- Dowsett, C.; Bielby, A.; Searle, R. Reconciling increasing wound care demands with available resources. J. Wound Care 2014, 23, 552, 554, 556–558. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Servizio Sanitario Nazionale: Cure Domiciliari. Available online: https://www.salute.gov.it/portale/lea/dettaglioContenutiLea.jsp?area=Lea&id=4706&lingua=italiano&menu=socioSanitaria (accessed on 10 November 2022).
- Arnold, N.; Weir, D. Retrospective analysis of healing in wounds cared for by ET nurses versus staff nurses in a home setting. J. Wound Ostomy Cont. Nurs. 1994, 21, 156–160. [Google Scholar] [CrossRef]
- Zarchi, K.; Martinussen, T.; Jemec, G.B. Wound healing and all-cause mortality in 958 wound patients treated in home care. Wound Repair Regen. 2015, 23, 753–758. [Google Scholar] [CrossRef]
- Ferrell, B.A.; Josephson, K.; Norvid, P.; Alcorn, H. Pressure ulcers among patients admitted to home care. J. Am. Geriatr. Soc. 2000, 48, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Artico, M.; D’ Angelo, D.; Piredda, M.; Petitti, T.; Lamarca, L.; De Marinis, M.G.; Dante, A.; Lusignani, M.; Matarese, M. Pressure injury progression and factors associated with different end-points in a home palliative care setting: A retrospective chart review study. J. Pain Symptom Manag. 2018, 56, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieper, B.; Templin, T.N.; Dobal, M.; Jacox, A. Wound prevalence, types, and treatments in home care. Adv. Wound Care 1999, 12, 117–126. [Google Scholar] [PubMed]
- Pieper, B.; Templin, T.; Dobal, M.; Jacox, A. Home care nurses’ ratings of appropriateness of wound treatments and wound healing. J. Wound Ostomy Cont. Nurs. 2002, 29, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Ustrell-Olaria, A.; Amorós-Miró, G. Prevalencia de heridas de la piel en pacientes de atención domiciliaria de 2 áreas básicas de salud de Barcelona: Implicaciones en la práctica enfermera. Enfermería Clínica 2008, 18, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Laible, J.; Mayer, H.; Evers, G.C. Prevalence of ulcus cruris in home care nursing. an epidemiological study in North Rhine-Westphalia. Pflege 2002, 15, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Lanau-Roig, A.; Fabrellas, N.; Sáez-Rubio, G.; Wilson, K. Time of chronic wound healing, as part of a prevalence and incidence study. Enfermería Glob. 2017, 16, 454–463. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, I.; Mégie, M.F. Prevalence of chronic wounds in Quebec home care: An exploratory study. Ostomy Wound Manag. 2006, 52, 46–48, 50, 47–52. [Google Scholar]
- Volpe, C. Lesioni Cutanee Croniche Trattate in Assistenza Domiciliare Integrata. Available online: https://www.epicentro.iss.it/ben/2002/gennaio02/1 (accessed on 10 November 2022).
- Panfil, E.M.; Mayer, H.; Junge, W.; Laible, J.; Lindenberg, E.; Trümner, A.; Wordel, A.; Evers, G.C. Wound management in patients with chronic wounds in ambulatory nursing--a pilot study. Pflege 2002, 15, 169–176. [Google Scholar] [CrossRef] [PubMed]
- García-Sánchez, F.J.; Martínez-Vizcaíno, V.; Rodríguez-Martín, B. Patients’ and caregivers’ conceptualisations of pressure ulcers and the process of decision-making in the context of home care. Int. J. Environ. Res. Public Health 2019, 16, 2719. [Google Scholar] [CrossRef] [PubMed]
- AIUC-Associazione Italiana Ulcere Cutanee (ONLUS). SILP: Studio Italiano Ulcere Da Pressione. Available online: http://www.aiuc.it/pagina/527/progetto+silp (accessed on 10 November 2022).
- Saito, E.; Shirato, M.; Kanagawa, K.; Sagawa, Y.; Nakamura, M. Incidence proportion estimation, prevalence and effective visiting nurse care of pressure ulcers. Nihon Koshu Eisei Zasshi 1999, 46, 1084–1093. [Google Scholar]
- Raeder, K.; Strube-Lahmann, S.; Müller-Werdan, U.; Kottner, J.; Lahmann, N.A.; Suhr, R. Prevalence and influencing factors of chronic wounds among clients of home care services in Germany. Z. Fur Evidenz Fortbild. Und Qual. Im Gesundh. 2019, 140, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, E. Longitudinal outcomes of home care in Korea to manage pressure ulcers. Res. Nurs. Health 2017, 40, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, A.C.; Mota, D.D.; Bachion, M.M.; Ferreira, A.C. Pressure ulcers in palliative home care patients: Prevalence and characteristics. Rev. Esc. Enferm. USP 2014, 48, 264–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sankaran, B.M.; Chakraborty, S.; Patil, V.M.; Raghavan, S.N.; Thomas, S.; Sen, S. Burden and outcomes of pressure ulcers in cancer patients receiving the kerala model of home based palliative care in India: Results from a prospective observational study. Indian J. Palliat. Care 2015, 21, 152–157. [Google Scholar] [CrossRef]
- Téot, L.; Geri, C.; Lano, J.; Cabrol, M.; Linet, C.; Mercier, G. Complex wound healing outcomes for outpatients receiving care via telemedicine, home health, or wound clinic: A randomized controlled trial. Int. J. Low Extrem. Wounds 2020, 19, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Gould, L.; Abadir, P.; Brem, H.; Carter, M.; Conner-Kerr, T.; Davidson, J.; DiPietro, L.; Falanga, V.; Fife, C.; Gardner, S.; et al. Chronic wound repair and healing in older adults: Current status and future research. J. Am. Geriatr. Soc. 2015, 63, 427–438. [Google Scholar] [CrossRef] [Green Version]
- Walker, N.; Rodgers, A.; Birchall, N.; Norton, R.; MacMahon, S. Leg ulcers in New Zealand: Age at onset, recurrence and provision of care in an urban population. N. Z. Med. J. 2002, 115, 286–289. [Google Scholar]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of classification systems in peripheral artery disease. Semin. Interv. Radiol. 2014, 31, 378–388. [Google Scholar] [CrossRef] [Green Version]
- Eklöf, B.; Rutherford, R.B.; Bergan, J.J.; Carpentier, P.H.; Gloviczki, P.; Kistner, R.L.; Meissner, M.H.; Moneta, G.L.; Myers, K.; Padberg, F.T.; et al. Revision of the CEAP classification for chronic venous disorders: Consensus statement. J. Vasc. Surg. 2004, 40, 1248–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santema, T.B.; Lenselink, E.A.; Balm, R.; Ubbink, D.T. Comparing the Meggitt-Wagner and the University of Texas wound classification systems for diabetic foot ulcers: Inter-observer analyses. Int. Wound J. 2016, 13, 1137–1141. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men | Women | All |
|---|---|---|---|
| Subjects with ulcers N (%) | 49 (35.5%) | 89 (64.5%) | 138 (100%) |
| Age, mean (SD) | 83.2 (9.8) | 87.8 (8.9) | 86.1 (9.4) |
| Pressure Ulcers | Other Types of Ulcers | All Ulcers | |||||||
|---|---|---|---|---|---|---|---|---|---|
| S. I | S. II ± I | S. III ± I/II | S. IV ± I/II/III | Unstageable ± I/II/III | All Stages | VU | DFU | ||
| Subjects with ulcers N (%) | 13 (9.4%) | 69 (50%) | 8 (5.8%) | 9 (6.5%) | 8 (5.8%) | 107 (77.5%) | 36 (26.1%) 1 | 10 (7.2%) 2 | 138 (100%) |
| Age, mean (SD) | 87.7 (6.9) | 86.6 (10.3) | 85.4 (5.1) | 92.8 (7.6) | 87.6 (4.3) | 87.2 (9.1) | 85.4 (9.4) | 77.6 (9.6) | 86.1 (9.4) |
| Number N (%) and location of ulcers | |||||||||
| Pelvis and hip | 18 (48.6%) | 58 (54.2%) | 8 (53.3%) | 5 (5.6%) | 2 (20%) | 91 (51.1%) | − | − | 91 (39.2%) |
| Sacrum | 14 (37.8%) | 45 (42.1%) | 6 (40%) | 5 (5.6%) | − | 70 (39.3%) | − | − | 70 (30.2%) |
| Trochanter | 1 (2.7%) | 4 (3.7%) | 1 (6.7%) | − | 2 (20%) | 8 (4.5%) | − | − | 8 (3.5%) |
| Hip | 1 (2.7%) | 2 (1.9%) | − | − | − | 3 (1.7%) | − | − | 3 (1.3%) |
| Groin | 1 (2.7%) | 1 (0.9%) | − | − | − | 2 (1.2%) | − | − | 2 (0.9%) |
| Ischium | 1 (2.7%) | 6 (5.6%) | − | − | − | 7 (3.9%) | − | − | 7 (3%) |
| Other | − | − | 1 (6.7%) | − | − | − | − | − | 1 (0.4%) |
| Foot | 12 (32.4%) | 26 (24.3%) | 5 (33.3%) | 4 (4.4%) | 7 (70%) | 54 (30.3%) | 31 (73.8%) | 11 (100%) | 96 (41.4%) |
| Heel | 8 (21.6%) | 17 (15.9%) | 3 (20%) | 1 (11.1%) | 6 (60%) | 35 (19.7%) | 3 (7.1%) | 2 (18.2%) | 40 (17.2%) |
| Big toe | 2 (5.4%) | 1 (0.9%) | 1 (6.7%) | 1 (11.1%) | 1 (10%) | 6 (3.4%) | 6 (14.3%) | 5 (45.5%) | 17 (7.3%) |
| Malleolus | 1 (2.7%) | 6 (5.6%) | 1 (6.7%) | − | − | 8 (4.5%) | 4 (9.5%) | − | 12 (5.2%) |
| Other toe | − | 1 (0.9%) | − | 1 (11.1%) | − | 2 (1.2%) | 6 (14.3%) | 2 (18.2%) | 10 (4.3%) |
| Other | 1 (2.7%) | 1 (0.9%) | − | 1 (11.1%) | − | 3 (1.7%) | 12 (28.6%) | 2 (18.2%) | 17 (7.3%) |
| Lower limb | 6 (16.2%) | 16 (14.9%) | 2 (13.3%) | − | − | 21 (11.8%) | 11 (26.2%) | − | 32 (13.8%) |
| Gluteus | 4 (14.8%) | 13 (12.1%) | − | − | − | 17 (9.6%) | − | − | 17 (7.3%) |
| Knee | 1 (2.7%) | 1 (0.9%) | 1 (6.7%) | − | − | 2 (1.2%) | − | − | 2 (0.9%) |
| Thigh | − | 1 (0.9%) | − | − | − | 1 (0.6%) | − | − | 1 (0.4%) |
| Calf | − | − | 1 (6.7%) | − | − | 1 (0.6%) | − | − | 1 (0.4%) |
| Other | 1 (2.7%) | 1 (0.9%) | − | − | − | − | 11 (26.2%) | − | 13 (5.6%) |
| Trunk and back | 1 (2.7%) | 7 (6.5%) | − | − | 1 (10%) | 9 (5.1%) | − | − | 9 (3.9%) |
| Total | 37 (100%) (15.9%) † | 107 (100%) (46.1%) † | 15 (100%) (6.5%) † | 9 (100%) (3.9%) † | 10 (100%) (4.3%) † | 178 (100%) (76.7%) † | 42 (100%) (18.1%) † | 11 (100%) (4.7%) † | 232 (100%) (100%) † |
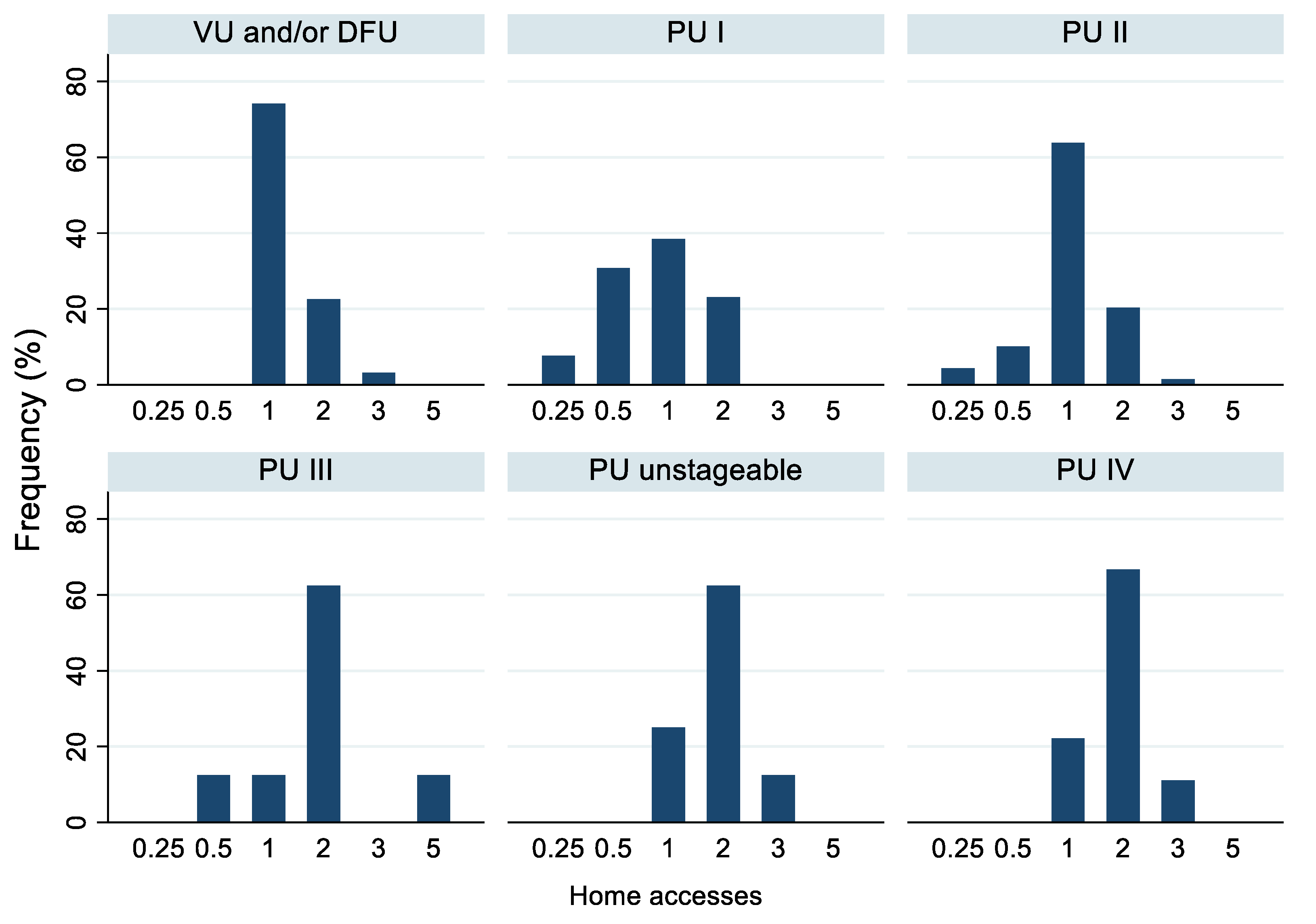
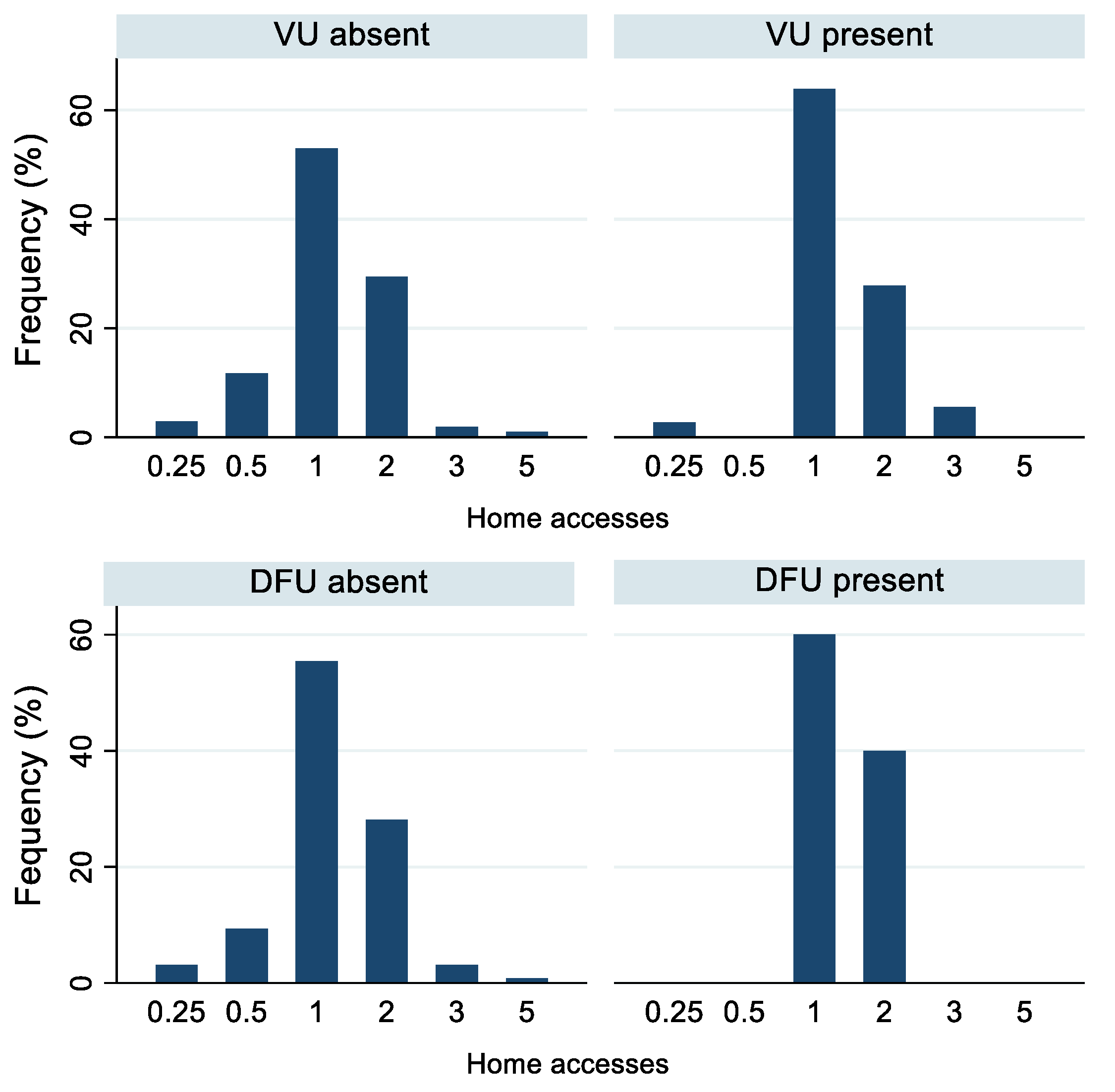
| 1 in 4 Weeks | 1 in 2 Weeks | 1 in a Week | 2 in a Week | 3 in a Week | 5 in a Week | |
|---|---|---|---|---|---|---|
| Ulcer type and stage | ||||||
| PU all stages | 4 (3.7%) | 12 (11.2%) | 54 (50.5%) | 33 (30.8%) | 3 (2.8%) | 1 (0.9%) |
| PU I | 1 (7.7%) | 4 (30.8%) | 5 (38.5%) | 3 (23.1%) | − | − |
| PU II | 3 (4.3%) | 7 (10.1%) | 44 (63.8%) | 14 (20.3%) | 1 (1.5%) | − |
| PU III | − | 1 (12.5%) | 1 (12.5%) | 5 (62.5%) | − | 1 (12.5%) |
| PU IV | − | − | 2 (22.2%) | 6 (66.7%) | 1 (11.1%) | − |
| PU unstageable | − | − | 2 (25.5%) | 5 (62.5%) | 1 (12.5%) | − |
| DFU | − | − | 6 (60%) | 4 (40%) | − | − |
| VU | 1 (2.8%) | − | 23 (63.9%) | 10 (27.8%) | 2 (5.6%) | − |
| Sex | ||||||
| Men | 2 (4.1%) | 2 (4.1%) | 23 (57.1%) | 18 (36.7%) | 3 (6.1%) | 1 (2%) |
| Women | 2 (2.2%) | 10 (11.2%) | 54 (60.7%) | 22 (24.7%) | 1 (1.1%) | − |
| Caregiver | ||||||
| Relative | 3 (4.8%) | 5 (7.9%) | 32 (50.8%) | 21 (33.3%) | 2 (3.2%) | − |
| Relative and professional | − | 4 (14.3%) | 16 (57.1%) | 7 (25%) | − | 1 (3.6%) |
| Not reported | 1 (5.3%) | 1 (5.3%) | 11 (57.9%) | 5 (26.3%) | 1 (5.3%) | − |
| Professional | − | 2 (8%) | 16 (64%) | 6 (24%) | 1 (4%) | − |
| Living alone | − | − | 2 (66.7%) | 1 (33.3%) | − | − |
| Degree of dependence | ||||||
| Partially dependent | 2 (3.8%) | 1 (1.9%) | 33 (63.5%) | 15 (28.8%) | 1 (1.9%) | − |
| Totally dependent | 2 (2.3%) | 11 (12.8%) | 44 (51.2%) | 25 (29.1%) | 3 (3.5%) | 1 (1.2%) |
| Total, N (%) | 4 (2.9%) | 12 (8.7%) | 77 (55.8%) | 40 (29%) | 4 (2.9%) | 1 (0.7%) |
| Characteristics | Partially Dependent | Totally Dependent |
|---|---|---|
| Sex | ||
| Men | 21 (40.4%) | 31 (59.6%) |
| Women | 28 (32.6%) | 58 (67.4%) |
| Type and stage of ulcer | ||
| PU I | 4 (30.8%) | 9 (69.2%) |
| PU II | 26 (37.7%) | 43 (62.3%) |
| PU III | 1 (12.5%) | 7 (87.5%) |
| PU IV | − | 9 (100%) |
| PU unstageable | 1 (12.5%) | 7 (87.5%) |
| PU all stages | 32 (29.9%) | 75 (70.1%) |
| VU | 19 (52.8%) | 17 (47.2%) |
| DFU | 6 (60%) | 4 (40%) |
| Total, N (%) | 49 (35.5%) | 89 (64.5%) |
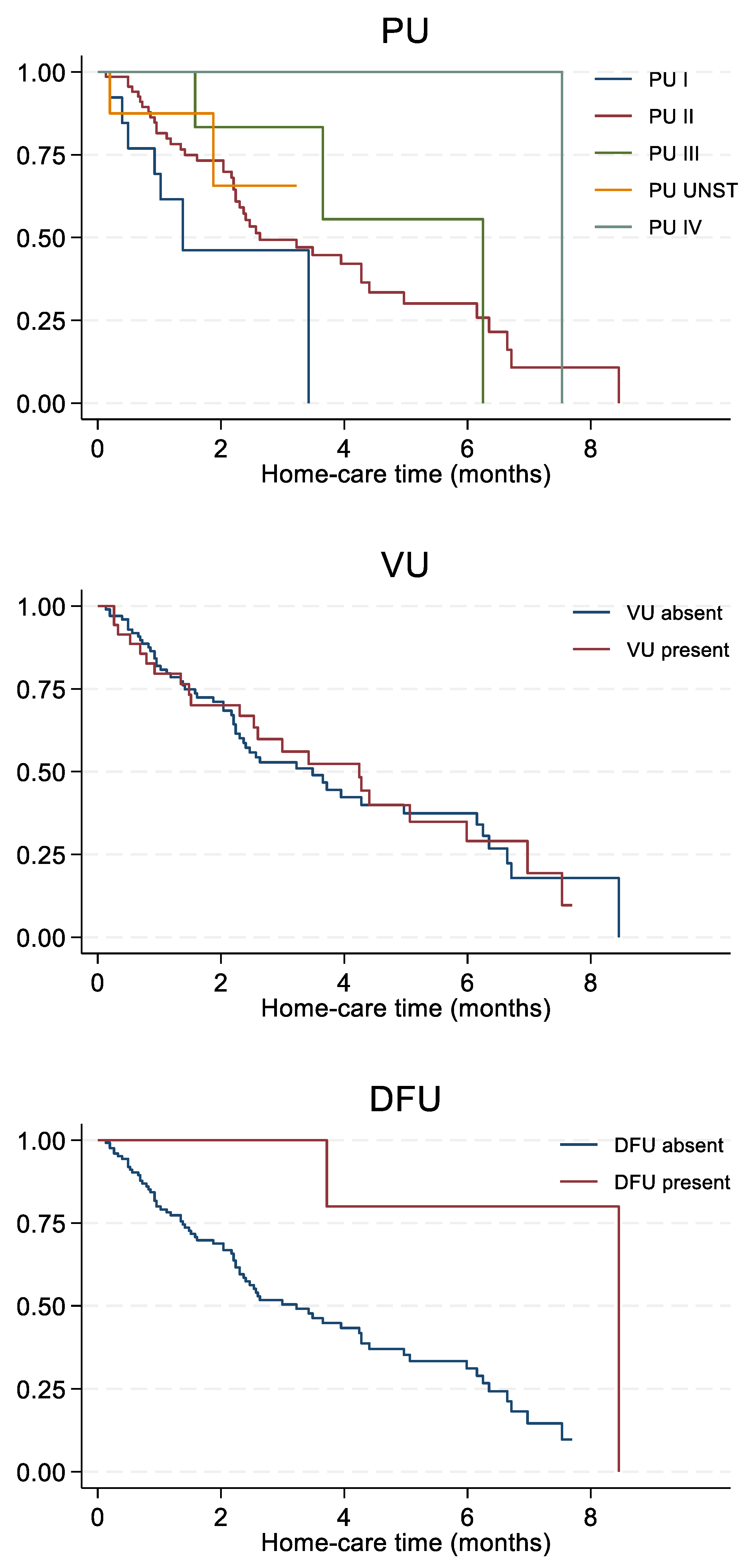
| Still in Care | Recovered | Deceased | Hospitalized | |
|---|---|---|---|---|
| Sex | ||||
| Men | 8 (16.3%) | 24 (49%) (32.4%) ‡ | 15 (30.6%) | 2 (4.1%) |
| Women | 16 (17.8%) | 50 (56.2%) (67.6%) ‡ | 17 (19.1%) | 6 (6.7%) |
| Type and stage of ulcer | ||||
| PU all stages | 17 (15.8%) | 55 (51.4%) (74.3%) ‡ | 30 (28.1%) | 5 (4.7%) |
| PU I | 3 (23.1%) | 7 (53.8%) (9.5%) ‡ | 3 (23.1%) | − |
| PU II | 9 (13%) | 42 (60.9%) (56.8%) ‡ | 17 (24.6%) | 1 (1.5%) |
| PU III | 1 (12.5%) | 3 (37.5%) (4.1%) ‡ | 3 (37.5%) | 1 (12.5%) |
| PU IV | 3 (33.3%) | 1 (11.1%) (1.4%) ‡ | 3 (33.3%) | 2 (22.2%) |
| PU unstageable | 1 (12.5%) | 2 (25%) (2.7%) ‡ | 4 (50%) | 1 (12.5%) |
| VU | 5 (13.9%) | 22 (61.1%) (29.7%) ‡ | 6 (16.7%) | 3 (8.3%) |
| DFU | 3 (30%) | 2 (20%) (2.7%) ‡ | 1 (10%) | 4 (40%) |
| Degree of dependence | ||||
| Partially dependent | 13 (25%) | 31 (59.6%) (41.9%) ‡ | 6 (11.5%) | 2 (3.8%) |
| Totally dependent | 11 (12.8%) | 43 (50%) (58.1%) ‡ | 26 (30.2%) | 6 (7%) |
| Number of home accesses | ||||
| 1 in 4 weeks | 2 (50%) | 2 (50%) (2.7%) ‡ | − | − |
| 1 in 2 weeks | − | 9 (75%) (12.2%) ‡ | 2 (16.7%) | 1 (8.3%) |
| 1 in a week | 10 (13%) | 48 (62.3%) (64.9%) ‡ | 14 (18.2%) | 5 (6.5%) |
| 2 in a week | 11 (27.5%) | 14 (35%) (18.9%) ‡ | 13 (32.5%) | 2 (5%) |
| 3 in a week | 1 (25%) | 1 (25%) (1.4%) ‡ | 2 (50%) | − |
| 5 in a week | − | − | 1 (100%) | − |
| Total, N (%) | 24 (17.4%) | 74 (53.6%) (100%) ‡ | 32 (23.2%) | 8 (5.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iamandii, I.; Kouassi, A.B.; Simonazzi, D.; Marchesi, C.; Vinceti, M.; Filippini, T. Healing Time of Skin Ulcers in Homecare Residents in the Province of Reggio Emilia, Northern Italy. Life 2022, 12, 1989. https://doi.org/10.3390/life12121989
Iamandii I, Kouassi AB, Simonazzi D, Marchesi C, Vinceti M, Filippini T. Healing Time of Skin Ulcers in Homecare Residents in the Province of Reggio Emilia, Northern Italy. Life. 2022; 12(12):1989. https://doi.org/10.3390/life12121989
Chicago/Turabian StyleIamandii, Inga, Abram Beatrice Kouassi, Davide Simonazzi, Cristina Marchesi, Marco Vinceti, and Tommaso Filippini. 2022. "Healing Time of Skin Ulcers in Homecare Residents in the Province of Reggio Emilia, Northern Italy" Life 12, no. 12: 1989. https://doi.org/10.3390/life12121989