
Intramedullary Spinal Cord Metastases from Differentiated Thyroid Cancer, a Case Report

 ,
,  and
and 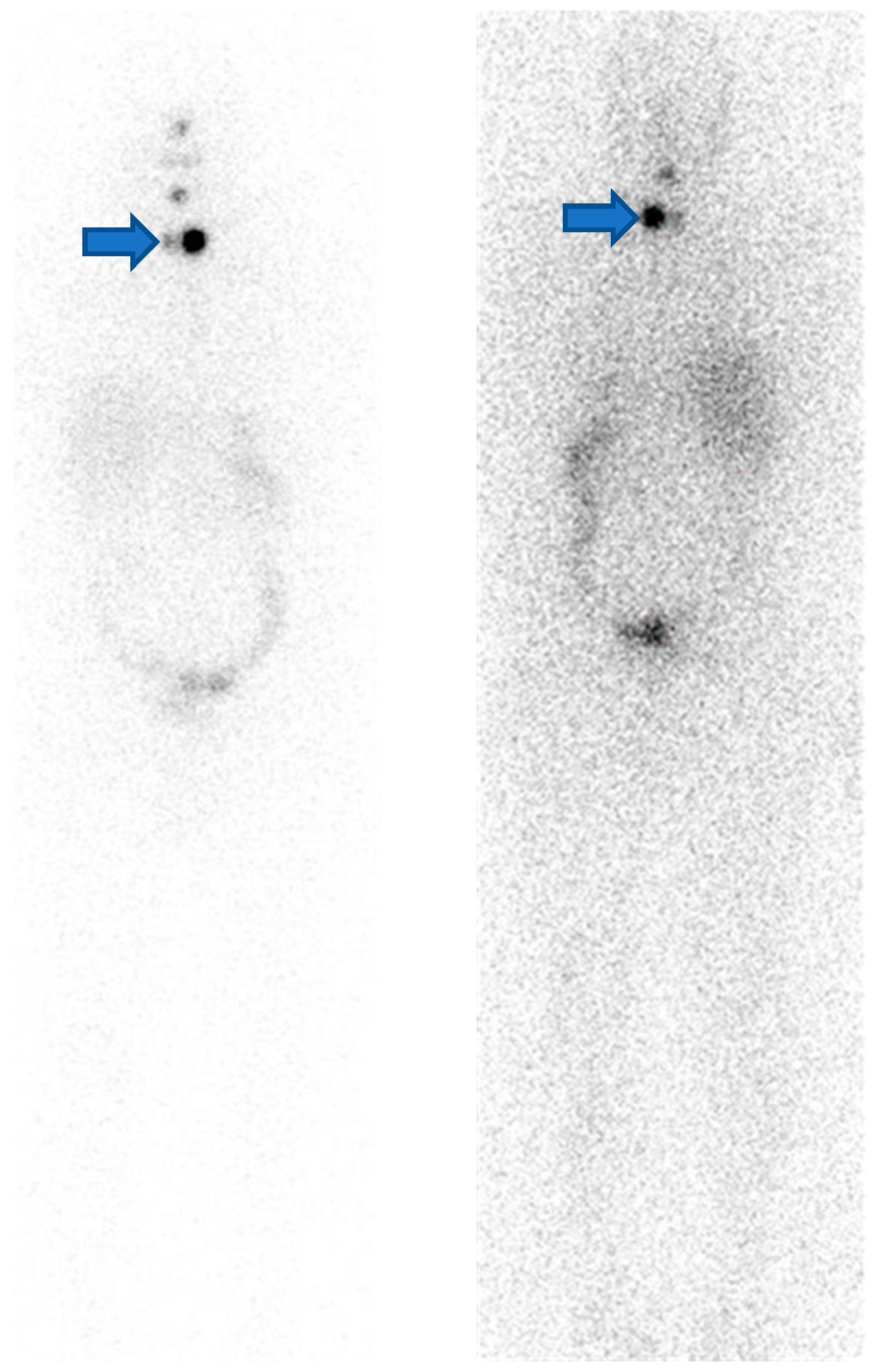{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
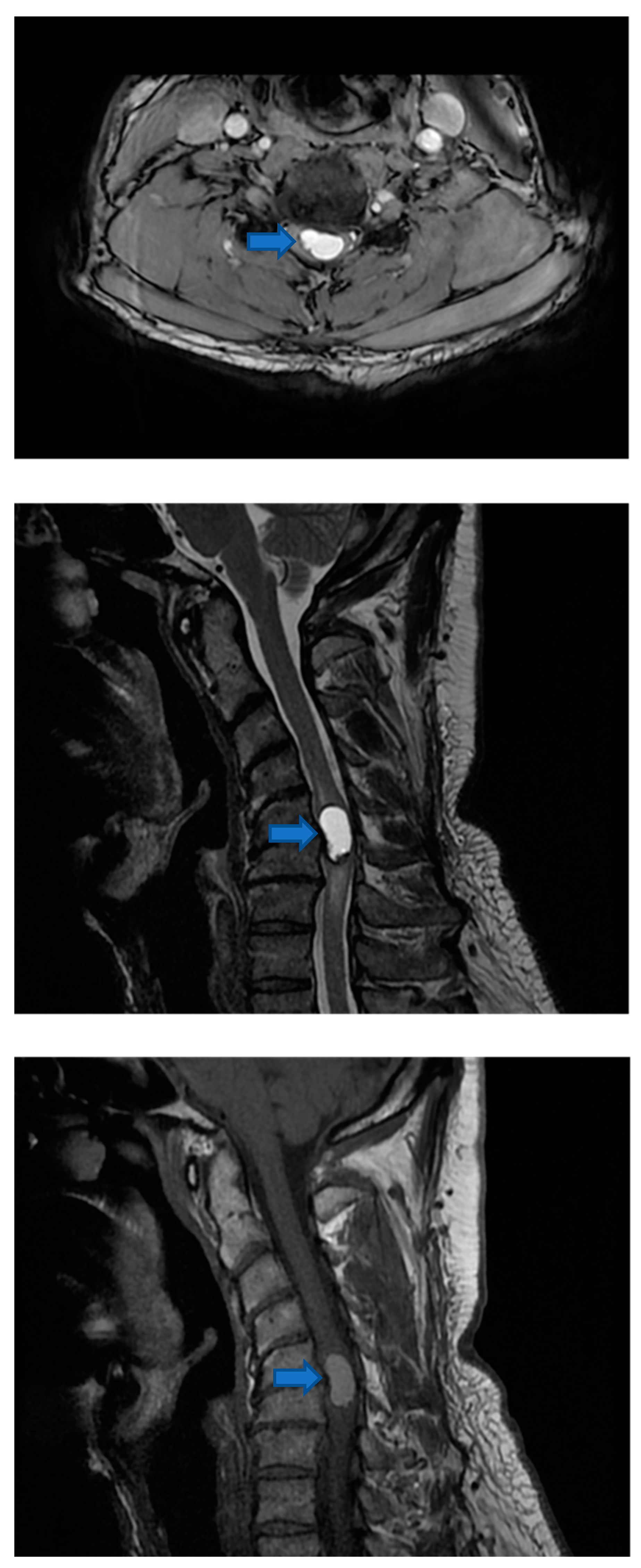
2.1. Pre-Surgical Intervention Imaging
2.2. Surgery
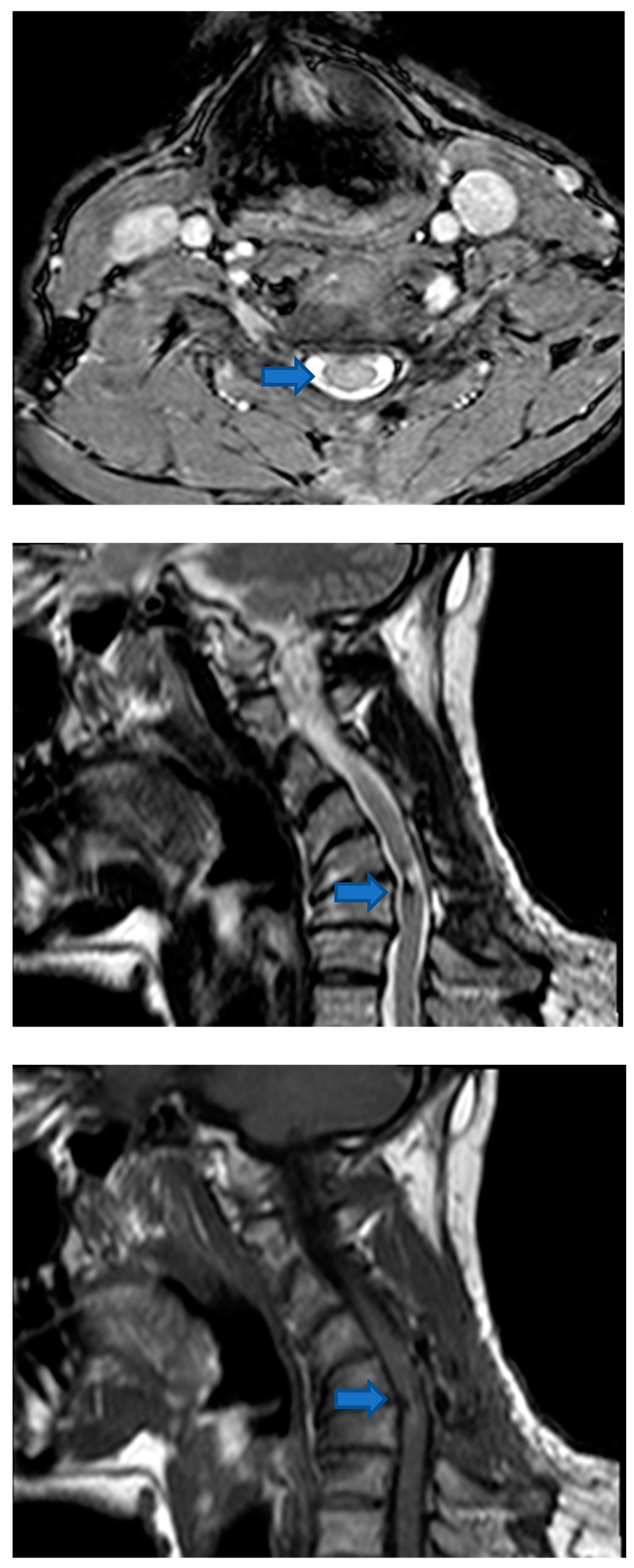
2.3. Post-Surgical Intervention Imaging
3. Discussion
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Grasso, G.; Meli, F.; Patti, R.; Giambartino, F.; Florena, A.M.; Iacopino, D.G. Intramedullary spinal cord tumor presenting as the initial manifestation of metastatic colon cancer: Case report and review of the literature. Spinal Cord 2007, 45, 793–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.S.; Kim, M.K.; Sym, S.J.; Kim, S.W.; Kim, W.K.; Kim, S.-B.; Ahn, J.-H. Intramedullary spinal cord metastases: A single-institution experience. J. Neurooncol. 2007, 84, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Mut, M.; Schiff, D.; Shaffrey, M.E. Metastasis to nervous system: Spinal epidural and intramedullary metastases. J. Neurooncol. 2005, 75, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, W.B.; Perrin, R.G. Evaluation and treatment of spinal metastases: An overview. Neurosurg. Focus 2001, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Diehn, F.E.; Rykken, J.B.; Wald, J.T.; Wood, C.P.; Eckel, L.J.; Hunt, C.H.; Schwartz, K.M.; Lingineni, R.K.; Carter, R.E.; Kaufmann, T.J. Intramedullary Spinal Cord Metastases: Prognostic Value of MRI and Clinical Features from a 13-Year Institutional Case Series. AJNR Am. J. Neuroradiol. 2015, 36, 587–593. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.Q. Nervous System Metastases From Systemic Cancer. Contin. Lifelong Learn. Neurol. 2015, 21, 415. [Google Scholar] [CrossRef]
- Schiff, D.; O’Neill, B.P. Intramedullary spinal cord metastases: Clinical features and treatment outcome. Neurology 1996, 47, 906–912. [Google Scholar] [CrossRef]
- Dunne, J.W.; Harper, C.G.; Pamphlett, R. Intramedullary spinal cord metastases: A clinical and pathological study of nine cases. Q. J. Med. 1986, 61, 1003–1020. [Google Scholar]
- Fakih, M.; Schiff, D.; Erlich, R.; Logan, T. Intramedullary spinal cord metastasis (ISCM) in renal cell carcinoma: A series of six cases. Ann. Oncol. 2001, 12, 1173–1177. [Google Scholar] [CrossRef]
- Asad, S.; Sher, I.; Peters-Willke, J.; Jessup, P. Neurotropic cutaneous malignant melanoma with contiguous spread to spinal cord, an extremely rare presentation. J. Spine Surg. 2016, 2, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Minomo, S.; Tokoro, A.; Utsumi, T.; Ishihara, M.; Akira, M.; Atagi, S. A case of long-term survival after multimodal local treatments of intramedullary spinal cord metastasis of squamous cell lung cancer. J. Thorac. Dis. 2016, 8, E681–E683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hrabalek, L. Intramedullary spinal cord metastases: Review of the literature. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czechoslov. 2010, 154, 117–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasko, V.V.; Saji, M. Molecular mechanisms involved in differentiated thyroid cancer invasion and metastasis. Curr. Opin. Oncol. 2007, 19, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.M.L.; Niu, T.; Zerfaoui, M.; Kunnimalaiyaan, M.; Friedlander, P.L.; Abdel-Mageed, A.B.; Kandil, E. A novel gene panel for prediction of lymph-node metastasis and recurrence in patients with thyroid cancer. Surgery 2020, 167, 73–79. [Google Scholar] [CrossRef]
- Janjua, N.; Wreesmann, V.B. Aggressive differentiated thyroid cancer. Eur. J. Surg. Oncol. 2018, 44, 367–377. [Google Scholar] [CrossRef]
- Xie, J.; Fan, Y.; Zhang, X. Molecular mechanisms in differentiated thyroid cancer. Front. Biosci. Landmark Ed. 2016, 21, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Veschi, V.; Verona, F.; Lo Iacono, M.; D’Accardo, C.; Porcelli, G.; Turdo, A.; Gaggianesi, M.; Forte, S.; Giuffrida, D.; Memeo, L.; et al. Cancer Stem Cells in Thyroid Tumors: From the Origin to Metastasis. Front. Endocrinol. 2020, 11, 566. [Google Scholar] [CrossRef]
- McKelvey, B.A.; Umbricht, C.B.; Zeiger, M.A. Telomerase Reverse Transcriptase (TERT) Regulation in Thyroid Cancer: A Review. Front. Endocrinol. 2020, 11, 485. [Google Scholar] [CrossRef]
- Bournaud, C.; Descotes, F.; Decaussin-Petrucci, M.; Berthiller, J.; de la Fouchardière, C.; Giraudet, A.-L.; Bertholon-Gregoire, M.; Robinson, P.; Lifante, J.-C.; Lopez, J.; et al. TERT promoter mutations identify a high-risk group in metastasis-free advanced thyroid carcinoma. Eur. J. Cancer 2019, 108, 41–49. [Google Scholar] [CrossRef]
- de la Fouchardière, C.; Decaussin-Petrucci, M.; Berthiller, J.; Descotes, F.; Lopez, J.; Lifante, J.-C.; Peix, J.-L.; Giraudet, A.-L.; Delahaye, A.; Masson, S.; et al. Predictive factors of outcome in poorly differentiated thyroid carcinomas. Eur. J. Cancer 2018, 92, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Celik, M.; Bulbul, B.Y.; Ayturk, S.; Durmus, Y.; Gurkan, H.; Can, N.; Tastekin, E.; Ustun, F.; Sezer, A.; Guldiken, S. The relation between BRAFV600E mutation and clinicopathological characteristics of papillary thyroid cancer. Med. Glas. 2020, 17, 30–34. [Google Scholar] [CrossRef]
- Sabra, M.M.; Dominguez, J.M.; Grewal, R.K.; Larson, S.M.; Ghossein, R.A.; Tuttle, R.M.; Fagin, J.A. Clinical outcomes and molecular profile of differentiated thyroid cancers with radioiodine-avid distant metastases. J. Clin. Endocrinol. Metab. 2013, 98, E829–E836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dabravolski, S.A.; Nikiforov, N.G.; Zhuravlev, A.D.; Orekhov, N.A.; Mikhaleva, L.M.; Orekhov, A.N. The Role of Altered Mitochondrial Metabolism in Thyroid Cancer Development and Mitochondria-Targeted Thyroid Cancer Treatment. Int. J. Mol. Sci. 2021, 23, 460. [Google Scholar] [CrossRef] [PubMed]
- Ely, K.A.; Bischoff, L.A.; Weiss, V.L. Wnt Signaling in Thyroid Homeostasis and Carcinogenesis. Genes 2018, 9, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Wang, X.; Gong, Y.; Deng, J. E-cadherin on epithelial–mesenchymal transition in thyroid cancer. Cancer Cell Int. 2021, 21, 695. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, H.; Guan, H.; Ke, W.; Liang, W.; Xiao, H.; Li, Y. Dermatopontin inhibits papillary thyroid cancer cell proliferation through MYC repression. Mol. Cell. Endocrinol. 2019, 480, 122–132. [Google Scholar] [CrossRef]
- Hoshino, A.; Costa-Silva, B.; Shen, T.-L.; Rodrigues, G.; Hashimoto, A.; Mark, M.T.; Molina, H.; Kohsaka, S.; Di Giannatale, A.; Ceder, S.; et al. Tumour exosome integrins determine organotropic metastasis. Nature 2015, 527, 329–335. [Google Scholar] [CrossRef] [Green Version]
- Wanleenuwat, P.; Iwanowski, P. Metastases to the central nervous system: Molecular basis and clinical considerations. J. Neurol. Sci. 2020, 412, 116755. [Google Scholar] [CrossRef]
- Dillon, W.P. Magnetic resonance imaging of head and neck tumors. Cardiovasc. Interv. Radiol. 1986, 8, 275–282. [Google Scholar] [CrossRef]
- Edwards, M.K. Magnetic resonance imaging of the head and neck. Dent. Clin. N. Am. 1993, 37, 591–611. [Google Scholar] [CrossRef]
- Klain, M.; Nappi, C.; Nicolai, E.; Romeo, V.; Piscopo, L.; Giordano, A.; Gaudieri, V.; Zampella, E.; Pace, L.; Carlo, C.; et al. Comparison of simultaneous 18F-2-[18F] FDG PET/MR and PET/CT in the follow-up of patients with differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 3066–3073. [Google Scholar] [CrossRef] [PubMed]
- Zampella, E.; Klain, M.; Pace, L.; Cuocolo, A. PET/CT in the management of differentiated thyroid cancer. Diagn. Interv. Imaging 2021, 102, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Blum, M.; Tiu, S.; Chu, M.; Goel, S.; Friedman, K. I-131 SPECT/CT Elucidates Cryptic Findings on Planar Whole-Body Scans and Can Reduce Needless Therapy with I-131 in Post-Thyroidectomy Thyroid Cancer Patients. Thyroid 2011, 21, 1235–1247. [Google Scholar] [CrossRef]
- Jeong, S.Y.; Lee, S.-W.; Kim, H.W.; Song, B.-I.; Ahn, B.-C.; Lee, J. Clinical applications of SPECT/CT after first I-131 ablation in patients with differentiated thyroid cancer. Clin. Endocrinol. (Oxf.) 2014, 81, 445–451. [Google Scholar] [CrossRef]
- Lee, S.-W. SPECT/CT in the Treatment of Differentiated Thyroid Cancer. Nucl. Med. Mol. Imaging 2017, 51, 297–303. [Google Scholar] [CrossRef]
- Schlumberger, M.; Leboulleux, S. Current practice in patients with differentiated thyroid cancer. Nat. Rev. Endocrinol. 2021, 17, 176–188. [Google Scholar] [CrossRef]
- Avram, A.M.; Esfandiari, N.H.; Wong, K.K. Preablation 131-I scans with SPECT/CT contribute to thyroid cancer risk stratification and 131-I therapy planning. J. Clin. Endocrinol. Metab. 2015, 100, 1895–1902. [Google Scholar] [CrossRef]
- Hommadi, M.; Belemlih, M.; Marnouch, E.; Maghous, A.; Zaghba, N.; Hamidi, F.Z.; Bazzine, A.; Saghir, K.A.; Elmarjany, M.; Sifat, H.; et al. Intramedullary spinal cord metastases: Report of three cases and review of the literature. Cancer/Radiothérapie 2021, 25, 169–174. [Google Scholar] [CrossRef]
- Hashii, H.; Mizumoto, M.; Kanemoto, A.; Harada, H.; Asakura, H.; Hashimoto, T.; Furutani, K.; Katagiri, H.; Nakasu, Y.; Nishimura, T. Radiotherapy for patients with symptomatic intramedullary spinal cord metastasis. J. Radiat. Res. 2011, 52, 641–645. [Google Scholar] [CrossRef] [Green Version]
- Redmond, K.J.; Lo, S.S.; Soltys, S.G.; Yamada, Y.; Barani, I.J.; Brown, P.D.; Chang, E.L.; Gerszten, P.C.; Chao, S.T.; Amdur, R.J.; et al. Consensus guidelines for postoperative stereotactic body radiation therapy for spinal metastases: Results of an international survey. J. Neurosurg. Spine 2017, 26, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadzipasic, M.; Giantini-Larsen, A.M.; Tatsui, C.E.; Shin, J.H. Emerging Percutaneous Ablative and Radiosurgical Techniques for Treatment of Spinal Metastases. Neurosurg. Clin. N. Am. 2020, 31, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Glicksman, R.M.; Tjong, M.C.; Neves-Junior, W.F.P.; Spratt, D.E.; Chua, K.L.M.; Mansouri, A.; Chua, M.L.K.; Berlin, A.; Winter, J.D.; Dahele, M.; et al. Stereotactic Ablative Radiotherapy for the Management of Spinal Metastases: A Review. JAMA Oncol. 2020, 6, 567–577. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volpe, F.; Piscopo, L.; Manganelli, M.; Falzarano, M.; Volpicelli, F.; Nappi, C.; Imbriaco, M.; Cuocolo, A.; Klain, M. Intramedullary Spinal Cord Metastases from Differentiated Thyroid Cancer, a Case Report. Life 2022, 12, 863. https://doi.org/10.3390/life12060863
Volpe F, Piscopo L, Manganelli M, Falzarano M, Volpicelli F, Nappi C, Imbriaco M, Cuocolo A, Klain M. Intramedullary Spinal Cord Metastases from Differentiated Thyroid Cancer, a Case Report. Life. 2022; 12(6):863. https://doi.org/10.3390/life12060863
Chicago/Turabian StyleVolpe, Fabio, Leandra Piscopo, Mariarosaria Manganelli, Maria Falzarano, Federica Volpicelli, Carmela Nappi, Massimo Imbriaco, Alberto Cuocolo, and Michele Klain. 2022. "Intramedullary Spinal Cord Metastases from Differentiated Thyroid Cancer, a Case Report" Life 12, no. 6: 863. https://doi.org/10.3390/life12060863