
Ischemic Heart Disease in Patients with Inflammatory Bowel Disease: Risk Factors, Mechanisms and Prevention

 , , ,
, , ,
Abstract
:1. Introduction
2. Epidemiological Links between IBD and IHD
Epidemiology
3. Risk Factors for IHD in IBD Patients
3.1. Traditional Cardiovascular Risk Factors
3.2. Risk Factors Related to IBD
3.2.1. Increased IHD with Disease Activity
3.2.2. IBD Treatment
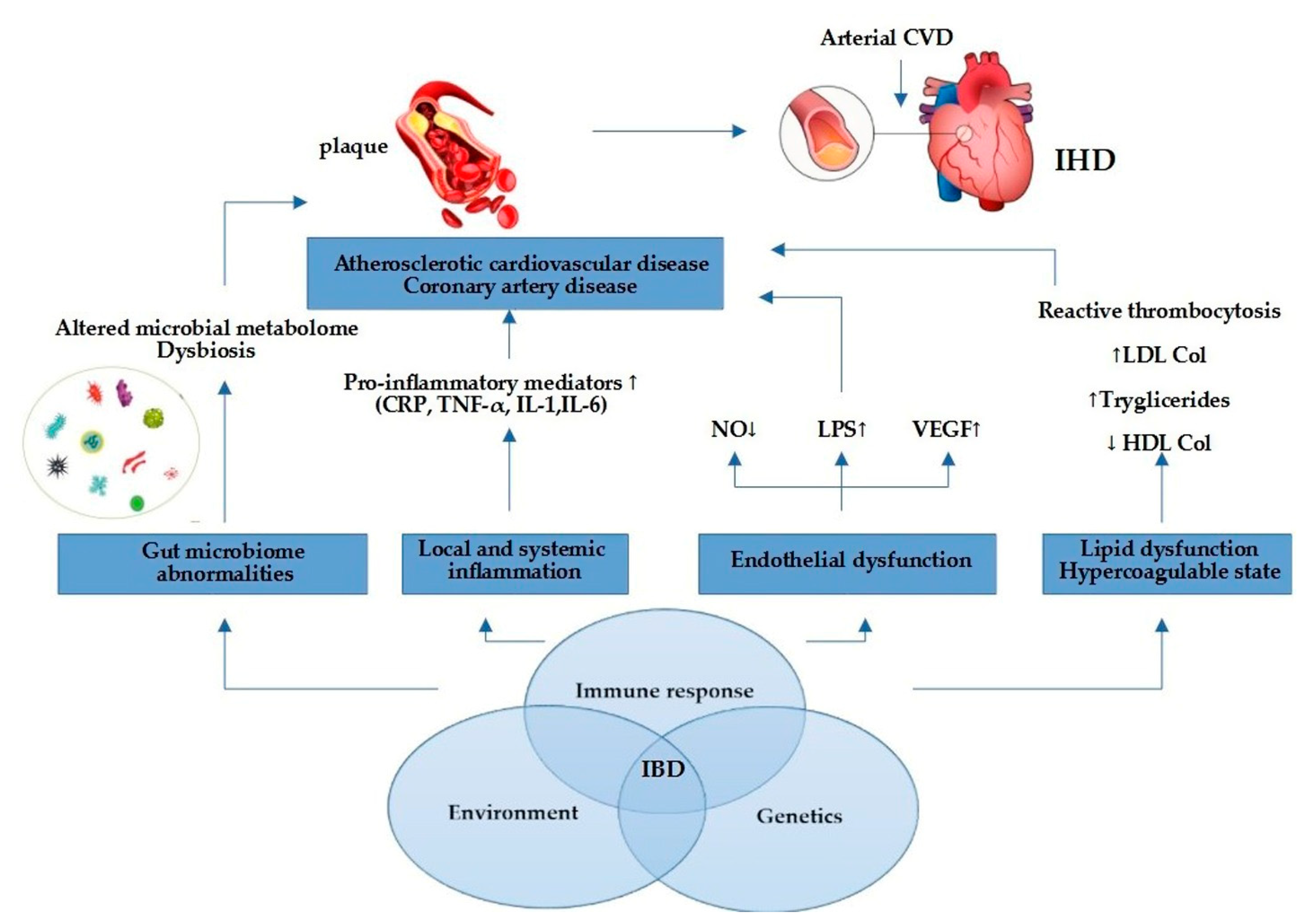
4. Inflammation—The Main Pathogenic Links between IBD and IHD
5. Proposed Strategies for IHD Prevention among IBD Patients
5.1. Traditional Cardiovascular Risk Factors Modification in IBD Patients
5.2. Disease Activity Control
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weissman, S.; Sinh, P.; Mehta, T.I.; Thaker, R.K.; Derman, A.; Heiberger, C.; Qureshi, N.; Amrutiya, V.; Atoot, A.; Dave, M.; et al. Atherosclerotic cardiovascular disease in inflammatory bowel disease: The role of chronic inflammation. World J. Gastrointest. Pathophysiol. 2020, 11, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Seyedian, S.S.; Nokhostin, F.; Malamir, M.D. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Herzog, D.; Fournier, N.; Buehr, P.; Rueger, V.; Koller, R.; Heyland, K.; Nydegger, A.; Spalinger, J.; Schibli, S.; Petit, L.M.; et al. Age at disease onset of inflammatory bowel disease is associated with later extraintestinal manifestations and complications. Eur. J. Gastroenterol. Hepatol. 2018, 30, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Hedin, C.R.H.; Vavricka, S.R.; Stagg, A.J.; Schoepfer, A.; Raine, T.; Puig, L.; Rieder, F. The pathogenesis of extraintestinal manifestations: Implications for IBD research, diagnosis, and therapy. J. Crohn’s Colitis 2019, 13, 541–554. [Google Scholar] [CrossRef]
- Cainzos-Achirica, M.; Glassner, K.; Zawahir, H.S.; Dey, A.K.; Agrawal, T.; Quigley, E.; Abraham, B.P.; Acquah, I.; Yahya, T.; Mehta, N.N.; et al. Inflammatory Bowel Disease and Atherosclerotic Cardiovascular Disease: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 76, 2895–2905. [Google Scholar] [CrossRef]
- Zanoli, L.; Boutouyrie, P.; Fatuzzo, P.; Granata, A.; Lentini, P.; Oztürk, K.; Cappello, M.; Theocharidou, E.; Tuttolomondo, A.; Pinto, A.; et al. Inflammation and Aortic Stiffness: An Individual Participant Data Meta-Analysis in Patients With Inflammatory Bowel Disease. J. Am. Heart Assoc. 2017, 6, e007003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigeh, A.; Sanchez, A.; Maestas, C.; Gulati, M. Inflammatory bowel disease and the risk for cardiovascular disease: Does all inflammation lead to heart disease? Trends Cardiovasc. Med. 2020, 30, 463–469. [Google Scholar] [CrossRef]
- Mitchell, N.E.; Harrison, N.; Junga, Z.; Singla, M. Heart Under Attack: Cardiac Manifestations of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2018, 24, 2322–2326. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Ahlehoff, O.; Lindhardsen, J.; Erichsen, R.; Jensen, G.V.; Torp-Pedersen, C.; Nielsen, O.H.; Gislason, G.H.; Hansen, P.R. Disease activity in inflammatory bowel disease is associated with increased risk of myocardial infarction, stroke and cardiovascular death—A Danish nationwide cohort study. PLoS ONE 2013, 8, e56944. [Google Scholar] [CrossRef]
- Kirchgesner, J.; Beaugerie, L.; Carrat, F.; Andersen, N.N.; Jess, T.; Schwarzinger, M. BERENICE study group. Increased risk of acute arterial events in young patients and severely active IBD: A nationwide French cohort study. Gut 2018, 67, 1261–1268. [Google Scholar] [CrossRef]
- Osterman, M.T.; Yang, Y.X.; Brensinger, C.; Forde, K.A.; Lichtenstein, G.R.; Lewis, J.D. No increased risk of myocardial infarction among patients with ulcerative colitis or Crohn’s disease. Clin. Gastroenterol. Hepatol. 2011, 9, 875–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rungoe, C.; Basit, S.; Ranthe, M.F.; Wohlfahrt, J.; Langholz, E.; Jess, T. Risk of ischaemic heart disease in patients with inflammatory bowel disease: A nationwide Danish cohort study. Gut 2013, 62, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Fumery, M.; Xiaocang, C.; Dauchet, L.; Gower-Rousseau, C.; Peyrin-Biroulet, L.; Colombel, J.F. Thromboembolic events and cardiovascular mortality in inflammatory bowel diseases: A meta-analysis of observational studies. J. Crohn’s Colitis 2014, 8, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Singh, H.; Loftus, E.V.; Pardi, D.S. Risk of cerebrovascular accidents and ischemic heart disease in patients with inflammatory bowel disease: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 382–393. [Google Scholar] [CrossRef]
- Ruisi, P.; Makaryus, J.N.; Ruisi, M.; Makaryus, A.N. Inflammatory bowel disease as a risk factor for premature coronary artery disease. J. Clin. Med. Res. 2015, 7, 257–261. [Google Scholar] [CrossRef] [Green Version]
- Close, H.; Mason, J.M.; Wilson, D.W.; Hungin, A.P.; Jones, R.; Rubin, G. Risk of Ischaemic Heart Disease in Patients with Inflammatory Bowel Disease: Cohort Study Using the General Practice Research Database. PLoS ONE 2015, 10, e0139745. [Google Scholar] [CrossRef] [Green Version]
- McAuliffe, M.E.; Lanes, S.; Leach, T.; Parikh, A.; Faich, G.; Porter, J.; Holick, C.; Esposito, D.; Zhao, Y.; Fox, I. Occurrence of adverse events among patients with inflammatory bowel disease in the Health Core Integrated Research Database. Curr. Med. Res. Opin. 2015, 31, 1655–1664. [Google Scholar] [CrossRef]
- Barnes, E.L.; Beery, R.M.; Schulman, A.R.; McCarthy, E.P.; Korzenik, J.R.; Winter, R.W. Hospitalizations for Acute Myocardial Infarction Are Decreased Among Patients with Inflammatory Bowel Disease Using a Nation wide In patient Database. Inflamm. Bowel Dis. 2016, 22, 2229–2237. [Google Scholar] [CrossRef] [Green Version]
- Feng, W.; Chen, G.; Cai, D.; Zhao, S.; Cheng, J.; Shen, H. Inflammatory Bowel Disease and Risk of Ischemic Heart Disease: An Updated Meta-Analysis of Cohort Studies. J. Am. Heart Assoc. 2017, 6, e005892. [Google Scholar] [CrossRef]
- Le Gall, G.; Kirchgesner, J.; Bejaoui, M.; Landman, C.; Nion-Larmurier, I.; Bourrier, A.; Sokol, H.; Seksik, P.; Beaugerie, L. Clinical activity is an independent risk factor of ischemic heart and cerebrovascular arterial disease in patients with inflammatory bowel disease. PLoS ONE 2018, 13, e0201991. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.H.; Tian, F. Inflammatory bowel disease and cardiovascular disease incidence and mortality: A meta-analysis. Eur. J. Prev. Cardiol. 2018, 25, 1623–1631. [Google Scholar] [CrossRef] [PubMed]
- Panhwar, M.S.; Mansoor, E.; Al-Kindi, S.G.; Sinh, P.; Katz, J.; Oliveira, G.H.; Cooper, G.S.; Ginwalla, M. Risk of myocardial infarction in inflammatory bowel disease: A population-based national study. Inflamm. Bowel Dis. 2019, 25, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Sinh, P.; Tabibian, J.H.; Biyani, P.S.; Mehta, K.; Mansoor, E.; Loftus, E.V.; Dave, M. Inflammatory Bowel Disease Does Not Impact Mortality but Increases Length of Hospitalization in Patients with Acute Myocardial Infarction. Dig. Dis. Sci. 2021, 66, 4169–4177. [Google Scholar] [CrossRef] [PubMed]
- Atzeni, F.; Nucera, V.; Galloway, J.; Zoltán, S.; Nurmohamed, M. Cardiovascular risk in ankylosing spondylitis and the effect of anti-TNF drugs: A narrative review. Expert Opin. Biol. Ther. 2020, 20, 517–524. [Google Scholar] [CrossRef]
- Katta, N.; Loethen, T.; Lavie, C.J.; Alpert, M.A. Obesity and Coronary Heart Disease: Epidemiology, Pathology, and Coronary Artery Imaging. Curr. Probl. Cardiol. 2021, 46, 100655. [Google Scholar] [CrossRef]
- Singh, S.; Dulai, P.S.; Zarrinpar, A.; Ramamoorthy, S.; Sandborn, W.J. Obesity in IBD: Epidemiology, pathogenesis, disease course and treatment outcomes. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 110–121. [Google Scholar] [CrossRef] [Green Version]
- Seminerio, J.L.; Koutroubakis, I.E.; Ramos-Rivers, C.; Hashash, J.G.; Dudekula, A.; Regueiro, M.; Baidoo, L.; Barrie, A.; Swoger, J.; Schwartz, M.; et al. Impact of Obesity on the Management and Clinical Course of Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2015, 21, 2857–2863. [Google Scholar] [CrossRef] [Green Version]
- Hu, Q.; Ren, J.; Li, G.; Wu, X.; Li, J. The Impact of Obesity on the Clinical Course of Inflammatory Bowel Disease: A Meta-Analysis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 2599–2606. [Google Scholar] [CrossRef] [Green Version]
- Jess, T.; Jensen, B.W.; Andersson, M.; Villumsen, M.; Allin, K.H. Inflammatory Bowel Diseases Increase Risk of Type 2 Diabetes in a Nationwide Cohort Study. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2020, 18, 881–888.e1. [Google Scholar] [CrossRef]
- Kumar, A.; Teslova, T.; Taub, E.; Miller, J.D.; Lukin, D.J. Comorbid Diabetes in Inflammatory Bowel Disease Predicts Adverse Disease-Related Outcomes and Infectious Complications. Dig. Dis. Sci. 2021, 66, 2005–2013. [Google Scholar] [CrossRef]
- Michalak, A.; Mosińska, P.; Fichna, J. Common links between metabolic syndrome and inflammatory bowel disease: Current overview and future perspectives. Pharmacol. Rep. PR 2016, 68, 837–846. [Google Scholar] [CrossRef]
- Golovics, P.A.; Verdon, C.; Wetwittayakhlang, P.; Filliter, C.; Gonczi, L.; Hahn, G.D.; Wild, G.E.; Afif, W.; Bitton, A.; Bessissow, T.; et al. Increased Prevalence of Myocardial Infarction and Stable Stroke Proportions in Patients with Inflammatory Bowel Diseases in Quebec in 1996–2015. J. Clin. Med. 2022, 11, 686. [Google Scholar] [CrossRef] [PubMed]
- Correia, P.; Machado, S.; Meyer, I.; Amiguet, M.; Eskandari, A.; Michel, P. Ischemic stroke on hormonal contraceptives: Characteristics, mechanisms and outcome. Eur. Stroke J. 2021, 6, 205–212. [Google Scholar] [CrossRef]
- Card, T.R.; Zittan, E.; Nguyen, G.C.; Grainge, M.J. Disease activity in inflammatory bowel disease is associated with arterial vascular disease. Inflamm. Bowel Dis. 2021, 27, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Agca, R.; Smulders, Y.; Nurmohamed, M. Cardiovascular disease risk in immune-mediated inflammatory diseases: Recommendations for clinical practice. Heart 2022, 108, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Sleutjes, J.; van Lennep, J.; van der Woude, C.J.; de Vries, A.C. Thromboembolic and atherosclerotic cardiovascular events in inflammatory bowel disease: Epidemiology, pathogenesis and clinical management. Ther. Adv. Gastroenterol. 2021, 14, 17562848211032126. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.D.; Scott, F.I.; Brensinger, C.M.; Roy, J.A.; Osterman, M.T.; Mamtani, R.; Bewtra, M.; Chen, L.; Yun, H.; Xie, F.; et al. Increased mortality rates with prolonged corticosteroid therapy when compared with antitumor necrosis factor-α-directed therapy for inflammatory bowel disease. Am. J. Gastroenterol. 2018, 113, 405–417. [Google Scholar] [CrossRef] [Green Version]
- Jaaouani, A.; Ismaiel, A.; Popa, S.-L.; Dumitrascu, D.L. Acute Coronary Syndromes and Inflammatory Bowel Disease: The Gut–Heart Connection. J. Clin. Med. 2021, 10, 4710. [Google Scholar] [CrossRef]
- Kirchgesner, J.; Nyboe Andersen, N.; Carrat, F.; Jess, T.; Beaugerie, L.; BERENICE Study Group. Risk of acute arterial events associated with treatment of inflammatory bowel diseases: Nationwide French cohort study. Gut 2020, 69, 852–858. [Google Scholar] [CrossRef]
- Paschou, S.A.; Kothonas, F.; Lafkas, A.; Myroforidis, A.; Loi, V.; Terzi, T.; Karagianni, O.; Poulou, A.; Goumas, K.; Vryonidou, A. Favorable effect of anti-TNF therapy on insulin sensitivity in nonobese, nondiabetic patients with inflammatory bowel disease. Int. J. Endocrinol. 2018, 2018, 6712901. [Google Scholar] [CrossRef] [Green Version]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68 (Suppl. S3), s1–s106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soysal, P.; Arik, F.; Smith, L.; Jackson, S.E.; Isik, A.T. Inflammation, frailty and cardiovascular disease. Adv. Exp. Med. Biol. 2020, 1216, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppkes, M.; Neurath, M.F. Cytokines in inflammatory bowel diseases—Update 2020. Pharmacol. Res. 2020, 158, 104835. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Liu, J.; Li, C.; Gao, J.; Li, X.; Chen, S.; Wu, S.; Ding, H.; Fan, H.; Hou, S. Cumulative exposure to high-sensitivity C-reactive protein predicts the risk of cardiovascular disease. J. Am. Heart Assoc. 2017, 6, e005610. [Google Scholar] [CrossRef]
- Tousoulis, D.; Oikonomou, E.; Economou, E.K.; Crea, F.; Kaski, J.C. Inflammatory cytokines in atherosclerosis: Current therapeutic approaches. Eur. Heart J. 2016, 37, 1723–1732. [Google Scholar] [CrossRef] [Green Version]
- Falloon, K.A.; Fiocchi, C. Current Therapy in Inflammatory Bowel Disease: Why and How We Need to Change? EMJ Innov. 2021, 6, 40–49. [Google Scholar] [CrossRef]
- Cibor, D.; Domagala-Rodacka, R.; Rodacki, T.; Jurczyszyn, A.; Mach, T.; Owczarek, D. Endothelial dysfunction in inflammatory bowel diseases: Pathogenesis, assessment and implications. World J. Gastroenterol. 2016, 22, 1067–1077. [Google Scholar] [CrossRef]
- Alkim, C.; Alkim, H.; Koksal, A.R.; Boga, S.; Sen, I. Angiogenesis in Inflammatory Bowel Disease. Int. J. Inflamm. 2015, 2015, 970890. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Jia, F.; Zhang, B.; Zhang, P. Risk of cardiovascular disease in inflammatory bowel disease. Exp. Ther. Med. 2017, 13, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S.S.; Wang, J.; Yannie, P.J.; Ghosh, S. Intestinal Barrier Dysfunction, LPS Translocation, and Disease Development. J. Endocr. Soc. 2020, 4, bvz039. [Google Scholar] [CrossRef] [Green Version]
- Kamperidis, N.; Kamperidis, V.; Zegkos, T.; Kostourou, I.; Nikolaidou, O.; Arebi, N.; Karvounis, H. Atherosclerosis and Inflammatory Bowel Disease-Shared Pathogenesis and Implications for Treatment. Angiology 2021, 72, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Kakuta, K.; Dohi, K.; Yamamoto, T.; Fujimoto, N.; Shimoyama, T.; Umegae, S.; Ito, M. Coronary Microvascular Dysfunction Restored After Surgery in Inflammatory Bowel Disease: A Prospective Observational Study. J. Am. Heart Assoc. 2021, 10, e019125. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Shi, R.; Mao, T.; Wang, Z.; Sun, Z.; Tan, X.; Wang, Y.; Li, J. Arterial Stiffness in Inflammatory Bowel Disease: An Updated Systematic Review and Meta-Analysis. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2021, 32, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Pepe, M.; Carulli, E.; Forleo, C.; Moscarelli, M.; Di Cillo, O.; Bortone, A.S.; Nestola, P.L.; Biondi-Zoccai, G.; Giordano, A.; Favale, S. Inflammatory Bowel Disease and Acute Coronary Syndromes: From Pathogenesis to the Fine Line Between Bleeding and Ischemic Risk. Inflamm. Bowel Dis. 2021, 27, 725–731. [Google Scholar] [CrossRef]
- Vanuytsel, T.; Tack, J.; Farre, R. The Role of Intestinal Permeability in Gastrointestinal Disorders and Current Methods of Evaluation. Front. Nutr. 2021, 8, 717925. [Google Scholar] [CrossRef]
- Steyers, C.M., III; Miller, F.J., Jr. Endothelial Dysfunction in Chronic Inflammatory Diseases. Int. J. Mol. Sci. 2014, 15, 11324–11349. [Google Scholar] [CrossRef] [Green Version]
- Lorey, M.B.; Öörni, K.; Kovanen, P.T. Modified Lipoproteins Induce Arterial Wall Inflammation During Atherogenesis. Front. Cardiovasc. Med. 2022, 9, 841545. [Google Scholar] [CrossRef]
- Biondi, R.B.; Salmazo, P.S.; Bazan, S.; Hueb, J.C.; de Paiva, S.; Sassaki, L.Y. Cardiovascular Risk in Individuals with Inflammatory Bowel Disease. Clin. Exp. Gastroenterol. 2020, 13, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.T.; Mahtta, D.; Chen, L.; Hussain, A.; Al Rifai, M.; Sinh, P.; Khalid, U.; Nasir, K.; Ballantyne, C.M.; Petersen, L.A.; et al. Premature Atherosclerotic Cardiovascular Disease Risk Among Patients with Inflammatory Bowel Disease. Am. J. Med. 2021, 134, 1047–1051.e2. [Google Scholar] [CrossRef]
- Dineen-Griffin, S.; Garcia-Cardenas, V.; Williams, K.; Benrimoj, S.I. Helping patients help themselves: A systematic review of self-management support strategies in primary health care practice. PLoS ONE 2019, 14, e0220116. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Hu, T.; Hao, H.; Hill, A.M.; Xu, C.; Liu, Z. Inflammatory bowel disease and cardiovascular diseases: A concise review. Eur. Heart J. Open 2022, 2, oeab029. [Google Scholar] [CrossRef]
- Harris, S.K.; Roos, M.G.; Landry, G.J. Statin use in patients with peripheral arterial disease. J. Vasc. Surg. 2016, 64, 1881–1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lochhead, P.; Khalili, H.; Sachs, M.C.; Chan, A.T.; Olén, O.; Ludvigsson, J.F. Association Between Statin Use and Inflammatory Bowel Diseases: Results from a Swedish, Nationwide, Population-based Case-control Study. J. Crohn’s Colitis 2021, 15, 757–765. [Google Scholar] [CrossRef]
- Czubkowski, P.; Osiecki, M.; Szymańska, E.; Kierkuś, J. The risk of cardiovascular complications in inflammatory bowel disease. Clin. Exp. Med. 2020, 20, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Harbord, M.; Annese, V.; Vavricka, S.R.; Allez, M.; Barreiro-de Acosta, M.; Boberg, K.M.; Burisch, J.; De Vos, M.; De Vries, A.M.; Dick, A.D.; et al. European Crohn’s and Colitis Organisation. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. J. Crohn’s Colitis 2016, 10, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Olivera, P.A.; Zuily, S.; Kotze, G.K.; Regnault, V.; Al Awadhi, S.; Bossuyt, P.; Gearry, R.B.; Ghosh, S.; Kobayashi, T.; Lacolley, P.; et al. International consensus on the prevention of venous and arterial thrombotic events in patients with inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2018, 18, 857–873. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year of Publication | Type of Study | Study Showing the Association between IBD and IHD | Conclusion |
|---|---|---|---|---|
| Osterman et al. [11] | 2011 | Retrospective cohort study | No | IBD patients did not appear to be at elevated risk of early MI when compared with patients from general practice. |
| Rungoe et al. [12] | 2013 | Cohort study | Positive | People diagnosed with IBD were compared with IBD-free individuals during 1997–2009 (n = 28,833). The risk of IHD was highest in the first year after IBD diagnosis (IRR = 2.13). The risk of IHD was 1.22 during 1–13 years of follow-up after IBD diagnosis. |
| Kristensen et al. [9] | 2013 | Cohort study | Positive | IBD patients had an increased total risk of MI (RR, 1.17 [95% confidence interval 1.05–1.31]). During periods of persistent IBD activity the RRs of MI increased to 1.49 (1.16–1.93). In remission periods, the risk of MI was similar to controls. |
| Fumery et al. [13] | 2014 | Meta-analysis | Positive | The study found an increased risk of IHD (RR, 1.23; 95% CI, 0.94–1.62). Cardiovascular mortality in patients with IBD compared to general population was not increased. |
| Singh et al. [14] | 2014 | Meta-analysis | Positive | There has been a modest increase in the risk of CV morbidity due to IHD, particularly in women. |
| Ruisi et al. [15] | 2015 | Cohort study | No | The study did not show an association with IBD and premature CV events in a cohort of 300 patients with IBD without traditional risk factors for CV disease. |
| Close et al. [16] | 2015 | Retrospective cohort study | Positive | A higher proportion of IBD patients were diagnosed with IHD: 2220 (11.6%) compared with 6504 (8.6%) of controls. Most IHD diagnoses predated the diagnosis of IBD. Patients with UC had a higher risk of IHD (unadjusted HR 1.3 (95% CI 1.1–1.5), p < 0.001) or MI (unadjusted HR 1.4 (95% CI 1.1–1.6), p = 0.004). |
| McAuliffe et al. [17] | 2015 | Retrospective cohort study | Positive | Patients with moderate to severe IBD had increased rates of MI vs. patients with mild IBD. |
| Barnes et al. [18] | 2016 | Retrospective cross-sectional study | No | Patients with IBD demonstrated lower rates of acute MI than in the general population (1.3% vs. 3.1%, p < 0.001). |
| Feng et al. [19] | 2017 | Meta-analysis | Positive | Increased risk of IHD in IBD patients (RR, 1.244; 95% CI, 1.142–1.355). Increased risk in CD (RR, 1.243; 95% CI, 1.042–1.482) compared to UC (RR, 1.206; 95% CI, 1.170–1.242). |
| Le Gall et al. [20] | 2018 | Cohort Study | Positive | Occurrence of AAE (acute coronary syndrome). Disease activity may increase the risk of AAE. |
| Sun et al. [21] | 2018 | Meta-analysis | Positive | Higher risk of MI in women with IBD than in men; inflammation seems to play a more important role in CV disease in women than in men. |
| Kirchgesner et al. [10] | 2018 | Cohort study | Positive | IBD patients are at increased risk of AAE—SIR 1.35, with the highest risk in young patients. |
| Panhwar et al. [22] | 2019 | Cohort study | Positive | The prevalence of MI was higher in patients with UC and CD than in patients without IBD (UC 6.7% vs. CD 8.8% vs. non-IBD 3.3%). The relative risk of MI was associated with a higher rate in younger patients, and decreased with age. |
| Sinh et al. [23] | 2021 | Retrospective cross-sectional study | No | The study showed no difference between in-hospital mortality in patients with MI with or without UC (7.75% vs. 7.05%; p = 0.25) or in patients with MI with or without CD (6.50% vs. 6.59%; p = 0.87). Patients with MI with IBD had a longer length of stay. |
| Guideline | Recommendation |
|---|---|
| ECCO, 2015 [65] The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. |
|
| International consensus on the prevention of venous and arterial thrombotic events in patients with inflammatory bowel disease, 2021 [66]. |
|
| 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes [67]. |
|
| 2019 ACC/AHA guidelines [68]. |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jucan, A.E.; Gavrilescu, O.; Dranga, M.; Popa, I.V.; Mihai, B.M.; Prelipcean, C.C.; Mihai, C. Ischemic Heart Disease in Patients with Inflammatory Bowel Disease: Risk Factors, Mechanisms and Prevention. Life 2022, 12, 1113. https://doi.org/10.3390/life12081113
Jucan AE, Gavrilescu O, Dranga M, Popa IV, Mihai BM, Prelipcean CC, Mihai C. Ischemic Heart Disease in Patients with Inflammatory Bowel Disease: Risk Factors, Mechanisms and Prevention. Life. 2022; 12(8):1113. https://doi.org/10.3390/life12081113
Chicago/Turabian StyleJucan, Alina Ecaterina, Otilia Gavrilescu, Mihaela Dranga, Iolanda Valentina Popa, Bogdan Mircea Mihai, Cristina Cijevschi Prelipcean, and Cătălina Mihai. 2022. "Ischemic Heart Disease in Patients with Inflammatory Bowel Disease: Risk Factors, Mechanisms and Prevention" Life 12, no. 8: 1113. https://doi.org/10.3390/life12081113